| International Journal of Mental Health Promotion |
DOI: 10.32604/ijmhp.2022.018030
ARTICLE
Mental Health Literacy of University Students in Vietnam and Cambodia
1Hamburg University of Applied Sciences, Department of Social Work, Hamburg, Germany
2VNU University of Education, Center for Research, Information and Service in Psychology (CRISP), Hanoi, Vietnam
3Thai Nguyen University of Agriculture and Forestry, Advanced Education Programs Office, Thai Nguyen City, Vietnam
4VNU-HCM University of Social Sciences and Humanities, Faculty of Education, Ho Chi Minh City, Vietnam
5Thai Nguyen University of Economics and Business Administration, Faculty of Economics, Thai Nguyen City, Vietnam
6Vinh University of Technology Education, Department of Scientific Management and International Partnerships, Vinh City, Vietnam
7Paragon International University, Department of Business Administration, Phnom Penh, Cambodia
*Corresponding Author: Gunter Groen. Email: gunter.groen@haw-hamburg.de
Received: 07 July 2021; Accepted: 04 November 2021
Abstract: Mental health literacy (MHL) refers to knowledge and attitudes that shape the recognition, management, and prevention of mental disorders. While the topic has been exhaustively researched in Western countries, research from Southeast Asia still is limited. Previous studies in this field showed a moderate recognition of mental disorders, a high prevalence of stigmatizing attitudes and a low willingness to seek professional help among Southeastern-Asian populations. This study explored the level of MHL among university students from different parts of Vietnam and Cambodia. Correlations with influencing factors (gender, age, study year, educational attainment of the parents, urban/rural origin, ethnicity, personal experiences with mental disorders) were also explored. An online survey, using a 30-item Vietnamese version of the Mental Health Literacy Scale (MHLS), was conducted at six university sites in Vietnam and Cambodia. Data of 1032 students from different study branches were included. The MHL of Vietnamese and Cambodian university students was lower, compared to samples from Australia or the UK. Females and students with a personal experience of mental disorders (self or family) showed a significantly higher MHL. No differences in MHL were found between students from different socioeconomic backgrounds (professional attainment of parents, urban/rural origin). Findings on the influence of ethnicity were inconclusive. MHL needs to be improved among the university students of Vietnam and Cambodia. Mental health promotion should specifically target male students, students from STEM branches, and international students.
Keywords: Help-seeking; mental disorders; mental health literacy; Southeastern Asia; stigma; university students
Globally, student mental health has become increasingly important. Results from the recent WHO World Mental Health Surveys International College Student (WMH-ICS) Project revealed a high prevalence of mental health problems among first-year college students from 19 colleges in eight different countries [1]. 35% scored positive for at least one lifetime mental disorder and 31% for at least one 12-month disorder. A lower prevalence (20.3%) was reported from the WHO WMH Surveys two years before [2]. This was conducted in a wider range of countries, including low- and middle-income countries (LMIC). Generally, severe mental health problems go along with role impairment in different areas of life. According to data from the WMH-ICS Project, around 43% of the students with at least one mental disorder reported severe role impairment, regarding work or academic success, home management, close personal relationships, or social life [3]. In most university settings, the mental health needs of students exceed the available resources.
Entering higher education is a critical point in life, not only in terms of personal development, orientation, and adjustment to a new environment but also regarding high academic demands. Additional financial problems or personal problems with family or peers may contribute to feelings of crisis, isolation, and self-doubt and thus impede academic performance [4–6]. Recent research indicates adverse effects of the COVID-19 pandemic on student mental health, specifically on anxiety [7,8]. Compared to the general population, students seem to be more vulnerable [9]. School and university closures, problems with remote learning, cancellation of social events, and precarious future career possibilities can lead to feelings of isolation and crisis and intensify emotional distress.
Higher education does not only present a challenge and a risk but it is also a chance for health promotion among young people. Based on the “Ottawa Charter for Health Promotion” [10] and the “Healthy Settings” approach [11], WHO developed a framework for Health Promoting Universities as early as 1998 [12]. The core idea is to embed health and well-being in all campus policies and to create a supportive environment that enhances the personal development of students and staff [13]. However, there are large differences in how this approach is understood and implemented [14,15]. The ASEAN University Network (AUN) was established in 2014. Despite mental health is an integral part of student health and well-being, which is explicitly mentioned in the AUN Healthy University Framework [16], the awareness for mental health at ASEAN universities is still comparatively low. Recognizing mental health problems, knowing when and where to seek help, and attitudes that hinder or facilitate help-seeking for mental health problems are subsumed under the term “mental health literacy”.
The concept of mental health literacy (MHL) was first described by Jorm et al. [17] and builds upon the concept of health literacy [18]. Components of MHL include (a) the ability to recognize specific disorders or psychological distress; (b) knowledge and beliefs about risk factors and causes; (c) knowledge and beliefs about self-help interventions; (d) knowledge and beliefs about professional help available; (e) attitudes which facilitate recognition and help-seeking; (f) knowledge of how to seek mental health information [19]. A more recent definition by Kutcher et al. [20] defines MHL as understanding how to obtain and maintain good mental health; understanding mental disorders and their treatment; decreasing stigma related to mental disorders; enhancing help-seeking efficacy. MHL constitutes an important general aim for prevention strategies and can also be seen as an indicator of existing awareness and education regarding mental health.
There is evidence from Australia, Europe, and the United States that MHL can be improved among young people via school- or university-based interventions [21]. Increasing MHL among young people is of utter importance. As young people tend to have more negative attitudes towards mental illness and are often reluctant to turn to adults for help, there is a high chance that mental health problems go unrecognized and undiagnosed in this age group. Non-recognition of mental health problems leads to severe delays in treatment [21,22].
First research on the MHL of students was predominantly conducted in Australia [23–27], in the UK and other high-income European countries [28–32] and also the United States [33,34]. In recent years, the topic gained in importance. Today, also research from non-western countries and LMIC can be found: e.g., Turkey [35], Sri Lanka [36], Saudi Arabia [37], the Caribean Islands [38], and also Southeast Asia [39–44].
1.2 Findings from Southeast Asia
Southeast-Asian studies focused on depression literacy [40,42,43], MHL of eating disorders [39], and MHL among international students [44]. One study compared perceptions of mental health and attitudes towards help-seeking between Vietnamese and US students [41] and reported higher rates of stigma and more negative attitudes towards people with a mental illness from the Vietnamese students. Khan et al. [42] found a moderate level of knowledge on depression, but an only cursory knowledge of treatment options among students in Malaysia. Among Vietnamese students, studied by Nguyen Thai and Nguyen et al. [43], 32% correctly labeled depression and more than 80% indicated that they would seek help for this condition. Ibrahim et al. [40] compared depression literacy and help-seeking attitudes between university and secondary school students from low-income households in Malaysia. They found a higher depression literacy, lower levels of self-stigma, and fewer negative beliefs towards mental illness among the university students, leading to more positive attitudes towards help-seeking. Salloum et al. [44] employed the Mental Health Literacy Scale (MHLS) among international postgraduate students in Malaysia and found a lower MHL, compared to UK or Australian samples which is in line with findings from cross-cultural research [22].
This study employs a Vietnamese version of the Mental Health Literacy Scale (MHLS) to understand the current knowledge on mental health and related perceptions and attitudes among university students in Cambodia and Vietnam. Additionally, correlations with demographic data and study-related factors will be explored. Our hypothesis is to find lower scores of mental health literacy, compared to Australian and UK samples. A second hypothesis is that the MHL of students will be influenced by gender, age, study branch, and history of mental illness. To our knowledge, there has not been a study exploring mental health literacy in student populations from different parts of Vietnam and Cambodia. Based on these results, an intervention for increasing mental health awareness and reducing stigma among university students and staff shall be developed in cooperation with partner universities in the above-named countries.
The study was conducted as an online survey in six different universities in Vietnam and Cambodia between July and October 2020. Universities from different scientific fields were included (Social Sciences and Humanities, Education, Technology, Economics, Agriculture). The participating Vietnamese universities were geographically diversified, spreading from the north to the south of Vietnam. Students were invited to participate via email, the university website, or through an in-class invitation. All universities shared the invitation between three or more faculties, using convenient sampling. We aimed at a sample size of 150 students per university.
