| International Journal of Mental Health Promotion |
DOI: 10.32604/ijmhp.2022.013177
REVIEW
Psychological Impacts of Coronavirus Outbreaks on Adults: A Rapid Evidence Review
1Faculty of Education, Monash University, Clayton, Melbourne, Victoria, 3800, Australia
2School of Health and Biomedical Sciences, College of Science, Engineering and Health, RMIT University, Melbourne, Bundoora, 3083, Australia
*Corresponding Author: Emily Berger. Email: emily.berger@monash.edu
Received: 24 August 2021; Accepted: 17 November 2021
Abstract: A recent rapid review highlighted the negative psychological impacts of quarantining during coronavirus outbreaks on the public. However, to date, there has been no review of the psychological impacts of coronavirus on adults using research from community samples and not restricted to people quarantined during coronavirus. A rapid review was conducted to provide timely evidence about the mental health implications of coronavirus outbreaks on adults and to inform psychological research concerning the current COVID-19 outbreak. Three databases and Google Scholar were searched and a total of 27 studies were identified. Symptoms of anxiety and depression were identified during coronavirus outbreaks alongside concerns about becoming infected and family becoming infected. Those with pre-existing mental health conditions, young adults, women and those reporting physical symptoms appear to be vulnerable to negative psychological outcomes during coronavirus outbreaks. How people think about and understand coronavirus, and the coping strategies employed by people, may play a role in mitigating negative psychological outcomes. Results demonstrate the adverse psychological impacts of coronavirus outbreaks on adults and the need for continued investment in mental health services for the wider community during these times. Further longitudinal research is required to ascertain the long-term psychological consequences of coronavirus outbreaks. This review can be used to inform continued research on the psychological impacts of COVID-19 on adults.
Keywords: Coronavirus; outbreak; adults; psychological impact; COVID-19
In response to the 2019 outbreak of COVID-19, a rapid review on the psychological impacts of quarantine on children and adults found “wide-ranging, substantial, and … long-lasting” effects of being quarantined [1]. In this rapid review, Brooks et al. [1] specifically explored the psychological impacts of quarantining during outbreaks and found increased symptoms of posttraumatic stress, confusion and anger among adults. Another review highlighted the negative impact of an outbreak on SARS survivors [2], but did not consider the impact of SARS on the general public. Health care workers are also adversely impacted; Kang et al. [3] found practitioners in Wuhan, China, reported increased levels of anxiety and distress as a result of dealing with COVID-19. Consequently, leading mental health organisations and media outlets worldwide have rushed to provide practical and psychological guidance as to how services, schools, and healthcare providers can respond to people during the COVID-19 crisis. An example of this innovation is the application of E-Rehabilitation and telehealth services for adults with mental or physical health concerns [4,5]. This rapid review was conducted to identify and synthesise the evidence regarding the psychological impacts of coronavirus on adults in the general community (including COVID-19, MERS [Middle East Respiratory Syndrome], and SARS [Severe Acute Respiratory Syndrome]). No known review to date has been conducted with this specific focus. These results can be used to guide the general public and inform the response of governments, mental health organisations, and the media regarding the mental health needs of the public during the current COVID-19 outbreak.
2.1 Search Strategy and Selection Criteria
We combined the key words of psych*, COVID-19, SARS, MERS, outbreak, infection, and coronavirus to search PubMed, PsycINFO, and Embase electronic databases. We broadened the search to adults in general since earlier reviews have already reported on the psychological impacts among quarantined people [1] and SARS survivors [2]. The methodology for this paper followed that of the recent rapid review conducted by Brooks et al. [1] and the rapid review methodology was selected as the best approach for timely synthesis of the coronavirus evidence for ongoing research into COVID-19 [6].
The eligibility criteria for inclusion in this review were: (1) Population: General population of adults (excluding studies focusing exclusively on patient groups and healthcare workers); (2) Behaviour: Preventive, avoidant, or management of pandemic disease behaviours; (3) Psychological: Perceived risk of pandemic, general psychological distress, or psychiatric disorder; and (4) Date: Published after 2002 (when SARS emerged as a pandemic).
A total of 1785 records were identified through database searching including Google Scholar searches. After deduplication, the remaining 1096 records were subject to title and abstract screening. A final 27 studies were deemed eligible according to the inclusion criteria for this review (see Fig. 1).
