| International Journal of Mental Health Promotion |
DOI: 10.32604/ijmhp.2022.017555
ARTICLE
Neighborhood Disadvantage and Self-Esteem—Do Socioeconomic and Relational Resources Matter?
1Department of Sociology, Kyung Hee University, Seoul, South Korea
2Kent State University, 700 Hilltop Drive, Kent, OH, 44224, USA
*Corresponding Author: Manacy Pai. Email: mpai@kent.edu
Received: 04 June 2021; Accepted: 13 December 2021
Abstract: Extensive research suggests that living in a socioeconomically disadvantaged neighborhood is associated with poor mental health. Few studies, however, have examined (1) whether neighborhood disadvantage is associated with residents’ self-esteem; and (2) the extent to which individual-level socioeconomic resources such as income and education, and relational resources such as marriage and social support moderate the association between neighborhood disadvantage and self-esteem. This study employs data from the Americans’ Changing Lives panel survey (hereafter ACL), a 15-year panel study of the U.S. adult population ages 25 and older in original sample. Because hierarchical linear model was employed to analyze data, findings provide fixed effect coefficients for independent variables at both the individual and census tract levels while controlling for random intercepts between census tracts. Findings based on data from the 4th wave of ACL reveal that neighborhood disadvantage is not associated with self-esteem. We do, however, find that living in a disadvantaged neighborhood worsens self-esteem for those who have lower levels of informal social support and are currently unmarried. These findings imply that while neighborhood disadvantage does not necessarily impact self-esteem, neighborhood disadvantage is detrimental to the self-esteem of those who report lower level of relational resources.
Keywords: Neighborhood disadvantage; self-esteem; social support; marital status; buffering hypothesis; status discrepancy hypothesis
Neighborhood socioeconomic context is a critical social structure that has serious implications for mental health. Disadvantaged neighborhoods often mean limited access to education, employment, and health care, all of which influence levels of everyday stress and mental health [1–5]. That said, research also reveals that the psychological consequences of living in a disadvantaged neighborhood vary widely based on individual-level characteristics of the residents [6,7]. While most studies assessing the mental health effect of neighborhood disadvantage have focused on depression [8,9], we contend that an equally important measure of the psychological ramifications of living in a socioeconomically deprived neighborhood is self-esteem. Self-esteem is a critical psychosocial resource to enhance mental health.
In the present study, we extend past research in two important ways. First, we focus our attention on a relatively under-assessed outcome in the studies of neighborhood disadvantage—specifically, self-esteem—which reflects individuals’ overall evaluation of their self [10]. There are some studies that have examined the association of neighborhood disadvantage with self-esteem, but the data utilized in these studies were not nationally representative [11,12]. Second, we argue in favor of re-examining the relevance of individual-level factors, such as personal socioeconomic and relational resources within the context of neighborhood disadvantage and the relatively underexamined outcome of self-esteem. As Ross and Mirowsky in their 2008 study [13] argued, “If neighborhood socioeconomic status affects residents’ health over and above their personal socioeconomic status, then neighborhood SES is more than the sum of its residents’ socioeconomic status. If there is no significant neighborhood effect once personal SES is adjusted, this is evidence that the apparent neighborhood effect is really compositional, due to the socioeconomic characteristics of the individuals who live there.” Paying heed to this argument, in our study, we examine the extent to which the relationship between neighborhood disadvantage and self-esteem is moderated by two individual-level characteristics, namely (a) economic resources, such as education and income; and (b) relational resources, such as being married and informal social support.
Our study offers two competing hypotheses to test the extent to which individual SES and relational resources moderate the relationship between neighborhood disadvantage and self-esteem. On one hand, we utilize the stress buffering hypothesis [14] to predict that those with higher economic and relational resources are less susceptible to the strain presented by their immediate neighborhoods. On the other hand, we employ the status discrepancy hypothesis [6] to suggest that the negative impact of neighborhood disadvantage on self-esteem may be stronger for those with higher socioeconomic and relational resources because those with more resources may experience cognitive dissonance associated with the discrepancies between their own personal status and the status of their neighborhood.
A moderating effect of individual characteristics on the association between neighborhood disadvantage and self-esteem would help us identify social groups that may be particularly vulnerable to neighborhood deprivation and for whom institutional and social resources are most needed. No research, in our view, has investigated these competing hypotheses to account for the moderating effects of individual-level characteristics on the association between neighborhood disorder and self-esteem. Below, we first review existing research pertinent to the proposed research questions. Upon that, we test our research propositions drawing on data from the 4th wave of the Americans’ Changing Lives survey.
1.1 Neighborhood Disadvantage, Individual-Level Characteristics, and Self-Esteem
Disadvantaged neighborhoods are characterized by a concentration of persons or households with poor socioeconomic status, chronic unemployment, receipt of public assistance, and an overall lack of social order [15]. Physical traits of disadvantaged neighborhoods, such as dilapidated housing, crumbling infrastructure and unwanted and harmful commercial establishments, such as adult book/video stores can be distressing to residents. Residents of disadvantaged neighborhoods often lack access to the most basic services needed for everyday living. It is only logical to assume that disadvantaged living conditions wear down feelings of safety, pride, and confidence in one’s community and instead result in mental distress.
While these global neighborhood traits impact mental health [1–3], a growing body of research pays attention to how the link between neighborhood characteristics and mental health is conditioned by individual-level traits/resources of residents [6,7,16]. For instance, in their effort to distinguish the effects of neighborhood vs. individual-level characteristics on mental health, Wheaton et al. [16] found that current neighborhood conditions do not uniformly impact early adult mental health. Moreover, their study showed that the neighborhood effects that do emerge are due in part to the chronic stressors experienced at the individual level.
Only a limited body of research, however, has moved past using depression or depressive symptoms to examine how neighborhood disadvantage affects residents’ sense of self. Boardman et al. [17], for instance, examined whether neighborhood traits, such as unemployment, poverty, and receipt of public assistance affect residents’ sense of personal control. Their study highlighted the relevance of examining jointly global neighborhood traits and individual-level characteristics of residents in order to truly discern the impact of neighborhoods on the outcome of self-efficacy. Similarly, in their study on neighborhood context and personal control, Kim et al. [6] found that individual-level characteristics, namely race, moderate the negative impact of declining neighborhoods on sense of personal control.
Despite these efforts to understand the links between neighborhood conditions and mental health, we still do not know much about how living in a disadvantaged neighborhood impacts residents’ sense of self. Although studies have utilized self-efficacy (or personal control) as their outcome variable, self-efficacy is not tantamount to self-esteem. The two are interrelated but are not the same. Both possess their own distinctive properties. It is not necessary that individuals who have high self-efficacy also simultaneously enjoy a high sense of self or self-esteem. Our sense of self or self-esteem is likely to be shaped by how we think we are viewed by others [10]; the extent to which we can distinguish ourselves from others; and the extent to which we attribute what happens to us because of our own actions or inactions [18].
Association between neighborhood disadvantage and self-esteem is likely for a myriad of reasons. Contrary to previous assumptions, research today points out that there exists a considerable variability in self-esteem over one’s life course [19,20], and as such, self-esteem may, after all, be malleable to community intervention. Moreover, theory of reflected appraisals [21] posits that given that we as humans evaluate ourselves based on the opinions of us held by others, the characteristics and reputation of a neighborhood may help clarify associations between neighborhood deprivation and feelings of self-worth [22,23]. Sense of self or self-esteem, also, is likely to be affected negatively by disadvantaged neighborhoods because a disadvantaged neighborhood is likely to be perceived by residents as signs of abandonment both by their neighbors and the larger society. While individuals often can refurbish spaces within their own homes and apartments, changes to an entire neighborhood are more difficult to implement; instead, efforts to improve a neighborhood often emerge out of a community-wide initiative put together by all those living in the neighborhood. However, doing so becomes monumentally more difficult given that witnessing a breakdown in one’s community likely weakens social ties within the community. In the disadvantaged neighborhoods, individuals likely begin to lose their pride in their neighborhood and sense of control over their environment [18], which in turn may perpetuate reduced levels of self-esteem. Finally, given the scarcity of resources and opportunities (e.g., spatial mismatching), individuals living in poor neighborhoods are more likely to experience financial and social instability (e.g., job loss; foreclosure/eviction; strained social relationships; dwindling social networks). However, it is possible that those living in deprived communities attribute their social and financial failures to individual incompetence rather than the very realistic social and fiscal constraints placed on them by where they live. Put simply, it is possible for residents of deprived neighborhoods to blame themselves as opposed to realizing that they are trapped in a myriad of socially, economically, politically constricting conditions [24]. Consequently, such attributions of personal incompetencies may contribute to a diminished feelings of self-worth.
