| International Journal of Mental Health Promotion |
DOI: 10.32604/ijmhp.2022.018332
ARTICLE
The Association between Physical Education and Mental Health Indicators in Adolescents: A Cross-Sectional Study
1School of Physical Education and Sports Training, Shanghai University of Sport, Shanghai, 200438, China
2Shanghai Research Centre for Physical Fitness and Health of Children and Adolescents, Shanghai University of Sport, Shanghai, 200438, China
*Corresponding Author: Yan Tang. Email: tybsh2011@126.com
Received: 16 July 2021; Accepted: 13 September 2021
Abstract: Objective: To explore the associations between physical education attendance and mental health indicators. Methods: Using data from the Global Student Health Survey, the frequency of physical education attendance, suicidality-related indicators, loneliness, bullying, and anxiety were all assessed using a standardized self-reported questionnaire. Multivariable logistic regression was used to estimate the association between physical education attendance and mental health-related indicators. Results: The study included 276,169 participants from 71 countries (47.3% males, aged 11–18 years old). After controlling for sex, age, food insecurity, close friends, physical activity, sedentary time, others’ help, and parents’ understanding, physical education attendance was not significantly associated with suicidal attempts, suicidal ideation, and anxiety. However, compared with no physical education attendance, individuals attending physical education for 1, 2, as well as 5 or more days had significantly reduced odds/ratios of suicide; only 2 days of physical education attendance was associated with a lower odds ratio for suffering from loneliness. Even 1 day of physical education was associated with not being bullied by others. Conclusion: This study suggests that physical education attendance may not have an effective role in reducing mental health illnesses in children and adolescents. Future studies are encouraged to corroborate or negate our research discoveries by using better and further improved study designs.
Keywords: Physical education; mental illness; loneliness; suicidality; bullying behaviors
Mental health problems, such as depression or anxiety disorders, have been and remain serious public health crises across the entireworld. Recent data shows that 792 million people in the world suffer from mental health disorders [1]. Specifically, 264 million and 284 million people are experiencing depression and anxiety disorders, respectively [1]. Among adolescents, it is much of the same. A global survey demonstrates that among 5–17 years old children and adolescents, the prevalence of mental health disorders was 6.7% [2]. In particular, 6.2% and 3.2% of them suffered from depression and anxiety, respectively. In China, a survey showed that about one in five Chinese children and adolescents experienced depression symptoms [3,4], and the proportions ranged from 10% to 50% in different regions [4]. Similarly, in the US, Ghandour et al. recently reported that 7.1% and 3.2% of children and youth had present anxiety or depression diagnoses, separately [5]. These data show that mental health problems are a serious public crisis across the planet. Considering that many adult mental health disorders begin in adolescence [6], adolescent mental health problems should be addressed in timely, thorough and effective manners.
To reduce the burden of mental health problems in adolescents, it is highly recommended to increase the physical activity (PA) levels of adolescents, as convincing evidence has confirmed the inverse association between PA and mental health problems, suggesting the protective effects of PA on mental health [7,8]. For example, a study based on Chinese adolescent samples indicated that sufficient PA was associated with lower risks of depression and anxiety symptoms [9]. Higher levels of PA participation in adolescents were also associated with lower levels of depression symptoms in Norwegian adolescents [10]. Associations between increased PA and decreased depression symptoms have been supported by evidence from systematic reviews [7,10]. McMahon et al. examined the association between PA engagement and anxiety and depression symptoms among adolescents from many European countries and found more frequent PA linked with lower scores of anxiety and depression [11]. These studies have informed all interested parties that sufficient PA could play an important role in reducing the likelihood of developing mental illness in adolescents.
As there are various modalities of PA, exploring the associations between different forms of PA and mental health outcomes is an interesting and worthwhile research question. These studies can provide evidence to design and implement more efficient and feasible interventions to reduce the burdens of mental health problems in adolescents. For example, there is evidence that more daily active travel behaviors were associated with lower odds of depression symptoms [12,13]. Recent studies also suggested that muscle strengthening exercises or activities were associated with better mental health indicators [14–16]. Owing to the varied settings of PA, more explorations are encouraged on the associations between various kinds of PA and improved mental health or the addressing of mental illness in young people [7]. Such investigations would be beneficial to design efficient mental health interventions incorporating PA or similar activities.