Mental health literacy was measured by an adapted version of the Mental Health Literacy Scale (MHLS) of O’Connor et al. [25]. The scale has excellent psychometric properties concerning mental health knowledge and also help-seeking [45,46]. It was translated and culturally adapted for Vietnam by Dang et al. [47] for use in school settings. In contrast to the original version, two items regarding gender-related risks and two items on professional confidentiality were omitted in the Vietnamese version. In Cambodia, the same 31-item version was used in the English language. The adapted version contained 8 items on recognition of mental disorders, 7 items on knowledge of self-help, professional help, and information-seeking, 9 items on attitudes that inhibit the recognition of mental disorders and appropriate help-seeking, and 7 items on the willingness to interact with people who suffer from a mental disorder. Items are rated on a 5-point Likert scale, ranging from “very likely” to “very unlikely” for recognition of disorders, from “strongly agree” to “strongly disagree” for knowledge on help-seeking and attitudes, and from “definitely willing” to “definitely unwilling” for questions on the willingness to interact.
Demographic data on age, gender, study program, study year, ethnic group, educational background of the parents, population of the hometown, and experiences with mental health problems were also collected.
Data were analyzed at Hamburg University of Applied Sciences (HAW), using IBM SPSS Statistics, Version 26. There were 1041 responses altogether. Responses with 8 or more missing answers were deleted, leaving 1032 responses for evaluation. Inverse items were recoded and missings were replaced by using the variable mean. The total means and mean scores of the four subscales (recognition, knowledge, attitudes, openness) were calculated. The internal consistency (Cronbach’s Alpha) was very good for three of the subscales (recognition: 0.867, attitudes: 0.845, openness: 0.884), and sufficient for knowledge (0.649). After exclusion of the knowledge item on managing emotions (avoid all activities or situations that made them feel anxious), the internal consistency of the knowledge subscale was 0.813. This led to a 30-item scale, with a possible MHL score of 30 to 150. Scores of the 30-item scale were normally distributed (Shapiro-Wilk test statistics: p = 0.250).
While the original version of O’Connor & Casey uses a 4-point Likert scale for the first 15 questions and a 5-point Likert scale for the next 20 questions, the Vietnamese version uses a 5-point Likert scale for the whole questionnaire. For comparing scores to the Australian sample of O’Connor et al. and other samples from literature, an adjusted total score was calculated.
Total scores and mean scores of the subscales were compared between men and women, older and younger students, students of different study years, and students with and without a personal experience of mental health problems, using t-test. Because several independent t-tests were conducted (n = 5), we used the Bonferroni correction to control for α errors. This led to a significance level of 0.01. ANOVA was used to compare the scores of students from different socioeconomic backgrounds (educational attainment of parents and population of the district where raised) and ethnicities. For technical reasons, it was not possible to merge the data on ethnic affiliation from the different samples. Therefore, this was evaluated separately for each of the university samples. For the different independent factors, effect sizes (Cohen’s d) were calculated.
Ethical approval was obtained from the Ethical Committee of Competence Center Health at Hamburg University of Applied Sciences. Each participating researcher signed a confidentiality declaration. Consent to participate was requested in the first question of the online survey.
3.1 Setting and Study Population
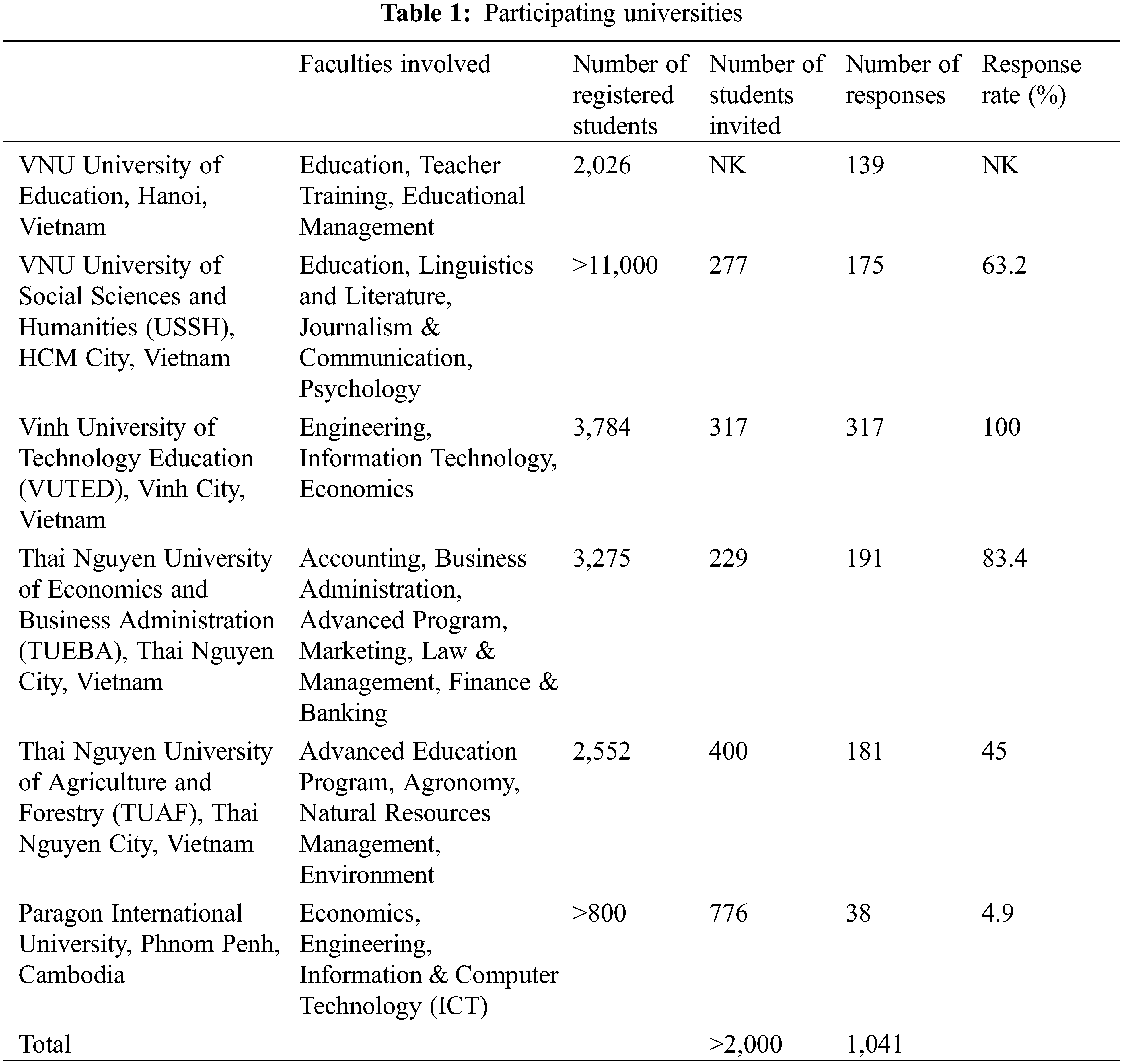
From the six Asian Universities who collaborated in this study, five were from Vietnam, and one from Cambodia, see Table 1. Participating faculties ranged from Education, Humanities, Economics and Business Administration to Agriculture, Engineering and Information & Computer Technology (ICT). In total, there were 1041 responses from more than 2000 students who were invited to take part in the survey. The response rate ranged between 45% and 100% in Vietnamese universities and was around 5% in the Cambodian university. The number of responses aimed at was reached (+/−10 %) by all but one university.
