| International Journal of Mental Health Promotion |
DOI: 10.32604/ijmhp.2022.018857
ARTICLE
The Effect of Brain Gym on Global Cognitive Function of Institutionalized Older People
1Escuela Superior de Tlahuelilpan, Universidad Autónoma del Estado de Hidalgo, Tlahuelilpan, Hidalgo, México
2Escuela Nacional de Enfermería y Obstetricia. Universidad Nacional Autónoma de México, Mexico City, México
3Departomento de Bioingenieria, Unidad Profesional Interdisciplinaria de Biotecnología del Instituto Politecnico Nacional (UPIBI-IPN), Mexico City, Mexico
4Instituto de Ciencias de la Salud. Universidad Autónoma del Estado de Hidalgo. Pachuca, Hidalgo. México. Scuela Superior de Tlahuelilpan, Universidad Autónoma del Estado de Hidalgo, Tlahuelilpan, Hidalgo, México
*Corresponding Author: Araceli Cano-Estrada. Email: edith_cano@uaeh.edu.mx
Received: 21 August 2021; Accepted: 26 November 2021
Abstract: Cognitive function of older adults is influenced by several factors such as age, sex, education, and physical activity so that it can impact the decrease in progressive cognitive function. It is necessary to implement cognitive training in old people’s care to prevent or delay the onset of age-related cognitive decline. Brain gym is a series of simple motion exercises and is an alternative therapy that stimulates the brain. This study aims to evaluate the effect of brain gym as a cognitive training intervention on global cognitive functioning of institutionalized older population. The study is a non-randomized quasi-experimental one using pre-and post-test control group design. The participants of the study were 65 years old or older who had been part of gerontological centers from a local community. They were divided into two groups: control and intervention, each one with 15 people. Mini-Mental State Examination was applied to the sample before and after the cognitive training. The brain gym training consists of bi-weekly group meeting for 12 weeks, lasting 50 min each. The treated group had a significantly better global cognitive function. Recalling (memory), orientation and language skills were the domains with the most significant changes (p < 0.05). On the other hand, no significant changes were found in the participants of control groups during post test. Our results suggest that cognitive training based in brain gym improves global cognitive function of institutionalized older people lease type your abstract here. Abstract of a research paper is typically 200 to 400 words in length, and 150 to 300 words for a review paper. Abstract shall be running continuously (not structured) and shall not include reference citations. Abbreviations that appear only once in the abstract should be defined in full. If abbreviations appear more than once, the full definitions should be provided first before they can be used elsewhere.
Keywords: Cognitive function; brain gymnastic; older people; gerontological center; physical activity
Cognitive skills play a crucial role in our daily functioning. Unfortunately, cognitive impairment is one of the most common complaints of aging, and the prevalence increases with age [1,2].
There are different tests to evaluate cognitive impairment, one of the most used at the international level is Mini Mental State Examination (MMSE). It is a simple test that evaluates different cognitive functions, and it can be tested in a little time, around 10 min. This test has been translated to different languages and it has good psychometry properties. Although among its limitations it does not allow to distinguish between the different types of dementia and mild cognitive impairment [3].
There are several risk factors that appear to have an impact on cognitive decline. Age, race and ethnicity, gender, and genetics are non-modifiable risk factors, while the modifiable risk factors are diabetes, head injuries, lifestyle, and education [4].
It is suggested that cognitive training is considered a useful non-pharmacological intervention activity for older people. The areas of cognition that are often examined include memory, language, visuospatial ability, speed of information processing, attention, and executive functioning [5–7]. Evidence suggests that cognitive training improves cognitive test performance in otherwise healthy older adults for the domain they are trained in [8–10].
Brain gym is a collection of simple movements aimed at connecting or uniting the mind and body. It was developed by Paul and Gail Dennisson in 1970 to improve various outcomes, including attention, memory, and academic skills [11]. Brain gym is a Kinesiology education program that has been promoted and applied in over 87 countries [12]. Kinesiology is defined as the study of the body’s movements and the relationship between the brain and body’s posture and brain functioning. All the movements taught in brain gym can increase the learning process and integrate all areas related to the learning process [13]. The brain gym materials have been translated into over 40 languages [12].