1.2 Moderating Mechanisms: Stress Buffering vs. Status Discrepancy Hypotheses
It is logical to assume that individuals’ socioeconomic status (SES) influences the type of neighborhood in which they reside. That is, those who are economically deprived with low levels of education and unstable jobs/income are more likely to end up in economically disadvantaged neighborhoods. They simply cannot afford to buy or rent houses in economically well-to-do neighborhoods. Consequently, as Ross et al. [13] put it: “If this is the case, then a vanishing association between neighborhood socioeconomic status and health with adjustment for individual socioeconomic status implies that the association was largely or entirely spurious—a compositional effect.” Our study tests precisely for this possibility. That is, does the association between neighborhood economic disadvantage and residents’ self-esteem vary based on their individual-level economic and social resources.
Drawing upon previous research of neighborhood disadvantage and mental health, we propose two competing hypotheses—stress buffering vs. status discrepancy—to account for how and why the association between neighborhood disadvantage and self-esteem is moderated by select individual attributes. In line with the stress process model [25,26], we argue that similar stressors do not similarly affect everyone’s self-esteem. The stress process model posits that individual characteristics may modify the stressor/stress outcome relationship. Personal socioeconomic resources, such as education and income and relational assets, such as social support and marriage are likely to protect residents from the otherwise psychologically harmful effects of a disadvantaged neighborhood. The buffering effect of individual-level resources in neighborhood studies already is being reported in several studies [27–29]. Individuals with greater socioeconomic resources or/and relational assets may be less susceptible to the detrimental neighborhood conditions that undermine one’s self-esteem because “loss of esteem may occur to the extent that the failure to cope adequately is attributed to one’s own ability or personality traits, as opposed to external cause” [14]. Accordingly, the impact of a disadvantaged neighborhood is suggested to be less damaging to the self-esteem of those who enjoy higher personal economic resources—education and income; and relational assets—namely, being married and enjoying strong informal relationships with friends, neighbors or/and relatives.
Alternatively, we utilize the status discrepancy hypothesis to argue that neighborhood disadvantage may be particularly draining on the self-esteem of those with greater socioeconomic and relational resources. Living in a disadvantaged neighborhood, individuals with greater socioeconomic and relational resources may feel isolated given the discrepancy between their personal status and the status of their neighborhood [30–32]. Individuals with scarce resources likely are accustomed to chronic stress because they are more likely to live in disadvantaged neighborhoods than people with greater resources. They may not experience the cognitive discrepancy from life in disadvantaged neighborhood, implying that neighborhood disadvantage is not an eventful or unexpected stressor. This is comparable to research on chronic illness that finds that older persons of lower SES are more accepting of chronic illness as they deem ill health to be the impending and as such, inescapable reality of their already difficult life [33]. Similarly, those with scarce economic and social resources may find it far less cognitively discrepant to live in neighborhoods that are disadvantaged. Contrarily, one study found that the negative effect of neighborhood disadvantage on sense of control, for instance, is more prevalent among those who report lower levels of economic hardship and are racial majority—whites—than their counterparts because “they may experience the cognitive dissonance between their perception of personal control and their surrounding community” [6].
Stress experienced by those who feel a discrepancy between their personal and neighborhood resources is not just limited to those with greater personal resources living in disadvantaged neighborhoods. There is some research that finds that by living in an affluent neighborhood, the less affluent people increase their risk of stress and ultimately mortality [34]. This could be because the cost of living in an affluent neighborhood may render residents with little to no disposable income to spend on things, they need most. The other assumption, however, is more reflective of the status discrepancy hypothesis. Put simply, it is not unreasonable to assume that being surrounded by well-to-do neighbors can dampen one’s sense of self and affect one’s health and well-being. In our study, we speculate that those with higher personal socioeconomic and relational assets are more vulnerable to neighborhood disadvantage given the discrepancy between their own status and the status of their immediate neighborhood.
In summary, neighborhood disadvantage is expected to negatively affect self-esteem, but residents’ self-esteem may not be uniformly influenced by neighborhood disadvantage. This study tests following hypotheses to examine the extent to which socioeconomic and relational resources moderate the influence of neighborhood disadvantage on self-esteem. The main analyses, therefore, test for interactions between neighborhood disadvantage and two types of individual resources in predicting self-esteem.
H1-1: The negative effect of neighborhood disadvantage on self-esteem is lower for residents with currently married and strong social support (Buffering hypothesis for relational resources).
H1-2: The negative effect of neighborhood disadvantage on self-esteem is greater for residents with currently unmarried and weak social support (Discrepancy hypothesis for relational resources).
H2-1: The negative effect of neighborhood disadvantage on self-esteem is lower for residents with more education and income (Buffering hypothesis for socioeconomic resources).
H2-2: The negative effect of neighborhood disadvantage on self-esteem is greater for residents with less education and income (Discrepancy hypothesis for socioeconomic resources).
This study employs data from the Americans’ Changing Lives panel survey (hereafter ACL), a 15-year panel study of the U.S. adult population ages 25 and older in original sample. The stratified, multistage area probability sample was drawn with an oversampling of both adults ages 60 and older and black adults. First wave in 1986 was conducted with 3,617 respondents, representing 70 percent of sampled households and 68 percent of sampled individuals. Wave 2 data was obtained in 1989, and wave 3 data was obtained in 1994. We use wave 4 data obtained in 2001 and 2002 to utilize census information collected in 2000. A fourth wave of panel study was conducted via telephone or face-to-face interviews when respondents were not available for interview. The final sample includes 1,787 respondents including proxy (n = 95) information, with a response rate of 83% of the respondents who survive after third wave. We did not exclude proxy information unlike previous study using same data [35], because we did find no significant difference in main findings with or without proxy information (results available upon request). 15 years have passed since first survey was administered, age ranges from 40 to 99.
This study uses 4th wave of ACL, obtained in 2002, linked to 2000 census information, there is limitation of data in that up-to-date census data of 2010 are not employed and structural changes in neighborhood since 2000 are not reflected. Despite these weakness in data, ACL are nationally representative data and recent studies examining neighborhood contexts and self-esteem employ regional data [12,36], which prevents finding national implication. In addition, neighborhood characteristics at the level of census tract may vary between 2000 and 2010 census data, our focus is not to examine trajectory of self-esteem over years and to compare the association of neighborhood disadvantage with self-esteem over period. Accordingly, we use ACL data collected in 2002 combined with 2000 census data for present study.
Self-esteem is respondents’ beliefs about their own general self-worth. Respondents’ beliefs about their own general self-worth were measured with three items from Rosenberg’s global self-esteem scale [37]: 1) “At times, I think I am no good at all”; 2) “All in all, I am inclined to feel that I am a failure”; and 3) “I take a positive attitude toward myself”. Responses were coded on a four-point scale, including “Strongly agree” (1), “Agree somewhat” (2), “Disagree somewhat” (3), and “Strongly disagree” (4). At each wave, a self-esteem index was created by computing a mean across the three items. One question, “I take a positive attitude toward myself” was reverse coded before being averaged in with other 2 items. All 3 items were standardized before being combined and then re-standardized to take the mean across items [38].
The reliability of the three-item index of self-esteem was 0.58. Previous study did not include a question of “I take a positive attitude toward myself” to comprise self-esteem index to increase to reliability [39]; however, we retain all three questions for two reasons. First, even without positive attitude question to measure self-esteem, reliability did not increase (alpha = 0.57). Second, three item self-esteem index still has construct validity such that it is negatively correlated with depression (r = –0.48, p = 0.001) and mastery (r = 0.38, p = 0.001) consistent with theoretical expectation in previous studies [40,41]. Therefore, self-esteem index composed of three items is employed in original format.
Neighborhood disadvantage was created from census data in 2000. Neighborhood characteristics were measured at the level of census tract. A few studies investigating the neighborhood effects upon social behavior and outcomes which used same ACL data gathered neighborhood information from not only census tract but also block numbering area or enumeration district of the respondents [16,42]. This study uses neighborhood characteristics only from census tract which has relatively stable boundaries and similar demographics characteristics so that neighborhood information is more reliable and stable, however. Neighborhood disadvantage was constructed based upon scores from four neighborhood measures including (1) a percent of female-headed household, (2) a percent of household receiving public assistance, (3) a percent of adult unemployment rate, and (4) a percent of person under poverty. All four variables were extensively employed in recent research exploring the effect neighborhood disadvantage upon outcomes [3,35,43–45]. Objective measure of neighborhood disadvantage was an average score of four measures above.
Socioeconomic Resources: Education and income were presented to measure socioeconomic status. For education, which is coded intervally to represent the highest year of schooling completed and ranges from 0 to 17. We use bracketed education to reflect different levels of school by years of schooling: 1 = 0–8 years, 2 = 9–11 years, 3 = 12 years, 4 = 13–15 years, 5 = 16 years, 6 = 16 and over years. Because educational information was only asked at wave 1, education was measured in 1986. Household income is the gross income of the respondent and spouse. Income was coded continuously ranging from $0 (zero) to $275,000. We used the imputed income measure, cleaned, and imputed by the ACL staff and then divide it by 1,000 so that one-unit increase of income means an increase of one thousand dollars.