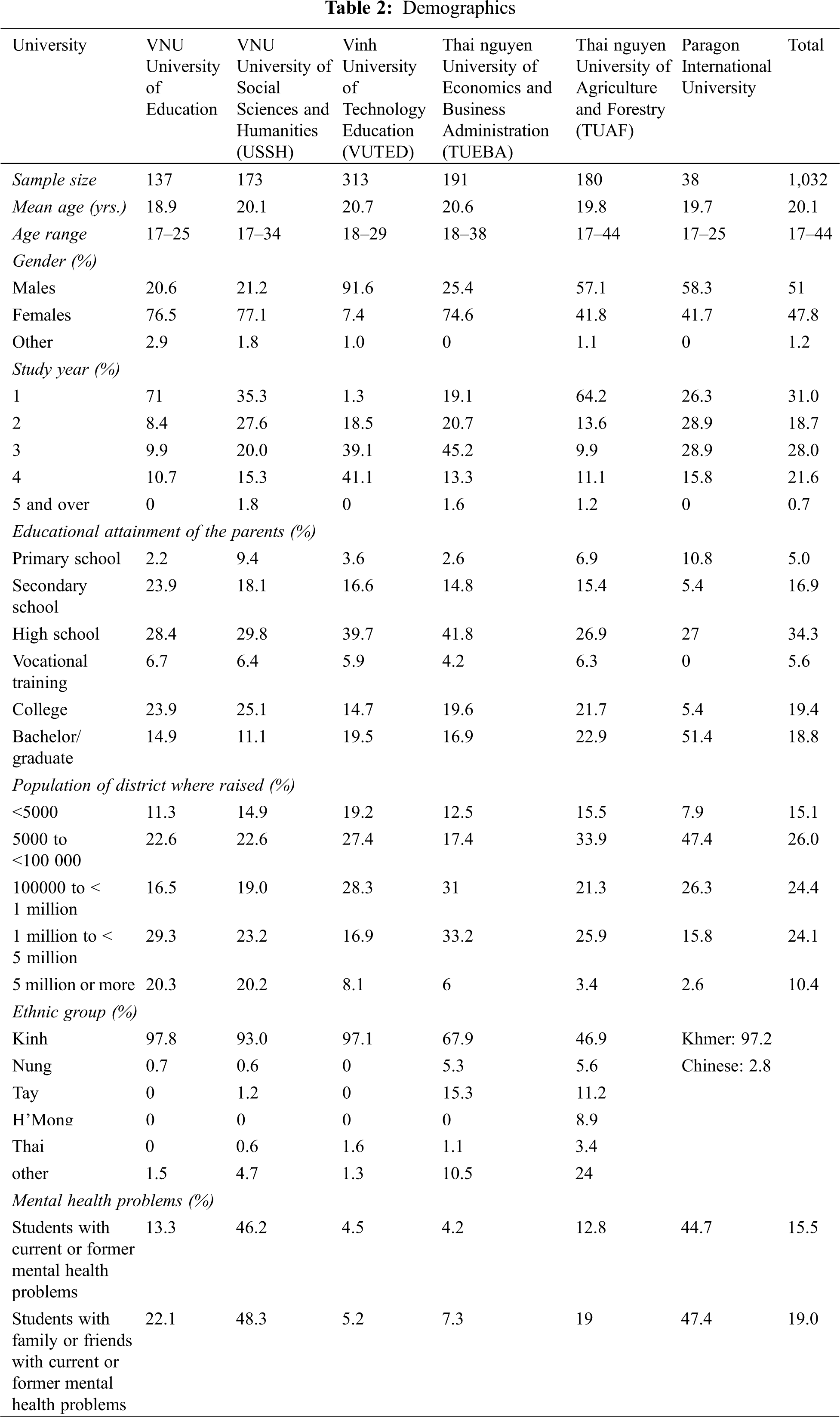
The mean age of the study participants was 20.1 years (range: 17–44), see Table 2. Gender distribution varied, with 91.6% male respondents at VUTED and around 75% female respondents at three other universities. The mean gender distribution was almost even, with 51% males and 47.8% females. The majority of Vietnamese students were of Kinh ethnicity, while students from Cambodia were predominately Khmer. One-third of study participants were in their first year of studies. Around 34% of the student’s parents had completed high school, while 40% had also completed college or university. 15.5% of students disclosed current or former mental health problems (range 4.2%–46.2%), and 19.0% had family or friends with current or former mental health problems (range 7.3%–48.3%).
The MHL score of the total sample (n = 1032) was 96.9 (SD = 13.1; range: 47–140). The adjusted total score for comparison with other samples was 108.13 (SD 19.43).
3.2.1 Recognition of Mental Disorders
Between 22.7% and 47.3% of students recognized mental disorders, by rating a true description of the disorder as “very likely” or “likely”. Recognition was lowest for social phobia (22.7%). Agoraphobia, general anxiety disorder, major depressive disorder, and bipolar disorder were recognized by around one-third of participants. A higher percentage of students recognized dysthymia (38%) and drug dependency (41.4%). 47.3% of students could identify personality disorder as a category of mental illness. Regarding self-help and professional treatment, 45% of students considered it helpful to improve their quality of sleep in times of anxiety or depression. 34.9% knew that Cognitive Behavior Therapy (CBT) was a therapy based on challenging negative thoughts and increasing helpful behaviors.
3.2.2 Knowledge on Help-Seeking Resources
Around half of the students were confident about seeking information on mental illness. 45% indicated that they knew where to seek information, by choosing “agree” or “strongly agree”. The confidence of using a computer or telephone for information-seeking was higher (61.4%), compared to using face-to-face appointments (54.5%). 61% were confident that they could access resources for mental health information.
3.2.3 Stigmatizing Attitudes and Openness
The highest scores were attained in the attitudes subscale (mean score per item 3.57) on attitudes that facilitate or inhibit the recognition of disorders and the willingness to engage in help-seeking behavior. Higher scores in this subscale indicated disagreement with stigmatizing attitudes while lower scores indicated agreement. The highest agreement was found with the statement that people with a mental illness could snap out of it if they wanted to (30.8%). 40% of students were not sure how to rate the statement on dangerousness (item 6.4). On the other hand, around two-thirds of the participants disagreed to the statement that treatment would not being effective (item 6.9) and that it was best to avoid mentally ill people (item 6.5), see Table 3.
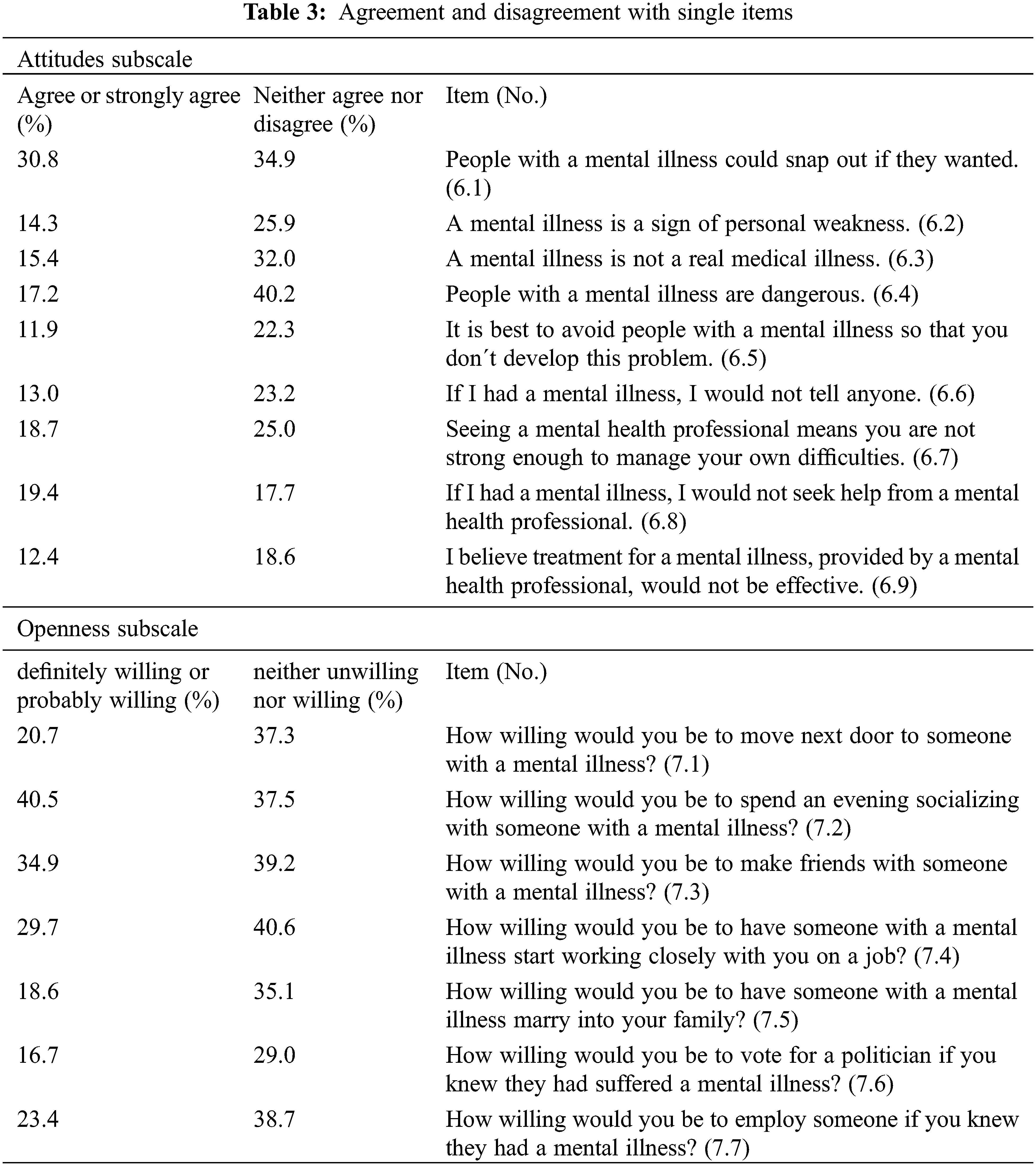
The lowest scores were found in the openness subscale (mean score per item 2.84) that assesses the willingness to interact with people who are suffering from a mental disorder. Only 16.7% indicated their willingness to vote for a politician who had suffered a mental disorder. 18.6% would be willing to have someone with a mental disorder marry into their family. 20.7% would be willing to move next door to someone with a mental illness. A high percentage of students (35%–40%) chose “neither unwilling nor willing” for items from this subscale, indicating a difficulty to decide. The only exception was item 7.6 (vote for a politician who had suffered a mental illness) where the majority of students indicated their unwillingness to do so.
