DOI:10.32604/CHD.2021.011694
| Congenital Heart Disease DOI:10.32604/CHD.2021.011694 | |
| Article |
Characterization of Malalignment between Atrial and Ventricular Septa in Overriding/Straddling Tricuspid and Mitral Valves
1The Labatt Family Heart Centre, The Hospital for Sick Children, University of Toronto, Toronto, Canada
2Division of Cardiology, Department of Paediatrics, The Hospital for Sick Children, University of Toronto, Toronto, Canada
3Department of Diagnostic Imaging, The Hospital for Sick Children, University of Toronto, Toronto, Canada
*Corresponding Author: Shi-Joon Yoo. Email: shi-joon.yoo@sickkids.ca
Received: 05 May 2020; Accepted: 12 October 2020
Abstract: Objective: Overriding/straddling of an atrioventricular valve is a consequence of atrial-ventricular septal malalignment. We sought to characterize the malalignment by analogizing it to a flap-door and using structured approach. Methods: The echocardiograms and magnetic resonance images of 35 patients with overriding/straddling tricuspid or mitral valve were evaluated to assess the following modifiers; the malaligned part of the septum, the reference structure, and the mechanism, direction and severity of malalignment. Results: The pathology included classic overriding tricuspid valve in 15, classic overriding mitral valve in 12, and overriding tricuspid valve with left juxtaposition of atrial appendages in 8. In classic overriding tricuspid valve, the ventricular septum was hinged to the anterior interventricular groove and its insertion to the posterior interventricular groove was displaced toward the right ventricle. The VSD primarily involved the inlet but also extended toward the anterior interventricular groove. In classic overriding mitral valve, the ventricular septum was hinged to the posterior interventricular groove and crux cordis. Its insertion to the anterior interventricular groove was displaced toward the left ventricle. The VSD primarily involved the anterior part but also extended toward the inlet. Overriding tricuspid valve with left juxtaposition of atrial appendages had a mild degree of malalignment with displacement/rotation of the atrioventricular junction. Evenly spaced short-axis images were most helpful in characterizing the pathology. Conclusions: Overriding/straddling atrioventricular valves can be easily understood by analogizing the atrial-ventricular septal malalignment to a flap-door and describing the pathology in a structured manner. Contrary to what has previously been known, the VSD is not limited to the inlet or outlet part of the ventricular septum.
Keywords: Malalignment; ventricular septal defect; overriding; straddling; tricuspid; mitral
Overriding of an atrioventricular valve is a consequence of malalignment between the atrial and ventricular septa [1–4]. In the majority of cases, overriding is associated with straddling of the tension apparatus. With varying severity of malalignment and overriding, the atrioventricular connection ranges from biventricular to univentricular double-inlet ventricular connection [1,2]. It has been described that the tricuspid valve overrides/straddles through a ventricular septal defect (VSD) involving the posterior or inlet part of the septum, while the mitral valve overrides/straddles through a VSD involving the anterior or infundibular part of the septum [1,2]. However, the usage of the words ‘posterior’ versus ‘anterior’ and ‘inlet’ versus ‘infundibular’ is inaccurate and misleading [3,5]. It is also important that the characteristics of the septal malalignment as well as its presence should be described understandably.
Based on our clinical experience and pathological observations, we hypothesize that the atrial-ventricular septal malalignment causing overriding/straddling of an atrioventricular valve can be better understood by analogizing the malaligned part of the septum to a flap-door panel that is hinged to the anterior or posterior interventricular groove (Fig. 1) and can be systematically evaluated by characterizing the following modifiers [6]:

Figure 1: Cartoons explaining the flap-door mechanism of the atrial-ventricular septal malalignment. A. The flap-door panel is hinged to the anterior interventricular groove with the free edge of the door panel at the back. With the malalignment in such a manner, the posterior insertion of the ventricular septum is offset from the crux cordis (asterisk). B. The flap-door panel is hinged to the posterior interventricular groove with the free edge of the door panel in the front. With malalignment in such a manner, the posterior insertion of the ventricular septum is kept at the crux cordis. AV, aortic valve; MV, mitral valve; PV, pulmonary valve; TV, tricuspid valve
1. The malaligned part of the septum,
2. The reference structure,
3. The mechanism of malalignment,
4. The direction of malalignment, and
5. The severity of malalignment
The present study was aimed to characterize the pattern of atrial-ventricular septal malalignment using the flap-door mechanism concept and apply a structured approach to the diagnosis in patients with an imaging diagnosis of tricuspid or mitral valve overriding/straddling. We also sought to find the most helpful imaging planes for the diagnosis of overriding/straddling valves and the characterization of the septal malalignment.
Overriding versus straddling [1,2]: Overriding describes the relationship of the valvar annulus in relation to the ventricular septum. Overriding of an atrioventricular valve implies that the underlying ventricular septum is malaligned from the atrial septal plane. Straddling refers to the attachment of the supporting tension apparatuses in both ventricles. Although overriding and straddling coexist in the majority, straddling may occur without overriding and overriding may occur without straddling. Straddling without overriding occurs without septal malalignment.
Tricuspid versus mitral valve: The atrioventricular valves are named by their ventricular designation: i.e., the valve of the morphologically right ventricle is called the tricuspid valve, and that of the morphologically left ventricle is called the mitral valve [5]. As the ventricular designation in naming the valves is not applicable in double inlet right or left ventricle, the valves are commonly named as the right and left atrioventricular valves [1]. Although this approach is logical, it limits the discussion of the pathological spectrum transitioning from biventricular to univentricular atrioventricular connection. For the sake of simplicity, we define the tricuspid and mitral valves as the valves on the sides of the right and left ventricles, respectively [7]. In hearts with D-loop or right hand pattern of ventricular relationship, the right atrioventricular valve is called the tricuspid valve and the left atrioventricular valve the mitral valve. In hearts with L-loop or left hand pattern of ventricular relationship, the right atrioventricular valve is called the mitral valve and the left atrioventricular valve the tricuspid valve.
Crux cordis: It is an external landmark of the heart where the atrioventricular sulcus is crossed by the continuation of the posterior interatrial and interventricular groove. In abnormal hearts with atrial-ventricular septal malalignment, the crux cordis is defined as the point where the posterior interatrial groove abuts on the atrioventricular sulcus [1,2].
Posteromedian muscle ridge (Also called posteromedial muscle or posterior ridge): In most hearts with tricuspid valve overriding or double inlet left ventricle, a muscle ridge arises from the posterior wall of the left ventricle at the junction between the two atrioventricular valvar annuli and extends toward the apex [1,2,8]. Its origin between the two atrioventricular valvar annuli corresponds to the crux cordis externally. The presence of the posteromedian muscle ridge as a distinct structure indicates that the inlet part of the ventricular septum is malaligned in relation to the primum part of the atrial septum. Normally it is considered to form a part of the ventricular septum. Although the posteromedian muscle ridge is an intraventricular structure, it has a constant relationship with the atrioventricular valves and therefore the primum part of the atrial septum in both normal and abnormal hearts [2]. Its presence is best appreciated in a stack of basal short-axis views as will be shown in the Results.