Physical education, as an essential component of PA for adolescents, occurred daily or frequently in school-aged children and adolescents in many countries (e.g., at least 3 times per week in China). As an approach to increasing PA, physical education may theoretically improve mental health or reduce the possibility of developing mental illness in adolescents. However, to date, very few studies have investigated the association between physical education and mental health indicators and generated inconsistent results.
When aggregating data from different research, a study using the meta-analytical method found no association between physical education and mental health in adolescents. In contrast, another recent systematic review and meta-analysis concluded that school-based physical activities may reduce anxiety, improve resilience and well-being, as well as increase positive mental health in children and adolescents [17]. In addition to the major research gap that studies investigating the roles of physical education on mental health indicators are limited, some other research gaps remain to be addressed.
First of all, multi-national studies assessing the association between physical education and mental health indicators are lacking. By using samples from various countries, it is conducive to increasing the generalizability of research findings on this topic. Second, previous studies investigating the association between physical education and mental health indicators have omitted some important confounders, like behavioral factors (e.g., physical activity and sedentary behavior). Adding these confounders is of great importance to more accurately study the association between physical education and mental health indicators. In order to address these gaps mentioned above across the literature, this study aims to explore the association between physical education and mental health indicators using data from multiple countries across the world. This study can inform physical education-related policies in different countries, as well as programs aimed to prevent or intervene in mental health problems among adolescents.
2.1 Study Survey and Participants
To achieve the research aim of this current study, public and available data from the Global School-Based Health Survey (GSHS) jointly supported by the World Health Organization (WHO) and the US Center for Disease Control (CDC) was used. The GSHS was a population-based questionnaire survey project that aimed to investigate risk behaviors and understand their influencing factors in adolescents across the world. More than 100 countries have been participating in this ongoing global survey project. The GSHS utilizes a standardized study design and sampling strategy to construct a nationally representative adolescent sample in each participating country. More details on the GSHS study methodology can be accessed at the website of the WHO (https://www.who.int/teams/noncommunicable-diseases/surveillance/systems-tools/global-school-based-student-health-survey/methodology) and the CDC (http://www.cdc.gov/gshs). All study participants filled up a standardized questionnaire in the local language to report their information on the variables assessed. The ethics approval from the ministry of education or health of each participating country was provided prior to the GSHS data collection. Only participants and their parents who provided written or verbal consent participated in this survey.
This study was a secondary analysis, which required no additional and specific ethics approval. In our study, we retained the latest dataset of each eligible participating country (some countries participated in multiple rounds of the GSHS survey) where these countries have variables that our study needed. In detail, data for this cross-sectional survey was retrieved from the GSHS website in early March of this year, 2022. Variables of physical education attendance, suicidal ideation, suicidal planning, suicidal attempts, loneliness, anxiety, instances of being bullied, sex, age, food insecurity, number of close friends, days of physical activity, sitting time, others’ help, and parental understanding were included for the final research analysis.
Finally, 276,169 participants of 11–18 years old from 71 countries were included in the current analysis as these participating countries provided data on the included variables after deleting missing cases. The GSHS survey and its associated measures were based on the US Youth Risk Behavior Surveillance (YRBS), which is one of largest health surveys in the world. The rationale and importance of the survey and measures can be accessed by previous materials [18–20], which can support our study theoretically.
2.2.1 Physical Education Attendance (Independent Variable)
To quantify the variable of physical education attendance, the question was used: “During this school year, on how many days did you go to physical education class each week?” Answers of this question included: 1 = 0 days, 2 = 1 day, 3 = 2 days, 4 = 3 days, 5 = 4 days and 6 = 5 or more days. In the further analysis, this variable was categorized into 1 = 0 days, 2 = 1–2 days, 3 = ≥3 days, in line with previous research [21].
2.2.2 Mental Health Indicators (Dependent Variables)
According to the availability of variables in the datasets, the current study included the following variables as mental health indicators: suicidal ideation, suicidal planning, suicidal attempting, loneliness, anxiety, and having been bullied. These variables were assessed by self-reported questionnaires under the standardized research protocol and measurement, which can be found in Table 1.

We selected the following variables as covariates in this survey, including sex, age, food insecurity, number of close friends, days of physical activity, sitting time, others’ help, and parental understanding. All these variables were assessed using a self-reported questionnaire which has been confirmed with acceptable validity and reliability [20].