Relational Resources: Marital status and informal social support were utilized to measure relational resources. Marital status is a fundamental social condition from which individuals expect social support [46]. Being married means development of an intimate relationship where we provide and receive social support. It is true that marital status may be a stressor because marital relationship is often accompanied with marital problems [47]; however, married people likely receive support not only from their partners but also from confidants than non-married ones [48]. Therefore, marital status is considered as a relational resource in present study. Currently married is reference (coded 0), non-married (separated, divorces, and/or widowed) is coded 1, and never married is coded 2.
Informal Social support is constructed from two variables. Respondents were asked about their agreement with the following questions: (1) “On the whole, how much do your friends and other relatives make you feel loved and cared for?”, and (2) “How much are these friends and relatives willing to listen when you need to talk about your worries or problems?” Responses were coded from 1 to 5, where 1 = a great deal, 2 = quite a bit, 3 = some, 4 = a little, 5 = not at all. Both questions were reverse coded then standardized to compute mean score. We employ social support index provided by ACL staff. High score means stronger levels of social support.
We control for demographic variables that could create spurious association between neighborhood characteristics and self-esteem. Demographic variables include gender (1 = female, 0 = male) and race (1 = black, 0 = non-black). We also test more detailed classification of race (non-Hispanic white [reference], black, Hispanic, and Asians/Native Americans) in additional analysis, and found no significant difference in coefficients of main independent variables in results; therefore, we used a simple race classification for analyses. Age is also measured in number of years. We employ (age-40) to represent the linear function of age variable because forty is the youngest age among respondents. Finally, functional limitations are also controlled because the influence of neighborhood disadvantage is particularly salient for residents whose functional health is limited. Respondents were asked if they had any difficulties, and if so, how much, in performing a variety of daily tasks, including bathing by themselves, climbing a few flights of stairs, walking several blocks, and doing heavy work around the house such as shoveling snow or washing walls. We used the imputed version of functional impairment computed by the ACL staff, with high score representing a great deal of functional difficulty. Response categories included 1 = in bed most or all day due to health/has a lot of difficulty or cannot bathe self, 2 = has a lot of difficulty or cannot climb a few flights of stairs or walk several blocks because of health, 3 = has a lot of difficulty or cannot do heavy work around the house such as shoveling snow or washing walls because of health, and 4 = does not have a lot of difficulty doing heavy work around the house such as shoveling snow or washing walls because of health. Because functional limitation is skewed and 81% reported ‘does not have a lot of difficulty’ so that 1, 2, and 3 are merged into one category. In the analyses, people who report functional impairment are coded one and people who do not report functional impairment are coded zero.
This study employs multilevel data, utilizing the census tract as the approximation of the neighborhood contexts [2,49,50]. Previous studies using the Americans’ Changing Lives data also employed census tract as the basic unit of neighborhood [44,51]. Hierarchical linear model was employed to analyze data because OLS regression methods assume that observations are uncorrelated each other. Robert [42] argued that multilevel technique is not required to analyze Americans’ change lives data because data were collected in national level and within group variation does not warrant multilevel technique. Among 1,763 respondents, 615 people (34.8%) are only residents surveyed in each tract, but about 15% of census tracts contain more than 9 residents. Preliminary analysis estimated an intercept only model, showing a moderate size of intra-class correlation. Intra-class correlation coefficient was calculated by using variances of random effects to investigate the extent to which total variability in self-esteem among residents was due to variations