| Computers, Materials & Continua DOI:10.32604/cmc.2022.031376 | |
| Article |
Innovative Fungal Disease Diagnosis System Using Convolutional Neural Network
1Department of Computer Science, Lahore Garrison University, Lahore, 54000, Pakistan
2Networks and Communications Department, College of Computer Science and Information Technology, Imam Abdulrahman Bin Faisal University, P.O. Box 1982, Dammam, 31441, Saudi Arabia
3Department of General Education, Skyline University College, University City of Sharjah, UAE
4Higher Colleges of Technology, Abu Dhabi, UAE
5Department of Enterprise Computing, Skyline University College, Sharjah, UAE
6Department of Computer Science, University of South Asia, Lahore, 54000, Pakistan
*Corresponding Author: Tahir Alyas. Email: tahiralyas@lgu.edu.pk
Received: 16 April 2022; Accepted: 26 May 2022
Abstract: Fungal disease affects more than a billion people worldwide, resulting in different types of fungus diseases facing life-threatening infections. The outer layer of your body is called the integumentary system. Your skin, hair, nails, and glands are all part of it. These organs and tissues serve as your first line of defence against bacteria while protecting you from harm and the sun. The It serves as a barrier between the outside world and the regulated environment inside our bodies and a regulating effect. Heat, light, damage, and illness are all protected by it. Fungi-caused infections are found in almost every part of the natural world. When an invasive fungus takes over a body region and overwhelms the immune system, it causes fungal infections in people. Another primary goal of this study was to create a Convolutional Neural Network (CNN)-based technique for detecting and classifying various types of fungal diseases. There are numerous fungal illnesses, but only two have been identified and classified using the proposed Innovative Fungal Disease Diagnosis (IFDD) system of Candidiasis and Tinea Infections. This paper aims to detect infected skin issues and provide treatment recommendations based on proposed system findings. To identify and categorize fungal infections, deep machine learning techniques are utilized. A CNN architecture was created, and it produced a promising outcome to improve the proposed system accuracy. The collected findings demonstrated that CNN might be used to identify and classify numerous species of fungal spores early and estimate all conceivable fungus hazards. Our CNN-Based can detect fungal diseases through medical images; earmarked IFDD system has a predictive performance of 99.6% accuracy.
Keywords: Deep machine learning; CNN; ReLU; skin disease; fungal
The clinical manifestations of dermatitis vary greatly. They might be transient or persistent, and they can be pleasant or unpleasant. Most have contextual origins, such as climate change or other factors, while some are hereditary. Several sores or syndromes are mild and not life-threatening, while others can be fatal. Child’s clinical manifestations come in a variety of forms. Bacterial pathogens, fungus, and viral diseases are the three types of infectious diseases [1]. Whereas most skin diseases are minor, others might indicate a more significant problem. Infections caused by fungi are widespread all over the world. Fungi human pathogens arise when an invasive fungus takes control of a section or part of the body so that the body’s immune system is unable to control it. The fungus may exist in the atmosphere, soils, waters,flora, and mammals [2]. In the human body, there is a certain fungus that exists naturally. There are two sorts of fungal species: those that are innocuous and those that are dangerous. When dangerous fungi enter the body, they might be difficult to eradicate because they can live in the environment and re-infect the patient attempting to recover [3].
Diabetic patients with a compromised immune system are especially vulnerable to the fungus. Rashes on non-infected human body areas can result from fungal diseases in a person’s body. A fungus on foot, for instance, may spread to the fingers [4]. Several distinct forms of fungal diseases can affect your skin, hair, nails, and body. These can also transmit from one human to the other, from animal to human, or, in rare cases, from the earth, air, and water to a human. Some fungal skin disorders are caused by an overabundance of your own healthy fungus. When people encounter an infectious person or animal and soil or air, people may start picking up fungi that cause illness. As a result, persons who participate in sports are more likely to get fungal skin infections. By exchanging contaminated objects such as clothing, towels, hairbrushes, socks, bedclothes, shoes, and so on, you might become infected with fungus. Fungi can be picked up by your feet or body in pool areas [5].
The type of fungus infection that is produced by this illness, as well as where it is located, determine the symptoms of fungal infection. The fungus might damage only one region of your body, or it can move from one place to another. Changes in your skin, hair, nails or other body parts may occur or may not bother you or cause discomfort. Fungal skin infections can result in various rashes and infections on the skin. Some are itchy, red, black, scaly, and pigmented and others may create an remarkable scale [6]. Candidiasis (Yeast Infection), Tinea infections, Tinea pedis, Tinea Captis and Nail ringworm are many forms of fungal diseases. Candida can overproduce if good bacteria numbers are disrupted or weakened by the immune system [7]. In Fig. 1 shows the candidiasis mouth infection with white spots.

Figure 1: Candidiasis mouth infection
Candidiasis, also known as moniliasis, is a yeast infection that affects the skin and mucous membranes. While yeast is an ordinary tenant of the colon and vaginal region, it is typically harmless. Candida can cause diseases assuming it outgrows control or, on the other hand, if it enters profound into the body. Antibiotics have also been linked to the growth of candida yeast [8]. Antibiotics, a high-sugar diet, excessive alcohol consumption, a compromised immune system, oral contraceptives, diabetes, and high-level stress are seven variables that might contribute to Candidiasis overgrowth. Candidiasis is a fungal infection that affects many body regions, most commonly the skin folds or the navel. Symptoms include rash, patches, pimples, itching, and burning. The signs of thrush in the mouth are as follows: Tongue and inner cheeks have white spots. The possible symptoms of pain at the corners of the mouth, on the corner of the lips edges, and cracks and minor cuts can be observed. Beds of nails, swelling, pain, pus, and a distinct white or yellow nail indicate fungal disease.
Brief medical history, clinical assessment of the children’s epidermal scrape, cultured scrape, blood sample, and faeces test are all used to diagnose this illness [9]. Medicating creams were used extensively to treat the condition. Severe infection in an immune-compromised kid is generally treated with oral anti-yeast medicine [10]. Suppositories are used to treat vaginal yeast infections.