Brain gym interventions have been applied to children to increase their academic performance [14,15]. However, it is also suggested that brain gym can be considered a useful physical therapy strategy for older adults since it can have a positive impact on brain functioning. A quasi-experimental study involving a group of healthy older adults shows they improved their cognitive performance through specific patterns of movements and brain exercises, very similar to the ones described in the Brain Gym Manual [16]. A small randomized controlled trial showed that brain gym intervention can enhance cognitive performance, specifically attention and memory, in older adults with dementia [17]. A similar result was found by Mendrofan et al. [18] in a quasi-experimental study using pre-and post-test design. In addition, a study on 68 older adults who had undergone brain gym for eight weeks found an increase in the quality of sleep and reduced anxiety [19]. However, it is considered that there is still little evidence to support the claims made about the benefits of brain gym on older adults with dementia.
It is important to mention that most of the studies about cognitive impairment have been in community-dwelling older adults and with interventions based on traditional exercise. This research was carried out with older adults who have attended the gerontological center, but they are part of a semi-rural population; so, they have low economic resources and low academic level. Scientific evidence is scarce about the cognitive impairment in this kind of population. Additionally, few studies have evaluated the benefit of new cognitive training.
In the present work, cognitive training based on brain gym was implemented on healthy institutionalized older people to evaluate the maintenance or improvement of global cognitive function.
This is a quasi-experimental, no randomized study with a pre-and post-test design to evaluate an intervention based on brain gym in institutionalized older adults through measuring the cognitive performance. It was no financed study, and it was done over four months due to the permission given at the institutions.
The participants were institutionalized older adults (≥65 years of age). The number of samples in the study was 30 older adults who attend gerontological centers from a local community and were willing to participate in the study. The sampling was no randomization, which was based on inclusion and exclusion criteria. In addition, for instructions of the institutions, the older adults were assigned by the chief of the gerontological center, into each group study, intervention group (n = 15), and a control group (n = 15). All the participants read and signed an informed consent about the aim of this research.