The study was approved by the institutional research ethics board. From the institutional database between 2000 and 2019, patients with the diagnosis of overriding and/or straddling of the tricuspid or mitral valve were identified. We also identified cases with the tricuspid or mitral valve having chordal attachment to the ventricular septal crest. We excluded patients with imaging studies of insufficient quality. We also excluded patients with a major degree of twisting or criss-crossing of the atrioventricular connection axes. A major degree of twisting was defined as the situation when neither the long nor the short axes of the two atrioventricular valves were able to be visualized in the same two dimensional imaging planes. Three investigators reviewed the images to reach a consensus regarding the severity of overriding, the disposition of the tension apparatuses, and the characteristics of the septal malalignment and VSD.
Assessment of overriding of an atrioventricular valve: A stack of images obtained across the short-axis of the atria and ventricles along with images obtained at and parallel to the four-chamber planes were used for the diagnosis and grading of the severity of atrioventricular valve overriding. The severity of overriding was classified into 4 grades according to the overriding valvar area: i.e., ≤25%, 26%–50%, 51%–75% and >75% of the valve committed to the opposite ventricle.
Assessment of the characteristics of the ventricular septal malalignment: The 5 modifiers of septal malalignment listed in the introduction were defined. The reference structures for this assessment included the atrial septal plane and the crux cordis as defined above. We classified the mechanism of the ventricular septal malalignment into three types: (1) malalignment with the hinges along the anterior interventricular groove, (2) malalignment with the hinges along the posterior interventricular groove, and (3) any other mechanism (Fig. 1). The severity of the malalignment was defined by the angle formed by the atrial and ventricular septum: ≤30°, 31°–60° and >60° of malalignment graded as mild, moderate and severe malalignment, respectively.
We identified 35 patients with an overriding/straddling atrioventricular valve who had appropriate echocardiograms for retrospective assessment. In 29 patients, cardiovascularmagnetic resonance (CMR) was also available. There were 23 (13 females, 10 males) with overriding/straddling tricuspid valve and 12 (4 females, 8 males) with overriding/straddling mitral valve. The visceral situs was solitus in all 23 with overriding/straddling tricuspid valve and 8 of 12 with overriding/straddling mitral valve, heterotaxy in 3 and inversus in one.
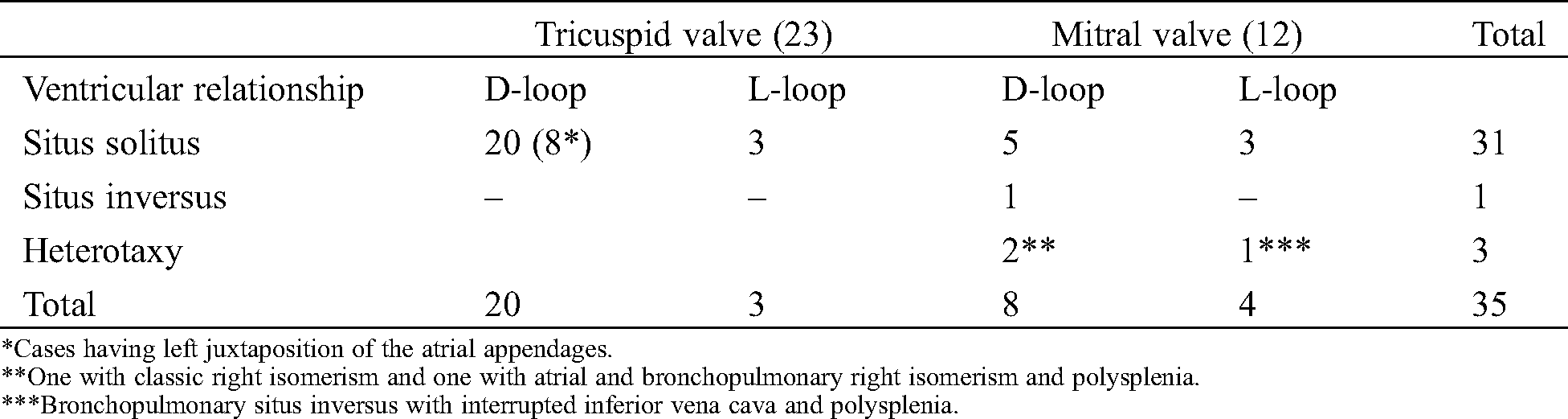
The distribution of patients according to situs, ventricular relationship and affected atrioventricular valve is summarized in Tab. 1. Eight with situs solitus and D-loop ventricles were associated with left juxtaposition of the atrial appendages and showed distinctly different findings as compared to the rest of the patients. Therefore, the study population was divided into three groups: (1) Classic tricuspid valve overriding/straddling, (2) Classic mitral valve overriding/straddling, and (3) Tricuspid valve overriding/straddling with left juxtaposition of the atrial appendages.
Table 1: Patient distribution according to the situs and the type of the ventricular relationships
3.1 Classic Overriding/Straddling Tricuspid Valve (n = 15)
All 15 showed malalignment of the ventricular septum relative to the atrial septal plane that could be explained by the flap-door mechanism illustrated in Fig. 1A. The anterior interventricular groove was aligned closely with the atrial septal plane, while the posterior interventricular groove was displaced toward the side of the right ventricle (rightward in 12 with D-loop ventricles and leftward in 3 with L-loop ventricles), resulting in offset between the posterior interventricular groove and the crux cordis (Fig. 2). The posterior medial part of the tricuspid valve was the primary part of overriding with the anterior aspect overriding less or not overriding. The severity of overriding was ≤25% in 7, 26%–50% in 3, 51%–75% in 3, and >75% in 2. Therefore, there was biventricular atrioventricular connection in 10 (concordant in 9 and discordant in 1) and double inlet left ventricle in 5. The posteromedian muscle ridge was identified in basal short-axis images as a separate spur-like structure along the posterior wall of the left ventricle between the tricuspid and mitral valve inflows in all except one who had mild septal malalignment and minimal overriding of the tricuspid valve. The straddling part of the tricuspid valve was supported by the papillary muscle located in the apex of the left ventricle near the posteromedian muscle ridge in 12. The remaining 3 had chordal insertion of the tricuspid valve to the left ventricular side of the ventricular septal crest with minimal overriding. The tricuspid valve had chordal insertion to the outlet septum in 8. The VSD was larger posteriorly along the posterior interventricular groove than anteriorly at the great arterial origin(s). The ventriculoarterial connection was concordant in 6, discordant in 6, double outlet right ventricle in 2, and single outlet with absent main pulmonary artery in 1. All 3 with L-loop ventricles had discordant ventriculoarterial connection. The outlet septum was aligned with the rest of the ventricular septum in 6 with concordant or discordant ventriculoarterial connection. The outlet septum was malaligned in relation to the rest of the ventricular septum in 6. The outlet septum was absent in 2 with pulmonary atresia.
