| International Journal of Mental Health Promotion |
DOI: 10.32604/ijmhp.2022.019623
ARTICLE
Mindfulness Intervention on Adolescents’ Emotional Intelligence and Psychological Capital during the COVID-19 Pandemic: A Randomized Controlled Trial
1Northwest Normal University, Lanzhou, 730070, China
2Hongkong Baptist University, Hong Kong, 999077, China
*Corresponding Author: Yue Yuan. Email: livia428192@foxmail.com
Received: 04 October 2021; Accepted: 27 January 2022
Abstract: Background: Since the outbreak of COVID-19 caused adults suffer from mental disorders, it would be an essential for psychologist to help individuals overcome mental disorders. Objective: This study aim to explore whether the intervention of mindfulness is an efficient method to enhance adolescents’ emotional intelligence (EI) and psychological capital (PC) to provide a theoretical basis and future directions for both targeted crisis intervention and psychological trauma recovery plans. Design: This research was designed as randomized controlled trial and total of 798 students were evaluated statistically. Methods: We used paired-sample t-tests and repeated measures ANOVA to compare every factor defined above by time and group. Then, we used Mplus to build LGCM to examine the trajectory of changes in EI and PC in the experimental group. Results and Conclusions: (1) The EI and PC scores had significantly different time points in the experimental group but not in the control group. (2) EI and PC tended to increase with intervention, and there were significant individual differences in the initial level and development speed. (3) Individuals’ EI could promote the growth of PC. This research indicated that mindfulness should be given increasing consideration to enhance mental health during the worldwide outbreak of COVID-19.
Keywords: COVID-19 pandemic; adolescents; mindfulness; preparation; emotional intelligence; psychological capital
The outbreak of COVID-19 has caused a global pandemic that threatens people’s physical health and has tremendous mental health impact [1–7]. In China, during the confinement period, between late January and the middle of March, adolescents were more vulnerable to passive emotion than adults [8–10]. Although some studies have reported the passive impact of individuals’ mental health during the COVID-19 pandemic [11–13], little is known about effective intervention methods for improving psychological health issues long term. It is essential and is also a responsible course of action for every psychologist to help individuals work through and even overcome mental disorders during the COVID-19 pandemic. Therefore, the main purpose of this study was to explore whether the intervention of mindfulness is an efficient method to enhance adolescents’ emotional intelligence and psychological capital during the COVID-19 pandemic and to provide a theoretical basis and future directions for both targeted crisis intervention and psychological trauma recovery plans.
Mindfulness refers to self-cultivation that focuses on meditation techniques with the goal of self-improvement and liberation. From the perspective of psychology, mindfulness is a conscious, nonjudgmental awareness of internal and external experiences that can be developed through practice [14]. When someone is practicing mindfulness, their emotion and cognition are more open and accepting [15]. Studies have indicated that mindfulness-based interventions can influence mental health in a positive way [16–19]. Researchers have integrated the concept of mindfulness and emotion regulation theoretically and have developed the mindfulness emotion regulation model [20]. This model claims there is no need to suppress, reevaluate or change emotional experiences but that one should train his or her awareness and nonreactivity of emotion systematically, which emphasizes that mindfulness training focused on awareness rather than being aware of emotional goals. Individuals intentionally select and recognize thoughts, emotions, and feelings but do not produce habitual responses, thereby gradually eliminating the process of automatic evaluation of distressing emotions (including sadness, anxiety, fear, disgust, satisfaction, and desire) [20]. This theoretical model has been supported by some empirical studies. For instance, clinical psychologists utilized the Freiburg Mindfulness Inventory to investigate the relationship between mindfulness and depressive symptoms among 514 college students, and they found that mindfulness can decrease depressive symptoms [21], which confirmed the mindfulness emotion regulation model and how it benefit for mental health.
Psychological capital (PC) represents the positive mental development of a person and relates to an individual’s development of personality and his/her mental health [22–24]. There are four aspects of PC: Self-efficacy, optimism, hope, and resilience. Self-efficacy indicates that individuals can put forth the effort necessary to successfully overcome a challenge. Optimism means that individuals can make positive attributions towards achievement now and in the future. Notably, hope represents one’s ability to redirect their routes to achieve an aim when required, and resilience refers to one’s ability to sustain hope and bounce back to achieve goals when surrounded by adversity and trouble [23,24]. Previous studies have indicated that PC resources positively predict individuals’ happiness and school engagement [25] among both college [26] and high school [27] students. Considering the wide range of negative emotional (depression, anxiety, tension, and anger) impacts during the outbreak of COVID-19 [28], PC resources are highly related to academic engagement and achievement [25]. Therefore, the intervention in this research is aimed to promote the PC of students to help them handle the passive emotional impact during the COVID-19 pandemic and boost their academic engagement and achievement.
In the book “Psychological Capital” [24], emotional intelligence (EI) is classified as a kind of potential PC and defined as an ability to recognize and comprehend someone’s own and other emotions so that this information can be used to guide an individual’s cognition and behaviors [29,30] including the ability to perceive the emotions of oneself and others; the ability to use emotions to make better decisions; the ability to understand emotions and the ability to manage the emotions of oneself and others. Later, Bar-On [31] defined EI as a noncognitive capacity in coping with environmental demands and stresses. Moreover, a large number of empirical studies have led to two different models of EI: the ability model and the mixed comprehensive model. The ability model defines EI as a type of intelligence that focuses on emotion itself and has a strong relationship with thinking [32]. The second model is the comprehensive model which assumes that EI is an individual’s ability and is also related to personality and traits [31,33]. The ability model of EI merely focuses on a set of individual abilities related to emotion [34,35], whereas the comprehensive model combines EI with personality and traits [31]. Thus, we chose the comprehensive model of EI as a theoretical framework for our study. Studies indicated EI is beneficial for regulating negative emotions [34,35]. For instance, Mavroveli et al. [36] and Kat et al. [37] reported a negative relationship between EI and the rate of depression and anxiety among young adults; that is, individuals with higher EI reported a lower rate of depressive and anxiety experiences. Moreover, adolescents with higher EI obtain better academic engagement and achieve higher scores on their exams [38,39].
The context of this research is that the COVID-19 outbreak caused a global pandemic with tremendous mental health impacts in addition to threats to people’s physical health [1]. Chinese adolescents (20%–40%) were found to be prone to serious mental problems [8,9]. As mentioned before, mindfulness is beneficial for increasing an individual’s mental health. Therefore, we chose mindfulness as an intervention method to help improve their EI and PC to further recover from the pandemic and maintain healthy minds.
This intervention research was conducted during the COVID-19 pandemic in China. Before March 15, 2021, the area where the school involved in the study was located had not had a case for two weeks. Confinement restrictions were lifted from the area in early March. This study started on March 15, when all students started school after a long period of confinement and the winter holiday. In addition, this research ended on November 27, 2021. During the research period, all the students studied at school every day. In the process of studying in school, they still faced strict pandemic prevention and control requirements, such as body temperature measurements being taken before entering school, not being allowed to get together in the school, wearing masks in class, and so on.