between communities. Result is 0.225 (level two variance: 0.593, level one variance: 0.173 = (0.173)/(0.173 + 0.593) = 0.225), which means that about 22.5% was due to variations between tracts, leading us to test hierarchical linear models. Multilevel analysis is also employed in previous studies using ACL [44,51]. Because of the multilevel structure of data such that individuals are clustered within communities, findings provide fixed effect coefficients for independent variables at both the individual and census tract levels while controlling for random intercepts between census tracts [52]. The data were weighted to correct for sample selection probabilities and non-response.
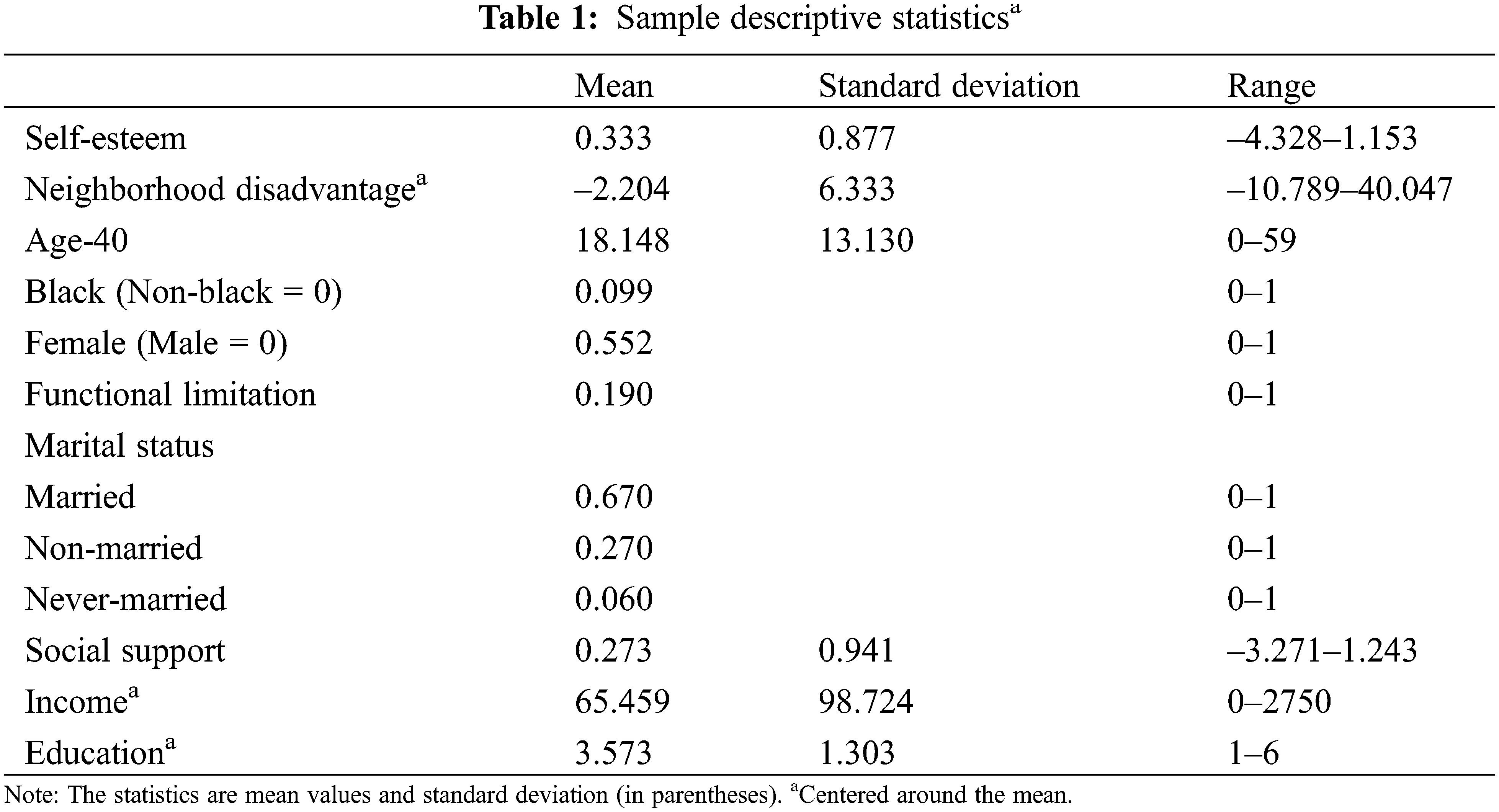
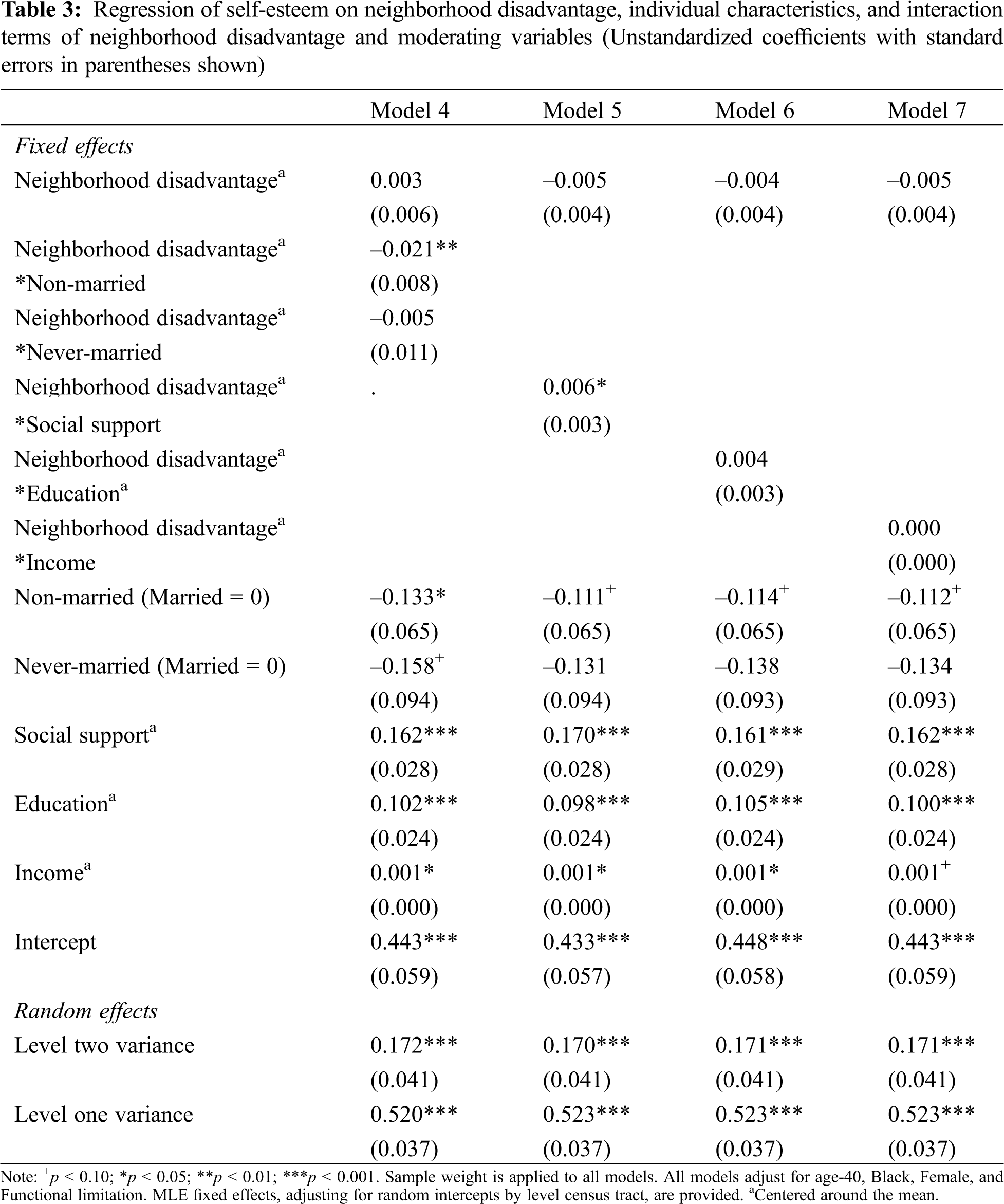
Table 1 reports descriptive statistics for all variables. Table 2 provides multi-level regression results. Self-esteem was progressively regressed on individual attributes to test hypotheses. Demographic and physical health variables are added in Model 1. Model 2 contains relational resource variables and Model 3 contains socioeconomic resource variable to see whether the association between neighborhood disadvantage and self-esteem is attributable to relational resource and socioeconomic resource variables respectively. Our main hypotheses are tested from Model 4 to Model 7. Model 4 is estimated with cross-level interaction terms between neighborhood disadvantage and marital status, and Model 5 is estimated with cross-level interaction term between neighborhood disadvantage and social support. Model 6 and Model 7 are respectively estimated with cross level interaction terms between neighborhood disadvantage and two measures of socioeconomic resource-education and income.
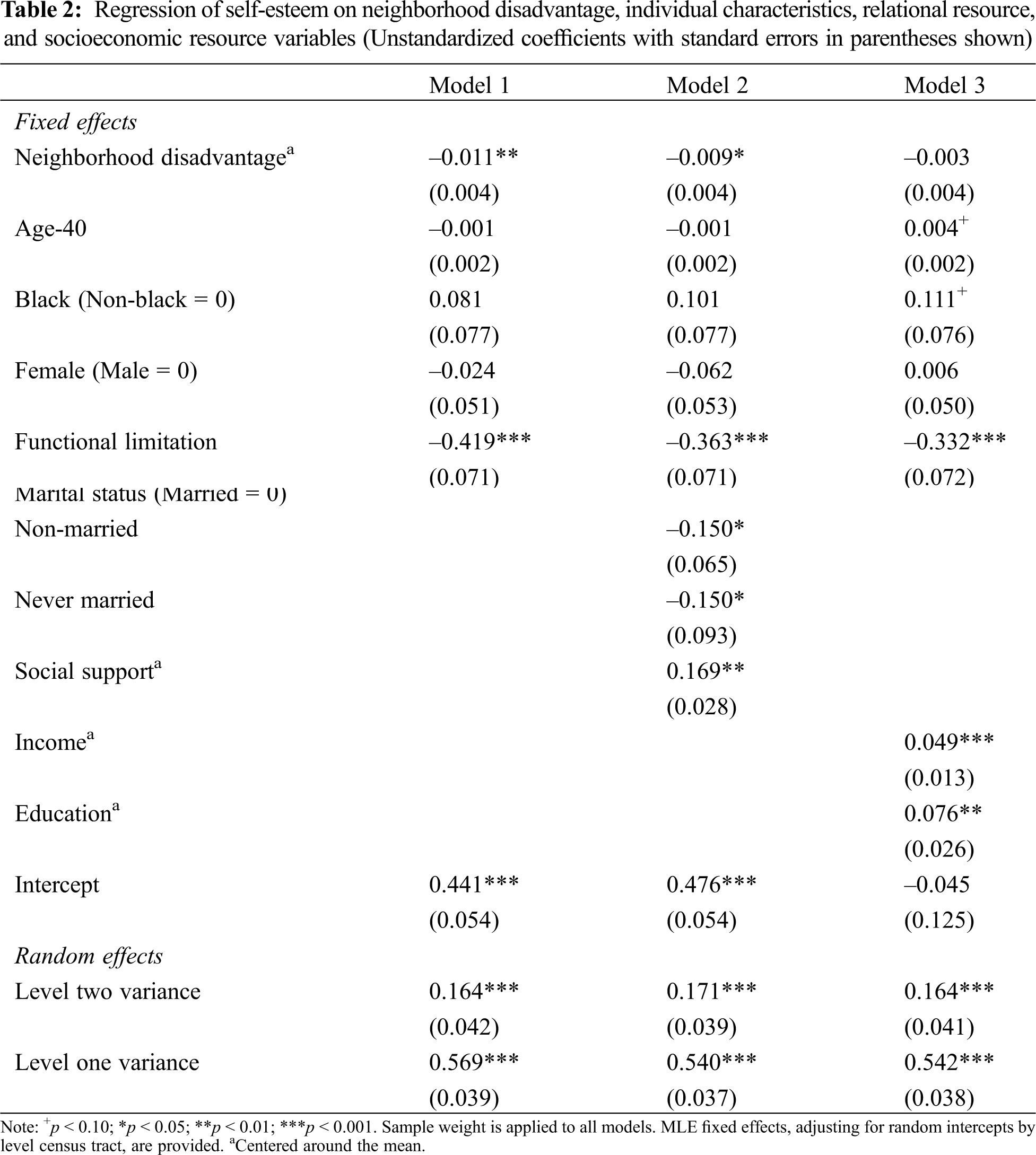
Neighborhood disadvantage is associated with decreased self-esteem with adjustment for gender, age, functional limitation, and race, as shown in Model 1 of Table 2. Age, race, and gender do not account for variation in self-esteem. With addition of social support and marital status, the effect of neighborhood disadvantage decreases about 22% ((0.011–0.009)/0.011) but remains significant at 0.05 level. Married persons show greater levels of self-esteem than non-married counterparts, and social support appears to have positive relationship with self-esteem. When individual socioeconomic resource is taken into consideration, neighborhood disadvantage is not associated with self-esteem. In supplementary analyses, income and education were added respectively to see which socioeconomic resource variable accounts for the association. Results (not shown) indicate that the inclusion of education appreciably accounts for the association of neighborhood disadvantage with self-esteem. Results from Model 1 to Model 3 are somewhat different from previous results which tests the impact of neighborhood disorder on self-esteem [11,36] and the impact of concentration of affluence in metropolitan areas on self-esteem [53] in that no association of neighborhood disadvantage with self-esteem is found. These contrary results show the association between neighborhood contexts with self-esteem still leaves room for further research.
Model 4 examines interaction between neighborhood disadvantage and marital status to investigate whether the association between the concentration of socioeconomic disadvantage in neighborhood and self-esteem varies by marital status. Interaction coefficient of non-married is negative and significant. Given that currently married is reference group, this result implies married people may be less influenced by neighborhood disadvantage in self-esteem compared with non-married. However, we found no statistically significant difference in self-esteem by neighborhood disadvantage between married and never married groups. Thus, buffering hypothesis (H1-1) is supported for non-married and discrepancy hypothesis (H1-2) is not supported. Model 5 investigates the moderating effect of social support. Social support is associated with greater levels of self-esteem, and interaction with neighborhood disadvantage is positive in predicting self-esteem. The negative effect of neighborhood disadvantage on self-esteem is attenuated by social support respondent receives. The influence of neighborhood disadvantage on self-esteem likely varies by levels of social support thus providing support for the buffering hypothesis. Like marital status, buffering hypothesis (H1-1) is supported and discrepancy hypothesis (H1-2) is not supported.