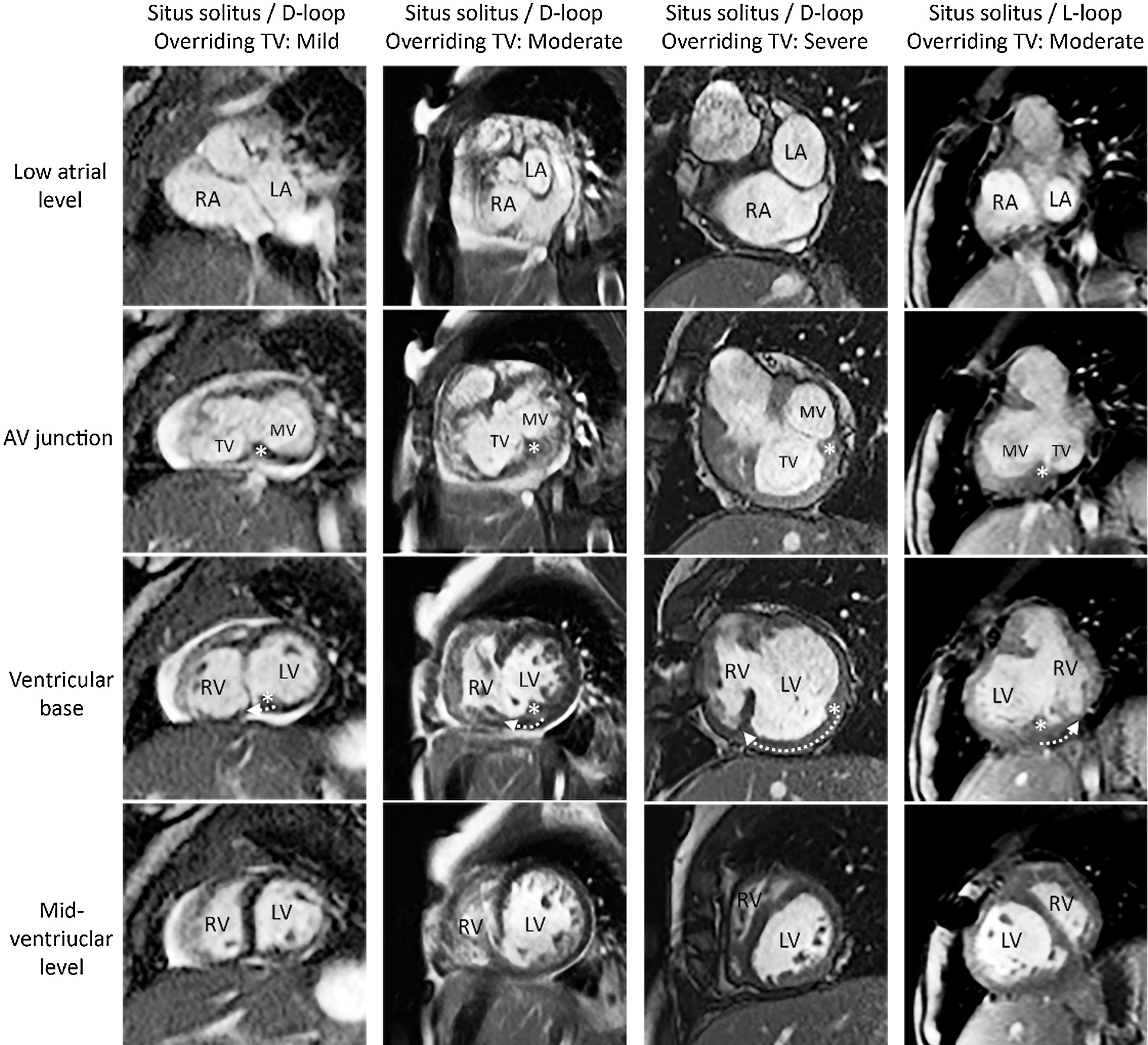
Figure 2: Short-axis MR images from 4 patients with overriding/straddling tricuspid valve. Three panels on the left show the cases with various severity of overriding in the setting of situs solitus and D-loop ventricles. Right hand panel shows the case occurring in the setting of situs solitus and L-loop ventricles. The location of the crux cordis/posteromedian muscle ridge is marked with an asterisk. The direction and degree of the malalignment is marked with a curved arrow in the third row figures. Note the increasing separation of the two structures with increasing severity of overriding. AV, atrioventricular; LA, left atrium; LV, left ventricle; MV, mitral valve; RA, right atrium; RV, right ventricle TV, tricuspid valve
3.2 Classic Overriding/Straddling Mitral Valve (n = 12)
This group consisted of 5 with situs solitus and D-loop ventricles, 3 with situs solitus and L-loop ventricles, 1 with situs inversus and D-loop ventricles and 3 with hetrotaxy. The mitral valve straddled and overrode the ventricular septum in all except one who had straddling without overriding.
Eleven with overriding mitral valve showed malalignment of the ventricular septum relative to the atrial septal plane that could be explained by the flap-door mechanism illustrated in Fig. 1B. The posterior interventricular groove was aligned with the atrial septum at the crux cordis, while the insertion to the anterior interventricular groove was displaced toward the side of the left ventricle (leftward in 7 with D-loop ventricles and rightward in 4 with L-loop ventricles) (Fig. 3). The anterior medial part of the mitral valve was the primary part of overriding with the posterior aspect overriding less or not overriding. The severity of overriding was ≤25% in 3, 26%–50% in 3, 51%–75% in 4, and >75% in 1. Therefore, there was biventricular atrioventricular connection in 6 (concordant in 2, discordant in 2 and mixed in 2) and double inlet right ventricle in 5. The posteromedian muscle ridge was not a separate muscular ridge in any of these patients. The straddling part of the mitral valve was supported by a separate papillary muscle that was inserted to the anterior apical aspect of the right ventricle in 8. The mitral valve had duplicate orifices with the anterior orifice committed to the right ventricle and the posterior orifice committed to the left ventricle in one (Fig. 4). The chords inserted to the anterior aspect of the right ventricular side of the septum and to additional papillary muscles in the right ventricle in one. The mitral valve had normally positioned anterolateral and posteromedial papillary muscles in the left ventricle in all except 2 with double inlet right ventricle including one with double orifice mitral valve. The VSD was larger anteriorly than posteriorly. However, the VSD extended toward the inlet along the tricuspid and mitral valve annuli in all. All had double outlet right ventricle except one with heterotaxy and right isomerism. The outlet septum was free floating in the right ventricular outflow tract in all 10 with double outlet right ventricle. In these patients, the outlet septum was in the same plane with or close to the atrial septal plane. In 4 with double outlet right ventricle with situs solitus and concordant atrioventricular connection, the VSD was closer to the left-sided pulmonary valve. Three of these patients had subpulmonary stenosis and one had subaortic stenosis. There was subpulmonary stenosis in 3 additional patients and subaortic stenosis in one additional patient. One had pulmonary atresia.