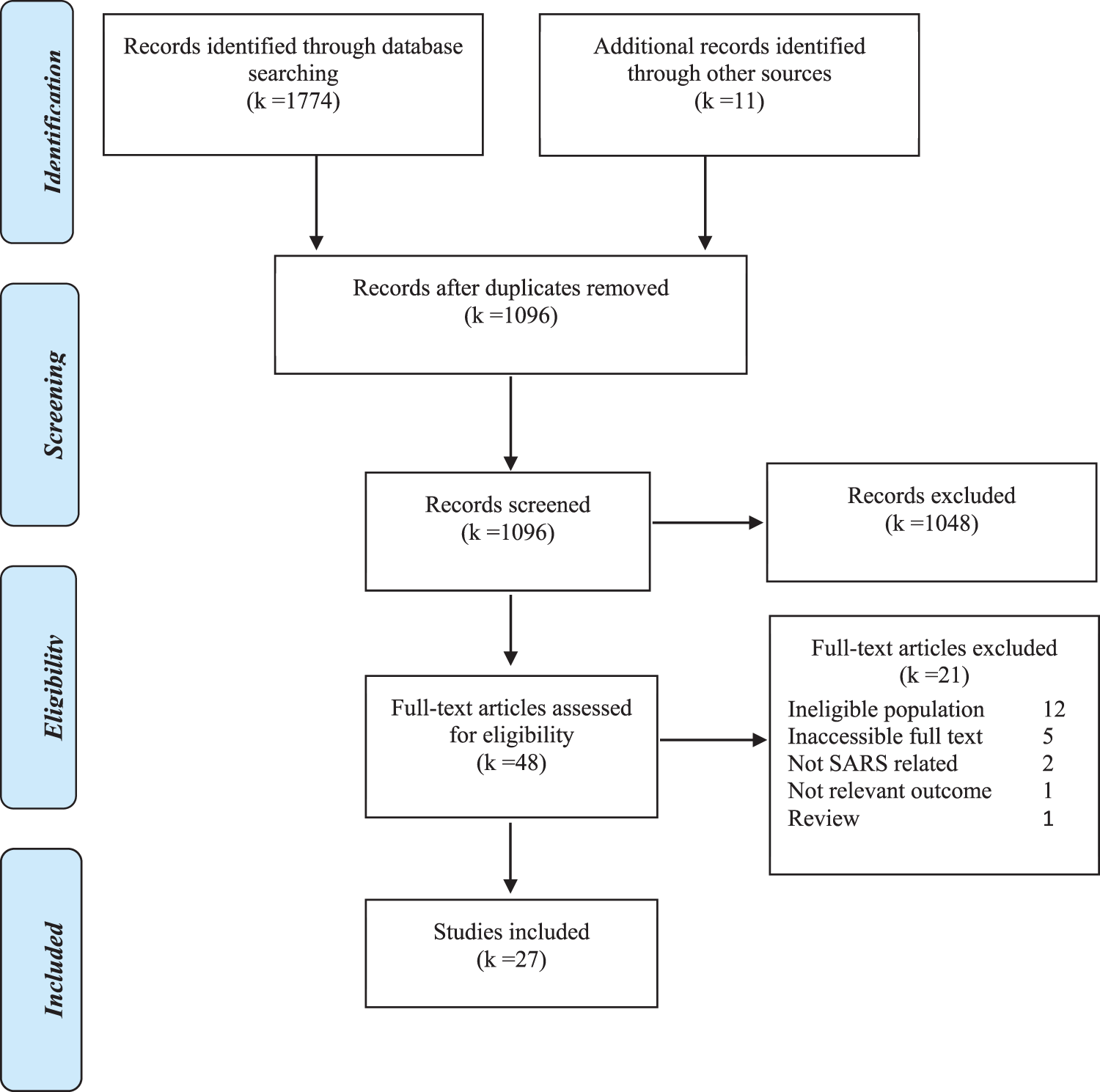
Figure 1: Study flow diagram
The characteristics of included studies are summarised in Table 1. There were two studies related to psychological outcomes associated with MERS, four with COVID-19, and 21 with the SARS outbreak. Ten studies were set in Hong Kong, nine in China, two in Singapore, one each in Saudi Arabia and Korea and another in New York exclusively. There were an additional three studies that compared population groups between countries, one between the USA and Canada, and another two between Hong Kong and Singapore. Most studies (k = 21) recruited participants from the general public, while three included university students, and one sampled older residents. One study compared SARS patients with a healthy control group from the public, and another compared the general public and university students. Two studies focused on particular subgroups including pregnant women and women attending antenatal clinics, and another which included participants involved in a cardiovascular risk study.