Dermatitis is a crucial pathogen skin infection that caterpillars do not cause Tinea. Various organisms, contingent upon their area on the body, cause ringworm. It is brought about by a parasitic disease (not a real worm). Organisms on the skin, hair, and nail bed are called dermatophytes. Fig. 2 shows ring-shaped, red, black, scaly patches with clear centres, indicative of ringworm. Other children or animals with The first line of treatment for this infection is medication, followed by homecare, which includes avoiding clothing that irritates the infected area, covering it with a dressing if you can’t avoid it, washing the diseased area and clothes daily to help disinfect your environments, cleaning and drying your infected area daily. Constricting ringworm is more likely in malnourished children who have poor hygiene, live in a warm area, have contact with other children or animals with ringworm infection, or are immunocompromised due to sickness or medication [11].

Figure 2: Tinea infections
Athletes’ foot fungus usually starts in the toes. It is most frequent in persons whose feet have gotten extremely sweaty due to being crammed into tight-fitting shoes. This frequent disease mainly affects [12] adolescent and adult males, as showed in Fig. 3.

Figure 3: Foot infection
A lot is going on physiologically throughout puberty, from changes in skin cells on the scalp to sweat glands in the feet—hormones released during this development period cause several physical and mental changes. Adolescents can navigate this difficult period by understanding exactly what is going on with their bodies. Its modest ramifications for children before to adolescence Sweating, not drying feet after swimming, wearing tight skin-fit socks and shoes, and warm climate circumstances are all causes of athlete’s foot [13]. Infections are treated in a variety of ways. Keep your feet clean and dry, and change your socks every day [14].
Scalp ringworm is a fungus that infects the hair on the scalp and the skin around it. Ringworm is a typical disease of the skin and nails brought about by organisms. The disease is designated “ringworm” since it can cause an irritated, red, roundabout rash. It occurs commonly in children, and it can also occur in grownups [15].
It typically affects youngsters between the ages of 2 and 10. Fig. 4. shows red and grey rings, scaly rash on the scalp, irritation of the scalp, hair loss on the infected region, rash elsewhere on the body, and occasionally bald spots. Tinea capitis is treated with an oral antifungal medicine that can only be obtained with a doctor’s prescription and medicated antifungal shampoo to prevent the fungus infection from spreading to others.
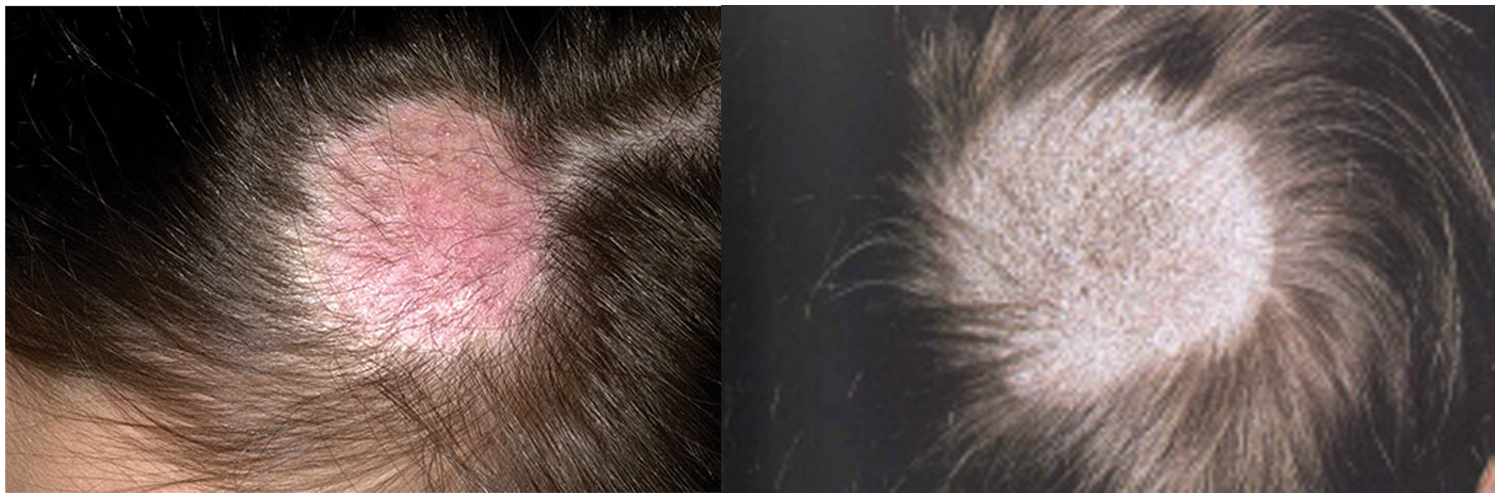
Figure 4: Scalp ringworm
Nail ringworm is a fungal infection that causes a thicker and deformed nails on the fingers or toes, as shown in Fig. 5. This illness affects the toenails more than the fingernails. The thickening of the ends of the nails and the yellow hue of the nails are also signs of nail ringworm. This infection is more common in adults and teenagers than in children. The therapy for nail ringworm begins with a visit to a dermatologist. Apply the antifungal cream your doctor advises, then wash and dry the affected area with a clean towel.

Figure 5: Nail ringworm
Tinea versicolor is a skin condition characterized by light or brighter areas of skin. As indicated in Fig. 6, patchwork is more often present on the chest trunks and shoulders. Adolescence and early adulthood are the most common times for it to occur. The fungus disrupts the skin’s normal pigmentation, resulting in small, discoloured areas. The hue of these areas is generally dimmer or darker [16].

Figure 6: Light and dark patches
Its clinical signs are as follows: white, pink, and dark-coloured spots appear primarily in the summer, infect only on the top layer of the skin, and the rash may appear on the trunk. Rash on the face is a rare occurrence. Heat exacerbates spots, Tinea versicolor diagnosis and therapy are based on the medical history of the sick person, physical examination, and the use of ultraviolet (UV) light to better visualize the patches. The skin can be scraped for culture, and medicated antimicrobial dandruff shampoo can be applied to the skin. The shampoo is applied to the skin overnight and then rinsed off the next day. Shampoo therapy is beneficial when it comes to being effective. Topical creams or oral antifungal medicines may be prescribed. Using computer-aided digital image processing design, this system may be used in hospitals to diagnose fungal illnesses properly. The effectiveness of the method is demonstrated in the outcomes section.
In children with cystic fibrosis, fungal lung disease manifests differently in immunocompetent, immunocompromised, and fibrosis patients. Pulmonary mycoses are the least common in immunocompetent youngsters, with endemic mycoses and Aspergillomas being the most common. Fungal respiratory infections occur more frequently and with greater severity in individuals with compromised [17]. Filamentous fungi like Aspergillus and Scedosporium have been isolated from the respiratory secretions of cystic fibrosis patients more frequently in recent years.