Figure 3: Short-axis MR images from 4 patients with overriding/straddling mitral valve. Three panels on the left show the cases with various severity of overriding in the setting of situs solitus and D-loop ventricles. Right hand panel shows the case occurring in the setting of situs solitus and L-loop ventricles. The location of the crux cordis is marked with an asterisk. The direction and degree of the malalignment is marked with a curved arrow in the second row figures. The ventricular septum inserts to the posterior interventricular groove that is aligned with the crux cordis. The anterior interventricular groove is deviated toward the side of the left ventricle in relation to the atrial septal plane in all cases. AV, atrioventricular; LA, left atrium; LV, left ventricle; MV, mitral valve; RA, right atrium; RV, right ventricle TV, tricuspid valve

Figure 4: Echocardiograms in short and long axis of the heart showing straddling mitral valve with double orifices. The posterior interventricular groove (asterisk) is aligned with the plane of the atrial septum and crux cordis (not shown). The anterior interventricular groove (x) is displaced toward the side of the left ventricle (LV). The left ventricle is moderately hypoplastic. LA, left atrium; M1and M2, mitral valve orifices; MPA, main pulmonary artery; TV, tricuspid valve
The patient with straddling mitral valve without overriding did not show significant septal malalignment with the chords of the anterior leaflet inserting to the right ventricular aspect of the septum below the VSD.
3.3 Overriding Tricuspid Valve Occurring with Left Juxtaposition of the Atrial Appendages (n = 8)
There was a mild degree of atrial-ventricular septal malalignment with the tricuspid valve displaced upward and slightly leftward in relation to the mitral valve in all (Fig. 5). As a consequence, the atrioventricular valves with the adjacent atrial septum appeared rotated clockwise as seen from the apex.
There was mild overriding of the anterior medial part of the tricuspid valve through the VSD involving the anterior aspect of the inlet part of the septum. The VSD did not reach the crux cordis in any of these patients. The posterior interventricular groove was aligned with the atrial septal plane at the crux cordis in all. Two had chordal insertion of the overriding tricuspid valve to the ventricular septal crest. No patient had overt straddling of the tricuspid valve. The tricuspid valve was hypoplastic in 3. The ventriculoarterial connection was double outlet right ventricle with the outlet septum free floating in the right ventricular outflow tract in 6. Two had discordant ventriculoarterial connection with pulmonary valve atresia.
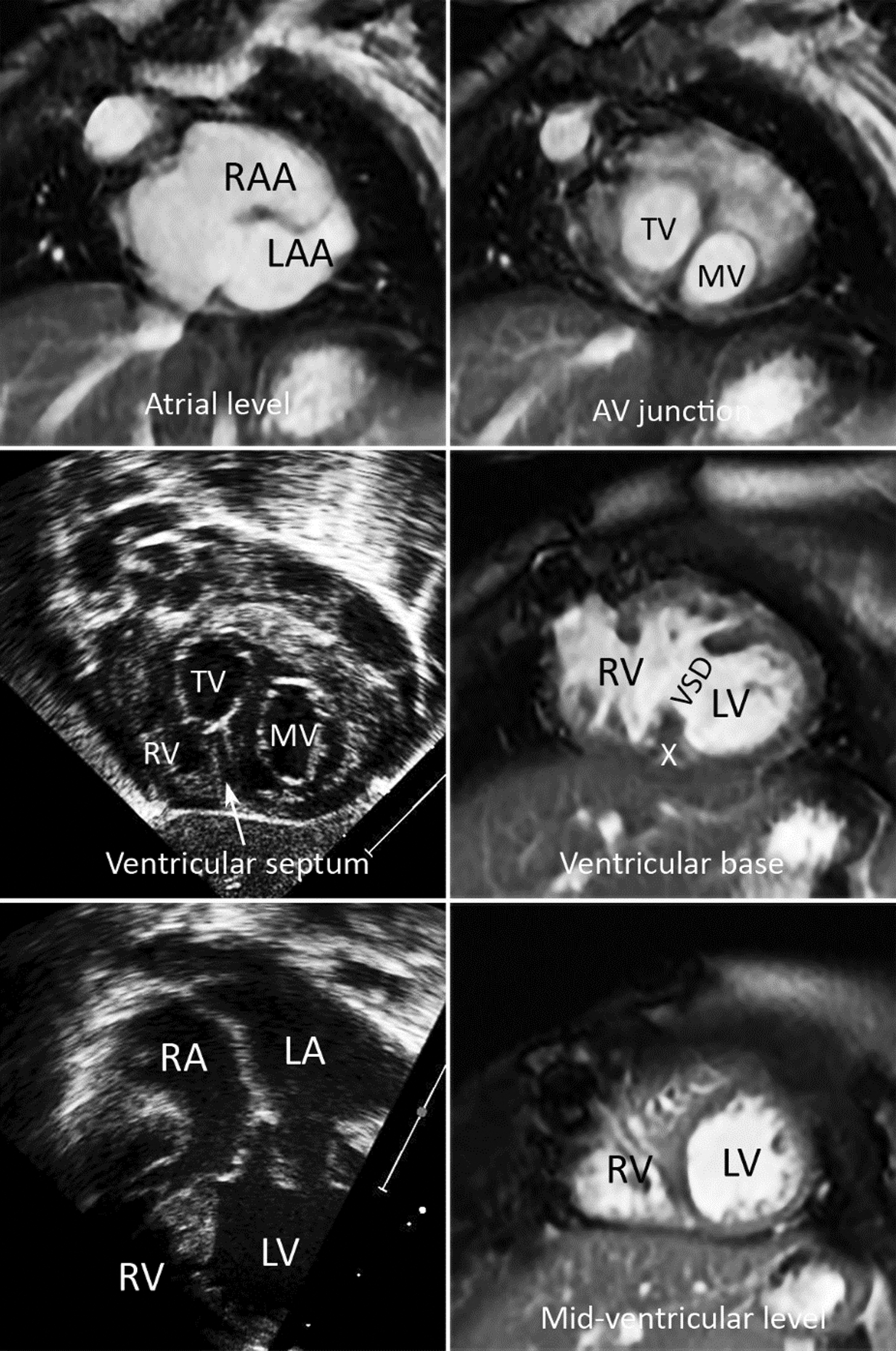
Figure 5: Short-axis MR images and echocardiograms in coronal and 4-chamber planes (lower two panels on the left) from a patient with left juxtaposition of the atrial appendages. The atrioventricular (AV) junction appears rotated clockwise as seen from the apex. The atrial septum is malaligned from the plane of the ventricular septum. Echo images show mild overriding of the tricuspid valve. The VSD involves the anterior part of the inlet septum and does not reach the posterior interventricular groove (X). LA, left atrium; LAA, left atrial appendage; LV, left ventricle; RA, right atrium; RAA, right atrial appendage; RV, right ventricle
3.4 Imaging Planes Best Showing Mitral Valve Overriding and Straddling
The primary diagnosis of overriding and/or straddling atrioventricular valve was made at the echocardiography using 4-chamber and parasternal long-axis oblique views. Among various imaging planes, serial short-axis planes extending from the atrium to the ventricular apex were most helpful in defining the presence and severity of the atrial-ventricular septal malalignment, the degree of overriding and the nature of straddling of an atrioventricular valve. The short-axis images across the ventricular outflow tracts were also most helpful in defining the ventriculoarterial connection and the relationship of the VSD to the subpulmonary and subaortic outflow tracts. The 4-chamber and other horizontal long axis views were helpful in visualizing the straddling tension apparatuses. The distance from the ventricular septal crest to the annulus of the overriding valve in these views varied according to the location of the imaging plane. Therefore, it was not possible to assess the severity of overriding using these views alone.