All the statistical analyses were performed using SPSS version 26.0. Considering the complex survey design of the GSHS, the statistical analysis took sampling weight into consideration in estimating the results of the current study (complex samples module). Descriptive statistics were used to report the characteristics of participants, including prevalence estimates of all the variables included in this study (both unweighted and weighted). A logistic regression model was used to assess the associations between physical education and mental health indicators with covariates adjusted. Results of the logistic regression model were presented in a form of odds ratios (ORs) with 95% confidence intervals (CIs). The statistical significance was set up as p < 0.05 with being two-sided.
The demographic information is outlined in Table 2. In total, data from 276,169 children and adolescents were included in the analysis. 51.5% of included participants were female, and most were aged 13–16 years old. The proportions of each level of food insecurity were 49.8% (never), 18.1% (rarely), 21.0% (sometimes), 3.9% (most of the time), and 2.5% (always). In addition, 62.8% of adolescents have 3 or more close friends, and only 6.7% of them have no close friends.

Referring to the frequency of physical activity, 25.4% of adolescents did not participate in physical activity and only 22.9% of participants spent 5 days or more on physical activity. In terms of daily sitting time, 79.2% of participants spent less than 1 h/day to 3–4 h/day sitting, and 16.9% spend 5–6 h/day to more than 8 h/day sitting. Regarding others’ help, 26.7% of participants reported that they sometimes get help from others; 19.9% and 19.8% reported a higher frequency (most of the time and always); 10.9% and 14.7% of reported a lower frequency (never and rarely). In terms of parental understanding, most participants (21.6%) reported that they never perceived parental understanding. The percentage of the participants who reported “rarely”, “sometimes”, “most of the time”, and “always” were 14.5%, 20.6%, 14.4%, and 20.9%, respectively.
Table 3 displays the prevalence of physical education and mental health outcomes. 21.2% of participants never take part in physical education. The percentage of participating in physical education for 1 day, 2 days, 3 days, 4 days, and 5 or more days were 30.5%, 17.7%, 3.9%, 2.8%, and 17.7%, respectively. Notably, 13.0 of participants reported the presence of suicidal ideation. Furthermore, 12.1% of participants reported that they ever made a suicidal plan and 11.4% have attempted suicide at least one time. In addition, 39.7% of adolescents reported having feelings of loneliness. The percentage of adolescents with anxiety was 32.4%. Notably, 28.4% of adolescents had the experience of being bullied by others.