Bacterial infections of the salivary glands occur in people with pre-existing diseases such as surgical healing, diabetes, or immunodeficiency. Bacterial infections are much less common than viral ones. A ductal obstruction or a retrograde progression of infection up the duct due to diminished salivary flow causes these infections. Radiation therapy or antidepressants may diminish salivary flow, allowing staphylococcal and streptococcal strains associated with the oral mucosa biofilm to infect the salivary gland [18].
The management of invasive fungal infections (IFI) in immunocompromised patients and those with predisposing factors is still a complicated topic worldwide. Medical education is a difficult task that necessitates resources and ongoing professional competency improvements. New medical advances and discoveries cannot be set aside for regular medical practice; they must be integrated immediately to meet present demands [19].
One of the most severe health issues among people with type 2 diabetes is a fungus, particularly Candida albicans. As a result, the goal of this study was to conduct a systematic review and meta-analysis to establish the prevalence of C. Albicans skin infection in individuals with type 2 diabetes. A comprehensive Meta-Analysis was used to examine the data. The random-effects model was utilized. The random-effects model was utilized for analysis, and the I2 index was used to measure study heterogeneity. To give up-to-date information on the performance and advances of polymerase chain reaction (PCR) methods to detect fungi that typically cause invasive fungal illness, this review has incorporated the knowledge and experience of the leads of each laboratory working team of the fungal PCR initiative. A molecular diagnosis of IFDD supplements the present array of mycological investigations. Providing better sensitivity and turnaround time over traditional methods while retaining the advantages of traditional tests (e.g., species-level identification and resistance identification) [20].
While host vulnerability may explain the occurrence of childhood disorders to some degree, exposure to infected people is essential. Posture rates of creatures in clinically normal scalps in widespread parts may be as high as 4%. Some of these children may develop ringworm, or the exporter status may be reversed. The mixture of high rates of endemicity, slight clinical signs of infection, and incapability to mount actual control measures has led to the continuance of hyperendemic foci for scalp ringworm. Typical causative organisms are Trichophyte tonsures (USA), Trichophyte Sudanese and Microspores Baudouin (Africa), and Trichophyte violaceus (North Africa, Middle East, and the Indian subcontinent). The diagnosis of the invasive fungal disease remains a problem for clinicians, and ever-changing treatment regimens raise patients’ risk of invasive infection. In a hematopoietic stem cell transplant patient with graft-vs.-host disease, genetic testing led to the discovery of co-infection with two fungus infections causing invasive illness [21].