Echocardiograms were far superior to MRI in demonstration of the chordae tendinae and their insertion sites (Figs. 4 and 5). On the other hand, it was much easier and objective with CMR than with echocardiograms to characterize the septal malalignment (Figs. 2, 3 and 5).
The tricuspid and mitral valves override the ventricular septum through the different types of VSD [1,2], implying different underlying mechanisms of atrial-ventricular septal malalignment. Our study provides the new insights into the characteristics of atrial-ventricular septal malalignment and the VSDs in overriding/straddling tricuspid and mitral valves.
4.1 Hinged Door Analogy for Ventricular Septal Malalignment
The atrial-ventricular septal malalignment can be conceptualized by analogizing the ventricular septum to a door panel that is hinged to either the anterior or the posterior interventricular groove (Figs. 1 and 6) [6]. In classic tricuspid valve overriding, the ventricular septum is hinged to the anterior interventricular groove and its insertion to the posterior interventricular groove is displaced toward the side of the right ventricle. In mitral valve overriding, the ventricular septum is hinged to the posterior interventricular groove and its insertion to the anterior interventricular groove is displaced toward the side of the left ventricle. These different mechanisms explain the distinctly different morphologic features between the hearts with tricuspid valve overriding and those with mitral valve overriding. In both conditions, there is a spectrum of overriding resulting in atrioventricular connection ranging from biventricular connection to double inlet right or left ventricular connection [1,2,8] (Fig. 6). It is also important to note that the ventricular relationship and the location and boundary of the VSD varies according to the severity of atrial-ventricular septal malalignment.
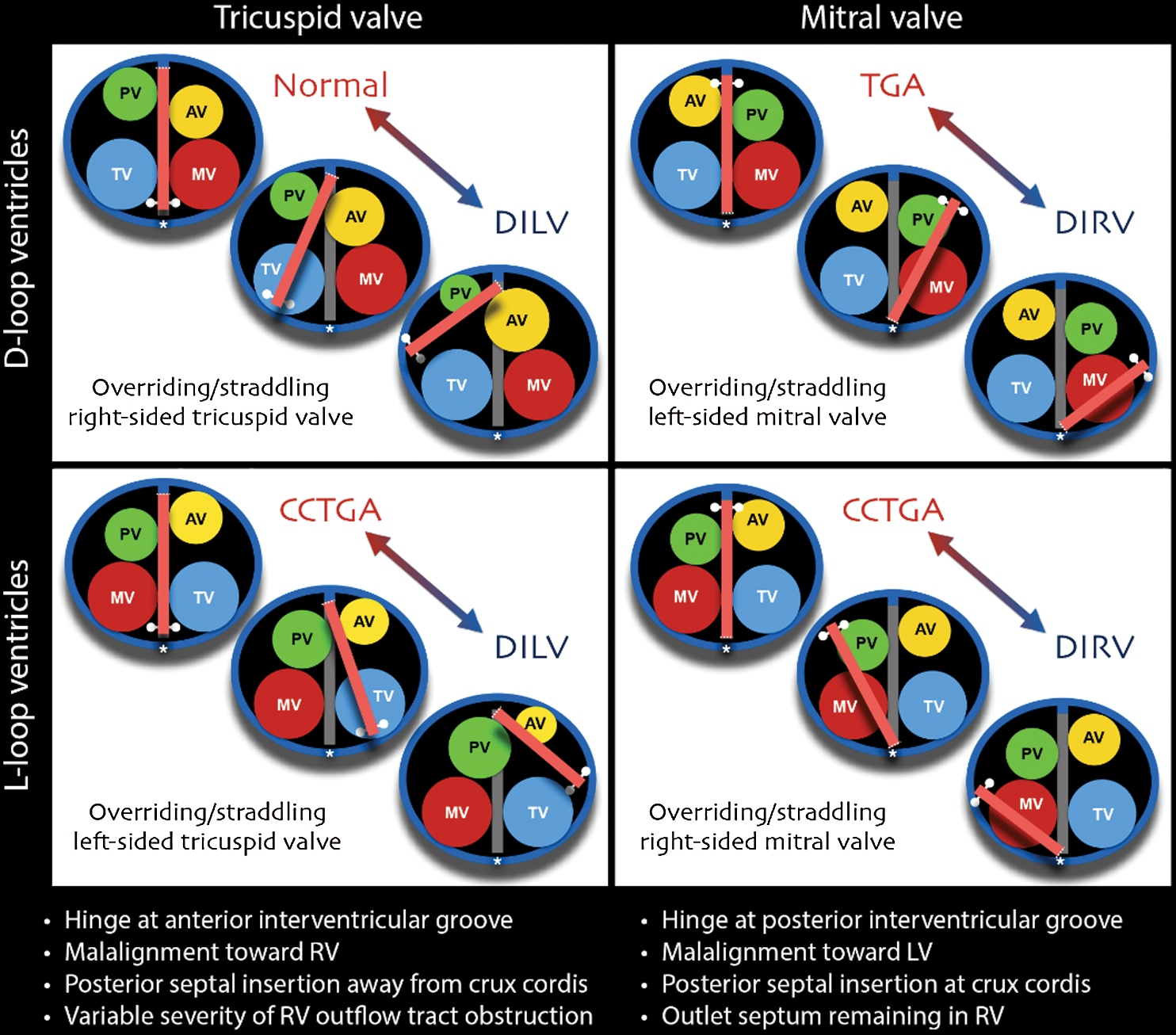
Figure 6: Cartoons of the flap-door mechanisms explaining the spectrums of the overriding tricuspid and mitral valves in the setting of situs solitus and D- and L-loop ventricles. The crux cordis is marked with an asterisk. CCTGA, congenitally corrected transposition of the great arteries; DILV, double inlet left ventricle; DIRV, double inlet right ventricle; LA, left atrium; LV, left ventricle; RA, right atrium; RV, right ventricle; TGA, transposition of the great arteries
4.2 Classic Tricuspid Valve Overriding
The atrial-ventricular septal malalignment is most severe posteriorly at the crux cordis and gradually becomes less severe anteriorly (Fig. 2) [3]. The posterior interventricular groove is offset from the crux cordis toward the side of the right ventricle. The VSD is more conspicuous posteriorly and less conspicuous anteriorly. The posterior medial aspect of the tricuspid valve is the primary site of overriding/straddling. With an increasing degree of malalignment, the ventricular septum becomes more horizontally oriented with the ‘posterior’ interventricular groove displaced superiorly and laterally away from the crux cordis, which is typically seen in hearts with double inlet left ventricle. Depending on the severity of malalignment, the VSD is bordered by different structures. The VSD may appear a perimembranous defect and confined to the inlet part when there is a mild degree of malalignment. With an increasing degree of malalignment, the VSD leaves the expected location of the membranous septum and extends toward the anterior interventricular groove. At the severest form, the VSD is bordered by a complete muscular margin. Previous studies also showed that overriding/straddling tricuspid valve was associated with various forms of VSD [3,5], supporting our observation and interpretation. As the outlet septum is an anterior structure aligned with or close to the anterior interventricular groove, it is only mildly displaced with minimal or mild encroachment of the right ventricular outflow tract. However, it can also be overtly malaligned from the rest of the septum when there is an additional associated conotruncal malformation such as tetralogy of Fallot or double outlet right ventricle.