Symptoms of anxiety and depression were observed in the general community during the SARS and COVID-19 outbreaks [24,28,29,32]. Posttraumatic stress symptoms were reported in relation to SARS [15,28]. Public concern centred on contraction or family contraction of coronavirus [14,17,29]. Studies showed levels of anxiety fluctuated over the course of the SARS outbreak [9]. Lau et al. [14] found worry and fear about contraction decreased from the initial stages to the middle stages of the SARS outbreak. Blendon et al. [8] found the Canadian and USA public experienced anxiety due to SARS outbreak, but that anxiety declined during the course of the outbreak. In Lai’s [13] study, depression in men and women returned to pre-pandemic levels after the SARS outbreak.
Emotional reactions of stress, anger and sadness were reported across several studies [10,29,31]. Lau et al. [15] found adults experienced feelings of helplessness and horror regarding the SARS outbreak. Feelings of loneliness and social isolation were found in the study by Lee et al. [17], as well as panic, nervousness and fear regarding the SARS outbreak reported in the study by Zhu and colleagues [33].
Event-related distress differed between younger and older adults. Sim et al. [28] reported adults of a younger age (not specified) experienced heightened psychological distress as a result of SARS compared to older adults. Yeung et al. [31] found younger people were more likely than older people to express anger regarding the SARS outbreak, though older people expressed more sadness. Subjective wellbeing was lower but community connectedness found to be greater in older people during the SARS outbreak [16]. Females compared to males were at greater risk of psychological distress related to SARS and COVID-19 [11,13,20,29].
3.3 Mental or Physical Disease
People also at risk of poor psychological health during the SARS outbreak were found to be those who had experienced depression or a psychiatric condition prior to the SARS outbreak [11,28]. In addition, Wang et al. [29] found people experiencing physical symptoms and those with poor self-rated health reported increased levels of stress, anxiety and depression in the beginning to the middle stages of COVID-19.
Several studies found increased use of precautionary measures among members of the public with greater anxiety about contracting SARS or MERS (e.g., wearing masks, staying away from public places [7,18,27,28]. Conversely, Wang et al. [29] found having access to information and engaging in health protective behaviours lowered stress, anxiety and depression among adults during COVID-19. Thus, from existing research it is unclear whether engaging in precautionary measures during outbreaks lowers anxiety or whether anxiety in and of itself leads to an increase in precautionary behaviour.
Another potentially mitigating factor for psychological outcomes was proximity to coronavirus cases. One study found living in regions with less (not more) cases of coronavirus was associated with heightened anxiety [30]. In other studies, higher SARS exposure and living in high risk epidemic areas was associated with greater anxiety and lowered subjective wellbeing [10,12,16]. Again, results are inconclusive regarding the role of proximity in determining adults’ mental health during coronavirus outbreaks.
How one thinks about and perceives an outbreak appears to plays a role in psychological outcomes. Qian et al. [26] and Xie et al. [30] found perceived susceptibility of contracting COVID-19 and subjective interpretations about SARS increased anxiety of adults. Similarly, acceptance of the pandemic experience was associated with psychological health during the SARS outbreak; studies finding that over time people tended to feel less threatened and more accepting of their circumstances surrounding the outbreak [14,25]. Qian et al. [25] suggested that this might be because “the students [university students] could endure and/or accept living with SARS. When shocked by SARS, they might assess their circumstances and the disease to be more severe than it really was” (p. 95). Their negative cognitions about the outbreak went down every week, even though there were still high cases of SARS in the community.