There are various reasons to undertake epidemiological research to assess the prevalence of oral candidiasis, including the possibility of a link between it and potentially malignant mucosal illnesses, as there is a link. Most oral health epidemiological research in Brazil focuses on tooth-related diseases. They integrate biological elements such as the prevalence of oral bacteria and serum cytokines in their techniques and the World health organization (WHO) recommended parameters. At the same time, industrialized and high-income countries have looked into these variables in conjunction with other diseases that affect the stomatognathic system. For optimum antifungal medication and prompt de-escalation of therapy, identifying the fungi that cause invasive mycosis is critical. The author showed that the internal transcribed spacer (ITS) 2 and D2 territory is very penetrating and precised for identifying fungal in individuals with a known finding of IFDD investigation. Fungi patterns in tissues and sterile bodily fluids taken from various sources had a sensitivity of 96.6 percent and a specificity of 98.2 percent in this cohort. A galactomannan was found in 43.9 percent of aspergillosis patients and 71.8 per cent of fungal sequencing [22].
The Proposed IFDD system empowered with transfer learning consists of training and deployment modules as shown in Figs. 7 and 8. The dataset is acquired from the kaggle website in the training module and uses an image stream from the camera. The converted images may need to be normalized due to low quality of camera resolution or any other reasons. Image preprocessing may convert the noisy images into fine quality using the data cleaning process. This dataset is augmented using Flip, Affine, Multiply, Linear-contrast, and Gaussian-Blur techniques to enhance the number of images for training. This preprocessed and augmented dataset is further divided into a training dataset and validation dataset with a ratio of 75%:25%, respectively. The first image and last three layers are configured for the desired dataset. The AlexNet pre-trained model with 1000 classes is imported from the cloud. The training dataset trains the customized model. After the testing dataset is validated on this trained model to check the validity of the trained model. If the results of the trained model with the testing dataset meet the threshold value, then save this trained model in the cloud for further application or retrained model to achieve the desired accuracy.
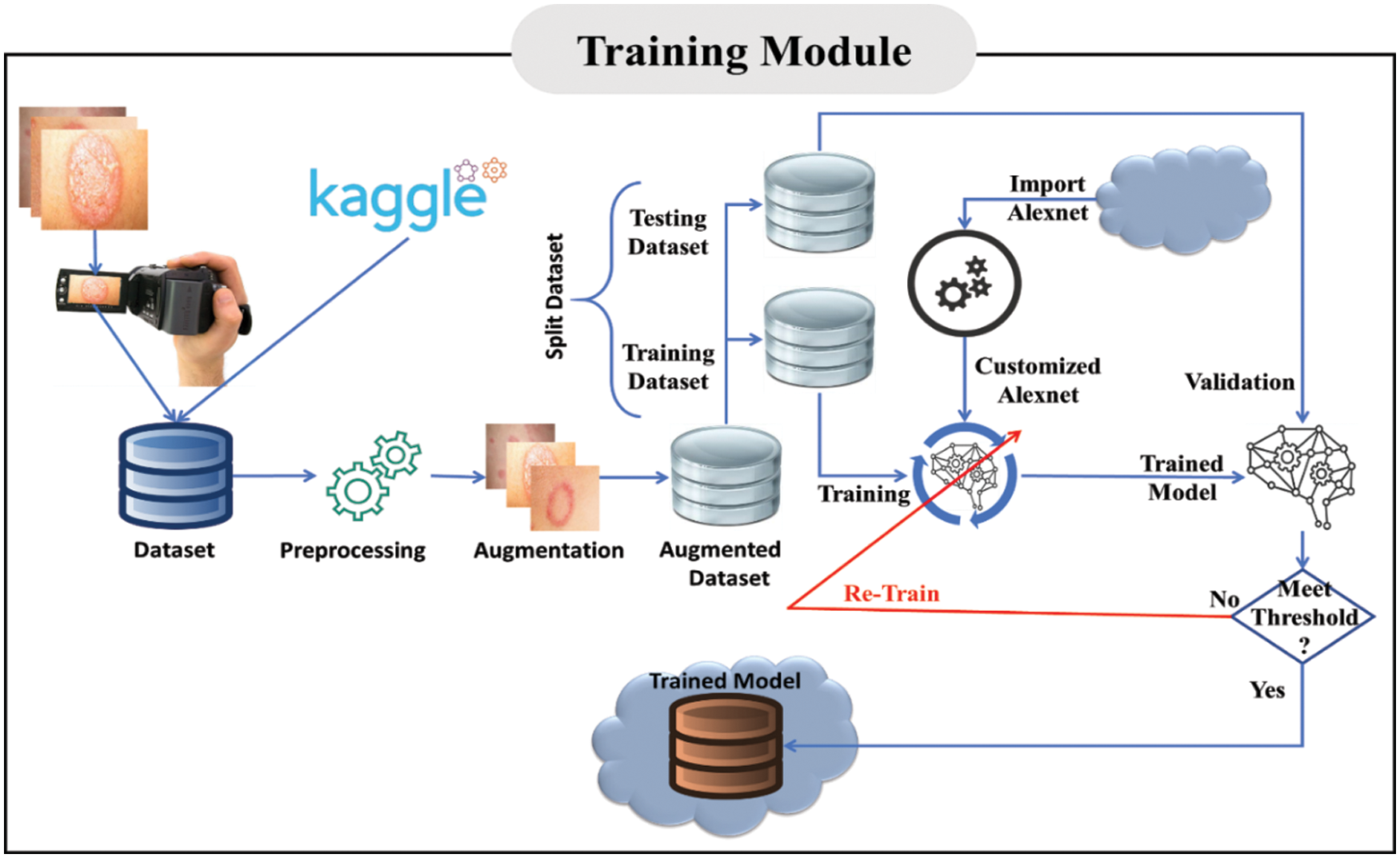
Figure 7: Training module of the proposed system
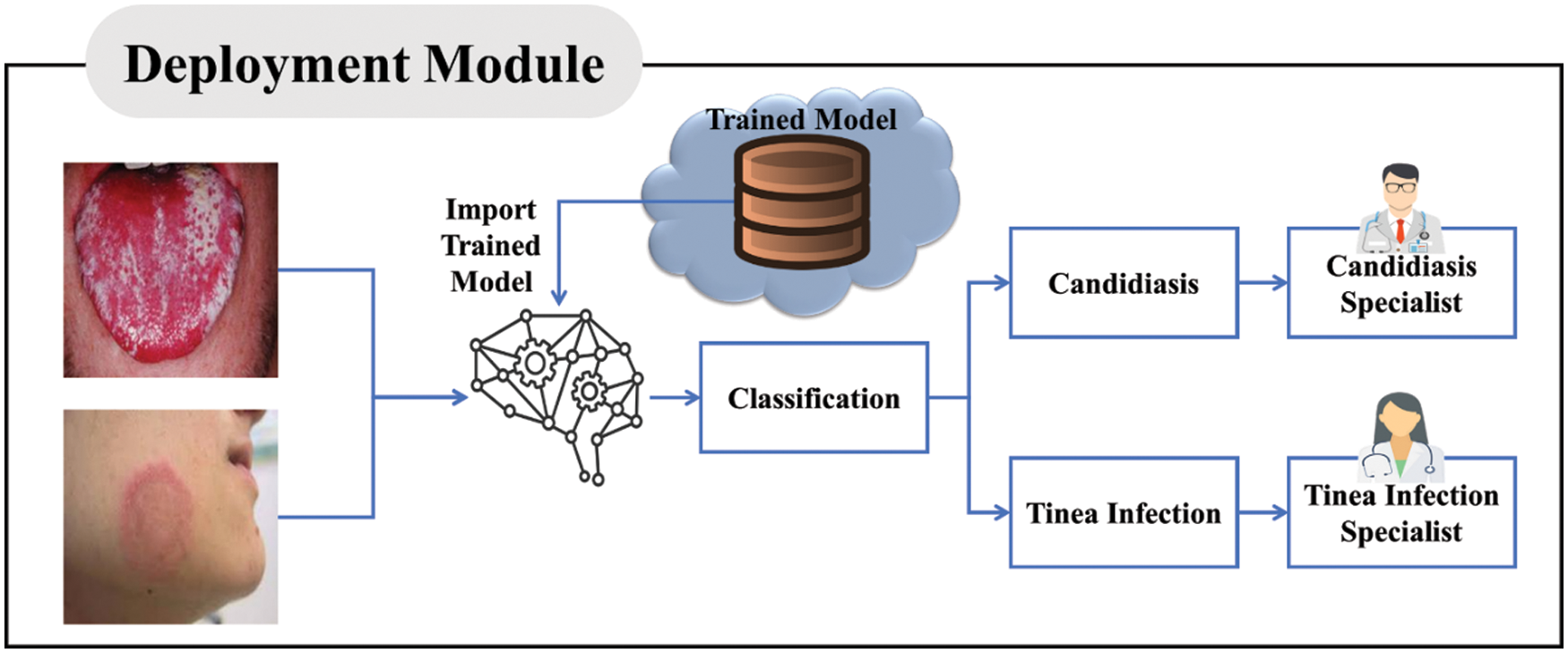
Figure 8: Deployment module of the proposed IFDD system
In Fig. 8 shows the working of the trained model and classification of the proposed IFDD system. In the deployment module, a patient sends the image of his\her infected area to the system, or a camera can take an actual-time image. A trained model is imported from the cloud storage to classify the disease. After classification, there are two possibilities: candidiasis disease or a Tinea infection. This model also recommends the desired specialist for the disease.
The input image stream may have noise, blurriness, and data not in a straightforward form, resulting in raw shape data that cannot yield acceptable image classification results. By reducing noise and blurriness, the preprocessing layer improves the quality of the raw photos. To reduce the noise and blurriness, multiple filters are utilized, which are the inputs of the configured AlexNet. The preprocessing of the input raw data stream is depicted in Fig. 9

Figure 9: Pre-processing image data
The captured image may not be of good quality due to noise or blurriness. Given below Eq. (1) of the noisy image.
where,
Due to its simplicity, the Gaussian noise model is widely used in Eq. (2). The Gaussian noise model can produce better results as compared to others models. This model is mathematically represented in Eq. (3).
where
The black dots on the images represent the impulse valued noise. The centred value 95 is overwritten by the value with 0 in Fig. 10 is noise.