The main researcher was the mental health teacher in the middle school. This research was approved by the Ethical Committee of Northwest Normal University (Granted No. 202003015). We selected all students in grades 8 (aged 14) and 9 (aged 15) (8 classes in each grade) in a total of 16 classes. At first, we sent the informed consent to students and their parents or guardians. All of them agreed to take part in this program and signed informed consent. Then, we administered the Emotional Intelligence Scale (EIS) and Psychological Capital Questionnaire (PCQ) to all students on paper in class on March 16th (T1). Then, we divided the 8 classes in each grade into 2 groups randomly; the experiment group comprised 4 classes (n = 412; males = 209, females = 203; age: M(SD) = 14.25(0.50)) and the control group comprised 4 classes (n = 408; males = 203, females = 205; age: M(SD) = 14.35(0.45)). There was no significant difference in EIS or PCQ scores between the experimental and control groups at T1 (p > 0.05).
In the experimental group, we conducted mindfulness practice interventions in the psychology class twice a week, and there was no intervention in the control group.
In the experiment group, Mindfulness Course which was developed by mindfulness instructors Jack Kornfield and Tara Brach and recorded by Chinese mindfulness instructors named Tong Huiqi and Guo Haifeng, was chosen as intervention training media. This course consists of 40 lessons, including “Arriving in presence,” “Conscious relaxing,” “Coming back to your senses,” “Attitude of friendliness,” “Mindfulness of breath,” “Calming and steadying with the breath,” “Counting the breath,” “Deepening the focus,” “Mindfulness of the body,” “Feeling from the inside out,” “Body scan,”“Naming sensations,” Working with intense sensations, Mindfulness and emotions, Beyond thoughts, The core practice, “Self-judgment and self-compassion,” “Resilience, healing and inner freedom,” “Emotion and inner resources,” “Emotion and accepting,” “Spacious awareness,” “Equanimity,” “Equanimity,” “Mindfulness of awareness,” “Empathy and compassion,” “Forgiveness,” “Seeing goodness,” “Intention,” “Conflict,” “Listening,” “Speaking,” “Trusting and inhabiting your being,” “Generosity and service,” “Nourishing a grateful heart” and “Aspiration and vision.” Every course of mindfulness practice lasts around ten minutes. In every class of psychology, we played 2 courses of mindfulness practice. After every course, we would take 10 min to let students share their feelings. In total, we conducted two-loops of the Mindfulness Course. Each loop of the course lasts around sixteen weeks.
We performed 3 assessments after 8 weeks, 16 weeks, and 24 weeks of intervention in May (T2), September (T3), and November (T4) in the experimental group. In the control group, we only performed assessments in November (T4). There was no intervention or assessment in June and July since it was the summer holiday for school. In the experimental group, 3 participants were absent during the second assessment (T2); 6 participants were absent during the third assessment (T3), 7 subjects were absent during the fourth assessment (T4), and 6 subjects were absent in the control group when we performed the assessment in November (T4). Therefore, there were 396 (males = 204, females = 192; age: M(SD) = 14.50(0.25)) participants in the experimental group and 402 (males = 200, females = 202; age: M(SD) = 14.35(0.45)) subjects in the control group, as shown in Fig. 1.
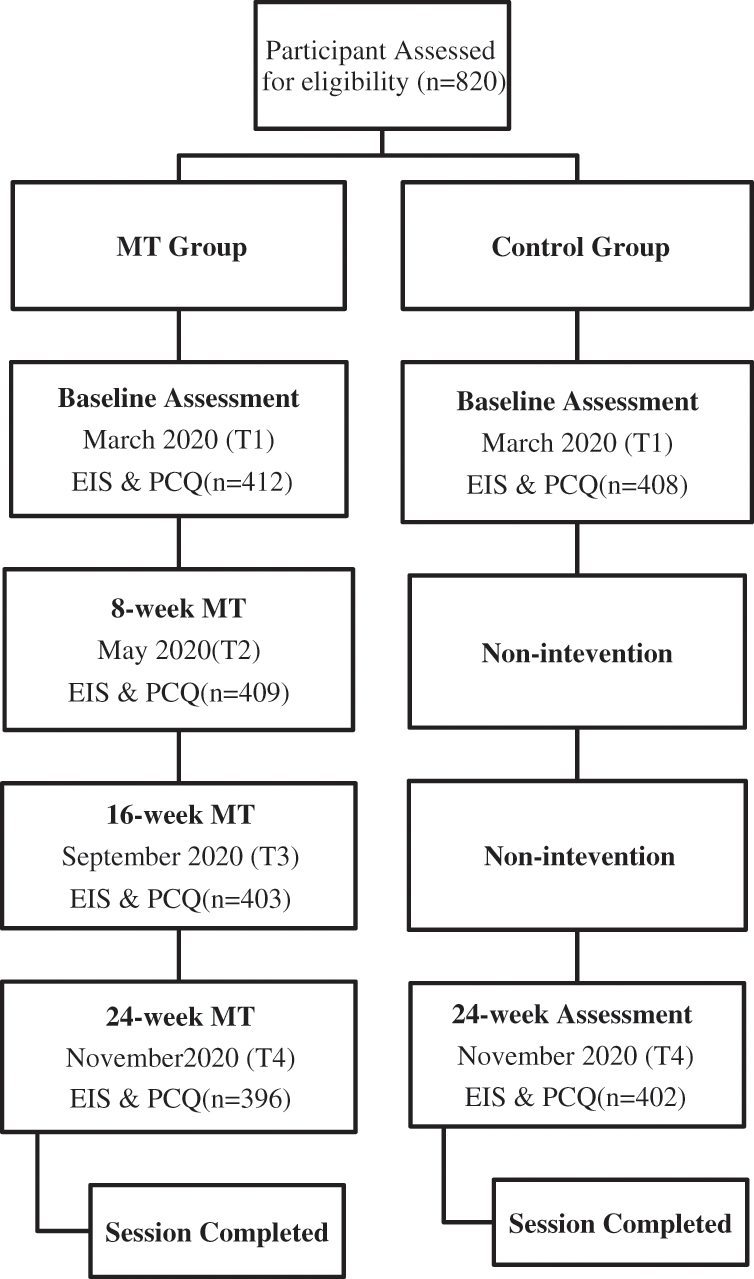
Figure 1: Flow diagram of controlled trial
In this research, SPSS 26.0 and Mplus Version 8.3 [40]. were used for data analysis. Firstly, we use a paired-sample t-test to compare every factor’s difference at a different time point. Then, repeated ANOVA was used to measure 2 (group: experiment, control) × 2 (time: T1 at baseline, T4 at 24-week intervention) to compare the difference between the experiment and control group at the time points of T1 and T4. Finally, we use Mplus Version 8.3 to build a latent growth model (LGM) in the experiment group. Specifically, in the experiment group, in order to examine the trajectory changes in the individual differences in the initial levels and speed of EI and PC, we exhibited an unconditional latent growth model. To examine whether EI’s trajectory is affected by PC, PC was used as the time variation factor in the latent growth model.