The inclusion criteria were as follow: i) aged 65 years old or above, ii) attended a gerontological center between 6 month and 3 years, iii) absence of a clinical diagnosis of dementia, and iv) independent ambulation. For the present study, people who presented any comorbidities or any acute illness were excluded, as well, older adults who have taken part in any other physical exercise or memory training program in the last 6 months and older people with severe visual impairment or hearing loss. In addition, people who did not finish the intervention program were eliminated from the study.
Mini-Mental State Examination (MMSE) was applied to all participants to determine their global cognitive function [20]. The MMSE instrument consisted of five domains, namely orientation, registration, attention, and counting, recalling, and language skills, described in 11 question items. The interpretation in the results of the MMSE is that if the MMSE value is in the range 24–30, then it is included in the category of normal cognitive function, while if it is less than or equal to 23, then it indicates reduced cognitive functioning.
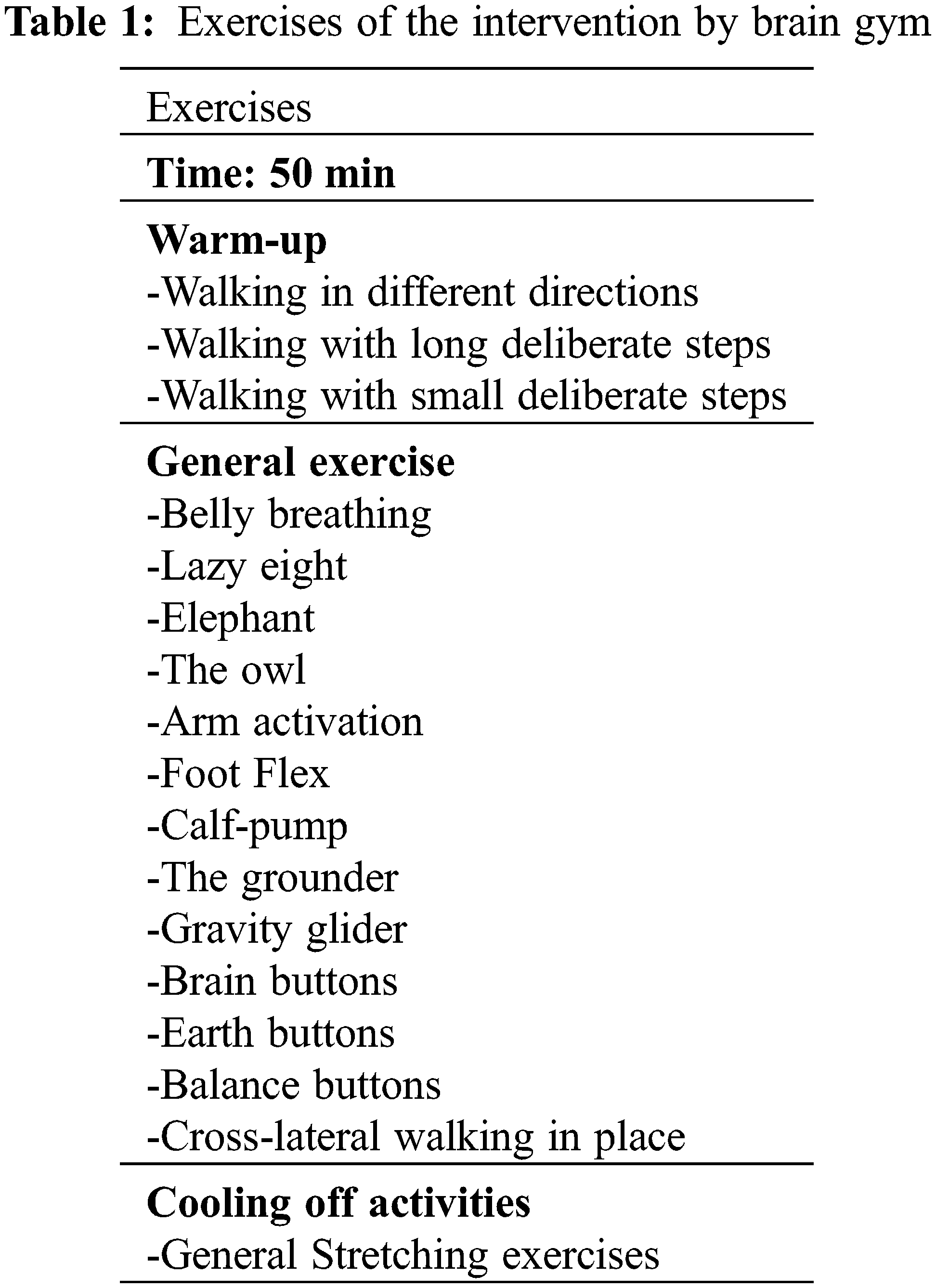
The intervention consisted of two sessions per week for 12 weeks and each session lasted for about 50 min. The participants were informed about the aspect that would be taken into account to include them in the program, with the purpose of motivating them and getting a good adherence level in the study. The program involved 10 min of warm-up exercises, 30 min of general excursive, focusing on fine motor involvement, balance, and hand-eye coordination, and, finally, five minutes of general stretching exercises for cooling-off activities [21]. All the exercises were explained and demonstrated to the intervention group. The first session included a presentation of cognitive function in old age. The movements used in each session are presented in Table 1. Notably, the control group only received educational talks on cognitive impairment.
Both groups were retested within two weeks following the completion of the cognitive training.
Data analyses were carried out with SPSS version 21. Pre-test and post-test comparisons were examined using a non-parametric test for dependent samples (Wilcoxon test), while Chi-square analyses were used to compare groups at the baseline of demographic variables. The comparison between the control group and intervention group as well as numeric variables (age and MMSE scores) were performed using the t-test for independent samples. Finally, multiple regression was performed to analyze the contribution of age and education on the cognitive function of older people. The level of significance was set at α < 0.05.
The research protocol followed the guidelines provided by the Helsinky Statement about biomedical research for humans [22] at the international level and General Law of Health at the national level [23]. The study was approved by the local ethics committee, and written informed consent was provided by all participants.