3.2.4 Associations with Demographic Variables
Using ANOVA, there was a significant effect of gender at the p < 0.01 level [F(2, 2011) = 43.44, p < 0.001] between the three groups. Post-hoc analysis using Bonferroni comparison showed that this was only attributable to the difference between males and females (p < 0.001). Further analysis was done by t-test, comparing males and females. Females had a higher total mean score, compared to males, t(1000) = –9.3, p = < 0.001) and also higher mean scores in three of the subscales, see Tables 4 and 5. For openness, the difference between males and females was non-significant, t(1000) = –2.39, p < 0.017. Cohen’s effect size (d = 0.57) suggested an overall moderate effect of gender.
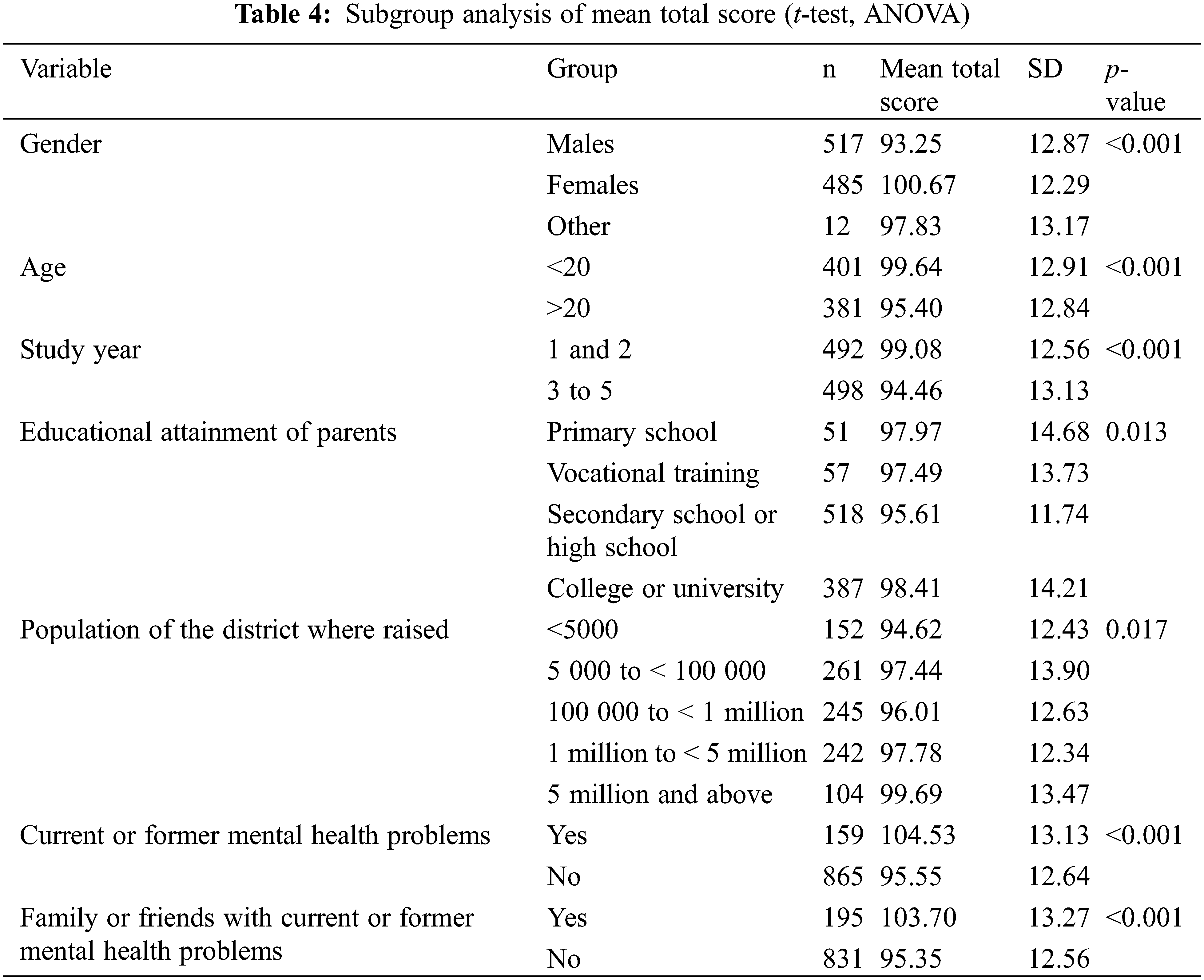
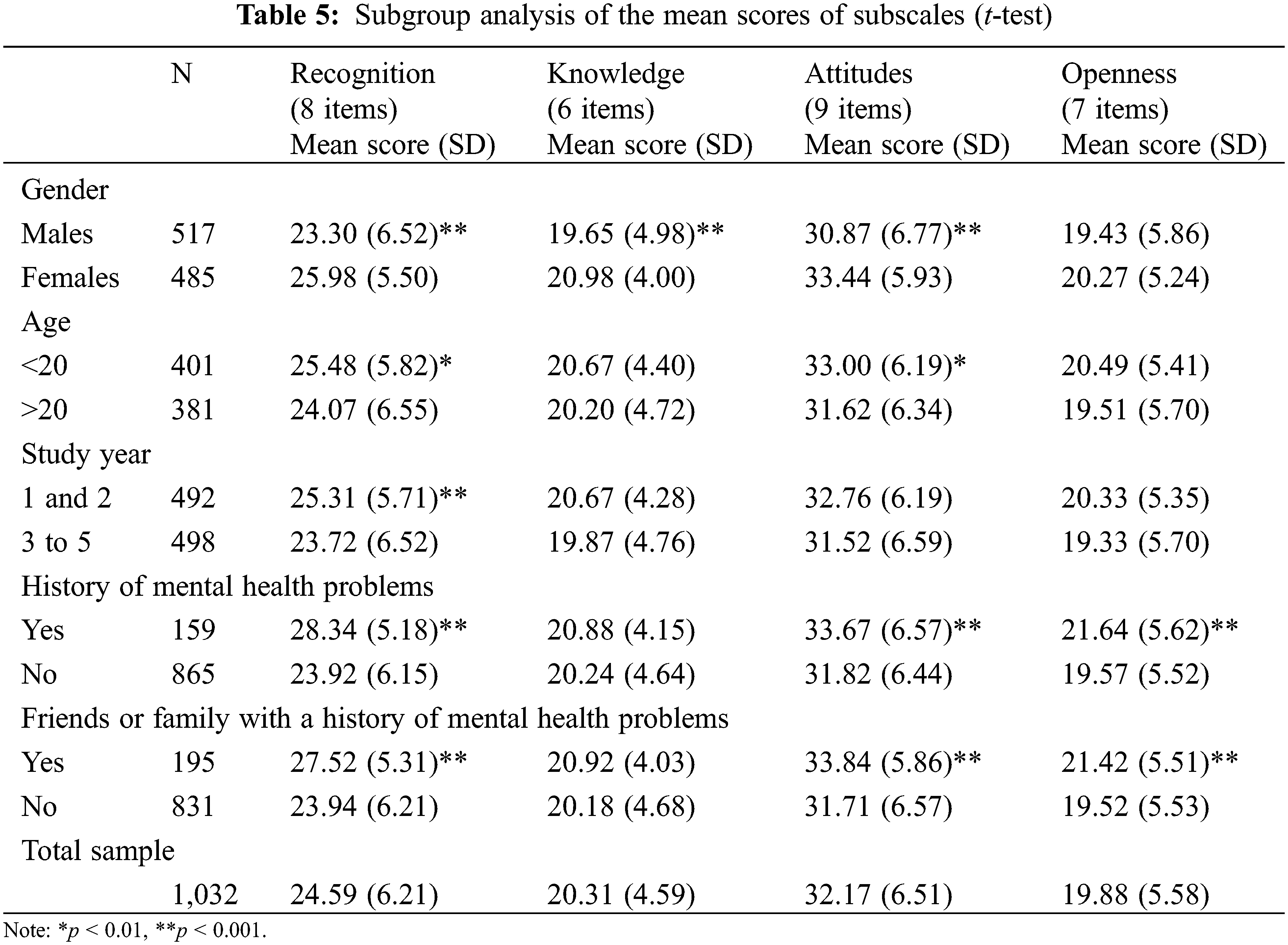
Using a median split, age was significantly associated with mental health literacy, with younger students under the age of 20 having a higher mean score, compared to students aged 21 and above; t(780) = 4.61, p < 0.001. The difference was also significant in two of the subscales, recognition of mental disorders and attitudes, see Tables 4 and 5. Study year was significantly associated with mental health literacy, with year-1 and year-2 students having a higher mean score, compared to more advanced students; t(988) = 5.66, p < 0.001. The difference was only significant in the recognition subscale. Cohen’s effect size indicated a small to moderate effect of age (d = 0.34) and study year (d = 0.35) on the MHL of students.