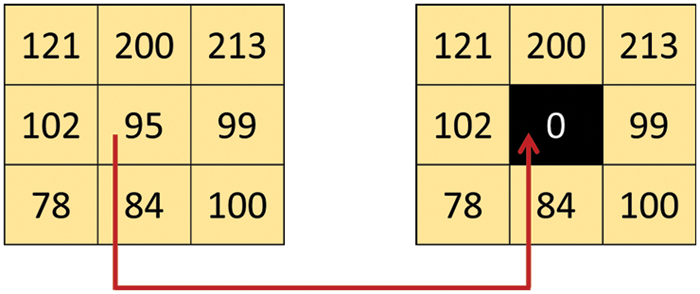
Figure 10: Salt pepper noise has tainted the pixel value
Machine Learning employs different methods such as Support Vector Machines (SVMs), Linear Regression, Decision Trees, and Neural Networks to address various problems. It’s a sophisticated object classification model. It’s a collection of layers that are joined in a specific order. These layers are the Convolution layer, which performs the convolution process, the Pooling layer, which performs the pooling process, the normalization layer, which performs the activation (ReLU) process, and the fully connected layer performs the fully connected process (Dense). It can have numerous convolution, pooling, and normalization layers, and they don’t have to be in that order. The full CNN Model employed in the proposed IFDD system Empowered with CNN is shown in Fig. 11.
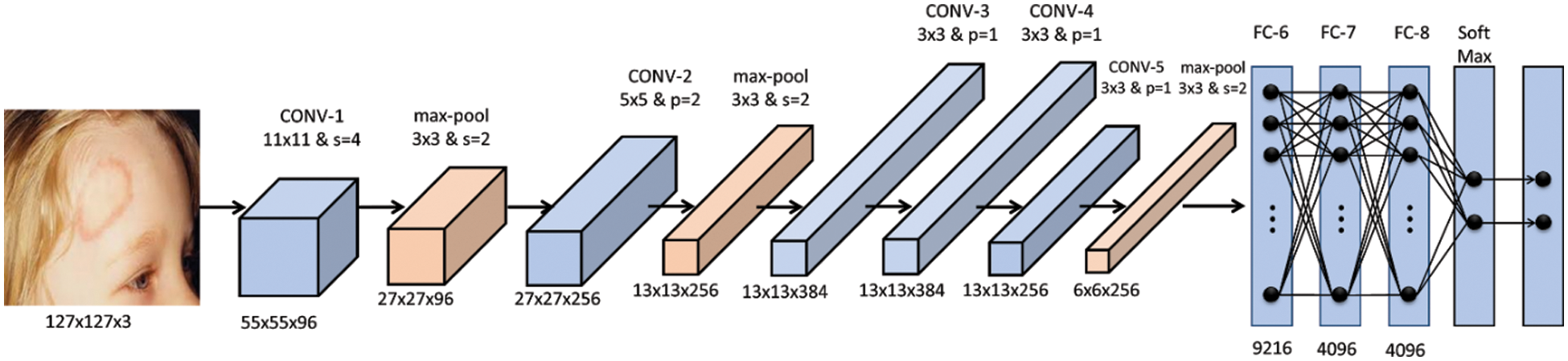
Figure 11: CNN model of the proposed IFDD system
For the acquisition of the images, many ways are employed using kernel technique. To acquire the features of the images using the kernel, many ways are employed. A kernel/filter matrix is utilized at the convolutional layer level to extract the object’s feature for the next layer. The kernel order can be changed to produce a new feature map or extend the data in one dimension while shrinking it. A kernel/filter matrix is utilized at the convolutional layer level to extract the object’s feature for the next layer. The kernel order can be changed to produce a new feature map or extend the data in one dimension while shrinking it. The sum of the product can be used to compute the values of the feature map.
Fig. 12 shows the low-level diagram of a convolution that converts the input matrix into the next layer by using the kernel. The Eq. (4) is used to calculate the convolution for the one pixel for the next layer
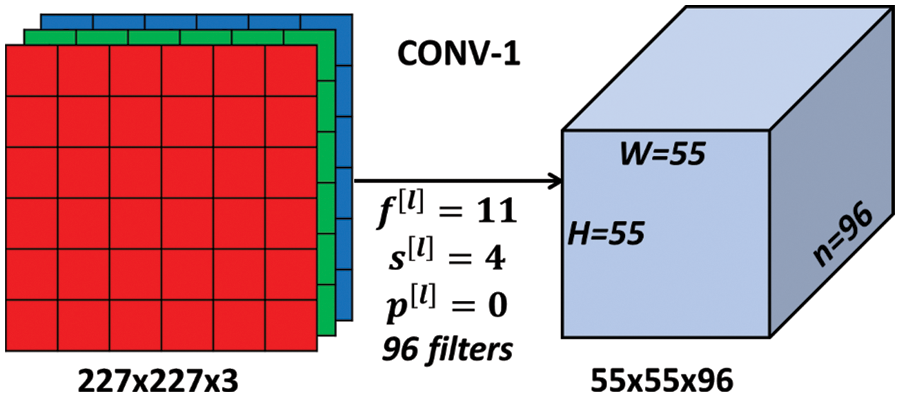
Figure 12: Convolutional layer in proposed IFDD system
A convolutional layer is the foundation of CNN, which is utilized for feature detection. Assume a 7 × 7 matrix with three RGB channels, a kernel of size 3 × 3 with three RGB, and stride value with 1, which showed in Fig. 13.
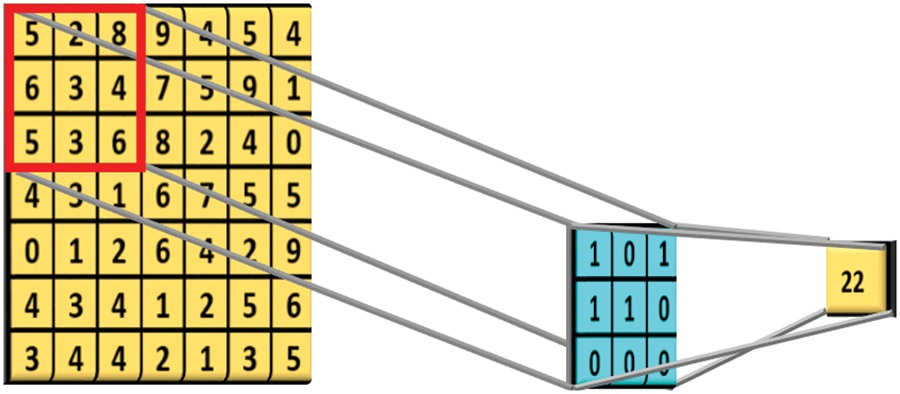
Figure 13: Feature matrix of size 3 kernal
The resultant map can be computed using the following Eq. (5) if the kernel 3 × 3 moves across the image 7 × 7 matrix with stride 1.