The same study compared two college samples in Beijing (which was heavily impacted by SARS) and Suzhou (where only one case was found); while citizens in both areas faced strict restrictions, restraints were more severe in Beijing. Nonetheless, the Suzhou subsample had more negative emotions in the first and second week than in the fourth week. The authors suggest that initially the Suzhou public were concerned that the number of SARS cases would increase; when no cases were reported, students returned back to their pre-disaster level of psychological functioning quicker [25]. In sum, Qian et al. [25] reported that the “cognitions of SARS played a mediating role between the external stress and other psychological responses (p. 96).”
Qian et al. [26] found confusion about coronavirus predicted anxiety while confidence to protect oneself lowered anxiety. Likewise, Wang et al. [29] found accurate information about COVID-19 lowered psychological distress, anxiety, stress and depression. Zhu et al. [33] found 84% of their community sample wanted more information about SARS and it was concluded that “the uncertainty people have about the epidemic development was a key cause of panic during this time” (p. 447).
A major source of knowledge is the media, with some research finding that how information is portrayed in the media impacts psychological health. Blendon et al. [8] found the proportion of the USA population who described themselves as concerned about SARS increased when they were told that people in Asia and Canada had died from the virus [8]. Xie et al. [30] pointed out that there was “disproportionate attention placed on reporting cases of SARS (a person who contracts SARS is more newsworthy than is someone who does not contract SARS)” (p. 1104). They continued by arguing that “living in the center of the epidemic would have provided a method for obtaining more SARS-related knowledge than would obtaining information only from media reports” (p. 1104).
Another potentially mitigating factor for psychological outcomes is coping. Greater use of avoidant coping strategies (e.g., denial, disengagement) predicted negative psychological symptoms in Chinese university students during the SARS outbreak [24]. However, active forms of coping (e.g., planning, problem solving) did not relate to psychological outcomes of this sample. In comparison, denial and planning were coping strategies observed in adults experiencing posttraumatic stress [28]. Chinese university students living in more exposed regions of SARS outbreaks were observed in another study to engage in greater use of coping behaviours (type of coping not clearly defined), however these coping behaviours did not decrease participants’ negative emotions [25]. After the SARS outbreak, poor psychological outcomes were associated with self-blame and interestingly, less use of substances [28].
Young adults were found by Yeung et al. [31] to employ more emotion-focused coping than middle-aged adults, but only at the peak of the outbreak, and this difference was not sustained throughout the outbreak period. Across all age groups, those who employed emotion-focused coping reported decreased anger and sadness, while use of problem-focused coping reduced sadness for older adults [31]. During the SARS outbreak, high community connectedness mitigated the risks of reduced wellbeing, depression and anxiety among adults [9,16].
This review highlights the adverse psychological impacts of coronavirus outbreaks on adults in the general population and the various factors that potentially mitigate these negative psychological health effects for adults. Feelings of anxiety, depression and posttraumatic stress were commonly reported by adults during coronavirus outbreaks [7,28,29]. Seven studies were conducted over the course of the outbreak being researched and subsequently these studies were able to document changes in people’s psychological reactions and cognitive appraisal of the unfolding circumstances. In these studies, researchers observed an increase in anxiety and distress followed by a decrease in anxiety and distress, from the earlier to the end stages of the outbreak, or after the outbreak had ceased [13–14,21]. Lai [13] found depression scores returned to pre-pandemic levels one month after the SARS outbreak. It is possible that people are able to return to their pre-pandemic functioning after the risk of contraction has passed, however most studies were cross sectional and few provided extensive longitudinal data; the maximum length of time after the outbreak that data were collected was six months.
Various demographic groups appear to be particularly vulnerable to adverse psychological outcomes, including those experiencing physical symptoms and those with poor self-rated physical health [29]. Those with pre-existing mental health issues, women and younger adults also appeared to be more vulnerable than other groups in the community to anxiety and other psychological concerns [11–13,21,26,16]. These groups might be particular targets for early psychological intervention and supports during outbreaks.
The results are inconclusive regarding the association between use of precautionary behaviours, such as wearing of masks and staying away from public places and anxiety. Some found a positive association between the two [7,18,27,28], however, Wang et al. [29] found the reverse; engaging in precautionary behaviours was associated with lower stress, anxiety and depression. Likewise, the results regarding the association between proximity to the pandemic and mental illness is unclear. Other factors may well be influencing these results.