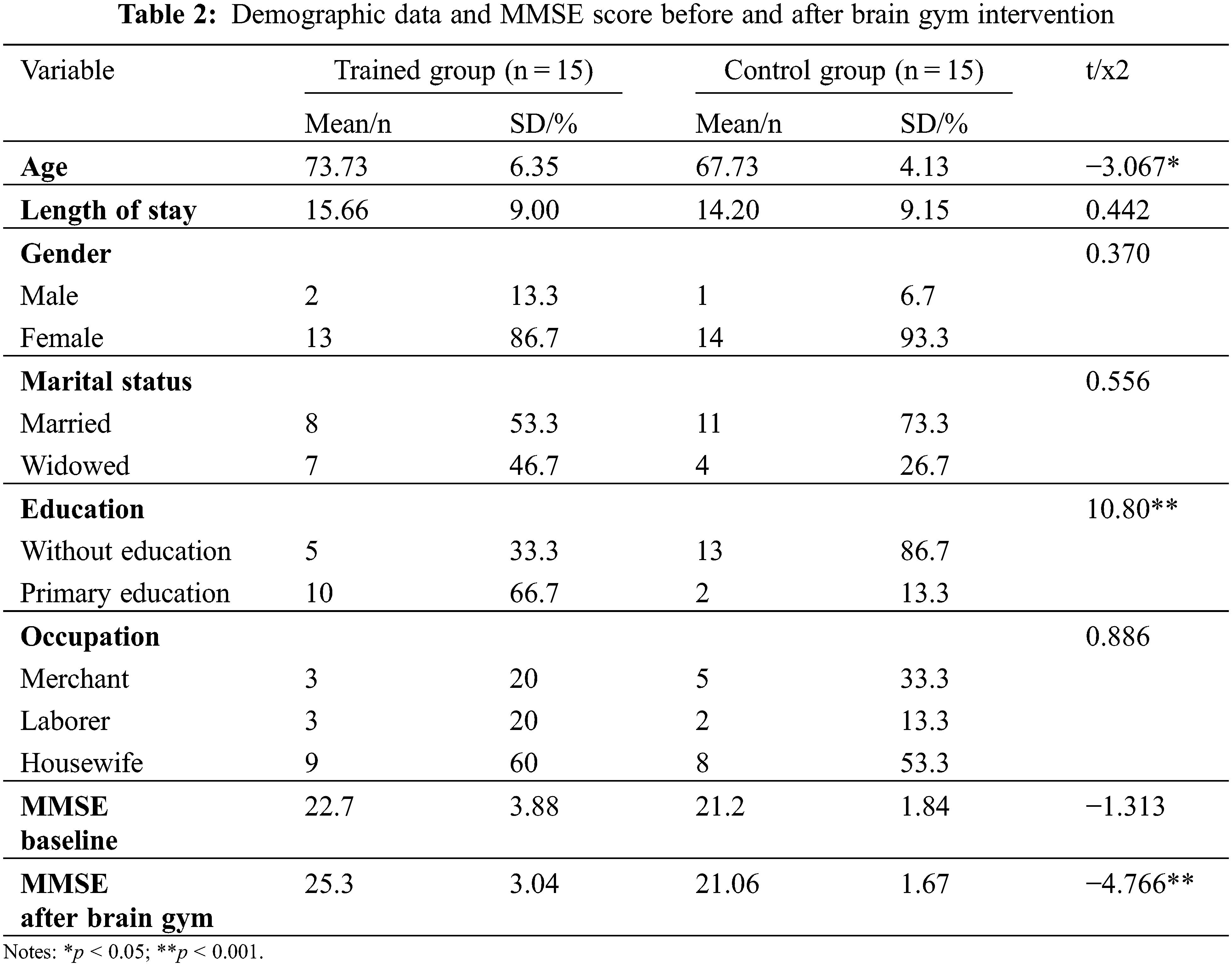
The overall sample had a mean age of 70.73 ± 6.08 years. Both groups had more females (90%) and most of them were housewives (63.33%). The sample was predominantly married (60%) and had low-level education. The length of stay was reported in months, and there was 1.4 months of difference between average length of stay of control and intervention group. Into the gerontological centers were not older adults diagnosed with dementia, but there were 9 older adults with mild cognitive impairment in the intervention group and 14 older adults with mild cognitive impairment in the control group.
There were no statistical differences between the treatment and control groups with respect to gender, length of stay, marital status, and occupation (p > 0.05); however, there was a significant number of people in the control group who had received no education (p < 0.01). In addition, there were significant differences in the age of the participants between the intervention and control groups (p < 0.01).
Table 2 shows the sample’s characteristics by group. The mean MMSE score at the baseline was without the normal range (<24) in both groups. The mean MMSE score was within a normal range (≥24) only in the training group after intervention by brain gym.