Where,
As a result, the produced feature map has a dimension of 5 × 5. Rectified Linear Unit (RLU) is a frequent activation function in neural networks, but especially on CNN as shown in Fig. 14. It is defined, mathematically in Eqs. (6) and (7)
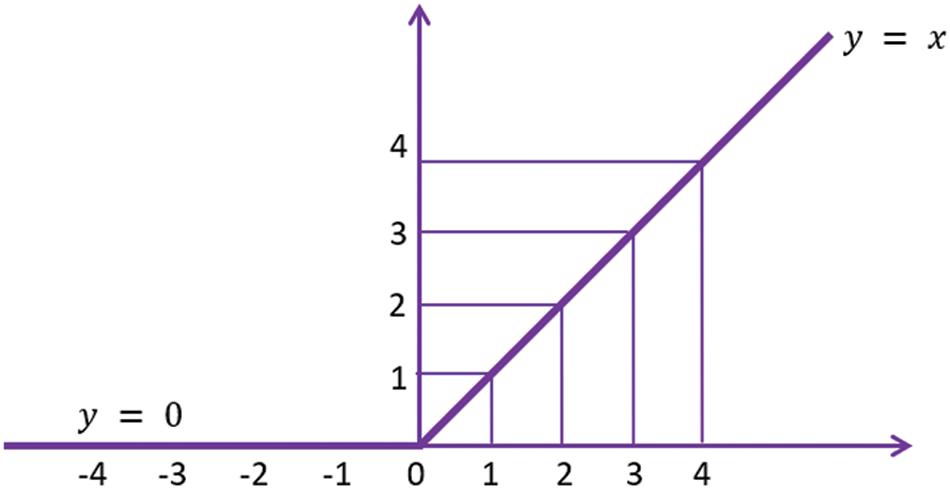
Figure 14: Rectified linear unit of the proposed IFDD system
In Fig. 14 shows the rectified linear unit values of
The max-pooling layer reduces the input values by weight and height but not depth. In CNN of the proposed IFDD system, 2 × 2 filter and stride value 2 is used as shown in Fig. 15.
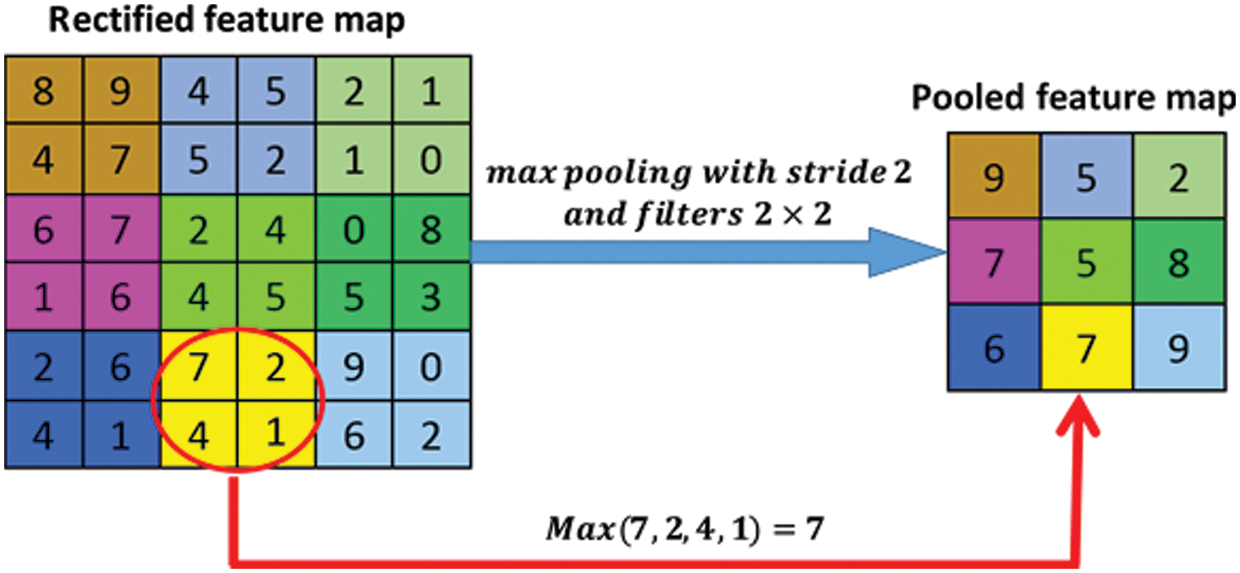
Figure 15: Pooled feature map
The classification layer results are produced by the final fully-connected layer, which is the input of the SoftMax layer. The output unit activation function is the SoftMax function in Eq. (8).
where
After the fully connected layer, the SoftMax function is used for a multiclass classification problem as shown in Eq. (9).
where
Several investigative approaches like computed tomography (CT), cell biopsy tests and medical resonance imaging (MRI) scan are used to detect fungal diseases. However, these examination measures are costly and time-consuming. As a result, this study developed a new technique that combines traditional learning algorithms like CNNs and support vector machines to create a hybrid classifier.
MATLAB-2020 is used for the simulation of the proposed IFDD system. A dataset used for simulation contains 4000 images classified into Candidiasis and Tinea Infections. The dataset was split into 75% images for training and 25% for validation. Figs. 16 and 17 show the performance graph and loss rate of system. The training rate of the proposed system is 99.6% shown in Fig. 16 and loss is 0.4% as shown in Fig. 17.