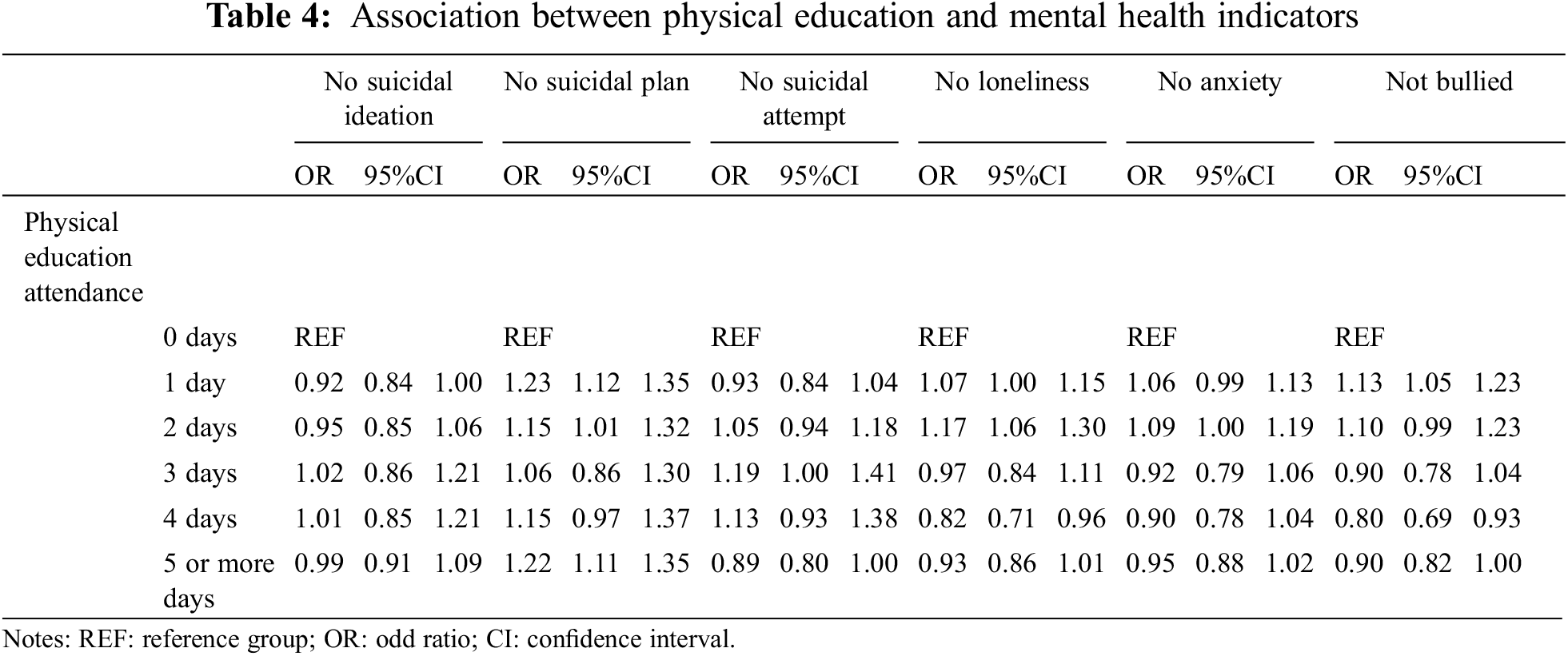
The associations between physical education and mental health indicators are shown in Table 4. Compared to not attending physical education, participating in physical education for 3 days (OR = 1.02, 95%CI: 0.86–1.21) and 4 days (OR = 1.01, 95%CI: 0.85–1.21) was positively associated with “no suicidal ideation”; participating in physical education for 1 day (OR = 0.92, 95%CI: 0.84–1.00), 2 days (OR = 0.95, 95%CI: 0.85–1.06), and 5 or more days (OR = 0.99, 95%CI: 0.91–1.09) was negatively associated with “no suicidal ideation”. Compared with not attending physical education, participating in physical education for 1 day (OR = 1.23, 95%CI: 1.12–1.35), 2 days (OR = 1.15, 95%CI: 1.1–1.32), 3 days (OR = 1.06, 95%CI: 0.86–1.30), 4 days (OR = 1.15, 95%CI: 0.97–1.37), and 5 or more days (OR = 1.22, 95%CI: 1.11–1.35) were positively associated with “No suicidal plan”. Compared with not participating in physical education, participating in physical education for 2 days (OR = 1.05, 95%CI: 0.94–1.18), 3 days (OR = 1.19, 95%CI: 1.00–1.41), 4 days (OR = 1.13, 95%CI: 0.93–1.38) were positively associated with “no suicidal attempt”; participating in physical education for 1 day (OR = 0.93, 95%CI: 0.84–1.04) and 5 or more days (OR = 0.89, 95%CI: 0.80–1.00) were negatively related to “no suicidal attempt”. Besides, only participating in physical education for 1 day (OR = 1.07, 95%CI: 1.00–1.15) and 2 days (OR = 1.17, 95%CI: 1.06–1.30) were positively associated with “no loneliness”, whereas 3 days (OR = 0.97, 95%CI: 0.84–1.11), 4 days (OR = 0.82, 95%CI: 0.71–0.96), and 5 or more days (OR = 0.93, 95%CI: 0.86–1.01) were negatively related to “no loneliness”. In addition, only participating in physical education for 1 day (OR = 1.06, 95%CI: 0.99–1.13) and 2 days (OR = 1.09, 95%CI: 1.00–1.19) were positively associated with “no anxiety”, 3 days (OR = 0.92, 95%CI: 0.79–1.06), 4 days (OR = 0.90, 95%CI: 0.78–1.04), 5 or more days (OR = 0.95, 95%CI: 0.88–1.02) were negatively related to “no anxiety”. Similarly, only participating in physical education for 1 day (OR = 1.13, 95%CI: 1.05–1.23) and 2 days (OR = 1.10, 95%CI: 0.99–1.23) were positively associated with “not bullied”, 3 days (OR = 0.90, 95%CI: 0.78–1.04), 4 days (OR = 0.80, 95%CI: 0.69–0.93), and 5 or more days (OR = 0.90, 95%CI: 0.82–1.00) were negatively related to “not bullied”.