3.1 The Contrast of the Experimental and Control Groups
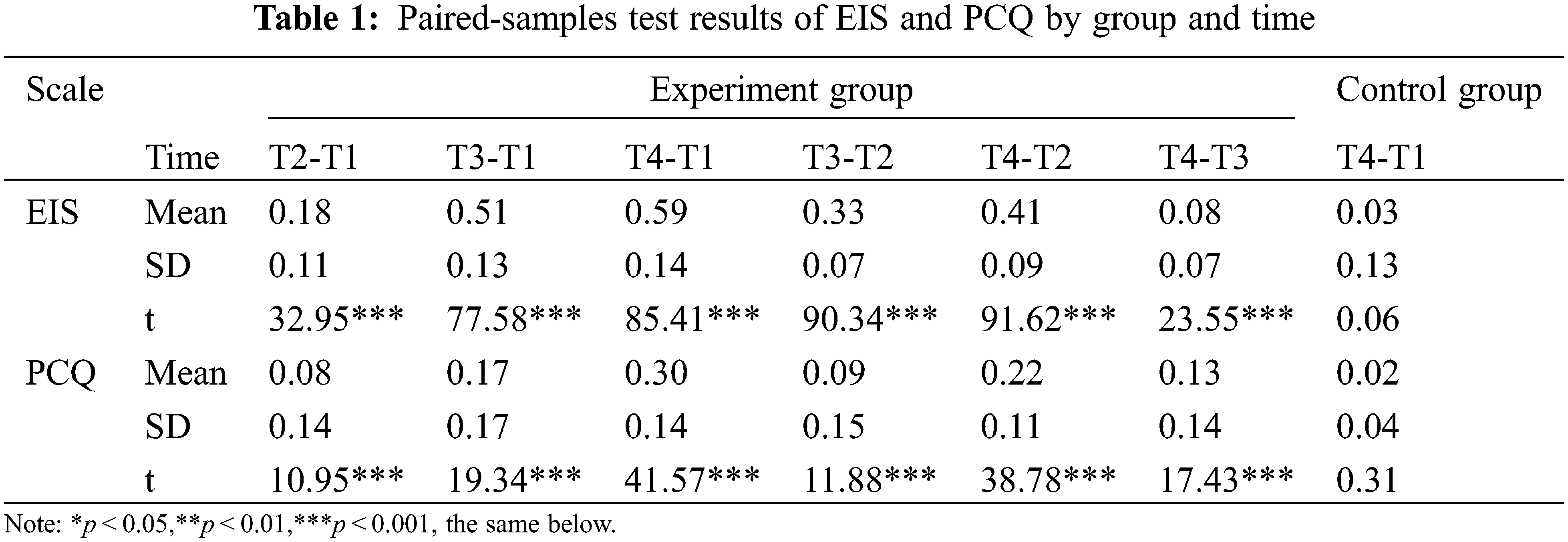
In order to examine how EI and PC were affected by mindfulness intervention at every time point, we performed a pair of sample t-test (Table 1) in the experiment and control groups. The result of the experiment group demonstrated that the score of EIS was in significant difference at 0.001 levels over time, which implied that mindfulness can enhance EI from T2 to T1, from T3 to T2, and from T4 to T3. Nonetheless, no significant differences were found in the control group, which proves there is no improvement in EI over time. Besides, the result of PCQ showed that psychological capital was significantly different in the experiment group from T2 to T1, from T3 to T2, and from T4 to T3 at 0.001 levels, while no significant differences were found in the control group. This result strongly indicated that PC can be improved by the intervention of mindfulness, but will not improve over time. Table 1 illustrated the descriptive statistics details of the experiment group and control group at T1, T2, T3, and T4, respectively.
Then, we submitted the data to a 2 (group: experiment, control) × 2 (time: T1 at baseline, T4 at 24-week intervention) mixed-design analysis of variance. Repeated measure ANOVA emulated how EIS and PCQ were influenced by mindfulness intervention in this research. The outcome of ANOVA illustrated that the main effect of time was significant (F = 7218.64, p < 0.001) at 0.001 level, and the main effect of the group were significant (F = 3487.96, p < 0.001) at 0.001 level as well. Fig. 2A depicted in different time points what is the contrast of EIS between groups of experimental and control. As we can see in Fig. 2A, the score of EIS has been significantly improved through 24-weeks intervention of mindfulness in the experiment group, while there is no significant enhancement in the control group. From this outcome, we can easily conclude that the intervention of mindfulness conduces to the enhancement of EIS. Meanwhile, for the result of PCQ, the outcome of repeated ANOVA proved that there was significant differences in the main effect of both times (F = 1057.53, p < 0.001) and group (F = 396.56, p < 0.001) at 0.001 level. Specifically, the comparison of the PCQ between the experiment and control group is illustrated in Fig. 2B. From Fig. 2B, we can see PCQ increased significantly after 24-week mindfulness cognitive therapy, while there is no significant difference in the control group at time points of T1 and T4, which indicated mindfulness cognitive therapy contributes to the growth of PCQ.
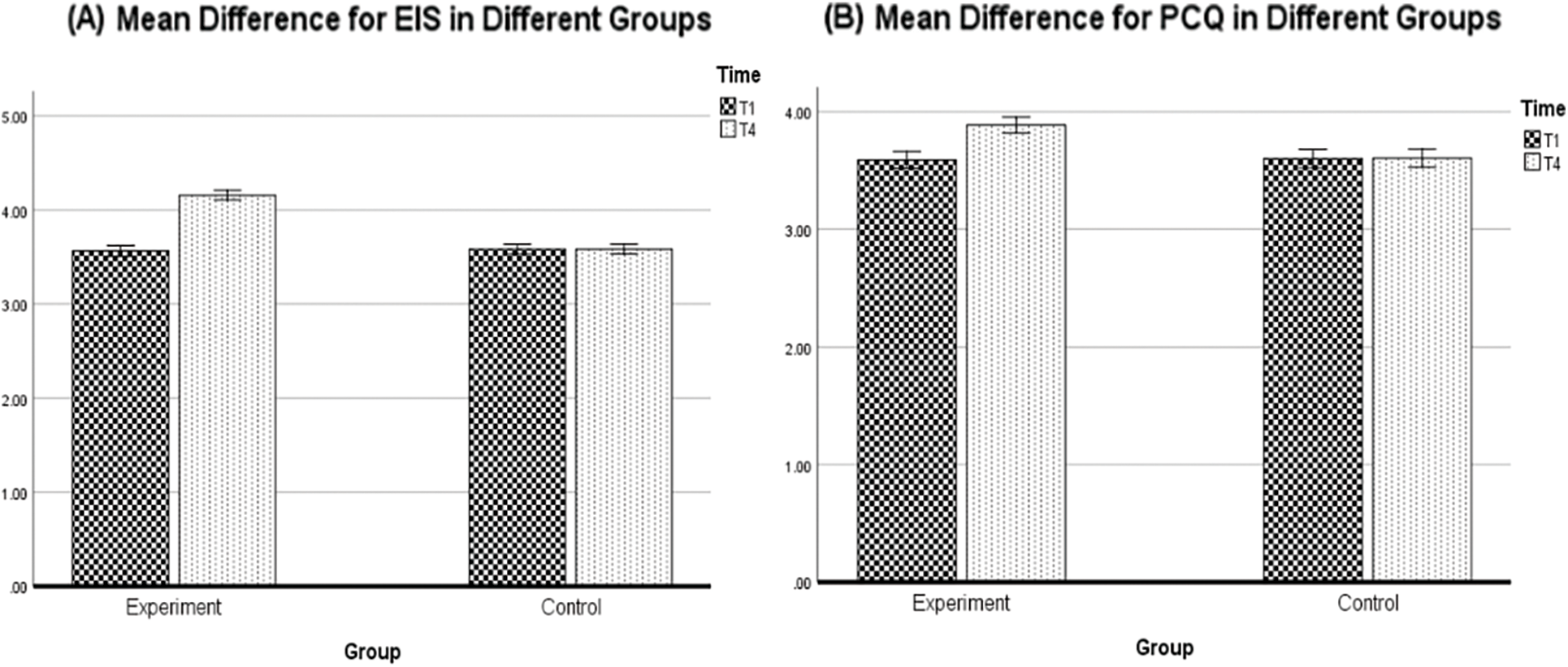
Figure 2: (A) Mean difference for EIS in different groups. (B) Mean difference for PCQ in different groups
3.2 Descriptive Statistics in the Experimental Group
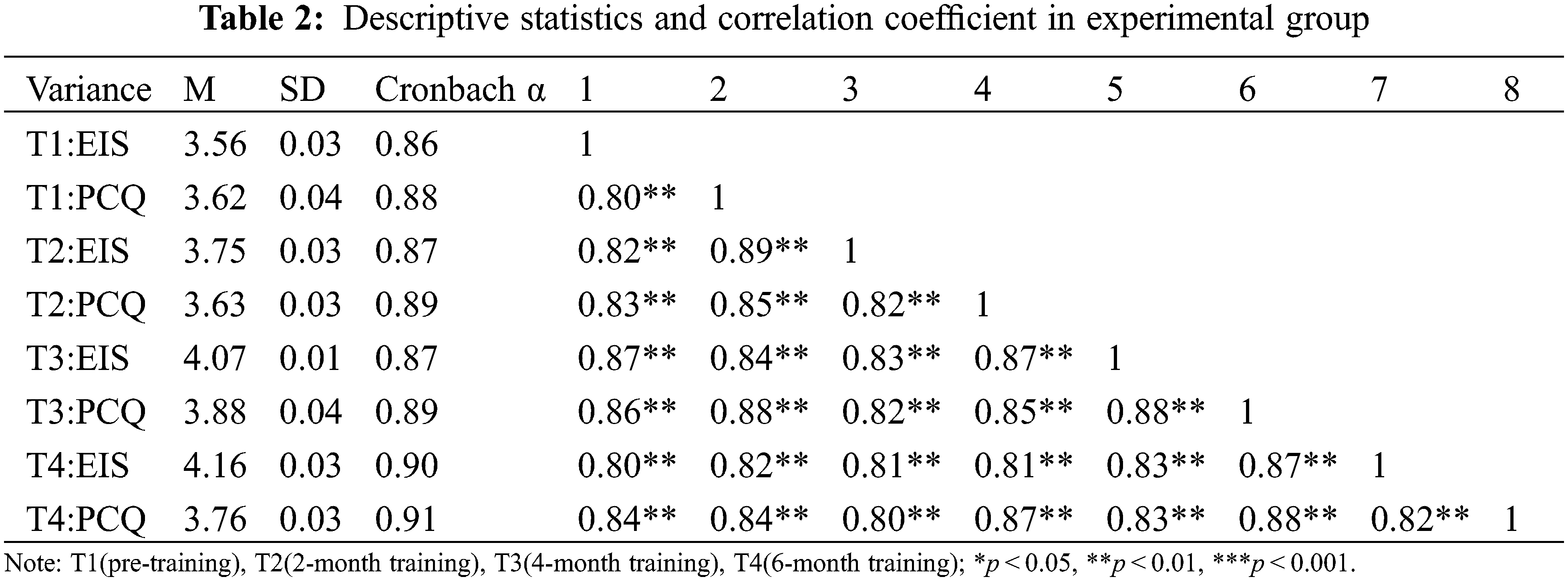
In the experiment group, the descriptive statistics were illustrated in Table 2, which includes the mean value (M), standard deviation (SD), skewness, kurtosis, Cronbach’s α, correlation coefficient matrix of both EI and PC at assessments of T1, T2, T3, T4 separately one by one. As can be seen in Table 2, EI and PC firmly and significantly correlated with each other at 4-time point tests (p < 0.001). On the other hand, in all assessments, the skewness and kurtosis of the EIS and PCQ were below 1.0, which indicated the acceptance of data departure from normality. Besides, from Table 2, we can see the skewness and kurtosis of the EIS and PCQ were 1.0 across all assessments, and the departure of data from normality was acceptable. Since all variables fulfill the normal distribution assumption, when performing the LGM, we applied the maximum likelihood (ML) method to forecast the parameters of the model.