A model was performed using multiple regression analysis to predict to what extent age and education can affect the amount of change in the MMSE score (Table 3). The education model was y = 15.740 + 2.899x, this model explains around 17% of the total amount of change in the MMSE score. On the other hand, no statistical significance was found in the interaction between age and the amount of change in the MMSE score. Therefore, there is a possibility of residual confounding, which means, the intervention group tended to be more educated, and it could be a confounding factor on the increase in MMSE score.

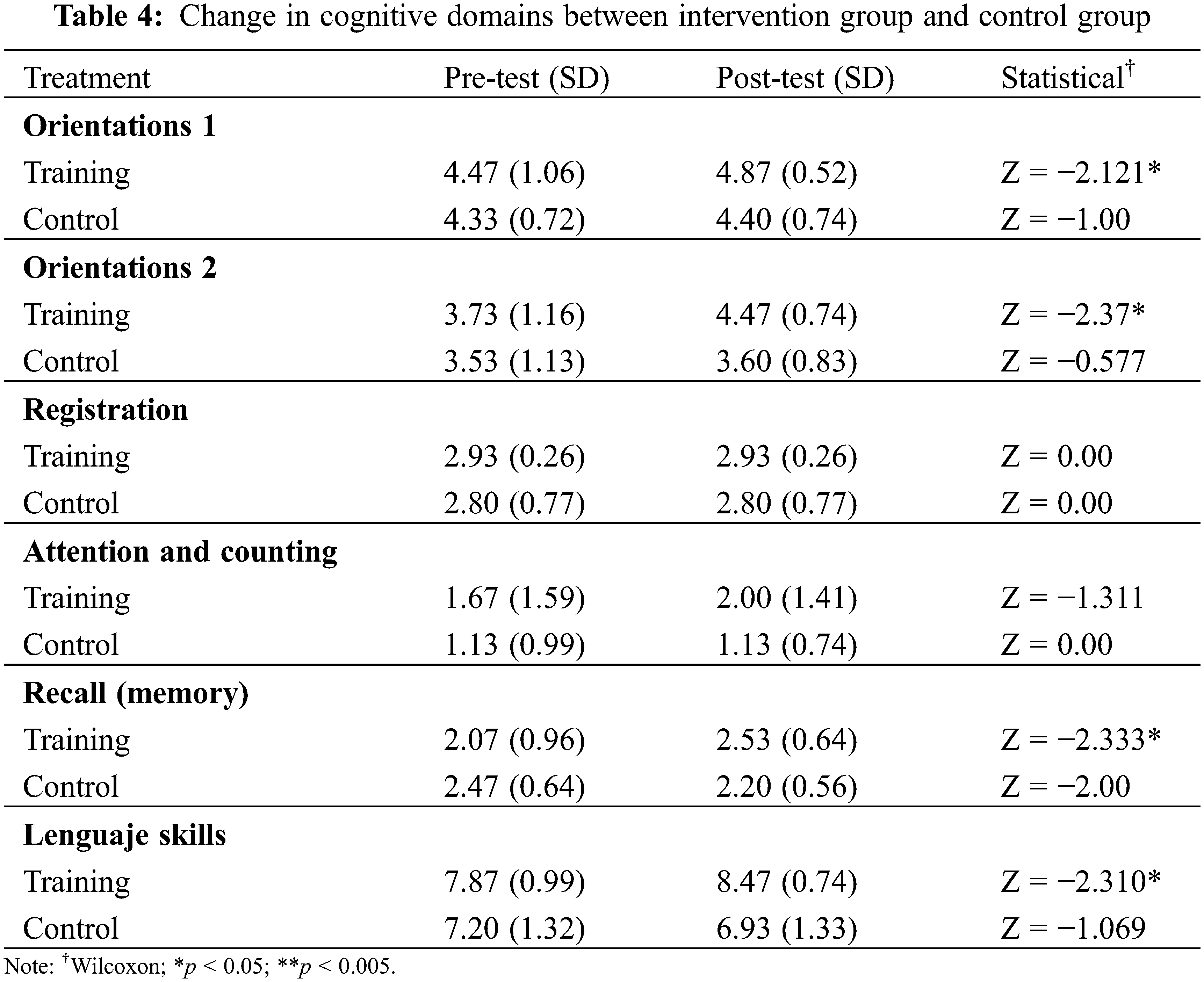
The orientation, attention, and counting, recalling (memory) and language skills were the domains that were found among most participants with the lowest mean MMSE score. No significant differences were detected between the control and intervention groups in the levels of cognition skills evaluated. All the intervention group participants attended all the sessions of brain gym.