Students with current or former mental health problems had a higher MHL, compared to students who never had mental health problems; t(1022) = 8.2, p < 0.001. This was true for all of the subscales, except for knowledge on self-treatment, knowledge on professional help and knowledge where to seek information, t(1022) = 1.64, p = 0.101, see Tables 4 and 5. Likewise, students with friends or family members with current or former mental health problems had higher MHL scores, compared to students without; t(1024) = 8.28, p < 0.001. This was true for all of the subscales, except knowledge, t(329) = 2.26, p = 0.024. Cohen’s d (0.68 for personal mental health problems, 0.64 for family mental health problems) suggested a moderate to large effect on MHL.
For comparison with other samples, an adjusted total score was calculated, which was 114.36 (SD 18.04) for students with mental health problems and 113.39 (SD 17.86) for students with friends or family members with mental health problems. Analysis of variance showed no significant effect of the educational attainment of the parents on mental health literacy of the students on the p < 0.01 level [F(3, 1009) = 3.60, p = 0.013]. Likewise, the environment where the students were raised was not significantly associated with mental health literacy [F(4, 999) = 3.04, p = 0.017], see Table 4.
Due to technical reasons, ethnicity could only be evaluated for each of the university samples separately. In three of the samples, more than 97% of respondents belonged to the ethnic majority (Kinh in Vietnam, Khmer in Cambodia), so that statistical comparisons were inappropriate. In two of the other three samples, there was no statistically significant difference in MHL found between the different ethnic groups [F(4, 166) = 0.80, p = 0.525; F(4, 185) = 0.49, p = 0.742]. In the most ethnically diverse university sample, differences between ethnic groups were significant on the 0.05 level [F(5, 173) = 6.58, p < 0.001], with students of Kinh ethnicity (46.9%) having a lower mean score (M = 91.65, SD = 11.52), compared to students of other ethnicities (other than Kinh, Nung, Tay, H’Mong or Thai; M = 104.19, SD = 13.42) who represented 24% of the students. Cohen’s effect size (f = 0.44) indicated a strong effect of ethnicity on the MHL of the students at this study site.
Comparing the total mean scores of the different university samples in Vietnam, students from Education or Social Sciences and Humanities had a higher MHL, compared to students from Technology, Economics, or Agriculture. This was mainly due to higher scores in the recognition subscale. Also, scores in the attitudes subscale, indicating the absence of stigmatizing attitudes, were slightly higher among students from educational or social sciences.
This study aimed at understanding the current knowledge on mental health and related attitudes among university students in Cambodia and Vietnam. To the best of our knowledge, this was the first study to obtain levels of MHL from a wide range of Vietnamese students and the first study to explore Cambodian university students on the level of MHL. The findings showed that students from Vietnamese and Cambodian universities had a lower level of MHL (108.13), compared to students from the UK (122.88; 123.50) [30,31] or Australia , (127.38) [25]. However, when compared to the Southeast-Asian sample of Salloum et al. [44] or other Vietnamese samples [43,47], the level of MHL among participating students was in the same range.
4.1 Recognition of Mental Disorders and Help-Seeking Intentions
Among the eight mental health problems presented in the MHLS, social phobia was the least often recognized. A higher percentage of students recognized other anxiety disorders, depressive disorders, bipolar disorder, and drug dependency. Concerning the low rate of recognition of social phobia, the findings in this study are consistent with other research [48,49]. Although social anxiety disorders are amongst the most common mental disorders globally [50], MHL on social anxiety among various populations was low [51]. Among laypeople, social anxiety is often confused with shyness, as a personality trait but not a medical condition [52]. According to the review of Furnham et al. [53], recognition of disorders among the general population of non-western countries varied, with high rates of recognition for depression and schizophrenia and remarkably lower rates for eating disorders, social phobia, and personality disorders. A study among Vietnamese students that used case vignettes found a similar rate of depression recognition (32%) as reported from our study sample [54]. Studies from Australia, the USA and the UK reported comparably higher rates of disorder recognition (up to 86%) among students and young people [26,33,55].
The ability to recognize mental disorders has implications for help-seeking. Correct recognition of depression was positively correlated with the recommendation to seek professional help among different student populations [33,36]. Nguyen Thai et al. [43] found that only 26% of the Vietnamese students correctly identified depression and showed appropriate help-seeking intentions. However, it must be considered that there is a difference between recommending treatment for a hypothetical situation and seeking professional treatment for an existing mental health condition. A study among nursing students in Thailand revealed low intentions to seek help for mental health problems despite positive attitudes towards help-seeking [56]. Beliefs about approval or disapproval of others (subjective norms) were another significant factor that shaped the help-seeking intentions in this study population.
Finally, psychological symptoms seem to influence MHL in a way that people who are actually in need of professional help are less likely to recognize mental health symptoms and to seek treatment. Kim et al. [33] found that students who showed symptoms of depression or significant psychological distress were less likely to recognize depression in a case vignette and also less likely to recommend help-seeking, compared to students without mental health problems. Shi et al. [57] reported similar findings from students in Singapore and Hong Kong: Young Asian adults had overall low intentions to seek help for mental health problems. Students with worse mental health conditions were more reluctant to seek help and had less favorable attitudes towards counseling, compared to students with better mental health.
4.2 Knowledge and Attitudes towards Self-Help and Treatment
Regarding knowledge on self-help and professional treatment, around 45% of the students in our study recommended improving the quality of sleep in times of mental health difficulties and 35% knew what Cognitive Behavior Therapy (CBT) was about. A study among non-medical students in Malaysia found that less than one-third recommended the use of antidepressants for depression treatment, while 20% recommended alternative medicines [42]. However, the majority of students recommended consulting a psychiatrist or general practitioner (GP). Nguyen Thai et al. [43] found that professional help (counselor or psychologist) and informal help through a close family member or friend were equally recommended by Vietnamese students. Fewer students recommended consulting a psychiatrist or a GP and around 22% thought it would be best to deal with the problem (depression) on one’s own. Beliefs that standard psychiatric treatment and medication are rather harmful than helpful are widespread in the general population, although these attitudes have slowly changed in developed countries in recent years [17,19,21,22,58]. Reluctance to take up medical treatment causes significant a delay of effective therapies and bears the risk of chronification which is particularly problematic where young people are concerned.
4.3 Attitudes towards Mental Disorders
Stigmatizing attitudes prevalent among the participating students were that people with a mental illness could snap out of it if they wanted to or that mental illness was not a real medical illness. Another negative attitude endorsed by the students was that mental illness and/or seeing a mental health professional was a sign of personal weakness. 19% of students indicated that they would not seek help from a mental health professional, even if suffering from a mental illness. 17% of students agreed to the statement that mentally ill people were dangerous and 40% could neither agree nor disagree. Only a minority of students would be willing to vote for a politician who had suffered a mental illness or to have someone with a mental illness marrying into their family. This aligns with the finding of Kamimura et al. [41], that Vietnamese students were more likely to perceive mentally ill people as dangerous, while students from the USA thought mental illness to be an illness like any other illness. Van der Ham et al. [54] evaluated the attitudes towards mental disorders, compared to a medical illness (diabetes) among adults in urban Vietnam. They found more positive attitudes towards people with diabetes, compared to people with mental disorders. Negative attitudes and stigma are still important issues that may hinder help-seeking in Southeast-Asian settings, including university settings [40,41].