4.3 Classic Mitral Valve Overriding
The atrial-ventricular sepal malalignment is most severe anteriorly along the anterior interventricular groove and gradually less severe posteriorly (Fig. 3). The ventricular septum inserts to the crux cordis where the interatrial and posterior interventricular grooves are aligned. The VSD is more conspicuous anteriorly and less conspicuous posteriorly. Although the major part of the VSD may appear anteriorly located, the VSD also extends toward the inlet along the mitral and tricuspid valves (Fig. 3) [1]. Therefore, describing the VSD in mitral valve overriding/straddling as an infundibular or anterior VSD by earlier investigators [1,2] is inaccurate and misleading [3,5]. The primary site of overriding/straddling is the anterior medial aspect of the mitral valve. With a lesser degree of overriding, the VSD may appear a perimembranous defect. With a greater degree of overriding, the VSD is at a significant distance from the membranous septal region. In a severe form, the mitral valve can be entirely committed to the right ventricle and the VSD is bordered by a completely muscular margin. As the ventricular outlet is not the primary site of malalignment, there is an offset alignment between the malaligned anterior part of the ventricular septum and the outlet septum. With gradually increasing degree of malalignment, the ventriculoarterial connection transitions from discordant or concordant connection to double outlet right ventricle. Reported cases show that the ventriculoarterial connection is most commonly double outlet right ventricle, less frequently discordant, and rarely concordant [1,4]. The outlet septum when present is usually free-floating in the right ventricular outflow tract with its lower edge not fused to the VSD margin.
4.4 Taussig-Bing Malformation and Mitral Valve Overriding/Straddling
When overriding/straddling mitral valve is associated with double outlet right ventricle or transposition in the setting of situs solitus and concordant atrioventricular connection, the VSD is usually located close to the left-sided pulmonary outflow tract. Because of the hemodynamic similarity, hearts with this combination have been described as Taussig-Bing malformation with mitral valve overriding/straddling [1,4,9–11]. However, it should be understood that Taussig-Bing malformation is associated with malalignment of the outlet or infundibular septum in relation to the rest of the ventricular septum, while double outlet right ventricle with mitral valve overriding/straddling is associated with malalignment between the atrial and ventricular septa (Fig. 7) [12,13]. In addition, mitral valve overriding/straddling is frequently associated with pulmonary outflow tract obstruction, whereas classic Taussig-Bing malformation is frequently associated with aortic outflow tract obstruction [4,5,10]. Although both conditions share a common feature of the VSD in subpulmonary location, they are fundamentally different pathological entities.

Figure 7: Classic Taussig-Bing malformation versus double outlet right ventricle in association with straddling mitral valve. In Taussig-Bing malformation, the VSD (D) is confined to the outlet part of the septum. In mitral valve straddling with double outlet right ventricle, the VSD extends toward the inlet along the tricuspid (TV) and mitral (MV) valves. The anterior interventricular groove is deviated toward the side of the left ventricle (dotted arrow in right lower panel) with its posterior insertion kept at the crux cordis (asterisk in right upper panel). The subpulmonary outflow tract (SP) is stenotic in mitral valve straddling. In Taussig-Bing malformation, the subaortic outflow tract (SA) is narrow. LV, left ventricle; OS, outlet septum; RV, right ventricle
4.5 Double Orifice Tricuspid and Mitral Valves with Straddling
A straddling tricuspid or mitral valve infrequently has two orifices that are supported by their own tension apparatuses (Fig. 4) [3,14–16]. The two orifices may have various degrees of commitment to the underlying ventricles. The hearts with one orifice remaining in the ventricle of its origin and the other orifice committed to the other ventricle are described as double outlet right or left atrium [3,13–15]. Rarely, the valve tissue dividing the two orifices may be firmly attached to the ventricular septal crest, leaving no interventricular communication.
4.6 Atrial-Ventricular Septal Malalignment in Atrioventricular Septal Defects
A common atrioventricular valve overrides and straddles the ventricular septum regardless of the given atrioventricular connection except for rare occasions where it is completely committed to one ventricle. Therefore, ‘overriding’ and ‘straddling’ are of a different significance in the context of a common atrioventricular valve. However, the so-called unbalanced atrioventricular sepal defect may show malalignment between the atrial and ventricular septa that is comparable to the malalignment seen with overriding/straddling tricuspid or mitral valve [1] (Fig. 8).