3.3 The Trajectory of Emotional Intelligence and Psychological Capital: Unconditional Latent Growth Curve Model (LGCM)
Unconditional linear latent growth model (LGM) and unconditional quadratic LGM were both executed to investigate the trajectory of EI and PC. The χ2 distribution, the root mean square error of approximation (RMSEA), and the comparative fit index (CFI) was all alsos used to determine model fit. A poor model fit was defined as 0.10 to 0.08, an acceptable model fit was defined as 0.08 to 0.05, and a good model fit was defined as 0.08 to 0.05 [41]. CFI values between 0.90 and 0.94 were regarded as acceptable, while values over 0.95 indicated a well-fitting model [41]. When the p-value was less than. 05, we assumed that statistical significance had been achieved. Our result of the latent growth curve model were illustrated in Table 3.
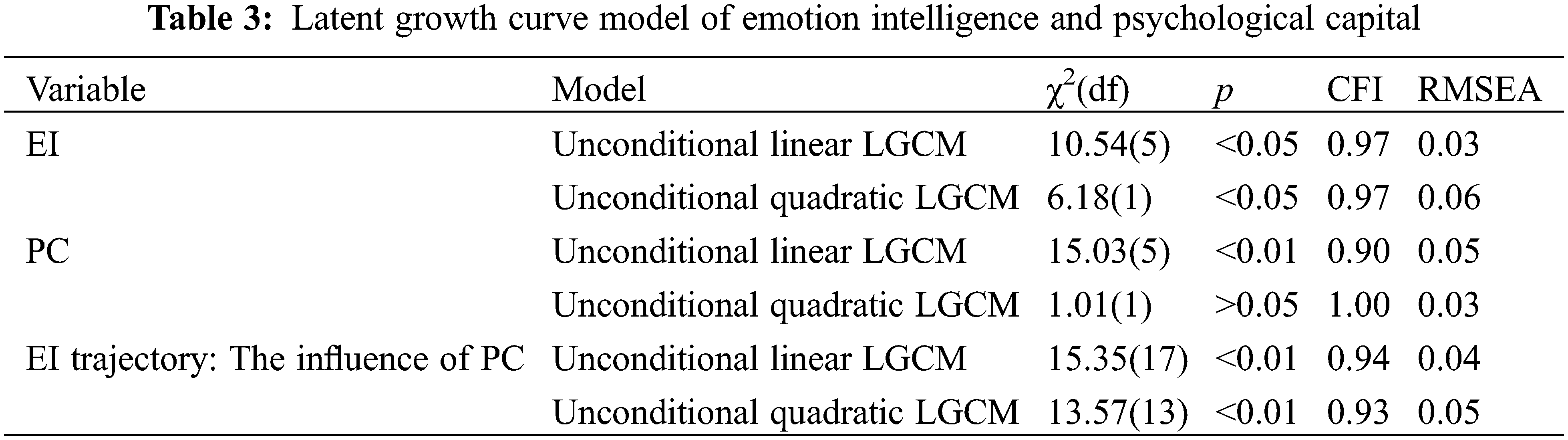
The fit of unconditional LGM of EIS (χ2(df) = 10.54(5); p < 0.001; CFI = 0.97; RMSEA = 0.03) is acceptable. Both the mean value of slope and the variance of the slope are significant. More specifically, the mean value of the slope is 0.21, which is significant at 0.05 level. And the variance of the slope is 0.001, which is significantly different at the level of 0.001. This shows that not only is the initial level of individuals a significant difference, but also that the growth rate of individuals is different significantly. The connection between the subject’s initial EI condition and growth rate is significantly positive, since the slope’s and intercept’s correlation coefficient is −0.004 (p < 0.01). More specifically, subjects who are in the low initial condition of EI score rise faster with the intervention of mindfulness. What’s more, from the data analysis of EIS made by Mplus, we can see the unconditional LGM suit better than the Unconditional Quadratic LGM (χ2(df) = 6.18(1); p < 0.001; CFI = 0.97; RMSEA = 0.06). This founding indicates that the trajectory of the subject’s EI illustrates a non-curve tendency. During the four tests, the slope of unconditional LGM of EIS is 0.32 (p < 0.001), indicating the score of EIS demonstrated an upward tendency. The linear slope is −0.04 (p < 0.001), showing that the rate of improvement enhanced month by month. Besides, there are significant inter-individual differences between the initial level of EI and the consecutive growth rate, since the variation of slope (σ2 ) is −0.097 (p < 0.001) and the variation of linear slope (σ2 ) is −0.002 (p < 0.001). Aside from that, the correlation coefficient of intercept and slope is 0.039 (p < 0.05); the correlation coefficient of the intercept and linear slope is 0.029 (p < 0.01); the correlation coefficient of slope and linear slope is −0.008 (p < 0.01), which all have significant differences. This result indicates there’s a considerable correlation between speed, acceleration, and the initial level of EI upward.