4.4 Factors Influencing Mental Health Literacy
Our data showed moderate effects of gender and personal experiences with mental disorders on the MHL of students and small effects of age and study year while the educational attainment of the parents and urban/rural origin did not have significant effects on the MHL of students. Regarding gender variation, female participants in this study exhibited significantly higher levels of MHL in the three dimensions recognition, help-seeking knowledge, and attitudes. This is in line with previous studies, where females often presented a higher MHL [22,26,30,33,53,55]. This tendency appears to be consistent across studies that used different MHL measures. One possible explanation is that the gender variation is linked to female socialization that encourages females to be more caring, sensitive, and alert to emotions and feelings [59]. However, in this study, gender was not a significant factor regarding “openness”, indicating that both, males and females, have the same level of willingness to interact (e.g., making friends, socializing, working) with people with mental health. Regarding the MHL of male university students, a low overall MHL, limited mental health knowledge, negative mental health beliefs and attitudes, high self-stigma, and low intentions to seek professional help were reported from university students in the USA [34]. This was even more pronounced among the students from STEM majors (Science, Technology, Engineering, and Mathematics). The review of Furnham et al. [22] likewise showed that men had more difficulties in identifying mental health symptoms and that they were more likely to recommend self-help instead of professional treatment.
Having personal experiences with mental health disorders was the other factor that had a moderate effect on MHL. Students with an experience of mental health disorders (having mental health problems by themselves or having family/friends with mental health problems) showed significantly higher levels of MHL. This was true for all of the subscales, except help-seeking knowledge. This difference is consistent with the current literature in Western countries and Vietnam [25,31,43,44,60]. The indifference in help-seeking knowledge between the two groups may reflect the fact that the mental health infrastructure in Vietnam and Cambodia is still very limited and scarce, especially in provinces [61,62]. Generally, reliable information on the mental health providers regarding their qualifications and the kind of treatment provided is difficult to find which also impedes access to treatment.
Age and study year had a small effect on the MHL in the way that younger students and year 1 and 2 students had a higher MHL, compared to older and more advanced students. These results are surprising, given the fact that knowledge should increase during studying. One possible explanation is that the finding may be an artifact, because the younger students in our study were predominantly from Educational and Social Sciences, while a higher percentage of older study participants studied Technology or Economics. Our data suggested differences across the study branches. Students from Educational or Social Sciences and Humanities had a higher MHL, compared to students from Technology, Economics, or Agriculture. Also, scores in the attitudes subscale which indicates the absence of stigmatizing attitudes were slightly higher among students from Educational or Social Sciences, compared to the students from other study branches. Differences in MHL between students of different study branches were also found by previous studies [32,34,63]. A possible explanation is that students who selected Education or Social Sciences as their major are interested in these topics and are more open which is reflected in higher MHL. Furthermore, classes such as “Introduction to Psychology” are compulsory in universities of Social Sciences or Education in Vietnam. Students from these branches could be trained for peer support as a measure of capacity building for mental health. For example, Mental Health First Aid is an approach that has been proven effective among various populations [64,65]. The vast majority of the Vietnamese students in the sample of Nguyen Thai et al. [43] thought First Aid Support (listening to others, encouraging physical activity, suggesting professional help) to be helpful and self-help interventions (learning how to relax, becoming more physically active, seeking information about the problem) were equally positively rated.
Our data did not support an effect of rural/urban origin on the MHL of students, although there is evidence from other research for a higher MHL among urban populations [53].
When discussing MHL in Southeast Asia, it must be noted that “mental health literacy” is a Western concept that may offend traditional conceptions of what causes and heals mental illness. Beliefs in supernatural or religious causes of mental illness will influence attitudes towards mentally ill people and the acceptance or non-acceptance of professional mental health treatment [21,53]. For example, van der Ham et al. [54] reported a mix of traditional and modern views from adults in Vietnam: Stress/tension or studying or thinking too much were the most often mentioned causes of mental illness while conflicts or internal emotional problems were less often mentioned. In their review on MHL, Furnham et al. [22] emphasize that mental disorders are differently defined and understood. Cross-cultural research shows that MHL is higher in developed countries, particularly the recognition of mental disorders. People from non-western or developing countries are more likely to somatize symptoms and to attribute their problems to a physical illness. Furthermore, people from non-western countries perceive other barriers in accessing treatment. It is not only negative attitudes and lower help-seeking intentions that lead to an underusage of mental health services but also structural barriers that are based in the health care system.
Another interesting finding is that ethnic minorities and migrant groups often exhibit a lower MHL, due to adherence to more traditional values [22]. This is a finding we could not replicate in our study, but which may be important when considering the needs of international students. For example, the study of Salloum et al. [44] conducted in Malaysia found a lower MHL among the students from other regions than Southeast Asia, compared to Southeast-Asian students. Soorkia et al. [63] found that “cultural mistrust” and adherence to traditional Asian values were components that inhibited mental health care utilization of South Asian students at a university in UK. So, when developing mental health promotion programs for students, international students might be a subgroup that requires special attention.
Several study limitations should be considered when interpreting these results. First, the large difference in sample size between Cambodia and Vietnam students made it impossible to explore the country/culture effects on mental health literacy. All Cambodian participants were recruited from one university in Cambodia, thus the generalizability of findings is limited. Second, the study used convenient sampling. It is possible that students with a good knowledge of and interest in mental health were more likely to participate in the study. Thus, the sample may not be representative of students in general. Finally, as this was a cross-sectional study, relationships between variables can only be described, rather than proved.
Despite these limitations, study results have several important implications. First, MHL should be addressed in university settings. Improving MHL is effective in promoting help-seeking behaviors and improving mental health outcomes [20]. Interventions need to address help-seeking knowledge and efficacy rather than merely increase the knowledge on mental health symptoms. Secondly, stigmatizing attitudes have to be addressed. Thirdly, mental health promotion could be integrated as a compulsory course in all universities, such as physical education courses. Given the fact that young people tend to seek support from peers rather than adults, educating students on how to support others in case of mental health problems seems promising. Effective mental health promotion could make use of both the strategies.
Finally, factors associated with low MHL included male gender and studying STEM majors. Although it was not supported by our data, there is evidence that students with an ethnic minority background and international students are other groups with comparably lower MHL. MHL interventions should be tailored and targeted towards these groups.
This study obtained data on MHL from more than 1000 students from different parts of Vietnam and Cambodia. MHL was lower, compared to student samples from Western countries but in the same range as was reported by other Asian studies. The MHL of Southeast-Asian students needs to be improved, particularly among male students and among students from STEM majors. International students and students from ethnic minorities could be other target groups. Mental health promotion should not only address knowledge on mental disorders but also stigmatizing attitudes that are widespread and knowledge on how to find help. Given the cultural differences between Western countries where the concept of MHL was developed and Southeast Asia, any health promotion project in this field should be informed by local stakeholders and take into account the different values and perspectives.
Students are one of the populations that are massively impacted by the current COVID-19 pandemic. Taking care of the mental health of students is more important than ever.
Funding Statement: The authors received no specific funding for this study.
Conflicts of Interest: The authors declare that they have no conflicts of interest to report regarding the present study.