Table 4 shows the groups’ means and standard deviation of the dependent variables at pre-test and post-test as well as the statistical value. After completing the training, there were significant changes in orientation, recalling (memory) and language skills among the participants of the intervention group (p < 0.05). There was a better score in attention skills, but it was of no statistical significance (p > 0.05). In addition, no significant changes were found in the participants of control groups in post-test (p > 0.05).
Different studies investigate the effect of cognitive training in preventing cognitive impairment [24] where structured activities were deployed to stimulate brain functioning. Physical exercises have been regarded as useful in improving cognitive functioning in older people, including those with cognitive impairment. The same is associated with aerobic exercises regarding modest improvements in attention, memory, speed processing, and executive function among older people. It is shown that brain gym has had the same results as traditional exercises [21,25]. In the present study, improvement in language, orientation, and memory (delayed recalling) was observed with brain gym intervention. Nevertheless, there are some limitations in this research as such the small and no randomized sample into the intervention and control group. Also, the intervention does not have a following in the time to estimate the duration of cognitive improvement.
In older people with normal cognition functioning, training improves cognitive performance in the domain of training, but evidence regarding prevention or delay of cognitive decline or dementia seems to be insufficient [9]. However, it has concluded that brain gym improves cognitive functioning in older adults with dementia [18]. Another study found significant differences in attention and memory in Alzheimer’s patients after applying brain gym [17].
Cognitive training appears to improve global cognitive function in the shorter term for people with mild cognitive impairment. Brain gym is a series of simple movements using the whole brain which are fun to do and improve learning skills. It also facilitates the flow of blood and oxygen into the brain [26]. The brain gym movement reactivates the neural pathways between the body and the brain, stimulating brain function to be more effective in the elderly [25].
In this study, the older people who presented normal cognition and attended cognitive training presented a major score in MMSE test. This is consistent with other studies, implying that brain gym has positive significant effects on cognitive functioning represented by the elderly by an increase of the MMSE score [27].
In this study, participants who had the lowest academic levels presented lower scores in the MMSE test. According to the results, which suggest that education is robustly associated with the level of cognitive functioning but not with the rate of cognitive impairment [28], having a higher level of education accompanied by being from higher social strata is assumed to reduce cognitive function decline [29]. However, there is evidence that age and education affect the MMSE score. People with higher education have a major score, while aged people with low education get a lower score [30]. Since in the present study the educational background of the intervention group was major than the control group, it cannot be denied that improvement of cognitive function may be an effect other than intervention, which is another study limitation.
Considering that there is no perfect test for cognitive impairment since all of them are affected by age and education, a test that applies at the community level is required. For future research, it suggests using more than one test to evaluate cognitive functions.
On the other hand, the results of the study first show that all participants present low MMSE scores; therefore, it is important to design and implement interventions for the delay and improve cognitive decline in older people. Exercises under brain gym stimulate the brain by releasing stress, increasing learning concentration, clearing the mind, and improving memory, so it is important to continue researching it [31].
Due to demographic changes, the elderly population is growing at a frantic pace. In most developed countries, the number of older people will outnumber the 15 years old or younger [32]. This shift in population will consequently result in many social and economic problems. Therefore, it is important to develop appropriate measures and strategies to prolong the active age of older individuals and improve their global cognitive function and quality of life.
The present study could be the base of future research on institutionalized older adults and a semi-rural or rural population about cognitive performance. In addition, this research is an approach to test an intervention to maintenance or improvement a cognitive function with new strategies as such as brain gym.
Acknowledgement: The Gerontological Centers from Hidalgo State in Mexico are acknowledged for their support in the development of this research.
Funding Statement: The authors received no specific funding for this study.
Conflicts of Interest: The authors declare that they have no conflicts of interest to report regarding the present study.