For PC, the unconditional LGM of PCQ (χ2(df) = 15.03(5); p < 0.001; CFI = 0.90; RMSEA = 0.05) fit well. The initial level and upward tendency of participants are significantly different since the mean of the slope is 3.583 (p < 0.001) and the variance of the slope is 0.098 (p < 0.001). The slope’s and intercept’s correlation coefficient is −0.014 (p < 0.01), suggesting that the relationship between the initial state of an individual’s PC and the growth rate of an individual’s PC is significantly positive. Specifically, participants who are in a low beginning state show faster growth. What’s more, the data fit the unconditional LGM (χ2(df) = 1.01(1); p > 0.05; CFI = 1.000; RMSEA = 0.03) better than the unconditional quadratic LGM. This means participants’ PC showed a non-curve trajectory by the intervention of mindfulness. As the data has shown in the four tests, the trajectory of PC is an upward increase during the mindfulness intervention (Slope = 0.064, p < 0.001). While the linear slope is 0.011 (p < 0.001), and the growth rate increased month by month. What’s more, there are obvious inter-individual differences between the initial level of PC and the subsequent change speed, while the data of the slope variation (σ2 ) is 0.194 (p < 0.001) and the data of linear slope variation (σ2 ) is 0.011 (p < 0.001). In addition, the correlation coefficient between slope and intercept (r = −0.285, p < 0.001); linear slope and intercept (r = 0.071, p < 0.001); the correlation coefficient of linear slope and slope (r =−0.032, p < 0.001) all have significant differences, indicating that there is a significant correlation between the initial level of PC growth, the speed, and acceleration of PC growth.
3.4 The Trajectory of Emotional Intelligence: The Influence of Psychological Capital
In order to inspect the effect of PC on the path of EI, we use PC as a time-varying covariate to set up a model of condition. In this model, the first level model’s equation is: EISit = αi + βiλt + γtωit + ξit. ωit is the PC mark of subject i at time t, and γt is PC’s partial regression coefficient to EI at time t. The second level equation of the model is: αi = μα + γαxi + ξαi; β1i = μβ1 + γβ1xi + ξβ1i; β2i = μβ2 + γβ2xi + ξβ2i.
The result demonstrated the data suit the LGM acceptable, χ2(17)=15.35, p < 0.01, CFI = 0.94, RMSEA = 0.04. The mean intercept is 0.980, and the mean slope is 0.059, both of them are significant at the level of 0.001. It shows that both the starting level and participants’ rate of growth are significantly different. The intercept and slope’s correlation coefficient is −0.001 (p < 0.001). This result indicated a negative connection between the participants’ beginning condition and upward rate. More specifically, participants with a low score in the initial state would rise faster.
We also conducted an unconditional quadratic LGM to explore the influence of PC on the trajectory of EI. The result of data show, χ2(13) = 13.57, p < 0.01, CFI = 0.93, RMSEA = 0.05. The variance of intercept is 0.003 (p > 0.05), which shows that there is no significant individual difference in the initial level. Nevertheless, the variance of the slope is 0.007 (p < 0.05) and the linear slope variance is −0.001 (p < 0.001). It shows the growth rate between individuals is significantly different.
The aim of the present research was to explore whether the intervention of mindfulness training is a constructive method in improving adolescents’ EI and PC during the unique period filled with COVID-19 pandemic prevention measures in school after over a month of lockdown. The findings of this study are threefold.
First, as we expected in this study, EI and PC were significantly improved in the experimental group, whereas there was no significant improvement in the control group, as can be seen in Figs. 2A and 2B. This result implied that EI and PC were positively enhanced by mindfulness training, which is in line with previous studies on the relationship between mindfulness and emotions [42–44].
Second, in the experimental group, to explore the trajectory of EI and PC, we conducted models of unconditional linear LGM and unconditional quadratic LGM. Our finding is that for both EI and PC, the unconditional linear LGM fit better than the unconditional quadratic LGM. From the parameters of the unconditional linear LGM, the slope was significantly positive, indicating the upward tendency of EI and PC during the intervention and testing period.
Third, EI and PC are highly associated [24]. Both of them have a significant impact on an individual’s mental health [25,36,37]. Most of the existing studies have adopted a cross-sectional research design to reveal the relationship between these two variables. However, our study used a latent growth model to set PC as a variable factor to investigate its role in the development of EI. The results showed that in the process of altering EI, PC can affect the changes in EI at the time, and a higher PC can accelerate the improvement of EI to a certain extent. Our empirical research also proved the theory of Luthans et al. [24].
One explanation of EI being improved by mindfulness training may be that mindfulness moderates the reaction to stressful and negative emotions [45,46]. As we mentioned in the introduction, the definition of mindfulness is a conscious, nonjudgmental awareness of internal and external experiences that can be developed through practice [14]. When someone is practicing mindfulness, their emotions and cognition are more open and accepted [14,15]. Therefore, by practicing mindfulness, individuals adopt more efficient and adaptive coping and emotion regulation strategies [47], and their EI ability is improved. While practicing mindfulness, individuals’ proprioceptive awareness with respect to their emotions, thoughts, or even bodily postures is cultivated, which is important for relaxation in this process [43,44]. Moreover, being aware of breathing is also a vital part of mindfulness practice. By focusing on breathing, especially deep breathing, individuals may obtain feelings of relaxation from inside that extend to the body and mind [42]. During the COVID-19 pandemic, individuals with high EI may use efficient strategies to regulate negative emotions and therefore perceive less of a threat [8,48]. In addition, a previous study by Kotsou et al. [49] measured the overall diurnal profile of cortisol, which is a biological basis related to stress and negative emotion. They found that individuals with higher EI reported less stress. Thus, mindfulness training plays a protective role in improving EI and is one of the most prominent methods to help adolescents during the COVID-19 pandemic.
One reason that mindfulness training enhanced adolescents’ PC may be the psychological well-being of subjects’ was enhanced by the intervention of mindfulness practicing. A study by Luthans et al. [22] indicated psychological capital is highly related to psychological well-being. What’s more, based on the studies of [50,51], they confirmed that a high level of PC could control the negative effect of stress or mental health issues. Also, psychological well-being can positively influence the qualities of PC. Mindfulness can provoke positive emotion [52], which is beneficial for enhancing the psychological well-being of an individual [53].