1. Auerbach, R. P., Mortier, P., Bruffaerts, R., Alonso, J., Benjet, C. et al. (2018). WHO World Mental Health Surveys International College Student Project: Prevalence and distribution of mental disorders. Journal of Abnormal Psychology, 127(7), 623–638. DOI 10.1037/abn0000362. [Google Scholar] [CrossRef]
2. Auerbach, R. P., Alonso, J., Axinn, W. G., Cuijpers, P., Ebert, D. D. et al. (2016). Mental disorders among college students in the World Health Organization World Mental Health Surveys. Psychological Medicine, 46(14), 2955–2970. DOI 10.1017/S0033291716001665. [Google Scholar] [CrossRef]
3. Alonso, J., Mortier, P., Auerbach, R. P., Bruffaerts, R., Vilagut, G. et al. (2018). Severe role impairment associated with mental disorders: Results of the WHO World Mental Health Surveys International College Student Project. Depression and Anxiety, 35(9), 802–814. DOI 10.1002/da.22778. [Google Scholar] [CrossRef]
4. Duffy, A., Saunders, K. E. A., Malhi, G. S., Patten, S., Cipriani, A. et al. (2019). Mental health care for university students: A way forward? Lancet. Psychiatry, 6(11), 885–887. DOI 10.1016/S2215-0366(19)30275-5. [Google Scholar] [CrossRef]
5. Rückert, H. W. (2015). Students’ mental health and psychological counselling in Europe. Mental Health & Prevention, 3(1–2), 34–40. DOI 10.1016/j.mhp.2015.04.006. [Google Scholar] [CrossRef]
6. Stallman, H. M. (2010). Psychological distress in university students: A comparison with general population data. Australian Psychologist, 45(4), 249–257. DOI 10.1080/00050067.2010.482109. [Google Scholar] [CrossRef]
7. Cao, W., Fang, Z., Hou, G., Han, M., Xu, X. et al. (2020). The psychological impact of the COVID-19 epidemic on college students in China. Psychiatry Research, 287(10224), 112934. DOI 10.1016/j.psychres.2020.112934. [Google Scholar] [CrossRef]
8. Sundarasen, S., Chinna, K., Kamaludin, K., Nurunnabi, M., Baloch, G. M. et al. (2020). Psychological impact of COVID-19 and lockdown among university students in Malaysia: Implications and policy recommendations. International Journal of Environmental Research and Public Health, 17(17), 6206. DOI 10.3390/ijerph17176206. [Google Scholar] [CrossRef]
9. Xiong, J., Lipsitz, O., Nasri, F., Lui, L. M. W., Gill, H. et al. (2020). Impact of COVID-19 pandemic on mental health in the general population: A systematic review. Journal of Affective Disorders, 277(1), 55–64. DOI 10.1016/j.jad.2020.08.001. [Google Scholar] [CrossRef]
10. WHO (n.d.). The Ottawa Charter for Health Promotion. http://www.who.int/healthpromotion/conferences/previous/ottawa/en/. [Google Scholar]
11. WHO (n.d.). Healthy Settings. http://www.who.int/healthpromotion/healthy-settings/en/. [Google Scholar]
12. WHO (1998). Health promoting universities. Copenhagen: WHO Regional Office for Europe. [Google Scholar]
13. 2015 International Conference on Health Promoting Universities and Colleges (2015). Okanagan Charter: An International Conference on Health Promoting Universities and Colleges. http://internationalhealthycampuses2015.sites.olt.ubc.ca/files/2016/01/Okanagan-Charter-January13v2.pdf [Google Scholar]
14. Newton, J., Dooris, M., Wills, J. (2016). Healthy universities: An example of a whole-system health-promoting setting. Global Health Promotion, 23(1_suppl), 57–65. DOI 10.1177/1757975915601037. [Google Scholar] [CrossRef]
15. Suárez-Reyes, M., van den Broucke, S., (2016). Implementing the health promoting university approach in culturally different contexts: A systematic review. Global Health Promotion, 23(1_suppl), 46–56. DOI 10.1177/1757975915623933. [Google Scholar] [CrossRef]
16. AUN Health Promotion Network (2017). AUN healthy university framework. Bangkok: Mahidol University. [Google Scholar]
17. Jorm, A. F., Korten, A. E., Jacomb, P. A., Christensen, H., Rodgers, B. et al. (1997). Mental health literacy: A survey of the public’s ability to recognise mental disorders and their beliefs about the effectiveness of treatment. Medical Journal of Australia, 166(4), 182–186. DOI 10.5694/j.1326-5377.1997.tb140071.x. [Google Scholar] [CrossRef]
18. WHO (2013). Health literacy. The solid facts. Copenhagen: WHO Regional Office for Europe. [Google Scholar]
19. Jorm, A. F. (2000). Mental health literacy: Public knowledge and beliefs about mental disorders. British Journal of Psychiatry, 177(5), 396–401. DOI 10.1192/bjp.177.5.396. [Google Scholar] [CrossRef]
20. Kutcher, S., Wei, Y., Coniglio, C. (2016). Mental health literacy: Past, present, future. Canadian Journal of Psychiatry, 61(3), 154–158. DOI 10.1177/0706743715616609. [Google Scholar] [CrossRef]
21. Jorm, A. F. (2012). Mental health literacy: Empowering the community to take action for better mental health. American Psychologist, 67(3), 231–243. DOI 10.1037/a0025957. [Google Scholar] [CrossRef]
22. Furnham, A., Swami, V. (2018). Mental health literacy: A review of what it is and why it matters. International Perspectives in Psychology: Research, Practice, Consultation, 7(4), 240–257. DOI 10.1037/ipp0000094. [Google Scholar] [CrossRef]
23. Grant, J., Bruce, C. P., Batterham, P. J. (2016). Predictors of personal, perceived and self-stigma towards anxiety and depression. Epidemiology and Psychiatric Sciences, 25(3), 247–254. DOI 10.1017/S2045796015000220. [Google Scholar] [CrossRef]
24. Martin, J. M. (2010). Stigma and student mental health in higher education. Higher Education Research & Development, 29(3), 259–274. DOI 10.1080/07294360903470969. [Google Scholar] [CrossRef]
25. O’Connor, M., Casey, L. (2015). The Mental Health Literacy Scale (MHLSA new scale-based measure of mental health literacy. Psychiatry Research, 229(1-2), 511–516. DOI 10.1016/j.psychres.2015.05.064. [Google Scholar] [CrossRef]
26. Reavley, N. J., McCann, T. V., Jorm, A. F. (2012). Mental health literacy in higher education students. Early Intervention in Psychiatry, 6(1), 45–52. DOI 10.1111/j.1751-7893.2011.00314.x. [Google Scholar] [CrossRef]
27. Smith, C. L., Shochet, I. M. (2011). The impact of mental health literacy on help-seeking intentions: Results of a pilot study with first year psychology students. International Journal of Mental Health Promotion, 13(2), 14–20. DOI 10.1080/14623730.2011.9715652. [Google Scholar] [CrossRef]
28. Bonabi, H., Müller, M., Ajdacic-Gross, V., Eisele, J., Rodgers, S. et al. (2016). Mental health literacy, attitudes to help seeking, and perceived need as predictors of mental health service use: A longitudinal study. Journal of Nervous and Mental Disease, 204(4), 321–324. DOI 10.1097/NMD.0000000000000488. [Google Scholar] [CrossRef]
29. Furnham, A., Cook, R., Martin, N., Batey, M. (2011). Mental health literacy among university students. Journal of Public Mental Health, 10(4), 198–210. DOI 10.1108/17465721111188223. [Google Scholar] [CrossRef]
30. Gorczynski, P., Sims-Schouten, W., Hill, D., Wilson, J. C. (2017). Examining mental health literacy, help seeking behaviours, and mental health outcomes in UK university students. Journal of Mental Health Training, Education and Practice, 12(2), 111–120. DOI 10.1108/JMHTEP-05-2016-0027. [Google Scholar] [CrossRef]
31. Gorczynski, P., Sims-Schouten, W., Wilson, C. (2020). Evaluating mental health literacy and help-seeking behaviours in UK university students: A country wide study. Journal of Public Mental Health, 19(4), 311–319. DOI 10.1108/JPMH-10-2019-0086. [Google Scholar] [CrossRef]
32. Lauber, C., Ajdacic-Gross, V., Fritschi, N., Stulz, N., Rössler, W. (2005). Mental health literacy in an educational elite. An online survey among university students. BMC Public Health, 5(1), 44. DOI 10.1186/1471-2458-5-44. [Google Scholar] [CrossRef]
33. Kim, J. E., Saw, A., Zane, N. (2016). The influence of psychological symptoms on mental health literacy of college students. American Journal of Orthopsychiatry, 85(6), 620–630. DOI 10.1037/ort0000074. [Google Scholar] [CrossRef]
34. Rafal, G., Gatto, A., DeBate, R. (2018). Mental health literacy, stigma, and help-seeking behaviors among male college students. Journal of American College Health, 66(4), 284–291. DOI 10.1080/07448481.2018.1434780. [Google Scholar] [CrossRef]