What people know and think about coronavirus appears to be an important factor when determining mental health outcomes. Xie et al. [30] found anxiety was greater for members of the public living in areas that were considered objectively better (less cases of SARS). According to the researchers, most people who lived closer to the SARS outbreak had, over time, considered the risk was reduced while those living away from immediate cases of SARS relied on the media to inform what they knew and thought about the outbreak and this increased distress levels [30]. Thus, higher exposure is not a sufficient explanation for the negative psychological impacts of virus outbreaks and research on the mental health effects of COVID-19 among high and low infected communities is required.
How people think about coronavirus and the information that is publicly available is potentially more important to social functioning, mental health and wellbeing than the frequency of contraction and severity of pandemics [25,30]. Awareness and understanding of COVID-19 can be due to direct exposure (i.e., being ill or having a family member who is ill) or indirect exposure as occurs through the media. To illustrate, Blendon et al. [8] referred to the “double-edged sword” of the media, in which the media helps people to prevent the spread of a pandemic, but also increases the anxiety of people who are not at high risk of contraction due to their geographical location. This research demonstrates that the spread of psychological distress due to coronavirus is not always proportional to the physical threat caused by the virus. Again, this points to the need for more research among less impacted communities as a result of COVID-19, as well as therapeutic and media reporting approaches that seek to minimise inaccurate interpretations of people about COVID-19 and the potential risks.
The results are unclear as to the types of coping strategies that best serve people during outbreaks. Coping is defined as efforts to deal with demands taxing or exceeding an individual’s resources [3] and is typically considered as a cognitive or behavioral response to something appraised as stressful. Again, underscoring the role of cognition and subjective interpretations of coronavirus, coping occurs in response to the way an event is perceived (subjective apprasial) rather than objective characteristics of the situation response [3]. Perhaps not unexpectantly, avoidant coping, involving denial of the outbreak, appears to be related to poor psychological symptoms [24]. Drawing on the broader coping literature, there is an argument that both problem-focused and emotion-focused coping may be beneficial to one’s mental health [34,35]. Problem-focused coping is aimed at resolving or altering the stressful event and typically involves efforts to remove the source of the stress or seeking information or assistance in handling the situation [3] (in the context of pandemics this could be related to engaging in precautionary behaviours). In comparison, emotion-focused coping aims to ameliorate “the negative emotions associated with the problem,” [3] (p. 751), for example, seeking support from friends and family or expressing feelings of worry or distress. In a coronavirus outbreak, emotional focused coping may consist of connecting with others [9,36] and allowing people to express their anxiety about the event. Results of this review and earlier literature points towards the need to encourage people to engage in more problem- and emotion-focused coping (and cognitive reappraisal) around COVID-19. These findings have clear implications for both mental health practitioners, the government and the media regarding how people should be instructed to maintain good mental health during COVID-19 and future pandemics.
The results of this review prompt a number of implications and recommendations for practitioners, the government and media:
1. How the media (traditional and social) and the government portray and explain COVID-19 is critical, as this will shape the way the public understands the pandemic and reacts. Messages need to be clear and consistent to avoid confusion and reduce distress.
2. As well as providing accurate information, media and governments should describe the precautionary behaviours that the community need to engage in and at the same time report on recovery rates, rather than focusing solely on death rates. This may serve to promote more adaptive cognitions along with positive psychological health.
3. Government messages should include information about how people can live through the outbreak (and periodic increases in infection rates) and the possible mental health issues and distress people may experience (e.g., sadness, stress, loneliness). Hopeful messages can be given to the public regarding the likelihood of their distress passing after the pandemic.
4. Psychological services play a role in helping people adjust their negative cognitions and employ problem- and emotion-focused coping strategies. Coping strategies of connecting with others and cognitive reappraisal (to increase objective interpretations of the unfolding circumstances) are shown to be important. However, it is possible that social distancing measures and quarantining as a result of COVID-19 have reduced people’s access to social and professional support. The coping strategies employed by people during COVID-19 and the potential impact of reduced access to formal and informal support is an area requiring more research.
5. Psychological and psychiatric personnel should be given an official platform through the media to communicate ways that people can adaptively cope and adjust to the changing circumstances around COVID-19. Psychological services appear to be more important during the outbreak and these services may subsequently be reduced as people adjust back to life after the pandemic.