The neurophysiological research on mindfulness and emotion indicated that by mindfulness, the activation of an individual’s left prefrontal brain area is enhanced, while the left prefrontal brain area can provoke positive emotion [52–54]. For instance, some studies of mindfulness using EEG technology test subjects’ brain electrical activity during mindfulness intervention, which they found increased the activation of the left prefrontal brain area while subjects were in the condition of mindfulness practicing [54]. Besides, based on the study of Barnhofer et al. [52], they found that in subjects with depression in the regular therapy group, their left prefrontal lobe activity decreased, marking the weakening of the positive emotion, accompanied by the worsening of depressive symptoms. However, in the group mindfulness therapy, symptoms of depression got better and was associated with increased activity of the left prefrontal lobe. Therefore, mindfulness increased PC by enhancing individuals’ activity of the left prefrontal lobe to promote their positive emotion and psychological well-being.
From our research, we can see that mindfulness training is also beneficial for improving the PC of adolescents. One possible explanation may be that psychological capital involves positive mental development [23,24], including self-efficacy, optimism, hope, and resilience. During mindfulness practice, individuals were encouraged to recognize and accept all feelings, whether they were positive, negative, or neutral [55–57]. By this means, mindfulness may reduce an individual’s negative patterns of cognition while increasing positive cognition and emotion patterns [19,58–60]. Thus, adolescents could develop a greater ability to perceive emotion in an acceptable way through this training, which is also beneficial for enhancing positive mental development and PC.
6 Contribution, Limitations, and Directions for Future Research
Studies have reported the passive impact of individuals’ mental health during the COVID-19 pandemic [11–13], and little is known about effective intervention methods for improving psychological health issues long-term. The present study proved that mindfulness intervention is an efficient method to enhance adolescents’ EI and PC during the COVID-19 pandemic, which provides a theoretical basis and future directions for both targeted crisis intervention and psychological trauma recovery plans.
Clearly, some limitations of this intervention should also be mentioned. First, we did not have a follow-up test after the mindfulness training intervention. In other words, we do not know whether EI and PC still trended upward after the intervention. Second, a growing amount of evidence has proven that there is a strong positive correlation between students’ EI and academic success [61,62]. Meanwhile, research on PC has also indicated that students with high PC experience better academic engagement and achievement than others [4,25,63,64]. Our study revealed that mindfulness training can increase adolescents’ EI and PC during the COVID-19 pandemic. Future research may investigate whether students’ academic achievement can be improved by means of mindfulness training.
Funding Statement: This research was funded by the Regional Science Fund Project of Northwest Normal University, Grant No. 31660281.
Conflicts of Interest: The authors declare that they have no conflicts of interest to report regarding the present study.
References
1. World Health Organization (2020). Mental health and psychosocial considerations during COVID-19 outbreak. World Health Organization. https://www.who.int/publications/i/item/WHO-2019-nCoV-MentalHealth-2020.1. [Google Scholar]
2. Holmes, E. A., O’Connor, R. C., Perry, V. H., Tracey, I., Wessely, S. et al. (2020). Multidisciplinary research priorities for the COVID-19 pandemic: A call for action for mental health science. The Lancet Psychiatry, 7(6), 547–560. DOI 10.1016/S2215-0366(20)30168-1. [Google Scholar] [CrossRef]
3. Cao, W., Fang, Z., Hou, G., Han, M., Xu, X. et al. (2020). The psychological impact of the COVID-19 epidemic on college students in China. Psychiatry Research, 287, 112934. DOI 10.1016/j.psychres.2020.112934. [Google Scholar] [CrossRef]
4. Liu, C., Zhao, Y., Tian, X., Zou, G., Li, P. (2015). Negative life events and school adjustment among Chinese nursing students: The mediating role of psychological capital. Nurse Education Today, 35, 754–759. DOI 10.1016/j.nedt.2015.02.002. [Google Scholar] [CrossRef]
5. McGinty, E. E., Presskreischer, R., Han, H., Barry, C. L. (2020). Psychological distress and loneliness reported by US adults in 2018 and April 2020. JAMA, 324(1), 93–94. DOI 10.1001/jama.2020.9740. [Google Scholar] [CrossRef]
6. Tang, W., Hu, T., Hu, B., Jin, C., Wang, G. et al. (2020). Prevalence and correlates of PTSD and depressive symptoms one month after the outbreak of the COVID-19 epidemic in a sample of home-quarantined Chinese University students. Journal of Affective Disorders, 274, 1–7. DOI 10.1016/j.jad.2020.05.009. [Google Scholar] [CrossRef]
7. Yue, Y. (2020). Mindfulness training on the resilience of adolescents under the COVID-19 epidemic: A latent growth curve analysis. Personality and Individual Differences, 1–9, 110560. DOI 10.1016/j.paid.2020.110560. [Google Scholar] [CrossRef]
8. Liang, L., Ren, H., Cao, R., Hu, Y., Qin, Z. et al. (2020). The effect of COVID-19 on youth mental health. Psychiatric Quarterly. DOI 10.1007/s11126-020-09744-3. [Google Scholar] [CrossRef]
9. Xie, X., Xue, Q., Zhou, Y., Zhu, K., Liu, Q. et al. (2020). Mental health status among children in home confinement during the coronavirus disease 2019 outbreak in Hubei Province, China. JAMA Pediatrics, 174(9), 898–900. DOI 10.1001/jamapediatrics.2020.1619. [Google Scholar] [CrossRef]
10. Crone, E. A., Achterberg, M., Dobbelaar, S., Euser, S., Bulk den van, B. et al. (2020). Neural and behavioral signatures of social evaluation and adaptation in childhood and adolescence: The Leiden consortium on individual development (L-CID). Developmental Cognitive Neuroscience, 45, 1–14. DOI 10.1016/j.dcn.2020.100805. [Google Scholar] [CrossRef]
11. Rogers, J. P., Chesney, E., Oliver, D., Pollak, T. A., McGuire, P. et al. (2020). Psychiatric and neuropsychiatric presentations associated with severe coronavirus infections: A systematic review and meta-analysis with comparison to the COVID-19 pandemic. The Lancet Psychiatry, 7(7), 611–627. DOI 10.1016/S2215-0366(20)30203-0. [Google Scholar] [CrossRef]
12. Wang, C., Pan, R., Wan, X., Tan, Y., Xu, L. et al. (2020). Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. International Journal of Environmental Research and Public Health, 17(5), 1729. DOI 10.3390/ijerph17051729. [Google Scholar] [CrossRef]