The current study aimed to explore the association between physical education attendance and mental health indicators in adolescents from 71 countries (sample size > 27,0000). Using a large size sample of adolescents, the present study mainly found that physical education attendance was not significantly associated with the selected mental health indicators in this study. Our results may have some practical implications regarding future mental health interventions for adolescents.
The present study mainly found that physical education attendance may not play an essential role in improving mental health indicators. This finding is consistent with a recently published systematic review and meta-analysis, in which the authors found that physical education had no relationship with mental health or mental ill-health [22], such as depression and quality of life. They also explained that the included number of studies that assessed physical education was small (n = 2), which may cause a non-significant association between physical education and mental health indicators.
Our results can support their findings, which implies that physical education attendance may not have the potential to improve mental health in adolescents. These findings are counterintuitive considering that as a related component of physical activity, physical education is expected to improve the mental health of adolescents. However, the current study could not identify significant and negative associations between physical education and various mental health indicators. Although no significant and consistent relationships between physical education and mental health were identified, there is not enough evidence at this stage to conclude that physical education is not associated with mental health [22], as published studies remain scanty. In this regard, future studies are encouraged to explore the association between characteristics of physical education and more indicators of mental health or illness.
Due to the limiting literature on this topic, we cannot provide well-described explanations. Nevertheless, some plausible explanations can be applied to interpret the unexpected research findings in the current study. One of the explanations is that the present study focused on mental illness-relevant outcomes (i.e., suicidal ideation, suicidal plan, suicidal attempt, loneliness, anxiety, and being bullied). We noted that some studies assumed that physical education is associated with mental health indicators [23], especially positive emotional indicators rather than negative emotional ones. Therefore, future research is encouraged to include positive and negative mental health indicators concurrently, and to examine whether differences exist between physical education attendance and the two different significant aspects of mental health.
Besides, in our study, each mental health indicator was measured with one item, which may result in a biased estimation of the association between physical education and mental health indicators. Another possible explanation concerns the measures of physical education attendance. As the current study just measured the days of physical education attendance, some important information on physical education may have been omitted, such as the duration of physical education and activity intensity during physical education. Moreover, participants in this study presented low attendance in physical education, which may be a reason for the non-significant relationship between physical education and mental health indicators.
Although this study did not give positive evidence of physical education in adolescent mental health, it can not be ignored that problems of poor physical and mental health appear more in the young age group in recent decades [24]. Meanwhile, a large number of studies support that the systematic decline of physical activity is also one of the reasons for this trend [25,26]. However, it is worth noting that the crowded school curriculum in some countries, especially Asian countries, physical education receives insufficient attention from school administrators with an evident deficiency in time spent teaching physical education [27,28]. The lack of facilities to meet youth’s needs in sports in the school environment is also another obstacle for students to achieve sufficient physical activities on school days [29]. Given existing evidence on the benefits of physical education and sports in schools [23], a comprehensive school PA program is still worth adopting to play its role in adolescents’ health.
As mentioned above, this study has several limitations. The first limitation is that the data analyzed in the study were of cross-sectional nature. Using this kind of study design cannot draw a causal conclusion, which implies that the direction of association between physical education and mental health indicators remains unaddressed in the current study. The second limitation is self-reported measures to assess physical education and mental health indicators. Self-reported measures are affected by recall bias and social desirability. Third, mental health indicators are merely assessed by single items respectively. This measure would be a barrier to accurately measuring the mental health status of adolescents. Despite these inherent study limitations, some strengths should be mentioned. The first one is the large sample from various countries, increasing the generalizability of our research findings. Moreover, this study is one of the very few studies to investigate the associations between physical education and mental health outcomes, giving more insights into the roles of physical activity in mental health.
This study suggests that physical education attendance may not be associated with mental health indicators. However, owing to the limited number of similar studies, it is not conclusive to establish convincing evidence concerning physical education and mental health indicators. Future studies should use more improved study designs to confirm or negate our research findings.
Funding Statement: The authors received no specific funding for this study.
Conflicts of Interest: The authors declare that they have no conflicts of interest to report regarding the present study.