6. Health practitioners require measures for assessing the psychological impact of the COVID-19 outbreak on adults, monitoring the potential for ongoing impacts and directing people to mental health services. This might involve an assessment or screening by mental health practitioners, including asking people about their knowledge about the outbreak and perceived susceptibility to contraction (and other subjective interpretations), in order to identify those at risk of experiencing heightened anxiety as a result of the outbreak.
There are a few limitations to note in relation to this review. Firstly, while this rapid review employed a systematic review procedure, this review was not a systematic review and therefore some important studies may have been missed. Similar rapid and systematic reviews in this area will be important as the literature surrounding COVID-19 increases. Furthermore, this review identified several limitations of the coronavirus literature, including the lack of longitudinal follow up with participants to observe the long-term implications of coronavirus on mental health. Other factors which should be included in future COVID-19 research may include comparisons of people from areas with high infection rates and lower infection rates, comparisons of districts with different public health measures in response to COVID-19, and research comparing countries with different morbidity and mortality rates from infection.
It is important to note that many of these mental health impacts were observed among those who were not directly impacted by the infectious diseases. As many measures attempt to control the spread of infectious diseases, the issue of mental and psychological health during and following such outbreaks requires greater attention. Given the lack of ongoing research in this area, longitudinal outcomes of coronavirus outbreaks is required in the months and years after an outbreak. Further research is also required comparing countries and regions with different contraction rates and government responses and how subjective interpretations relate to psychological wellbeing and recovery in adults after coronavirus outbreaks. In addition, few studies used diagnostic measurements and future studies will need to do so in order to obtain accurate prevalence rates of psychiatric disorders, including disorder severity and chronicity.
Living through an epidemic or pandemic can have negative mental health consequences for adults. What the public knows and thinks about coronavirus and the coping strategies employed appear to play a key role in determining mental health outcomes. The findings in this review have implications for the media and research regarding the current COVID-19 outbreak, as well as for psychological and community services during pandemic outbreaks.
Funding Statement: The authors received no specific funding for this study.
Conflicts of Interest: The authors declare that they have no conflicts of interest to report regarding the present study.
References
1. Brooks, S. K., Webster, R. K., Smith, L. E., Woodland, L., Wessely, S. et al. (2020). The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. The Lancet, 395, 912–920. [Google Scholar]
2. Gardner, P. J., Moallef, P. (2015). Psychological impact on SARS survivors: Critical review of the English language literature. Canadian Psychology/Psychologie Canadienne, 56(1), 123–135. [Google Scholar]
3. Kang, L., Li, Y., Hu, S., Chen, M., Yang, C. et al. (2020). The mental health of medical workers in Wuhan, China dealing with the 2019 novel coronavirus. The Lancet. Psychiatry, 7(3), e14. [Google Scholar]
4. Berger, E., Reupert, A. (2020). The COVID-19 pandemic in Australia: Lessons learnt. Psychological Trauma: Theory, Research, Practice and Policy, 12(5), 494–496. [Google Scholar]
5. Srivastav, A. K., Samuel, A. J. (2020). E-rehabilitation: One solution for patients with Parkinson’s disease in COVID-19 era. Parkinsonism & Related Disorders, 75, 128–129. [Google Scholar]