13. Qiu, J., Shen, B., Zhao, M., Wang, Z., Xie, B. et al. (2020). A nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: Implications and policy recommendations. General Psychiatry, 33(2), e100213. DOI 10.1136/gpsych-2020-100213. [Google Scholar] [CrossRef]
14. Kabatzinn, J. (1994). Wherever you go, there you are: Mindfulness meditation in everyday life. Behaviour Research and Therapy, 33, 996–996. [Google Scholar]
15. Bishop, S. R., Lau, M., Shapiro, S., Carlson, L., Anderson, N. D. et al. (2004). Mindfulness: A proposed operational definition. Clinical Psychology: Science and Practice, 11, 230–241. DOI 10.1093/clipsy.bph077. [Google Scholar] [CrossRef]
16. Ramel, W., Goldin, P. R., Carmona, P. E., McQuaid, J. R. (2004). The effects of mindfulness meditation on cognitive processes and affect in patients with past depression. Cognitive Therapy and Research, 28, 433–455. DOI 10.1023/B:COTR.0000045557.15923.96. [Google Scholar] [CrossRef]
17. Goldin, P., Ramel, W., Gross, J. (2009). Mindfulness meditation training and self-referential processing in social anxiety disorder: Behavioral and neural effects. Journal of Cognitive Psychotherapy, 23(3), 242–257. DOI 10.1891/0889-8391.23.3.242. [Google Scholar] [CrossRef]
18. Slagter, H. A., Lutz, A., Greischar, L. L., Nieuwenhuis, S., Davidson, R. J. (2008). Theta phase synchrony and conscious target perception: Impact of intensive mental training. Journal of Cognitive Neuroscience, 21(8), 1536–1549. DOI 10.1162/jocn.2009.21125. [Google Scholar] [CrossRef]
19. Garland, E. L., Hanley, A. W., Goldin, P. R., Gross, J. J. (2017). Testing the mindfulness-to-meaning theory: Evidence for mindful positive emotion regulation from a reanalysis of longitudinal data. PLoS One, 12(12), e0187727. DOI 10.1371/journal.pone.0187727. [Google Scholar] [CrossRef]
20. Chambers, R., Gullone, E., Allen, N. B. (2009). Mindful emotion regulation: An integrative review. Clinical Psychology Review, 29(6), 560–572. DOI 10.1016/j.cpr.2009.06.005. [Google Scholar] [CrossRef]
21. Jimenez, S. S., Niles, B. L., Park, C. L. (2010). A mindfulness model of affect regulation and depressive symptoms: Positive emotions, mood regulation expectancies, and self-acceptance as regulatory mechanisms. Personality and Individual Differences, 49(6), 645–650. DOI 10.1016/j.paid.2010.05.041. [Google Scholar] [CrossRef]
22. Luthans, F., Avolio, B. J., Avey, J. B., Norman, S. M. (2007). Positive psychological capital: Measurement and relationship with performance and satisfaction. Personnel Psychology, 60(3), 541–572. DOI 10.1111/j.1744-6570.2007.00083.x. [Google Scholar] [CrossRef]
23. Luthans, F., Youssef, C. M., Avolio, B. J. (2007a). Psychological capital: Developing the human competitive edge. Journal of Asian Economics, 8, 315–332. [Google Scholar]
24. Luthans, F., Youssef, C. M., Avolio, B. J. (2007b). Psychological capital: Developing the human competitive edge. New York, NY, USA: Oxford University Press. [Google Scholar]
25. Ahmed, U., Umrani, W. A., Qureshi, M. A., Samad, A. (2018). Examining the links between teachers support, academic efficacy, academic resilience, and student engagement in Bahrain. International Journal of Advanced and Applied Sciences, 5, 39–46. DOI 10.21833/ijaas.2018.09.008. [Google Scholar] [CrossRef]
26. Zhang, R., Ewalds-Kvist, B. M., Li, D., Jiang, J. (2019). Chinese students’ satisfaction with life relative to psychological capital and mediated by purpose in life. Current Psychology, 38, 260–271. DOI 10.1007/s12144-018-9849-z. [Google Scholar] [CrossRef]
27. Datu, J. A. D., King, R. B., Valdez, J. P. M. (2016). Psychological capital bolsters motivation, engagement, and achievement: Cross-sectional and longitudinal studies. The Journal of Positive Psychology, 13(3), 260–270. DOI 10.1080/17439760.2016.1257056. [Google Scholar] [CrossRef]
28. Xiang, Y. T., Yang, Y., Li, W., Zhang, L., Zhang, Q. et al. (2020). Timely mental health care for the 2019 novel coronavirus outbreak is urgently needed. The Lancet Psychiatry, 7(3), 228–229. DOI 10.1016/S2215-0366(20)30046-8. [Google Scholar] [CrossRef]
29. Salovey, P., Mayer, J. D. (1990). Emotional intelligence. Imagination, Cognition and Personality, 9(3), 185–211. DOI 10.2190/DUGG-P24E-52WK-6CDG. [Google Scholar] [CrossRef]
30. Goleman, D. (1996). Emotional intelligence: Why it can matter more than IQ. New York: Bantam Books. [Google Scholar]
31. Bar-On, R. (2006). The bar-on model of emotional-social intelligence (ESI). Psicothema, 18, 13–25. [Google Scholar]
32. Mayer, J. D., Salovey, P. (1997). What is emotional intelligence? In: Salovey, P., Sluyter, D. J. (EdsEmotional development and emotional intelligence: Educational implications, pp. 3–31. New York, NY: Basic Books. [Google Scholar]
33. Guti´errez-Cobo, M. J., R., C., Fernandez-Berrocal, P. (2017). The three models of emotional intelligence and performance in a hot and cool go/no-go task in undergraduate students. Frontiers in Behavioral Neuroscience, 11, 33. DOI 10.3389/fnbeh.2017.00033. [Google Scholar] [CrossRef]
34. Mayer, J. D., Salovey, P., Caruso, D. R. (2000). Competing models of emotional intelligence. In: Sternberg, I. R. J. (EdHandbook of human intelligence, pp. 396–420. New York: Cambridge University Press. [Google Scholar]
35. Mayer, J. D., Caruso, C. D. R., Salovey, P. (2016). The ability model of emotional intelligence: Principles and updates. Emotion Review, 8(4), 290–300. DOI 10.1177/1754073916639667. [Google Scholar] [CrossRef]
36. Mavroveli, S., Petrides, K. V., Rieffffe, C., Bakker, F. (2007). Trait emotional intelligence, psychological well-being and peer-rated social competence in adolescence. British Journal of Developmental Psychology, 25(2), 263–275. DOI 10.1348/026151006X118577. [Google Scholar] [CrossRef]
37. Kat, D., Luke, D., Justine, L., Emily, R. B., Nathan, S. et al. (2019). Differentiating the contributions of emotional intelligence and resilience on adolescent male scholastic performance. Personality and Individual Differences, 145, 75–81. DOI 10.1016/j.paid.2019.03.023. [Google Scholar] [CrossRef]
38. Downey, L., Mountstephen, J., Lloyd, J., Hansen, K., Stough, C. (2008). Emotional intelligence and scholastic achievement in Australian adolescents. Australian Journal of Psychology, 60(1), 10–17. DOI 10.1080/00049530701449505. [Google Scholar] [CrossRef]
39. Pekrun, R., Elliot, A. J., Maier, M. A. (2009). Achievement goals and achievement emotions: Testing a model of their joint relations with academic performance. Journal of Educational Psychology, 101(1), 115–135. DOI 10.1037/a0013383. [Google Scholar] [CrossRef]
40. Muthén, B., Muthén, L. K. (1998–2019). Mplus user’s guide (7th ed.). Los Angeles, CA: Muthén & Muthén. [Google Scholar]
41. Browne, M., Cudeck, R. (1992). Alternative ways of assessing model fit. Sociological Methods & Research, 21, 230–258. DOI 10.1177/0049124192021002005. [Google Scholar] [CrossRef]