Model 6 examines interaction between neighborhood disadvantage and education to investigate whether the association between the concentration of socioeconomic disadvantage in neighborhood and self-esteem varies by levels of education. Interaction is not significant, implying that the detrimental effect of neighborhood disadvantage on self-esteem does not vary by residents’ levels of education. Even though “education develops habits, skills, resources, and abilities that enable people to achieve a better life” [54], learned effectiveness to deal with adversity and poor social resources in disadvantaged areas through education may not make a difference in association between neighborhood disadvantage and self-esteem. Thus, both buffering hypothesis (H2-1) and discrepancy hypothesis (H2-2) fail to find support. Model 7 investigates the moderating effect of income. Income is associated with greater levels of self-esteem but does not moderate the association between neighborhood disadvantage and self-esteem. The influence of neighborhood disadvantage on self-esteem is independent of levels of income. Both buffering (H2-1) and discrepancy (H2-2) hypotheses are not supported.
To better illustrate the buffering hypothesis, we plot the effects of neighborhood disadvantage on self-esteem at two different levels of social support based upon the results of Model 5 of Table 3. We compare individuals with lower level of social support (one standard deviation below the mean) to those with higher level of social support (one standard deviation above the mean). As shown in Fig. 1, residents of lower social support are predicted to show lower levels of self-esteem than those with greater social support from mean) with the increase of neighborhood disadvantage. Even though neighborhood disadvantage appears to have harmful effects upon self-esteem, it may be more pronounced among residents with poor social support. With strong social support, respondents may learn to cope with realities associated with neighborhood disadvantage. This finding supports the buffering hypothesis such that residents who have socioeconomic resource are likely to be less vulnerable to the detrimental effects of neighborhood disadvantage.
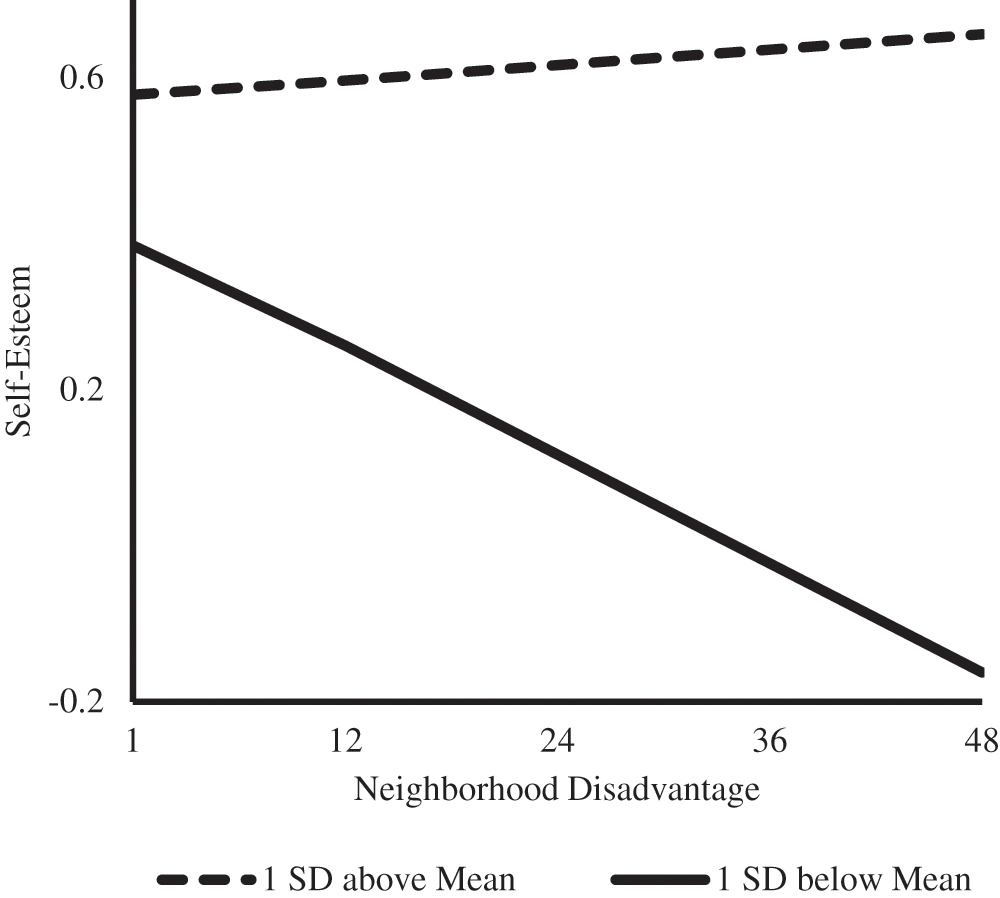
Figure 1: Neighborhood disadvantage and self-esteem at two levels of social support
The purpose of our study was to examine the impact of neighborhood disadvantage on the relatively under-assessed mental health outcome—self-esteem—in the studies of neighborhood context and mental health. Moreover, we wanted to assess the extent to which the relationship between neighborhood disadvantage and self-esteem is moderated by two individual-level characteristics, namely (a) socioeconomic resources, such as education and income; and (b) relational resources, namely marital status, and informal social support. Findings based on data from the 4th wave of ACL reveal that neighborhood disadvantage does not necessarily translate into poor self-esteem. Results, however, also show that living in a disadvantaged neighborhood worsens self-esteem for those who are currently unmarried and have lower levels of informal social support. These findings show that living in disadvantaged areas may have differing association with self-esteem by residents’ relational resources.
4.1 Marital Status and Informal Social Support Act as Buffers
Previous studies testing the moderating impact of individual-level resources on the link between neighborhood disadvantage and mental health provide inconsistent findings in that both buffering, and discrepancy hypotheses are supported depending upon health outcomes and measures of neighborhood characteristics [6,21,55,56]. According to the present study, people who are unmarried and have less social support are more vulnerable to neighborhood disadvantage than their counterparts with regard to self-esteem. Research demonstrates that one of the mechanisms linking marriage with positive mental health is the stress buffering function of spousal support [57,58]. When living in a neighborhood that you perceive to be lacking order, for instance, it is only reasonable to assume that having a spouse may render both emotional and practical help. There are reasons to believe that unlike other social relationships (e.g., friends, relatives, members of congregation), a marital relationship may involve more frequent interactions that may translate into a more sustained form of support. We argue that it could be a simple function played by a spouse like being able to share the common frustrations related to one’s living conditions or being able to take a walk in one’s neighborhood that you otherwise may perceive to be relatively unsafe.
Marriage especially among those who are otherwise socioeconomically disadvantaged and living in disadvantaged neighborhoods also may be a mark of personal achievement. Getting married was part of the American dream for all regardless of social class. Today, however, we see variations in marriage based on social class [53]. Specifically, more and more individuals from lower SES either delay or forgo getting married. At first blush, we might be eager to attribute this trend to the growing acceptance of non-marital relationships. And, while acceptance of cohabiting and other forms of family formation may play their part, the class divide in marriage is more reflective of the changing economic circumstances [59]. Unlike the past, today those without college degree lack stability in employment and income [59], both of which likely dissuade those in lower social class to tie the knot. When grappling with the otherwise poor social and economic conditions associated with disadvantaged neighborhoods, being married might signal a personal milestone or symbol of social status. As such, while the support offered by a spouse might be comparable to support found in other non-marital relationships, being married for those in disadvantaged neighborhoods may carry added heft.
Like spousal support, support from friends and relatives also play a role of a stress reliever. That is, the negative impact of disadvantaged neighborhoods is moderated by those who enjoy strong systems of informal social support. Friends and relatives often help identify or/and contextualize for us the stressors that we perceive as most threatening; they aid in crafting a plan to cope with stressors [60] and consequently, alleviate stress and restore emotional balance. Moreover, those in support network can help with informational support, namely by offering advice, guidance, and feedback on a situation [60,61]. During a crisis, emotional support in the form of a mere friendly ear can signal relief [60,61]. Regardless of the form in which support is given, it is the joint venture to help address the stressor that likely alleviates stress and maintains one’s sense of self-esteem.
The finding in our study that informal social support does help maintain self-esteem among those living in disadvantaged neighborhoods is of significance especially considering some research suggesting that living in disorderly and disadvantaged neighborhoods is associated with perceptions of low social support [4,62]. One speculation surrounding this finding is that the perceptions of lower support among residents of disadvantaged neighborhoods signal their own inability to effectively provide support to relatives, friends, and neighbors given the financial stress in their lives. Those living in disadvantaged conditions also may be less likely to trust their neighbors thereby impeding the formation of strong social bonds [63]. In light of these existing findings, our results revealing the protective effect of social support among those who live in disadvantaged neighborhoods yet again underscores the import of informal social networks for sense of self.