35. Pehlivan, Ş., Tokur Kesgi, N. M., Uymaz, P. (2021). Psychological distress and mental health literacy in university students. Perspectives in Psychiatric Care, 57(3), 1433–1441. DOI 10.1111/ppc.12709. [Google Scholar] [CrossRef]
36. Amarasuriya, S. D., Jorm, A. F., Reavley, N. J. (2018). Predicting intentions to seek help for depression among undergraduates in Sri Lanka. BMC Psychiatry, 18(1), 122. DOI 10.1186/s12888-018-1700-4. [Google Scholar] [CrossRef]
37. Mahfouz, M. S., Aqeeli, A., Makeen, A. M., Hakami, R. M., Najmi, H. H. et al. (2016). Mental health literacy among undergraduate students of a Saudi tertiary institution: A cross-sectional study. Mental Illness, 8(2), 6806. DOI 10.1108/mi.2016.6806. [Google Scholar] [CrossRef]
38. Youssef, F. F., Bachew, R., Bodie, D., Leach, R., Morris, K. et al. (2014). Knowledge and attitudes towards mental illness among college students: Insights into the wider English-speaking Caribbean population. International Journal of Social Psychiatry, 60(1), 47–54. DOI 10.1177/0020764012461236. [Google Scholar] [CrossRef]
39. Chen, A., Mond, J. M., Kumar, R. (2010). Eating disorders mental health literacy in Singapore: Beliefs of young adult women concerning treatment and outcome of bulimia nervosa. Early Intervention in Psychiatry, 4(1), 39–46. DOI 10.1111/j.1751-7893.2009.00156.x. [Google Scholar] [CrossRef]
40. Ibrahim, N., Amit, N., Shahar, S., Wee, L. H., Ismail, R. et al. (2019). Do depression literacy, mental illness beliefs and stigma influence mental health help-seeking attitude? A cross-sectional study of secondary school and university students from B40 households in Malaysia. BMC Public Health, 19(Suppl 4), 544. DOI 10.1186/s12889-019-6862-6. [Google Scholar] [CrossRef]
41. Kamimura, A., Trinh, H. N., Johansen, M., Hurley, J., Pye, M. et al. (2018). Perceptions of mental health and mental health services among college students in Vietnam and the United States. Asian Journal of Psychiatry, 37(5), 15–19. DOI 10.1016/j.ajp.2018.07.012. [Google Scholar] [CrossRef]
42. Khan, T. M., Sulaiman, S. A., Hassali, M. A. (2010). Mental health literacy towards depression among non-medical students at a Malaysian university. Mental Health in Family Medicine, 7, 27–35. [Google Scholar]
43. Nguyen Thai, Q. C., Nguyen, T. H. (2018). Mental health literacy: Knowledge of depression among undergraduate students in Hanoi, Vietnam. International Journal of Mental Health Systems, 12(1), 19. DOI 10.1186/s13033-018-0195-1. [Google Scholar] [CrossRef]
44. Salloum, A., Ismail, S. (2020). Factors associated with mental health literacy among international postgraduate students. International Journal of Public Health and Clinical Sciences, 7, 14–27. [Google Scholar]
45. Wei, Y., McGrath, P. J., Hayden, J., Kutcher, S. (2016). Measurement properties of tools measuring mental health knowledge: A systematic review. BMC Psychiatry, 16(1), 297. DOI 10.1186/s12888-016-1012-5. [Google Scholar] [CrossRef]
46. Wei, Y., McGrath, P. J., Hayden, J., Kutcher, S. (2017). Measurement properties of mental health literacy tools measuring help-seeking: A systematic review. Journal of Mental Health, 26(6), 543–555. DOI 10.1080/09638237.2016.1276532. [Google Scholar] [CrossRef]
47. Dang, H. M., Weiss, B., Lam, T., Ho, H. (2018). Mental health literacy and intervention program adaptation in the internationalization of school psychology for Vietnam. Psychology in the Schools, 55(8), 941–954. DOI 10.1002/pits.22156. [Google Scholar] [CrossRef]
48. Coles, M. E., Coleman, S. L. (2010). Barriers to treatment seeking for anxiety disorders: Initial data on the role of mental health literacy. Depression and Anxiety, 27(1), 63–71. DOI 10.1002/da.20620. [Google Scholar] [CrossRef]
49. Coles, M. E., Ravid, A., Gibb, B., George-Denn, D., Bronstein, L. R. et al. (2016). Adolescent mental health literacy: Young people’s knowledge of depression and social anxiety disorder. Journal of Adolescent Health, 58(1), 57–62. DOI 10.1016/j.jadohealth.2015.09.017. [Google Scholar] [CrossRef]
50. Bandelow, B., Michaelis, S. (2015). Epidemiology of anxiety disorders in the 21st century. Dialogues in Clinical Neuroscience, 17, 327–335. DOI 10.31887/DCNS. [Google Scholar] [CrossRef]
51. Furnham, A., Lousley, C. (2013). Mental health literacy and the anxiety disorders. Health, 5(3), 720–726. DOI 10.4236/health.2013.53A071. [Google Scholar] [CrossRef]
52. Barlow, D. H. (2004). Anxiety and its disorders: The nature and treatment for anxiety and panic. New York: Guilford Press. [Google Scholar]
53. Furnham, A., Hamid, A. (2014). Mental health literacy in non-western countries: A review of the recent literature. Mental Health Review Journal, 19(2), 84–98. DOI 10.1108/MHRJ-01-2013-0004. [Google Scholar] [CrossRef]
54. van der Ham, L., Wright, P., van, T. V., Doan, V. D. K., Broerse, J. E. W. (2011). Perceptions of mental health and help-seeking behavior in an urban community in Vietnam: An explorative study. Community Mental Health Journal, 47(5), 574–582. DOI 10.1007/s10597-011-9393-x. [Google Scholar] [CrossRef]
55. Furnham, A., Annis, J., Cleridou, K. (2014). Gender differences in the mental health literacy of young people. International Journal of Adolescent Medicine and Health, 26(2), 283–292. DOI 10.1515/ijamh-2013-0301. [Google Scholar] [CrossRef]
56. Pumpuang, A. S., Nopporn, V. (2018). Factors predicting intention among nursing students to seek professional psychological help. Pacific Rim International Journal of Nursing Research, 22, 200–211. [Google Scholar]
57. Shi, J., Kim, H. K., Su, Y., Kong, H. (2020). Mental health conditions in young Asian adults and motivation to seek counseling: A cross-country study. Asia Pacific Journal of Public Health, 32(6–7), 328–333. DOI 10.1177/1010539520937091. [Google Scholar] [CrossRef]
58. Ten Have, M., de Graaf, R., Ormel, J., Vilagut, G., Kovess, V. et al. (2010). Are attitudes towards mental health help-seeking associated with service use? Results from the European study of epidemiology of mental disorders. Social Psychiatry and Psychiatric Epidemiology, 45(2), 153–163. DOI 10.1007/s00127-009-0050-4. [Google Scholar] [CrossRef]
59. Connell, R. (2012). Gender, health and theory: Conceptualizing the issue, in local and world perspective. Social Science & Medicine, 74(11), 1675–1683. DOI 10.1016/j.socscimed.2011.06.006. [Google Scholar] [CrossRef]
60. Thai, T. T., Vu, N. L. L. T., Bui, H. H. T. (2020). Mental health literacy and help-seeking preferences in high school students in ho Chi Minh City, Vietnam. School Mental Health, 12(2), 378–387. DOI 10.1007/s12310-019-09358-6. [Google Scholar] [CrossRef]
61. Dang, H. M., Lam, T., Dao, A., Weiss, B. (2020). Mental health literacy at the public health level in low- and middle-income countries: An exploratory mixed methods study. PLoS One, 15(12), e0244573. DOI 10.1371/journal.pone.0244573. [Google Scholar] [CrossRef]
62. UNICEF Vietnam, Overseas Development Institute (2018). Mental health and psychosocial wellbeing among children and young people in selected provinces and cities in Viet Nam. Ha Noi: UNICEF Vietnam. [Google Scholar]
63. Soorkia, R., Snelgar, R., Swami, V. (2011). Factors influencing attitudes towards seeking professional psychological help among South Asian students in Britain. Mental Health, Religion & Culture, 14(6), 613–623. DOI 10.1080/13674676.2010.494176. [Google Scholar] [CrossRef]
64. Burns, S., Crawford, G., Hallett, J., Hunt, K., Chih, H. J. et al. (2017). What’s wrong with John? A randomised controlled trial of Mental Health First Aid (MHFA) training with nursing students. BMC Psychiatry, 17(1), 111. DOI 10.1186/s12888-017-1278-2. [Google Scholar] [CrossRef]
65. Morgan, A. J., Ross, A., Reavley, N. J. (2018). Systematic review and meta-analysis of Mental Health First Aid training: Effects on knowledge, stigma, and helping behaviour. PLoS One, 13(5), e0197102. DOI 10.1371/journal.pone.0197102. [Google Scholar] [CrossRef]
 | This work is licensed under a Creative Commons Attribution 4.0 International License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. |