42. Gu, J., Strauss, C., Bond, R., Cavanagh, K. (2015). How do mindfulness-based cognitive therapy and mindfulness-based stress reduction improve mental health and wellbeing? A systematic review and meta-analysis of mediation studies. Clinical Psychology Review, 37, 1–12. DOI 10.1016/j.cpr.2015.01.006. [Google Scholar] [CrossRef]
43. Roy, A., Druker, S., Hoge, E. A., Brewer, J. A. (2020). Physician anxiety and burnout. symptom correlates and a prospective pilot study of app-delivered mindfulness training. JMIR mHealth uHealth, 8(4), e15608. DOI 10.2196/15608. [Google Scholar] [CrossRef]
44. Spijkerman, M. P. J., Pots, W. T. M., Bohlmeijer, E. T. (2016). Effectiveness of online mindfulness-based interventions in improving mental health: A review and meta-analysis of randomised controlled trials. Clinical Psychology Review, 45, 102–114. DOI 10.1016/j.cpr.2016.03.009. [Google Scholar] [CrossRef]
45. Mikolajczak, M., Luminet, O. (2008). Trait emotional intelligence and the cognitive appraisal of stressful events: An exploratory study. Personality and Individual Differences, 44(7), 1445–1453. DOI 10.1016/j.paid.2007.12.012. [Google Scholar] [CrossRef]
46. Mikolajczak, M., Nelis, D., Hansenne, M., Quoidbach, J. (2008). If you can regulate sadness, you can probably regulate shame: Associations between trait emotional intelligence, emotion regulation and coping efficiency across discrete emotions. Personality and Individual Differences, 44(6), 1356–1368. DOI 10.1016/j.paid.2007.12.004. [Google Scholar] [CrossRef]
47. Ruiz-Aranda, D., Extremera, N., Pineda-Galán, C. (2014). Emotional intelligence, life satisfaction and subjective happiness in female student health professionals: The mediating effect of perceived stress. Journal of Psychiatric and Mental Health Nursing, 21(2), 106–113. DOI 10.1111/jpm.12052. [Google Scholar] [CrossRef]
48. Marcin, M., Magdalena, B. M. (2020). Trait emotional intelligence and emotional experiences during the COVID-19 pandemic outbreak in Poland: A daily diary study. Personality and Individual Differences, 168, 110348. DOI 10.1016/j.paid.2020.110348. [Google Scholar] [CrossRef]
49. Kotsou, I., Nelis, D., Grégoire, J., Mikolajczak, M. (2011). Emotional plasticity: Conditions and effects of improving emotional competence in adulthood. Journal of Applied Psychology, 96(4), 827–839. DOI 10.1037/a0023047. [Google Scholar] [CrossRef]
50. Jain, A. K., Giga, S. I., Cooper, C. L. (2013). Stress, health and well-being: The mediating role of employee and organizational commitment. International Journal of Environmental Research and Public Health, 10 (10), 4907–4924. DOI 10.3390/ijerph10104907. [Google Scholar] [CrossRef]
51. Koller, S. L., Hicks, R. E. (2016). Psychological capital qualities and psychological wellbeing in Australian mental health professionals. International Journal of Psychological Studies, 8(2), 41–53. DOI 10.5539/ijps.v8n2p41. [Google Scholar] [CrossRef]
52. Barnhofer, T., Duggan, D., Crane, C., Hepburn, S., Fennell, M. J. V. et al. (2007). Effects of meditation on frontal alpha-asymmetry in previously suicidal individuals. Neuroreport, 18(7), 709–812. DOI 10.1097/WNR.0b013e3280d943cd. [Google Scholar] [CrossRef]
53. Chan, A. S., Han, Y. M. Y., Cheung, M. C. (2008). Electroencephalographic (EEG) measurements of mindfulness-based triarchic body-pathway relaxation technique: A pilot study. Applied Psychophysiology and Biofeedback, 33(1), 39–47. DOI 10.1007/s10484-008-9050-5. [Google Scholar] [CrossRef]
54. Davidson, R. J., Kabat-Zinn, J., Schumacher, J., Rosenkranz, M., Muller, D. et al. (2003). Alterations in brain and immune function produced by mindfulness meditation. Psychosomatic Medicine, 65, 564–570. DOI 10.1097/01.PSY.0000077505.67574.E3. [Google Scholar] [CrossRef]
55. Hargus, E., Crane, C., Barnhofer, T., Williams, J. M. G. (2010). Effects of mindfulness on meta-awareness and specificity of describing prodromal symptoms in suicidal depression. Emotion, 10(1), 34–42. DOI 10.1037/a0016825. [Google Scholar] [CrossRef]
56. Michalak, J., Hölz, A., Teismann, T. (2011). Rumination as a predictor of relapse in mindfulness-based cognitive therapy for depression. Psychology and Psychotherapy: Theory. Research and Practice, 84(2), 230–236. DOI 10.1348/147608310X520166. [Google Scholar] [CrossRef]
57. Shahar, B., Britton, W. B., Sbarra, D. A., Figueredo, A. J., Bootzin, R. R. (2010). Mechanisms of change in mindfulness-based cognitive therapy for depression: Preliminary evidence from a randomized controlled trial. International Journal of Cognitive Therapy, 3(4), 402–418. DOI 10.1521/ijct.2010.3.4.402. [Google Scholar] [CrossRef]
58. van den Hurk, P. A. M., van Aalderen, J. R., Giommi, F., Donders, R. A. R. T., Barendregt, H. P. et al. (2012). An investigation of the role of attention in mindfulness-based cognitive therapy for recurrently depressed patients. Journal of Experimental Psychopathology, 3(1), 103–120. DOI 10.5127/jep.024811. [Google Scholar] [CrossRef]
59. Geschwind, N., Peeters, F., Drukker, M., van Os, J., Wichers, M. (2011). Mindfulness training increases momentary positive emotions and reward experience in adults vulnerable to depression: A randomized controlled trial. Journal of Consulting and Clinical Psychology, 79(5), 618–628. DOI 10.1037/a0024595. [Google Scholar] [CrossRef]
60. Segal, Z. V., Williams, J. M. G., Teasdale, J. D. (2013). Mindfulness-based cognitive therapy for depression. In: A new approach to preventing relapse, New York: Guilford Press. [Google Scholar]
61. Costa, A., Faria, L. (2015). The impact of emotional intelligence on academic achievement: A longitudinal study in Portuguese secondary school. Learning and Individual Differences, 37, 38–47. DOI 10.1016/j.lindif.2014.11.011. [Google Scholar] [CrossRef]
62. Perera, H. N., DiGiacomo, M. (2015). The role of trait emotional intelligence in academic performance during the university transition: An integrative model of mediation via social support, coping, and adjustment. Personality and Individual Differences, 83, 208–213. DOI 10.1016/j.paid.2015.04.001. [Google Scholar] [CrossRef]
63. Liu, C. H., Zhang, E., Wong, G., Hyun, S., Hahm, H. C. (2020). Factors associated with depression, anxiety, and PTSD symptomatology during the COVID-19 pandemic: Clinical implications for U.S. young adult mental health. Psychiatry Research, 290, 113172. DOI 10.1016/j.psychres.2020.113172. [Google Scholar] [CrossRef]
64. Jha, A. P., Denkova, E., Zanesco, A. P., Witkin, J. E., Rooks, J. et al. (2019). Does mindfulness training help working memory “work” better? Current Opinion in Psychology, 28, 273–278. DOI 10.1016/j.copsyc.2019.02.012. [Google Scholar] [CrossRef]
 | This work is licensed under a Creative Commons Attribution 4.0 International License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. |