4.2 Why Do Higher Education and Income Not Act as a Buffers?
We were surprised to find that the relationship between neighborhood disadvantage and self-esteem is not conditioned either by education or income. Education provides both cognitive and non-cognitive skills, a variety of psychosocial resources (e.g., sense of control) that alleviate stress, foster happiness and ultimately are predictable of healthy self-esteem [54,64]. Education, according to the fundamental cause perspective, serves as a flexible resource that connects individuals to knowledge, money, power, and prestige [65]; and flexible resources operate in ways outside of the individual. That is, a person with higher education probably is likely to be surrounded by others with similar educational credentials and this by default may result in what Lutfey and Freese refer to as the “spillover benefits.” For example, those with higher education in a higher SES neighborhood enjoy the luxury of health-enhancing circumstances that come along as a package deal [66]. All those in such a neighborhood have the resources to maintain their immediate environment when it comes to factors, such as noise, litter, crime, and violence. These spillover benefits often are missing in disadvantaged neighborhoods and personal educational credentials probably do not translate into access to such benefits. That is, having a college or post-college degree, which signals one’s own personal accomplishment, may not come handy when it comes time to stopping street crime, fixing the crumbling roads and houses, or securing access to quality goods and services within one’s immediate neighborhood.
Like education, income is a resource that helps us cope with a variety of chronic stressors, including coping with ill health. Income helps at every stage of the life course ranging from being able to put children through good schools to making decisions related to one’s job, housing, health care, and retirement [65]. Those with higher income, consequently, likely enjoy heightened sense of self or self-esteem. That said, our study does not reveal income to play any role in the relationship between neighborhood disadvantage and self-esteem. Like in the case of education, income is only as good as its’ power to change one’s everyday circumstances. If one’s income does not translate into the luxury of living in a clean, safe, and orderly neighborhood, then personal income may mean very little for one’s sense of self. That is not to say that personal income does not carry its weight in terms of everyday outcomes of health and well-being. It very well does according to century worth of research connecting income and health [65–68]; however, in our study we find that personal income has no effect on the relationship between living in disadvantaged neighborhoods and residents’ sense of self or self-esteem.
4.3 Limitations and Future Directions
Taken together, our findings do extend the research on neighborhood disadvantage and mental health. The work here suggests that we recognize that the impact of community-based policies, programs, and interventions may not be equally consequential for all residents across all health outcomes. Our work, however, is not without limitations. First, Census tract information is employed to measure the extent of socioeconomic disadvantage in neighborhoods. However, researchers continue to question whether census tract is the most appropriate unit to uncover residential contexts. Future studies interested in carrying forward the present line of questioning should employ a multiprong approach to defining and examining “neighborhoods.” This approach could include development of census block group maps, review of land use, field visits and observation in the communities of interest.
Second, it also is possible that the lack of statistically significant relationship between neighborhood disadvantage and self-esteem was reflective of the measurement limitation of combining varied neighborhood characteristics into one index. Air pollution, noise, residential mobility, and the duration of residence are possible examples to overcome current approach to neighborhood operationalization based upon census information [69,70]. Future research, in addition to assessing neighborhood disadvantage, would benefit from exploring the differential impact on self-esteem of physical and social neighborhood disorder. Third, Rosenberg’s original self-esteem measurement contains 10 items, but ACL provides only three items to compute self-esteem score. This lack of data information may result in low reliability of self-esteem measurement and little association with neighborhood disadvantage as a result. Another data containing full items to measure self-esteem are expected to contribute to more nuanced findings.
Fourth, we do concede that selection bias remains a concern. We acknowledge that neighborhood self-selection can possibly inflate reported associations. Sorting out the extent of this potential selection bias remains a methodological challenge in research on the health implications of neighborhood conditions. In order to discern the collective socioeconomic status of the neighborhood, we followed Bosma and colleagues’ approach by aggregating and matching individual reports on socioeconomic status to the neighborhood level SES. While Bosma and colleagues assess the impact of neighborhood SES on mortality, in using this methodological approach, they posit the following: “An advantage of this approach is that the effect of neighborhood socioeconomic status on mortality can be stringently controlled for equivalent measures on the individual level. This allows an accurate examination of genuine contextual effects and, to a large extent, excludes the possibility that any adverse effect of poor neighborhoods is fully based on poorer people living in poorer neighborhoods [71].”
That neighborhood conditions affect our health and sense of self is hardly a surprise; however, the state of our mental health, particularly our sense of worth may be just as likely to shape the ways in which we perceive our neighborhood. Future studies, therefore, should test for the potential bidirectionality between neighborhood environment and self-esteem. Given the possibility for model misspecification, it also would be wise for future studies to test the influence of unobserved individual characteristics (e.g., personality predispositions). Selection bias raises some other issues as well. For instance, residents of economically deprived neighborhoods are less likely to live into late life. As such, our sample may represent a group of residents who have survived the harsh realities of their lives and become more psychologically resilient as a result of those experiences. That said, we argue that the findings in our study have emerged, not because of such selection biases, but despite of them. While we are constrained by data limitations, we do urge future researchers to rely on long-term prospective data and consider “pre-move” health and changes in residents’ health at several points of time “after their move” into neighborhoods.
Fifth, we use ACL’s fourth wave collected in 2002 to use 2000 census information for neighborhood measurement. Given that these data were first collected in 1986, 4th wave data contain respondents who survived over 16 years, which may have resulted in selection bias. That is, respondents with better health and higher social status may have selected into the sample [72]. Therefore, respondents in the 4th wave may be less influenced by neighborhood disadvantage than those who were part of the original sample, indicating that the characteristics of our study sample may be restricted to predict population parameters. Future inquiry employing more recent neighborhood information and appropriate sample framework might overcome these issues.
Finally, given that the data we utilized for this study are almost 20 years old, findings may seem less reliable in the evolving social and cultural contexts. That said, the present study emerges as a reminder for the significance of social networks and social capital on one’s sense of self and ultimately, health. Although ample attention has been provided to family members, who admittedly remain as the primary caregivers [73], there also has been renewed interest in other informal sources of support, such as neighbors and friends [74,75]. And this shifting focus towards non-kin ties is important given that family as a social institution continues to evolve, family structures change [76], more individuals make the choice to remain childless [77], and non-kin, including neighbors and friends become integral part of our present and future social network [78].
As such, moving forward, research should consider the differential impact of varied social relationships on the link between neighborhood disadvantage and self-esteem. For instance, if companionship and support are the key mechanisms helping married people maintain self-esteem amidst poor living conditions, what separates them from their peers who are in alternative yet committed relationships. Findings from our work here suggest that to truly discern the link between disadvantaged neighborhoods and mental health, researchers need to assess (a) mental health by utilizing different measures of it; and (b) wide array of individual-level attributes and the role they play both, additively and interactively, in predicting how neighborhood conditions similarly or differentially impact mental health of residents.
Funding Statement: The authors received no specific funding for this study.
Conflicts of Interest: The authors declare that they have no conflicts of interest to report regarding the present study.