References
1. Dattani, S., Ritchie, H., Roser, M. (2021). Mental Health. https://ourworldindata.org/mental-health. [Google Scholar]
2. Erskine, H. E., Baxter, A. J., Patton, G., Moffitt, T. E., Patel, V. et al. (2017). The global coverage of prevalence data for mental disorders in children and adolescents. Epidemiology and Psychiatric Sciences, 26(4), 395–402. DOI 10.1017/S2045796015001158. [Google Scholar] [CrossRef]
3. Li, J., Li, J., Liang, J., Qian, S., Jia, R. et al. (2019). Depressive symptoms among children and adolescents in China: A systematic review and meta-analysis. Medical Science Monitor: International Medical Journal of Experimental and Clinical Research, 25, 7459–7470. DOI 10.12659/MSM.916774. [Google Scholar] [CrossRef]
4. Zgambo, M., Kalembo, F., Guoping, H., Honghong, W. (2012). Depression among Chinese children and adolescents: A rview of the literature. International Journal of Child, Youth & Family Studies, 3(4), 442. DOI 10.18357/ijcyfs34.1201211543. [Google Scholar] [CrossRef]
5. Ghandour, R. M., Sherman, L. J., Vladutiu, C. J., Ali, M. M., Lynch, S. E. et al. (2019). Prevalence and treatment of depression, anxiety, and conduct problems in US children. The Journal of Pediatrics, 206, 256–267. DOI 10.1016/j.jpeds.2018.09.021. [Google Scholar] [CrossRef]
6. Jones, P. B. (2013). Adult mental health disorders and their age at onset. The British Journal of Psychiatry, 54, s5–s10. DOI 10.1192/bjp.bp.112.119164. [Google Scholar] [CrossRef]
7. Biddle, S. J., Ciaccioni, S., Thomas, G., Vergeer, I. (2018). Physical activity and mental health in children and adolescents: An updated review of reviews and an analysis of causality. Psychology of Sport and Exercise, 42, 146–155. DOI 10.1016/j.psychsport.2018.08.011. [Google Scholar] [CrossRef]
8. Lubans, D., Richards, J., Hillman, C., Faulkner, G., Beauchamp, M. et al. (2016). Physical activity for cognitive and mental health in youth: A systematic review of mechanisms. Pediatrics, 138(3), e20161642. DOI 10.1542/peds.2016-1642. [Google Scholar] [CrossRef]
9. Chi, X., Liang, K., Chen, S., Huang, Q., Huang, L. et al. (2021). Mental health problems among Chinese adolescents during the COVID-19: The importance of nutrition and physical activity. International Journal of Clinical and Health Psychology, 21(3), 100218. DOI 10.1016/j.ijchp.2020.100218. [Google Scholar] [CrossRef]
10. Kleppang, A. L., Hartz, I., Thurston, M., Hagquist, C. (2018). The association between physical activity and symptoms of depression in different contexts-a cross-sectional study of Norwegian adolescents. BMC Public Health, 18(1), 1368. DOI 10.1186/s12889-018-6257-0. [Google Scholar] [CrossRef]
11. McMahon, E. M., Corcoran, P. O., Regan, G., Keeley, H., Cannon, M. et al. (2017). Physical activity in european adolescents and associations with anxiety, depression and well-being. European Child & Adolescent Psychiatry, 26(1), 111–122. DOI 10.1007/s00787-016-0875-9. [Google Scholar] [CrossRef]
12. Gu, J., Chen, S. (2020). Association between active travel to school and depressive symptoms among early adolescents. Children, 7(5), 41. DOI 10.3390/children7050041. [Google Scholar] [CrossRef]
13. Liu, S., Chen, S., Zhu, X., Stubbs, B., Yu, Q. et al. (2021). Association between active school travel and depressive symptoms among 51,702 adolescents in 26 low-and middle-income countries. International Journal of Mental Health Promotion, 23(2), 141–153. DOI 10.32604/IJMHP.2021.016274. [Google Scholar] [CrossRef]
14. Bennie, J. A., Teychenne, M., Tittlbach, S. (2020). Muscle-strengthening exercise and depressive symptom severity among a nationally representative sample of 23,635 German adults. Journal of Affective Disorders, 266, 282–287. DOI 10.1016/j.jad.2020.01.172. [Google Scholar] [CrossRef]
15. Bennie, J. A., Shakespear-Druery, J., de Cocker, K. (2020). Muscle-strengthening exercise epidemiology: A New frontier in chronic disease prevention. Sports Med Open, 6(1), 40. DOI 10.1186/s40798-020-00271-w. [Google Scholar] [CrossRef]