1. Salthouse, T. (2012). Consequences of age-related cognitive declines. Annual Review of Psychology, 63, 201–226. DOI 10.1146/annurev-psych-120710-100328. [Google Scholar] [CrossRef]
2. Harada, C. N., Love, M. C. N., Triebel, K. (2013). Normal cognitive aging. Clinics in Geriatric Medicine, 29(4), 737–752. DOI 10.1016/j.cger.2013.07.002. [Google Scholar] [CrossRef]
3. Llamas-Velasco, S., Llorente-Ayuso, L., Contador, I., Bermejo-Pareja, F. (2015). Spanish versions of the minimental sate examination (MMSE). Questions for their use in clinical practice. Revue Neurologique, 61(8), 363–371. DOI 10.33588/rn.6108.201507. [Google Scholar] [CrossRef]
4. Klimova, B., Valis, M., Kuca, K. (2017). Cognitive decline in normal aging and its prevention: A review on non-pharmacological lifestyle strategies. Clinical Intervention in Aging, 12, 903–910. DOI 10.2147/CIA.S132963. [Google Scholar] [CrossRef]
5. Kwok, T. C. Y., Bai, X., Li, J. C. Y., Ho, F. K. Y., Lee, T. M. C. (2012). Effectiveness of cognitive training in Chinese older people with subjective cognitive complaints: A randomized placebo-controlled trial. International Journal of Geriatric Psychiatry, 28(2), 208–215. DOI 10.1002/gps.3812. [Google Scholar] [CrossRef]
6. Vidovich, R. L., Lautenschlager, N. T., Fliker, L., Clare, L., McCaul, K. et al. (2014). The PACE study: A randomized clinical trial of cognitive activity strategy training for older people with mild cognitive impairment. The American Journal of Geriatric Psychiatry, 23(4), 360–372. DOI 10.1016/j.jagp.2014.04.002. [Google Scholar] [CrossRef]
7. Hyer, L., Scott, C., Atkinson, M. M., Mullen, C. M., Lee, A. et al. (2015). Cognitive training program to improve working memory in older adults with MCI. Clinical Gerontologist, 39(5), 410–427. DOI 10.1080/07317115.2015.1120257. [Google Scholar] [CrossRef]
8. Reichman, W. E., Fiocco, A. J., Rose, N. S. (2010). Exercising the brain to avoid cognitive decline: Examining the evidence. Aging Health, 6(5), 565–584. DOI 10.2217/AHE.10.54. [Google Scholar] [CrossRef]
9. Butler, M., McCreedy, E., Nelson, V. A., Desai, P., Ratner, E. et al. (2018). Does cognitive training prevent cognitive decline? Annals of Internal Medicine, 168, 63–68. DOI 10.7326/M17-1531. [Google Scholar] [CrossRef]
10. Toman, J., Klímová, B., Valis, M. (2018). Multidomain lifestyle intervention strategies for the delay of cognitive impairment in healthy aging. Nutrients, 10, 1560. DOI 10.3390/nu10101560. [Google Scholar] [CrossRef]
11. Denninson, G., Denninson, P. (1994). Brain gym: Teacher’s edition revised. Ventura, CA: Edu-Kinesthetics, Inc. [Google Scholar]
12. Brain Gym International. Brain Gym Program (2018). http://www.braingym.org. [Google Scholar]
13. Hoffman, S. J., Harris, J. C., Hoffman, S. J. (2009). Introduction to kinesiology, studying physical activity, pp. 570. USA: Human Kinetic Press. [Google Scholar]
14. Watson, A., Kelso, G. L. (2014). The effect of brain gym on academic engagement for children with developmental disabilities. International Journal of Special Education, 29(2), 7. [Google Scholar]
15. Marpaung, M. G., Sareharto, T. P., Purwanti, A., Hermawati, D. (2017). Brain gym to increase academic performance of children aged 10–12 years old (experimental study in tembalang elementary school and pedalangan elementary school semarang). 2nd International Conference on Tropical and Coastal Region Eco Development, vol. 55, 012017. Bali, Indonesia. DOI 10.1088/1755-1315/55/1/012017. [Google Scholar] [CrossRef]
16. Sidiarto, L. D., Kusumoputro, S., Munir, R., Nugroho, W. (2003). The efficacy of specific patterns of movements and brain exercises on the cognitive performance of healthy senior citizen in Jakarta. Medical Journal of Indonesia, 12(3), 155–161. DOI 10.13181/mji.v12i3.107. [Google Scholar] [CrossRef]