1. Evans, G. W., Wells, N. M., Hoi-Yan Chan, E., Saltzman, H. (2000). Housing quality and mental health. Journal of Consulting & Clinical Psychology, 68(3), 526–530. DOI 10.1037/0022-006X.68.3.526. [Google Scholar] [CrossRef]
2. Finch, B. K., Phuong Do, D., Heron, M., Bird, C., Seeman, T. et al. (2010). Neighborhood effects on health: Concentrated advantage and disadvantage. Health & Place, 16(5), 1058–1060. DOI 10.1016/j.healthplace.2010.05.009. [Google Scholar] [CrossRef]
3. Haines, V. A., Beggs, J. J., Hurlbert, J. S. (2011). Neighborhood disadvantage, network social capital, and depressive symptoms. Journal of Health & Social Behavior, 52(1), 58–73. DOI 10.1177/0022146510394951. [Google Scholar] [CrossRef]
4. Cutrona, C. E., Wallace, G., Wesner, K. A. (2006). Neighborhood characteristics and depression—An examination of stress processes. Current Directions in Psychological Science, 15(4), 188–192. DOI 10.1111/j.1467-8721.2006.00433.x. [Google Scholar] [CrossRef]
5. Galea, S., Ahern, J., Nandi, A., Tracy, M., Beard, J. et al. (2007). Urban neighborhood poverty and the incidence of depression in a population based cohort study. Annals of Epidemiology, 17(3), 171–179. DOI 10.1016/j.annepidem.2006.07.008. [Google Scholar] [CrossRef]
6. Kim, J., Conley, M. E. (2011). Neighborhood disorder and the sense of personal control: Which factors moderate the association? Journal of Community Psychology, 39(8), 894–907. DOI 10.1002/jcop.20476. [Google Scholar] [CrossRef]
7. Wight, R. G., Ko, M. J., Aneshensel, C. S. (2011). Urban neighborhoods and depressive symptoms in late middle age. Research on Aging, 33(1), 28–50. DOI 10.1177/0164027510383048. [Google Scholar] [CrossRef]
8. Cromley, E. K., Wilson-Genderson, M., Pruchno, R. A. (2012). Neighborhood characteristics and depressive symptoms of older people: Local spatial analyses. Social Science & Medicine, 75(12), 2307–2316. DOI 10.1016/j.socscimed.2012.08.033. [Google Scholar] [CrossRef]
9. Ivey, S. L., Kealey, M., Kurtovich, E., Hunter, R. H., Prohaska, T. R. et al. (2014). Neighborhood characteristics and depressive symptoms in an older population. Aging & Mental Health, 19(8), 713–722. DOI 10.1080/13607863.2014.962006. [Google Scholar] [CrossRef]
10. Gecas, V. (1989). The social-psychology of self-efficacy. Annual Review of Sociology, 15(1), 291–316. DOI 10.1146/annurev.so.15.080189.001451. [Google Scholar] [CrossRef]
11. Haney, T. J. (2007). Broken windows and self-esteem: Subjective understandings of neighborhood poverty and disorder. Social Science Research, 36(3), 968–994. DOI 10.1016/j.ssresearch.2006.07.003. [Google Scholar] [CrossRef]
12. Wong, W. W., Mikhail, C., Ortiz, C. L., Lathan, D., Moore, L. A. et al. (2014). Body weight has no impact on self-esteem of minority children living in inner city, low-income neighborhoods: A cross-sectional study. BMC Pediatrics, 14(1), 483. DOI 10.1186/1471-2431-14-19. [Google Scholar] [CrossRef]
13. Ross, C. E., Mirowsky, J. (2008). Neighborhood socioeconomic status and health: Context or composition? City & Community, 7(2), 163–179. DOI 10.1111/j.1540-6040.2008.00251.x. [Google Scholar] [CrossRef]
14. Cohen, S., Wills, T. A. (1985). Stress, social support, and the buffering hypothesis. Psychological Bulletin, 98(2), 310–357. DOI 10.1037/0033-2909.98.2.310. [Google Scholar] [CrossRef]
15. Ross, C. E., Mirowsky, J. (2001). Neighborhood disadvantage, disorder, and health. Journal of Health and Social Behavior, 42(3), 258–276. DOI 10.2307/3090214. [Google Scholar] [CrossRef]
16. Wheaton, B., Clarke, P. (2003). Space meets time: Integrating temporal and contextual influences on mental health in early adulthood. American Sociological Review, 68(5), 680–706. DOI 10.2307/1519758. [Google Scholar] [CrossRef]
17. Boardman, J. D., Robert, S. A. (2000). Neighborhood socioeconomic status and perceptions of self-efficacy. Sociological Perspectives, 43(1), 117–136. DOI 10.2307/1389785. [Google Scholar] [CrossRef]
18. Rohe, W. M., Basolo, V. (2016). Long-term effects of homeownership on the self-perceptions and social interaction of low-income persons. Environment & Behavior, 29(6), 793–819. DOI 10.1177/0013916597296004. [Google Scholar] [CrossRef]
19. Baldwin, S. A., Hoffmann, J. P. (2002). The dynamics of self-esteem: A growth-curve analysis. Journal of Youth and Adolescence, 31(2), 101–113. DOI 10.1023/A:1014065825598. [Google Scholar] [CrossRef]
20. Greene, M. L., Way, N. (2005). Self-esteem trajectories among ethnic minority adolescents: A growth curve analysis of the patterns and predictors of change. Journal of Research on Adolescence, 15(2), 151–178. DOI 10.1111/j.1532-7795.2005.00090.x. [Google Scholar] [CrossRef]
21. Mead, G. H. (1934). Mind, self and society. Chicago: Chicago University Press. [Google Scholar]
22. Haney, T. (2007). “Broken windows” and self-esteem: Subjective understandings of neighborhood poverty and disorder. Social Science Research, 36(3), 968–994. DOI 10.1016/j.ssresearch.2006.07.003. [Google Scholar] [CrossRef]
23. Macintyre, S., Maciver, S., Soomans, A. (1993). Area, class and health: Should we be focusing on places or people? Journal of Social Policy, 22(2), 213–234. DOI 10.1017/S0047279400019310. [Google Scholar] [CrossRef]
24. Cutrona, C. E., Wallace, G., Wesner, K. A. (2006). Neighborhood characteristics and depression: An examination of stress processes. Current Directions in Psychological Science, 15(4), 188–192. DOI 10.1111/j.1467-8721.2006.00433.x. [Google Scholar] [CrossRef]
25. Aneshensel, C. S., Avison, W. R. (2015). The stress process. Society & Mental Health, 5(2), 67–85. DOI 10.1177/2156869315585388. [Google Scholar] [CrossRef]
26. Turner, J. R., Lloyd, D. A. (1999). The stress process and the social distribution of depression. Journal of Health & Social Behavior, 40(4), 374–404. DOI 10.2307/2676332. [Google Scholar] [CrossRef]
27. Kim, J., Ross, C. E. (2009). Neighborhood-specific and general social support: Which buffers the effect of neighborhood disorder on depression? Journal of Community Psychology, 37(6), 725–736. DOI 10.1002/jcop.20327. [Google Scholar] [CrossRef]
28. Ross, C. E., Jang, S. J. (2000). Neighborhood disorder, fear, and mistrust: The buffering role of social ties with neighbors. American Journal of Community Psychology, 28(4), 401–420. DOI 10.1023/A:1005137713332. [Google Scholar] [CrossRef]
29. Schieman, S., Meersman, S. C. (2004). Neighborhood problems and health among older adults: Received and donated social support and the sense of mastery as effect modifiers. Journals of Gerontology Series B-Psychological Sciences & Social Sciences, 59(2), S89–S97. DOI 10.1093/geronb/59.2.S89. [Google Scholar] [CrossRef]
30. Crowder, K., South, S. J. (2003). Neighborhood distress and school dropout: The variable significance of community context. Social Science Research, 32(4), 659–698. DOI 10.1016/S0049-089X(03)00035-8. [Google Scholar] [CrossRef]
31. Mayer, S. E., Jencks, C. (1989). Growing up in poor neighborhoods: How much does it matter? Science, 243(4897), 1441–1445. DOI 10.1126/science.243.4897.1441. [Google Scholar] [CrossRef]
32. Schieman, S., Pearlin, L. I. (2006). Neighborhood disadvantage, social comparisons, and the subjective assessment of ambient problems among older adults. Social Psychology Quarterly, 69(3), 253–269. DOI 10.1177/019027250606900303. [Google Scholar] [CrossRef]
33. Pound, P., Gompertz, P., Ebrahim, S. (1998). A patient-centered study of the consequences of stroke. Clinical Rehabilitation, 12(4), 338–347. DOI 10.1191/026921598677661555. [Google Scholar] [CrossRef]
34. Winkleby, M., Cubbin, C., Ahn, D. (2006). Effect of cross-level interaction between individual and neighborhood socioeconomic status on adult mortality rates. American Journal of Public Health, 96(12), 2145–2153. DOI 10.2105/AJPH.2004.060970. [Google Scholar] [CrossRef]
35. Weden, M. A., Carpiano, R. A., Robert, S. A. (2008). Subjective and objective neighborhood characteristics and adult health. Social Science & Medicine, 66(6), 1256–1270. DOI 10.1016/j.socscimed.2007.11.041. [Google Scholar] [CrossRef]
36. Hill, T. D., Burdette, A. M., Jokinen-Gordon, H. M., Brailsford, J. M. (2013). Neighborhood disorder, social support, and self-esteem: Evidence from a sample of low-income women living in three cities. City & Community, 12(4), 380–395. DOI 10.1111/cico.12044. [Google Scholar] [CrossRef]
37. Rosenberg, M. (1965). Society and the adolescent self-image. USA: Princeton University Press. [Google Scholar]
38. House, J. S. (2010). Americans’ changing lives: Waves I, II, III, and IV, 1986, 1989, 1994, and 2002. Inter-university Consortium for Political and Social Research (ICPSR) [distributor]. Ann Arbor. [Google Scholar]