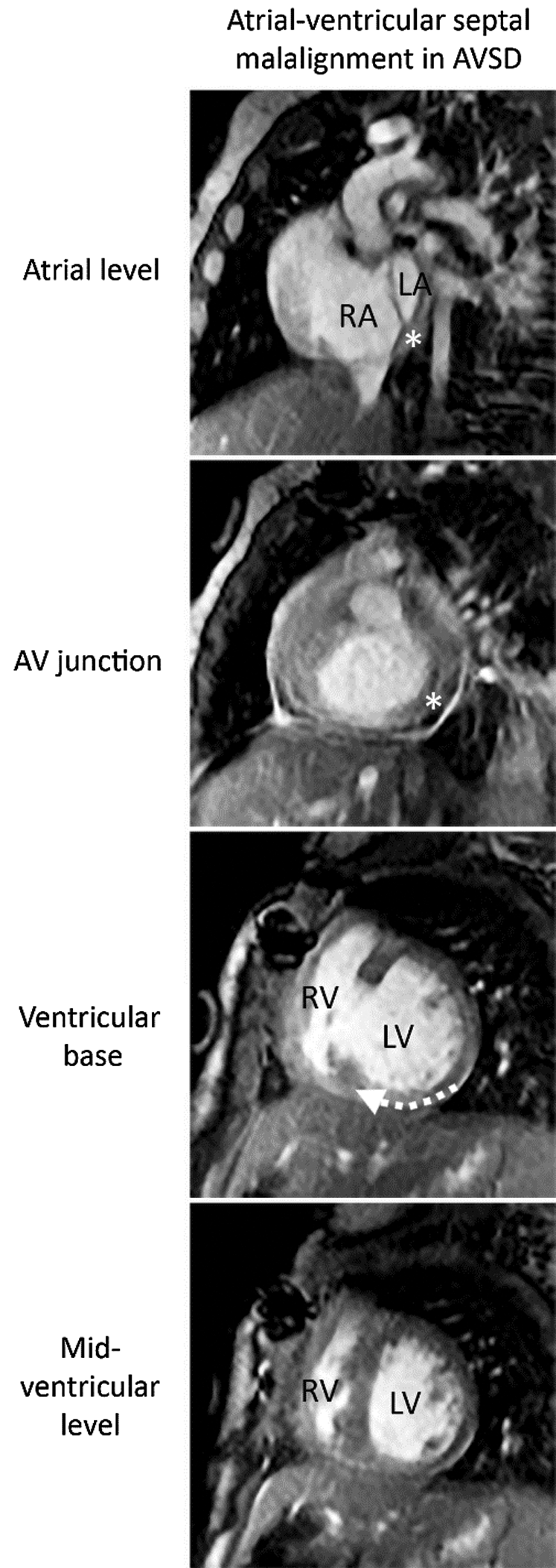
Figure 8: Atrial-ventricular septal malalignment in a patient with unbalanced atrioventricular septal defect (AVSD). The ventricular septum is hinged to the anterior interventricular groove. Its insertion to the posterior interventricular groove is offset from the plane of the atrial septum and the crux cordis (asterisk) and displaced toward the side of the right ventricle (dotted arrow). Note the similarity between this case and the case shown in Fig. 2 second column. As the atrioventricular valve is a common valve, there is no posteromedian muscle ridge formed
4.7 Tricuspid Valve Overriding in Left Juxtaposition of the Atrial Appendages
The tricuspid valve overriding/straddling may be associated with left juxtaposition of the atrial appendages [5,17,18]. Displacement of the major part of the right atrium is associated with abnormal position of the tricuspid valve and abnormal orientation of the atrial septum (Fig. 5). Our 8 patients consistently showed a clockwise rotation of the atrioventricular junction as seen from the apex. As the underlying ventricular septum is less severely displaced than the atrial septum, there is a mild degree of malalignment between the two resulting in a VSD with tricuspid valve overriding. In contrast to the classic cases of tricuspid valve overriding, the VSD in these patients involved only the anterior part of the inlet septum and did not reach the crux cordis (Fig. 5). Overriding was invariably minimal with no straddling. Only 2 patients had chordal attachment to the ventricular septal crest. The tricuspid valve is often hypoplastic [5]
4.8 Disposition of the Tension Apparatus in Classic Straddling Tricuspid and Mitral Valves
The disposition of the tension apparatus is not only variable but also difficult to assess with existing imaging tools. Although our study does not provide accurate information regarding the tension apparatuses, there are a few general features to emphasize.
The tricuspid valve and its tension apparatus appear to retain their usual positions in relation to the atrium that they belong to, while it is the underlying ventricular septum that moves around. The tension apparatus of the straddling part of the tricuspid valve is attached to the posterior medial aspect of the left ventricular wall, the posterior median muscle ridge or the left ventricular aspect of the septum [2]. The straddling tricuspid valve often has an additional chordal insertion to the outlet septum.
When the mitral valve straddles, the primary part of straddling is supported by an additional tension apparatus that is inserted to the ventricular septal crest, the right ventricular aspect of the septum or the right ventricular wall. It may also insert to the medial papillary muscle of Lancisi. On the other hand, the anterolateral and posteromedial papillary muscles keep their usual positions in relation to the atrium. With a greater severity of ventricular malalignment toward the left ventricle, the anterolateral papillary muscle may become a right ventricular structure. In the severest form, both anterolateral and posteromedial papillary muscles belong to the right ventricle, and the left ventricle remains as a slit of cavity posteriorly at the corner of the crux cordis without papillary muscles.
Echocardiography plays a primary role in the diagnosis of overriding/straddling tricuspid or mitral valve [3,4,19–21]. A four-chamber plane and tailored long-axis planes appear the most commonly used imaging planes. However, precise assessment of the nature and severity of the septal malalignment and valve overriding requires short-axis images [3,4]. En-face view of the atrioventricular junction using 3D echocardiography allows precise determination of the relationship of the overriding valve annulus to the ventricular septum [21]. The stack of short-axis images also provides the information regarding the disposition of the papillary muscles. While short-axis imaging at echocardiography is often limited, CMR provides unlimited choice of orientation for imaging planes that are evenly spaced and strictly parallel to each other. Echocardiography and CMR are complementary.
This retrospective study is limited by small numbers of each group of patients and lack of accurate surgical or pathological correlation. The study population does not reflect the whole cohort of a large referral center in this retrospective study that included the cases with adequate image quality only. The concept that we introduce in this paper is the general rule and does not apply to all cases. Examples of exception to these rules include twisted or criss-cross hearts, which are often associated with overriding/straddling atrioventricular valves [1,4,5]. The atrioventricular junction in this particular pathology is different in every individual case and hard to conceptualize.
Overriding/straddling tricuspid and mitral valves constitute spectrums of abnormal atrioventricular connection ranging from biventricular connection to double inlet right or left ventricular connection. The pathological constellations of overriding/straddling valves can be easily understood by analogizing the malaligned part of the ventricular septum to a flap-door panel hinged to the anterior or posterior interventricular groove and describing the modifiers of malalignment. Contrary to what has generally been known, the VSD is not limited to inlet or outlet part of the ventricular septum. While echocardiography is the primary diagnostic modality, CMR plays an important complementary role. Evenly spaced stacks of images in short-axis plane provide objective and accurate information regarding the nature and severity of the septal malalignment, the severity of overriding, and the disposition of the tension apparatus.
Acknowledgement: We thank Dr. Christopher Lam for valuable comments and corrections on the manuscript.
Funding Statement: The authors received no specific funding for this study.
Conflicts of Interest: The authors declare that they have no conflicts of interest to report regarding the present study.