6. Hartling, L., Guise, J. M., Hempel, S., Featherstone, R., Mitchell, M. D. et al. (2017). Fit for purpose: Perspectives on rapid reviews from end-user interviews. Systematic Reviews, 6(1), 32. [Google Scholar]
7. AlNajjar, N. S., Attar, L. M., Farahat, F. M., AlThaqafi, A. (2017). Psychobehavioural responses to the 2014 Middle East respiratory syndrome-novel corona virus (MERS CoV) among adults in two shopping malls in Jeddah, Western Saudi Arabia. Eastern Mediterranean Health Journal, 22(11), 817–823. [Google Scholar]
8. Blendon, R. J., Benson, J. M., DesRoches, C. M., Raleigh, E., Taylor-Clark, K. (2004). The public’s response to severe acute respiratory syndrome in toronto and the United States. Clinical Infectious Diseases, 38(7), 925–931. [Google Scholar]
9. Cheng, C., Cheung, M. W. (2005). Psychological responses to outbreak of severe acute respiratory syndrome: A prospective, multiple time-point study. Journal of Personality, 73(1), 261–285. [Google Scholar]
10. Chua, S. E., Cheung, V., McAlonan, G. M., Cheung, C., Wong, J. W. et al. (2004). Stress and psychological impact on SARS patients during the outbreak. Canadian Journal of Psychiatry. Revue Canadienne de Psychiatrie, 49(6), 385–390. [Google Scholar]
11. Des Jarlais, D. C., Galea, S., Tracy, M., Tross, S., Vlahov, D. (2006). Stigmatization of newly emerging infectious diseases: AIDS and SARS. American Journal of Public Health, 96(3), 561–567. DOI 10.2105/AJPH.2004.054742. [Google Scholar] [CrossRef]
12. Jin, Z., Zhao, K., Xia, Y., Chen, R., Yu, H. et al. (2020). Psychological responses to the Coronavirus Disease (COVID-19) outbreak. chinaXiv:202003.00005V1. [Google Scholar]
13. Lai, D. (2008). Impact of severe acute respiratory syndrome (SARS) on depressive symptoms of older Chinese in Hong Kong. Hallym International Journal of Aging, 10, 77–84. DOI 10.2190/HA.10.2.a. [Google Scholar] [CrossRef]
14. Lau, J. T., Yang, X., Tsui, H., Kim, J. H. (2003). Monitoring community responses to the SARS epidemic in Hong Kong: From day 10 to day 62. Journal of Epidemiology and Community Health, 57(11), 864–870. DOI 10.1136/jech.57.11.864. [Google Scholar] [CrossRef]
15. Lau, J. T., Yang, X., Pang, E., Tsui, H. Y., Wong, E. et al. (2005). SARS-related perceptions in Hong Kong. Emerging Infectious Diseases, 11(3), 417–424. [Google Scholar]
16. Lau, A. L., Chi, I., Cummins, R. A., Lee, T. M., Chou, K. L. et al. (2008). The SARS (Severe Acute Respiratory Syndrome) pandemic in Hong Kong: Effects on the subjective wellbeing of elderly and younger people. Aging & Mental Health, 12(6), 7746–760. DOI 10.1080/13607860802380607. [Google Scholar] [CrossRef]
17. Lee, D. T., Sahota, D., Leung, T. N., Yip, A. S., Lee, F. F. et al. (2006). Psychological responses of pregnant women to an infectious outbreak: A case-control study of the 2003 SARS outbreak in Hong Kong. Journal of Psychosomatic Research, 61(5), 707–713. DOI 10.1016/j.jpsychores.2006.08.005. [Google Scholar] [CrossRef]
18. Lee, S. Y., Yang, H. J., Kim, G., Cheong, H. K., Choi, B. Y. (2016). Preventive behaviors by the level of perceived infection sensitivity during the korea outbreak of Middle East respiratory syndrome in 2015. Epidemiology and Health, 38, e2016051. [Google Scholar]
19. Leung, G. M., Lam, T. H., Ho, L. M., Ho, S. Y., Chan, B. H. et al. (2003). The impact of community psychological responses on outbreak control for severe acute respiratory syndrome in Hong Kong. Journal of Epidemiology and Community Health, 57(11), 857–863. DOI 10.1136/jech.57.11.857. [Google Scholar] [CrossRef]
20. Leung, G. M., Quah, S., Ho, L. M., Ho, S. Y., Hedley, A. J. et al. (2004). A tale of two cities: Community psychobehavioral surveillance and related impact on outbreak control in Hong Kong and Singapore during the severe acute respiratory syndrome epidemic. Infection Control and Hospital Epidemiology, 25(12), 1033–1041. DOI 10.1086/502340. [Google Scholar] [CrossRef]