39. Shaw, B. A., Liang, J., Krause, N. (2010). Age and race differences in the trajectories of self-esteem. Psychology & Aging, 25(1), 84–94. DOI 10.1037/a0018242. [Google Scholar] [CrossRef]
40. Falci, C. D. (2011). Self-esteem and mastery trajectories in high school by social class and gender. Social Science Research, 40(2), 586–601. DOI 10.1016/j.ssresearch.2010.12.013. [Google Scholar] [CrossRef]
41. Thoits P. A., Hewitt L. N. (2001). Volunteer work and well-being. Journal of Health & Social Behavior, 42(2), 115–131. DOI 10.2307/3090173. [Google Scholar] [CrossRef]
42. Robert, S. A. (1998). Community-level socioeconomic status effects on adult health. Journal of Health and Social Behavior, 39(1), 18–37. DOI 10.2307/2676387. [Google Scholar] [CrossRef]
43. Aneshensel, C. S., Ko, M. J., Chodosh, J., Wight, R. G. (2011). The urban neighborhood and cognitive functioning in late middle age. Journal of Health & Social Behavior, 52(2), 163–179. DOI 10.1177/0022146510393974. [Google Scholar] [CrossRef]
44. Ruel, E., Reither, E. N., Robert, S. A., Lantz, P. M. (2010). Neighborhood effects on BMI trends: Examining BMI trajectories for Black and White women. Health & Place, 16(2), 191–198. DOI 10.1016/j.healthplace.2009.09.009. [Google Scholar] [CrossRef]
45. Zimmerman, G. M., Messner, S. F. (2010). Neighborhood context and the gender gap in adolescent violent crime. American Sociological Review, 75(6), 958–980. DOI 10.1177/0003122410386688. [Google Scholar] [CrossRef]
46. Turner, J. R., Marino, F. (1994). Social support and social-structure—A descriptive epidemiology. Journal of Health & Social Behavior, 35(3), 193–212. DOI 10.2307/2137276. [Google Scholar] [CrossRef]
47. Thoits, P. A. (1995). Stress, coping, and social support processes—Where are we—What next. Journal of Health & Social Behavior, 35, 53–79. DOI 10.2307/2626957. [Google Scholar] [CrossRef]
48. Ross, C. E. (1989). Explaining the social patterns of depression—Control and problem-solving—Or support and talking. Journal of Health & Social Behavior, 30(2), 206–219. DOI 10.2307/2137014. [Google Scholar] [CrossRef]
49. Ross C. E., Mirowsky J. (2008). Neighborhood socioeconomic status and health: Context or composition? City & Community, 7(2), 163–179. DOI 10.1111/j.1540-6040.2008.00251.x. [Google Scholar] [CrossRef]
50. Ruel, E., Robert, S. A. (2009). A model of racial residential history and its association with self-rated health and mortality among black and white adults in the United States. Sociological Spectrum, 29(4), 443–466. DOI 10.1080/02732170902904616. [Google Scholar] [CrossRef]
51. Yao, L., Robert, S. A. (2011). Examining the racial crossover in mortality between African American and White older adults: A multilevel survival analysis of race, individual socioeconomic status, and neighborhood socioeconomic context. Journal of Aging Research, 2011, 132073. DOI 10.4061/2011/132073. [Google Scholar] [CrossRef]
52. Robert, S. A., Reither, E. N. (2004). A multilevel analysis of race, community disadvantage, and body mass index among adults in the US. Social Science & Medicine, 59(12), 2421–2434. DOI 10.1016/j.socscimed.2004.03.034. [Google Scholar] [CrossRef]
53. Oliver, E. J. (2016). Mental life and the metropolis in suburban America. Urban Affairs Review, 39(2), 228–253. DOI 10.1177/1078087403254445. [Google Scholar] [CrossRef]
54. Mirowsky, J., Ross, C. E. (2003). Education, social status, and health. USA: Aldine de Gruyter. [Google Scholar]
55. Latkin, C. A., Curry, A. D. (2003). Stressful neighborhoods and depression: A prospective study of the impact of neighborhood disorder. Journal of Health & Social Behavior, 44(1), 34–44. DOI 10.2307/1519814. [Google Scholar] [CrossRef]
56. Stockdale, S. E., Wells, K. B., Tang, L., Belin, T. R., Zhang, L. et al. (2007). The importance of social context: Neighborhood stressors, stress-buffering mechanisms, and alcohol, drug, and mental health disorders. Social Science & Medicine, 65(9), 1867–1881. DOI 10.1016/j.socscimed.2007.05.045. [Google Scholar] [CrossRef]
57. Dehle, C., Larsen, D., Landers, J. E. (2001). Social support in marriage. American Journal of Family Therapy, 29(4), 307–324. DOI 10.1080/01926180126500. [Google Scholar] [CrossRef]
58. Pasch, L. A., Bradbury, T. N. (1998). Social support, conflict, and the development of marital dysfunction. Journal of Consulting and Clinical Psychology, 66(2), 219–230. DOI 10.1037/0022-006X.66.2.219. [Google Scholar] [CrossRef]
59. Cherlin, A. (2010). The marriage-go-round: The state of marriage and the family in America today. USA: Vintage Books, Random House Division, Inc. [Google Scholar]
60. Caplan, G. (1981). Mastery of stress—Psychosocial-aspects. American Journal of Psychiatry, 138(4), 413–420. DOI 10.1176/ajp.138.4.413. [Google Scholar] [CrossRef]
61. Krause, N. (2006). Neighborhood deterioration, social skills, and social relationships in late life. International Journal of Aging & Human Development, 62(3), 185–207. DOI 10.2190/7PVL-3YA2-A3QC-9M0B. [Google Scholar] [CrossRef]
62. Aneshensel, C. S., Sucoff, C. A. (1996). The neighborhood context of adolescent mental health. Journal of Health & Social Behavior, 37(4), 293–310. DOI 10.2307/2137258. [Google Scholar] [CrossRef]
63. Hill, T. D., Ross, C. E., Angel, R. J. (2005). Neighborhood disorder, psychophysiological distress, and health. Journal of Health & Social Behavior, 46(2), 170–186. DOI 10.1177/002214650504600204. [Google Scholar] [CrossRef]
64. House, J. S., Lepkowski, J. M., Kinney, A. M., Mero, R. P., Kessler, R. C. et al. (1994). The social stratification of aging and health. Journal of Health & Social Behavior, 35(3), 213–234. DOI 10.2307/2137277. [Google Scholar] [CrossRef]
65. Link, B. G., Phelan, J. (1995). Social conditions as fundamental causes of disease. Journal of Health and Social Behavior, 35, 80–94. DOI 10.2307/2626958. [Google Scholar] [CrossRef]
66. Lutfey, K., Freese, J. (2005). Toward some fundamentals of fundamental causality: Socioeconomic status and health in the routine clinic visit for diabetes. American Journal of Sociology, 110(5), 1326–1372. DOI 10.1086/428914. [Google Scholar] [CrossRef]
67. Adler, N. E., Newman, K. (2002). Socioeconomic disparities in health: Pathways and policies. Health Affairs, 21(2), 60–76. DOI 10.1377/hlthaff.21.2.60. [Google Scholar] [CrossRef]
68. Lantz, P. M., Lynch, J. W., House, J. S., Lepkowski, J. M., Mero, R. P. et al. (2001). Socioeconomic disparities in health change in a longitudinal study of US adults: The role of health-risk behaviors. Social Science & Medicine, 53(1), 29–40. DOI 10.1016/S0277-9536(00)00319-1. [Google Scholar] [CrossRef]
69. Sharkey, P., Faber, J. W. (2014). Where, when, why, and for whom do residential contexts matter? Moving away from the dichotomous understanding of neighborhood effects. Annual Review of Sociology, 40(1), 559–579. DOI 10.1146/annurev-soc-071913-043350. [Google Scholar] [CrossRef]
70. Sampson, R. J., Raudenbush, S. W. (1999). Systematic social observation of public spaces: A new look at disorder in urban neighborhoods. American Journal of Sociology, 105(3), 603–651. DOI 10.1086/210356. [Google Scholar] [CrossRef]
71. Bosma, H., Dike van de Mheen, H., Borsboom, G. J., Mackenbach, J. P. (2001). Neighborhood socioeconomic status and all-cause mortality. American Journal of Epidemiology, 153(4), 363–371. DOI 10.1093/aje/153.4.363. [Google Scholar] [CrossRef]
72. Robins, R. W., Trzesniewski, K. H., Tracy, J. L., Gosling, S. D., Potter, J. (2002). Global self-esteem across the life span. Psychology & Aging, 17(3), 423–434. DOI 10.1037/0882-7974.17.3.423. [Google Scholar] [CrossRef]
73. Szinovacz, M. E., Davey, A. (2008). Introduction: Caregiving in context. In: Oermann, M. H., Heinrich, K. T. (Eds.Annual review of nursing education, 6. New York: Springer. [Google Scholar]
74. Cantor, H. (1979). Neighbors and friends: An overlooked resource in the informal support system. Research on Aging, 1, 434–463. DOI 10.1177/016402757914002. [Google Scholar] [CrossRef]
75. Vasunilashorn, S., Steinman, B. A., Liebig, P. S., Pynoos, J. (2012). Aging in place: Evolution of a research topic whose time has come. Journal of Aging Research, 2012, 1–6. DOI 10.1155/2012/120952. [Google Scholar] [CrossRef]
76. Seltzer, J. A. (2019). Family change and changing family demography. Demography, 56(2), 405–426. DOI 10.1007/s13524-019-00766-6. [Google Scholar] [CrossRef]
77. Blackstone, A. (2014). Childless… or Childfree? Contexts, 13(4), 68–70. DOI 10.1177/1536504214558221. [Google Scholar] [CrossRef]
78. Smith, K. P., Nicholas, A. C. (2008). Social networks and health. Annual Review of Sociology, 34(1), 405–429. DOI 10.1146/annurev.soc.34.040507.134601. [Google Scholar] [CrossRef]
 | This work is licensed under a Creative Commons Attribution 4.0 International License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. |