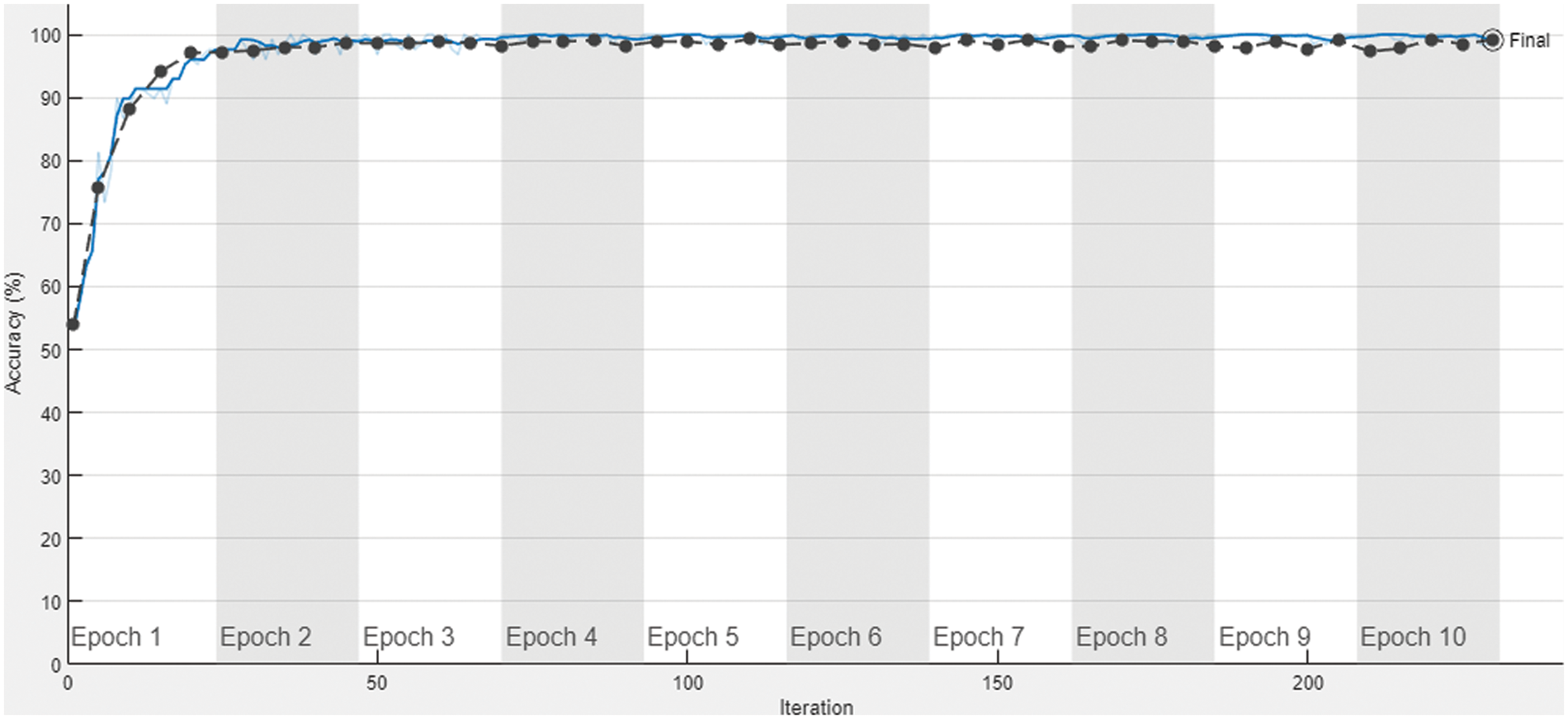
Figure 16: Accuracy of proposed IFDD system
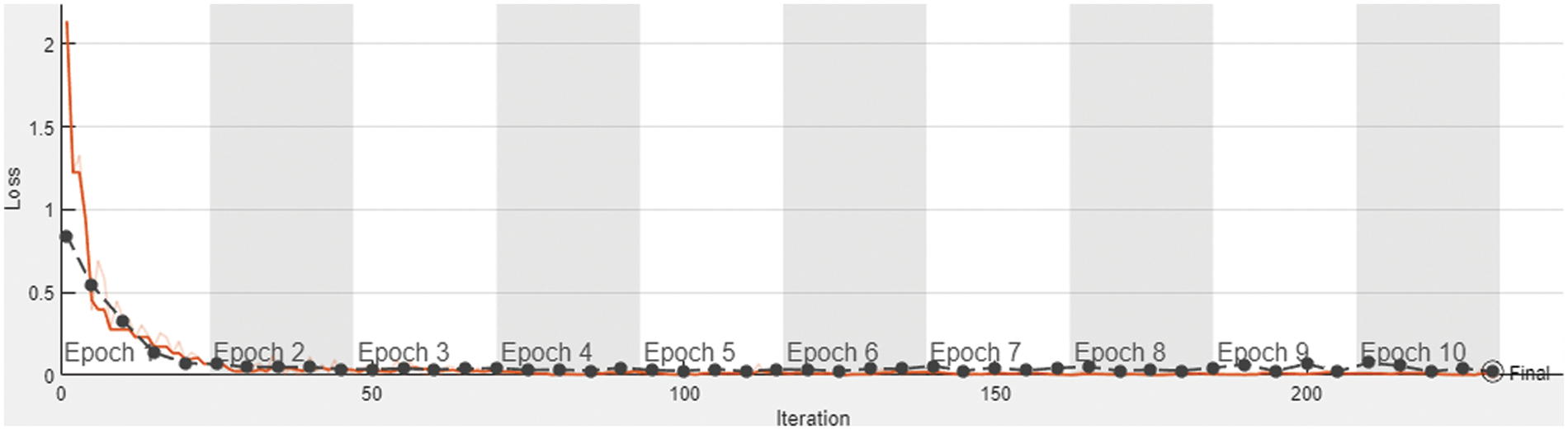
Figure 17: Loss of proposed IFDD system
In Figs.16 and 17 blue and black dotted marks lines demonstrate the training and validation the data respectively.
The validation results play a significant role in accepting or rejecting the trained IFDD model. For this purpose, performance metrics, Accuracy, false negative rate (FNR), true positive rate (TPR), true negative rate (TNR), positive predictive value (PPV), negative predictive value (NPV), false-positive rate (FPR), false omission rate (FOR), and F1-Score are used. Validation percentages of the proposed system are mentioned in Tab. 1.

A sample of 16 images is given for validation to the proposed IFDD system, as shown in Fig. 18. Tina Infection and Candidiasis disease are classified successfully by the proposed IFDD system.