21. Leung, G. M., Ho, L. M., Chan, S. K., Ho, S. Y., Bacon-Shone, J. et al. (2005). Longitudinal assessment of community psychobehavioral responses during and after the 2003 outbreak of severe acute respiratory syndrome in Hong Kong. Clinical Infectious Diseases, 40(12), 1713–1720. DOI 10.1086/429923. [Google Scholar] [CrossRef]
22. Leung, G. M., Quah, S., Ho, L. M. (2009). Community psycho-behavioural surveillance and related impact on outbreak control in Hong Kong and Singapore during the SARS epidemic. Hong Kong Medical Journal, 9, 30–34. [Google Scholar]
23. Li, J. B., Yang, A., Dou, K. (2020). Chinese public’s knowledge, perceived severity, and perceived controllability of COVID-19 and their associations with emotional and behavioural reactions, social participation, and precautionary behaviour: A national survey. BMC Public Health, 20, 1589. DOI 10.1186/s12889-020-09695-1. [Google Scholar] [CrossRef]
24. Main, A., Zhou, Q., Ma, Y., Luecken, L. J., Liu, X. (2011). Relations of SARS-related stressors and coping to Chinese college students’ psychological adjustment during the 2003 Beijing SARS epidemic. Journal of Counseling Psychology, 58(3), 410–423. DOI 10.1037/a0023632. [Google Scholar] [CrossRef]
25. Qian, M., Ye, D., Zhong, J., Xu, K., Zhang, L. et al. (2005). Behavioural, cognitive and emotional responses to SARS: Differences between college students in Beijing and Suzhou. Stress and Health, 21, 87–98. DOI 10.1002/(ISSN)1532-2998. [Google Scholar] [CrossRef]
26. Qian, M., Wu, Q., Wu, P., Hou, Z., Liang, Y. et al. (2020). Psychological responses, behavioral changes and public perceptions during the early phase of the COVID-19 outbreak in China: A population based cross-sectional survey. medRxiv. https://www.medrxiv.org/content/10.1101/2020.02.18.20024448v1.full-text. [Google Scholar]
27. Quah, S., Hin-Peng, L. (2004). Crisis prevention and management during SARS outbreak, Singapore. Emerging Infectious Diseases, 10, 364–368 DOI 10.3201/eid1002.030418. [Google Scholar] [CrossRef]
28. Sim, K., Huak Chan, Y., Chong, P. N., Chua, H. C., Wen Soon, S. (2010). Psychosocial and coping responses within the community health care setting towards a national outbreak of an infectious disease. Journal of Psychosomatic Research, 68(2), 195–202. DOI 10.1016/j.jpsychores.2009.04.004. [Google Scholar] [CrossRef]
29. Wang, C., Pan, R., Wan, X., Tan, Y., Xu, L. et al. (2020). Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. International Journal of Environmental Research and Public Health, 17(5), 1729. DOI 10.3390/ijerph17051729. [Google Scholar] [CrossRef]
30. Xie, X. F., Stone, E., Zheng, R., Zhang, R. G., (2011). The ‘Typhoon Eye effect’: Determinants of distress during the SARS epidemic. Journal of Risk Research, 14(9), 1091–1107 DOI 10.1080/13669877.2011.571790. [Google Scholar] [CrossRef]
31. Yeung, D. Y., Fung, H. H. (2007). Age differences in coping and emotional responses toward SARS: A longitudinal study of Hong Kong Chinese. Aging & Mental Health, 11(5), 579–587. DOI 10.1080/13607860601086355. [Google Scholar] [CrossRef]
32. Yu, H. Y. R., Ho, S. C., So, K. F. E., Lo, Y. L. (2005). The psychological burden experienced by Hong Kong midlife women during the SARS epidemic. Stress and Health, 21, 177–184. DOI 10.1002/(ISSN)1532-2998. [Google Scholar] [CrossRef]
33. Zhu, X., Wu, S., Miao, D., Li, Y. (2008). Changes in emotion of the Chinese public in regard to the SARS period. Social Behavior and Personality: An International Journal, 36, 447–454. DOI 10.2224/sbp.2008.36.4.447. [Google Scholar] [CrossRef]
34. Folkman, S., Moskowitz, J. T. (2004). Coping: Pitfalls and promise. Annual Review of Psychology, 55, 745–774 DOI 10.1146/annurev.psych.55.090902.141456. [Google Scholar] [CrossRef]
35. Carroll, L. (2013). Problem-focused coping. In: Gellman M. D, Turner J. R (Eds.Encyclopedia of behavioral medicine, pp. 1540–1541. Springer, New York, NY. [Google Scholar]
36. Lazarus, R. S., Folkman, S. (1984). Stress, appraisal, and coping. New York, NY: Springer Publishing Company. [Google Scholar]
 | This work is licensed under a Creative Commons Attribution 4.0 International License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. |