16. Bennie, J. A., De Cocker, K., Biddle, S., Teychenne, M. J. (2020). Joint and dose-dependent associations between aerobic and muscle-strengthening activity with depression: A cross-sectional study of 1.48 million adults between 2011 and 2017. Depression and Anxiety, 37(2), 166–178. DOI 10.1002/da.22986. [Google Scholar] [CrossRef]
17. Andermo, S., Hallgren, M., Nguyen, T. T., Jonsson, S., Petersen, S. et al. (2020). School-related physical activity interventions and mental health among children: A systematic review and meta-analysis. Sports Medicine-Open, 6(1), 25. DOI 10.1186/s40798-020-00254-x. [Google Scholar] [CrossRef]
18. Center for Disease Control and Prevention (2021). Youth risk behavior surveillance system. https://www.cdc.gov/healthyyouth/data/yrbs/index.htm. [Google Scholar]
19. Kann, L., Warren, W., Collins, J. L., Ross, J., Collins, B. et al. (1993). Results from the national school-based 1991 youth risk behavior survey and progress toward achieving related health objectives for the nation. Public Health Reports, 108(Suppl 1), 47–55. [Google Scholar]
20. Brener, N. D., Collins, J. L., Kann, L., Warren, C. W., Williams, B. I. (1995). Reliability of the youth risk behavior survey questionnaire. American Journal of Epidemiology, 141(6), 575–580. DOI 10.1093/oxfordjournals.aje.a117473. [Google Scholar] [CrossRef]
21. Uddin, R., Salmon, J., Islam, S., Khan, A. (2020). Physical education class participation is associated with physical activity among adolescents in 65 countries. Scientific Reports, 10(1), 22128. DOI 10.1038/s41598-020-79100-9. [Google Scholar] [CrossRef]
22. White, R. L., Babic, M. J., Parker, P. D., Lubans, D. R., Astell-Burt, T. et al. (2017). Domain-specific physical activity and mental health: A meta-analysis. American Journal of Preventive Medicine, 52(5), 653–666. DOI 10.1016/j.amepre.2016.12.008. [Google Scholar] [CrossRef]
23. Bailey, R. (2006). Physical education and sport in schools: A review of benefits and outcomes. Journal of School Health, 76(8), 397–401. DOI 10.1111/j.1746-1561.2006.00132.x. [Google Scholar] [CrossRef]
24. Mojtabai, R., Olfson, M., Han, B. (2016). National trends in the prevalence and treatment of depression in adolescents and young adults. Pediatrics, 138(6). DOI 10.1542/peds.2016-1878. [Google Scholar] [CrossRef]
25. Haßdenteufel, K., Feißt, M., Brusniak, K., Lingenfelder, K., Matthies, L. M. et al. (2020). Reduction in physical activity significantly increases depression and anxiety in the perinatal period: A longitudinal study based on a self-report digital assessment tool. Archives of Gynecology and Obstetrics, 302, 53–64. DOI 10.1007/s00404-020-05570-x. [Google Scholar] [CrossRef]
26. Kari, J. T., Pehkonen, J., Hutri-Kähönen, N., Raitakari, O. T., Tammelin, T. H. (2017). Longitudinal associations between physical activity and educational outcomes. Medicine & Science in Sports & Exercise, 49(11), 2158–2166. DOI 10.1249/MSS.0000000000001351. [Google Scholar] [CrossRef]
27. Morgan, P. J., Hansen, V. (2008). Classroom teachers’ perceptions of the impact of barriers to teaching physical education on the quality of physical education programs. Research Quarterly for Exercise and Sport, 79(4), 506–516. DOI 10.1080/02701367.2008.10599517. [Google Scholar] [CrossRef]
28. Jenkinson, K. A., Benson, A. (2010). Barriers to providing physical education and physical activity in victorian state secondary schools. Australian Journal of Teacher Education, 35(8), 1–17. DOI 10.14221/ajte.2010v35n8.1. [Google Scholar] [CrossRef]
29. Hatfield, D. P., Chomitz, V. R. (2015). Increasing children’s physical activity during the school day. Current Obesity Reports, 4(2), 147–156. DOI 10.1007/s13679-015-0159-6. [Google Scholar] [CrossRef]
 | This work is licensed under a Creative Commons Attribution 4.0 International License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. |