1. Milo, S., Ho, S. Y., Macartney, F. J., Wilkinson, J. L., Becker, A. E. et al. (1979). Straddling and overriding atrioventricular valves: Morphology and classification. American Journal of Cardiology, 44(6), 1122–1134. DOI 10.1016/0002-9149(79)90178-4. [Google Scholar] [CrossRef]
2. Wenink, A. C., Gittenberger-de Groot, A. C. (1982). Straddling mitral and tricuspid valves: Morphologic differences and developmental backgrounds. American Journal of Cardiology, 49(8), 1959–1971. DOI 10.1016/0002-9149(82)90216-8. [Google Scholar] [CrossRef]
3. Pessotto, R., Padalino, M., Rubino, M., Kadoba, K., Büchler, J. R. et al. (1999). Straddling tricuspid valve as a sign of ventriculoatrial malalignment: A morphometric study of 19 postmortem cases. American Heart Journal, 138(6), 1184–1195. DOI 10.1016/S0002-8703(99)70086-4. [Google Scholar] [CrossRef]
4. Fraisse, A., del Nido, P. J.,Gaudart, J., Geva, T. (2001). Echocardiographic characteristics and outcome of straddling mitral valve. Journal of the American College of Cardiology, 38(3), 819–826. DOI 10.1016/S0735-1097(01)01441-3. [Google Scholar] [CrossRef]
5. Bharati, S., McAllister Jr, H. A., Lev, M. (1979). Straddling and displaced atrioventricular orifices and valves. Circulation, 60(3), 673–684. DOI 10.1161/01.CIR.60.3.673. [Google Scholar] [CrossRef]
6. Yoo, S. J., Saito, M., Hussein, N., Golding, F., Goo, H. W. et al. (2020). Systematic approach to malalignment type ventricular septal defects. Journal of the American Heart Association, (In press). [Google Scholar]
7. Bevilacqua, M., Sanders, S. P., Van Praagh, S., Colan, S. D., Parness, I. (1991). Double-inlet single left ventricle: Echocardiographic anatomy with emphasis on the morphology of the atrioventricular valves and ventricular septal defect. Journal of the American College of Cardiology, 18(2), 559–568. DOI 10.1016/0735-1097(91)90615-G. [Google Scholar] [CrossRef]
8. Devloo-Blancquaert, A., Ritter, D. G. (1978). Muscle ridge between atrioventricular valves and malalignment of junction of these valves with ventricular septum. British Heart Journal, 40(11), 1267–1274. DOI 10.1136/hrt.40.11.1267. [Google Scholar] [CrossRef]
9. Kitamura, N., Takao, A., Ando, M., Imai, Y., Konno, S. (1974). Taussig-Bing heart with mitral valve straddling: Case reports and postmortem study. Circulation, 49(4), 761–767. DOI 10.1161/01.CIR.49.4.761. [Google Scholar] [CrossRef]
10. Muster, A. J., Bharati, S., Aziz, K. U., Idriss, F. S., Paul, M. H. et al. (1979). Taussig-Bing anomaly with straddling mitral valve. Journal of Thoracic and Cardiovascular Surgery, 77(6), 832–842. DOI 10.1016/S0022-5223(19)38185-1. [Google Scholar] [CrossRef]
11. Stellin, G., Zuberbuhler, J. R., Anderson, R. H., Siewers, R. D. (1987). The surgical anatomy of the Taussig-Bing malformation. Journal of Thoracic and Cardiovascular Surgery, 93(4), 560–569. DOI 10.1016/S0022-5223(19)36385-8. [Google Scholar] [CrossRef]
12. Koshiyama, H., Aoki, M., Akiyama, S., Nakamura, Y., Hagino, I. et al. (2014). Successful biventricular repair of double-outlet right ventricle with transposition of the great arteries, pulmonary stenosis, and straddling mitral valve. Annals of Thoracic Surgery, 97(4), 1431–1433. DOI 10.1016/j.athoracsur.2013.07.063. [Google Scholar] [CrossRef]
13. Yim, D., Dragulescu, A., Ide, H., Seed, M., Grosse-Wortmann, L. et al. (2018). Essential modifiers of double outlet right ventricle: Revisit with endocardial surface images and 3-dimensional print models. Circulation Cardiovascular Imaging, 11, e006891. [Google Scholar]
14. Eberhardt, L., Chetaille, P., Kreitmann, B. (2005). A very unusual combination of straddling and overriding of the tricuspid valve associated with clefting of the mitral valve. Cardiology in the Young, 15(4), 422–424. DOI 10.1017/S1047951105000879. [Google Scholar] [CrossRef]
15. Edwin, F., Kinsley, R. H., Mamorare, H. M., Govendrageloo, K. (2012). The spectrum of double-outlet right atrium including hearts with three atrioventricular valves. European Journal of Cardiothoracic Surgery, 41(4), 947–949. DOI 10.1093/ejcts/ezr073. [Google Scholar] [CrossRef]
16. Beroukhim, R. S., Geva, T. (2010). Echocardiographic features of double-outlet right atrium and straddling tricuspid valve with intact ventricular septum: A rare cardiac anomaly associated with pulmonary atresia and single coronary artery ostium. Journal of the American Society of Echocardiography, 23(5), 580.e5–580.e10. DOI 10.1016/j.echo.2009.09.027. [Google Scholar] [CrossRef]
17. Zhang, Y. Q., Yu, Z. Q., Zhong, S. W., Wu, L. P., Chen, G. Z. et al. (2010). Echocardiographic assessment of juxtaposition of the right atrial appendage in children with congenital heart disease. Echocardiography, 27(7), 878–884. DOI 10.1111/j.1540-8175.2009.01148.x. [Google Scholar] [CrossRef]
18. Frescura, C., Thiene, G. (2012). Juxtaposition of the atrial appendages. Cardiovascular Pathology, 21(3), 169–179. DOI 10.1016/j.carpath.2011.02.002. [Google Scholar] [CrossRef]
19. Smallhorn, J. F., Sutherland, G. R., Anderson, R. H., Macartney, F. J. (2082). Cross-sectional echocardiographic assessment of conditions with atrioventricular valve leaflets attached to the atrial septum at the same level. British Heart Journal, 48(4), 331–341. DOI 10.1136/hrt.48.4.331. [Google Scholar] [CrossRef]
20. Barron, J. V., Sahn, D. J., Valdes-Cruz, L. M., Lima, C. O., Grenadier, E. et al. (1984). Two-dimensional echocardiographic evaluation of overriding and straddling atrioventricular valves associated with complex congenital heart disease. American Heart Journal, 107(5), 1006–1014. DOI 10.1016/0002-8703(84)90842-1.
21. Vogel, M., Ho, S. Y., Lincoln, C., Anderson, R. H. (2000). Transthoracic three-dimensional echocardiography for the assessment of straddling tricuspid or mitral valves. Cardiology in the Young, 10(6), 603–609. DOI 10.1017/S104795110000888X. [Google Scholar] [CrossRef]
 | This work is licensed under a Creative Commons Attribution 4.0 International License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. |