Figure 18: Testing results of the trained IFDD system
Innovative fungal disease diagnosis has a significant impact on health and economic consequences. Millions of people suffer from various fungi diseases and uncomfortable human lifelike hair dryness, skin fungus, and allergic indications. The human body can be affected by such serious infections caused by some fungi or viruses. Given the high level of uncertainty in diagnosing fungal infections and analyzing treatment responses. Artificial intelligence could play a significant role in developing imaging-based machine learning solutions for numerous problems. In this research, several experiments using existing CNN architectures were applied to a fungal dataset with classes of Tina Infection and Candidiasis disease. The best result was obtained with an accuracy of 99.6% on the proposed CNN-Based system.
Acknowledgement: Thank you to our coworkers for their moral and technical assistance.
Funding Statement: The authors received no specific funding for this study.
Conflicts of Interest: The authors declare that they have no conflicts of interest to report regarding the present study.
References
1. L. Xie, W. Zhong, W. Shi and S. Sun, “Spectrum of fungal keratitis in North China,” Ophthalmology, vol. 113, no. 11, pp. 1943–1948, 2006. [Google Scholar]
2. M. Li and L. Zhang, “Research advance of fungal keratitis,” International Journal of Ophthalmology and Clinical Research, vol. 8, no. 2, pp. 384–387, 2008. [Google Scholar]
3. S. Belliappa, J. Hade, S. Kim, B. D. Ayres and D. S. Chu, “Surgical outcomes in cases of contact lens-related fusarium keratitis,” Eye Contact Lens, vol. 36, no. 4, pp. 190–194, 2010. [Google Scholar]
4. L. Xie, H. Zhai, J. Zhao, S. Sun and X. Dong, “Antifungal susceptibility for common pathogens of fungal keratitis in Shandong Province, China,” American Journal of Ophthalmology, vol. 146, no. 2, pp. 260–265, 2008. [Google Scholar]
5. M. A. Dahlgren, A. Lingappan and K. R. Wilhelmus, “The clinical diagnosis of microbial keratitis,” American Journal of Ophthalmology, vol. 143, no. 6, pp. 940–944, 2007. [Google Scholar]
6. P. Kryszkiewicz, A. Kliks and H. Bogucka, “Small-scale spectrum aggregation and sharing,” IEEE Journal Selected Areas Communication, vol. 34, no. 10, pp. 2630–2641, 2016. [Google Scholar]
7. Q. Qiu, Z. Liu, Y. Zhao, D. Wei and X. Wu, “Automatic detecting cornea fungi based on texture analysis,” in IEEE Int. Conf. on Smart Cloud, China, 2016. [Google Scholar]
8. F. Riaz, A. Hassan, S. Rehman and U. Qamar, “Texture classication using rotation and scale invariant gabor texture features,” IEEE Signal Process Letter, vol. 20, no. 6, pp. 607–610, 2013. [Google Scholar]
9. L. S. Davis, S. A. Johns and J. K. Aggarwal, “Texture analysis using generalized co-occurrence matrices,” IEEE Transactions on Pattern Analysis and Machine Intelligence, vol. 1, no. 3, pp. 251–259, 1979. [Google Scholar]
10. D. A. Clausi and H. Deng, “Design-based texture feature fusion using Gaborlters and co-occurrence probabilities,” IEEE Transactions on Image Processing, vol. 14, no. 7, pp. 925–936, 2005. [Google Scholar]
11. T. Ojala, K. Valkealahti, E. Oja and M. Pietikäinen, “Texture discrimination with multidimensional distributions of signed gray-level differences,” Pattern Recognition, vol. 34, no. 3, pp. 727–739, 2001. [Google Scholar]
12. Z. Li, S. Guo, L. Yu and V. Chang, “Evidence-efficient affinity propagation scheme for virtual machine placement in data center,” IEEE Access, vol. 8, pp. 158356–158368, 2020. [Google Scholar]
13. N. Naz, S. Abbas, M. Adnan and M. Farrukh, “Efficient load balancing in cloud computing using multi-layered mamdani fuzzy inference expert system,” International Journal of Advanced Computer Science and Applications (IJACSA), vol. 10, no. 3, pp. 569–577, 2019. [Google Scholar]
14. R. Rahim, “Comparative analysis of membership function on Mamdani fuzzy inference system for decision making,” Journal of Physics, vol. 930, no. 1, pp. 12029, 2017. [Google Scholar]
15. N. Iqbal, S. Abbas, M. A. Khan, T. Alyas, A. Fatima et al., “An RGB image cipher using chaotic systems, 15-puzzle problem and DNA computing,” IEEE Access, vol. 7, pp. 174051–174071, 2019. [Google Scholar]
16. T. Alyas, I. Javed, A. Namoun, A. Tufail, S. Alshmrany et al., “Live migration of virtual machines using a mamdani fuzzy inference system,” Computers, Materials & Continua, vol. 71, no. 2, pp. 3019–3033, 2022. [Google Scholar]
17. D. Zhang, J. Hu, F. Li, X. Ding, A. K. Sangaiah et al., “Small object detection via precise region-based fully convolutional networks,” Computers, Materials & Continua, vol. 69, no. 2, pp. 1503–1517, 2021. [Google Scholar]
18. J. Wang, Y. Wu, S. He, P. K. Sharma, X. Yu et al., “Lightweight single image super-resolution convolution neural network in portable device,” KSII Transactions on Internet and Information Systems (TIIS), vol. 15, no. 11, pp. 4065–4083, 2021. [Google Scholar]
19. J. Wang, Y. Zou, P. Lei, R. S. Sherratt and L. Wang, “Research on recurrent neural network based crack opening prediction of concrete dam,” Journal of Internet Technology, vol. 21, no. 4, pp. 1161–1169, 2020. [Google Scholar]
20. S. He, Z. Li, Y. Tang, Z. Liao, F. Li et al., “Parameters compressing in deep learning,” Computers, Materials & Continua, vol. 62, no. 1, pp. 321–336, 2020. [Google Scholar]
21. W. Sun, G. C. Zhang, X. R. Zhang, X. Zhang and N. N. Ge, “Fine-grained vehicle type classification using lightweight convolutional neural network with feature optimization and joint learning strategy,” Multimedia Tools and Applications, vol. 80, no. 20, pp. 30803–30816, 2021. [Google Scholar]
22. B. Zafar, S. A. Z. Naqvi, M. Ahsan, A. Ditta, U. Baneen et al., “Enhancing collaborative and geometric multi-kernel learning using deep neural network,” Computers, Materials & Continua, vol. 72, no. 3, pp. 5099–5116, 2022. [Google Scholar]
 | This work is licensed under a Creative Commons Attribution 4.0 International License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. |