17. Yágüez, L., Shaw, K. N., Morris, R., Matthews, D. (2011). The effects on cognitive functions of a movement-based intervention in patients with Alzheimer’s type dementia: A pilot study. International Journal of Geriatric Psychiatry, 26(2), 173–181. DOI 10.1002/gps.2510. [Google Scholar] [CrossRef]
18. Mendrofa, F. A. M., Iswanti, D. I., Hani, U. (2020). Efficacy o brain gym on the cognitive function improvement of people with dementia. Journal Keperawatan Jiwa, 8(4), 557–564. DOI 10.26714/jkj.8.4.2020.557-564. [Google Scholar] [CrossRef]
19. Effendy, E., Prasanty, N., Utami, N. (2019). The effects of brain gym on quality of sleep anxiety in elderly at nursing home care case medan. Macedoniana Journal of Medical Sciences, 7(16), 2595–2598. DOI 10.3889/oamjms.2019.397. [Google Scholar] [CrossRef]
20. Llamas-Velasco, S., Llorente-Ayuso, L., Contador, I., Bermejo-Pareja, F. (2015). Spanish versions of the minimental state examination (MMSE). Questions for their use in clinical practice. Revue Neurologique, 61(8), 363–371. [Google Scholar]
21. Cancela, J. M., Vila-Suaréz, M. H., Vaconcelos, J., Lima, A., Ayán, C. (2015). Efficacy of bain gym training on the cognitive performance and fitness level of active older adults: A preliminary study. Journal of Aging and Physical Activity, 23, 653–658. DOI 10.1123/japa.2014-0044. [Google Scholar] [CrossRef]
22. Association, W. M. (2001). world medical association declaration of Helsinki. ethical principles for medical research involving human subjects. Bulletin of the World Health Organization, 79(4), 373–374. World Health Organization. [Google Scholar]
23. Secretaría de Salud. Ley General de Salud. Titulo V. México (2021). http://www.diputados.gob.mx/LeyesBiblio/pdf_mov/Ley_General_de_Salud.pdf. [Google Scholar]
24. Kane, R., Butler, M., Fink, H., Brasure, M., Davila, H. et al. (2017). Interventions to prevent age-related cognitive decline, mild cognitive impairment, and clinical Alzheimer’s-type dementia. Report No. 17-EHC008-EF. Agency for Healthcare Research and Quality (US). [Google Scholar]
25. Ayán, C., Sánchez-Lastra, M. A., Cabenelas, P., Cancela, J. M. (2018). Effects of brain Gym® exercises in institutionalized older adults with cognitive impairment. Revista Internacional de Medicina y Ciencias de la Actividad Física y el Deporte, 18 (72), 769–781. [Google Scholar]
26. Suhari, S., Astuti, A., Rahmawati, P. M., Musviro, M. (2019). Brain gym improves cognitive function for elderly with dementia. International Conference of Kerta Cendekia Nursing Academy, 1, 57–62. DOI10.5281/zenodo.3365503. [Google Scholar] [CrossRef]
27. Ardian, I., Nuraini, N. (2018). The effectiveness of brain gym and brain vitalization gym in increasing cognitive function of the elderly in pucang gading social rehabilitation unit of semarang. NurseLine Journal, 3(1), 38. DOI 10.19184/nlj.v3i1.7001. [Google Scholar] [CrossRef]
28. Wilson, R. S., Hebert, L. E., Scherr, P. A., Barnes, L. L., Mendes de Leon, C. F. et al. (2009). Educational attainment and cognitive decline in old age. Neurology, 72, 460–5. DOI 10.1212/01.wnl.0000341782.71418.6c. [Google Scholar] [CrossRef]
29. Sangundo, M. F. (2016). Effect of brain gym practice to cognitive function of the elderly. Mutiara Medika, 9(2 Suppl 1), 86–94. [Google Scholar]
30. Romo-Galindo, D. A., Padilla-Moya, E. (2018). Use cognitive tests to detect people with dementia in Mexican population. Archivos de Neurociencias, 23(4), 26–34. [Google Scholar]
31. Azizah, L., Martiana, T., Soedirham, O. (2017). The improvement of cognitive function and decrease the level of stress in the elderly with brain gym. International Journal of Nursing and Midwifery Science, 1(1), 26–31. DOI 10.29082/IJNMS/2017/Vol1.Iss1.33. [Google Scholar] [CrossRef]
32. Szmigiera, M. (2017). Proportion of selected Age groups of world population in 2017, by region. Statista. https://www.statista.com/statistics/265759/world-population-by-age-and-region/. [Google Scholar]
 | This work is licensed under a Creative Commons Attribution 4.0 International License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. |