DOI:10.32604/csse.2023.024605
| Computer Systems Science & Engineering DOI:10.32604/csse.2023.024605 | |
| Article |
Neural Cryptography with Fog Computing Network for Health Monitoring Using IoMT
1Department of Computer Science and Engineering, Coimbatore Institute of Engineering and Technology, Coimbatore, 641109, India
2Department of Applied Cybernetics, Faculty of Science, University of Hradec Králové, 50003, Hradec Králové, Czech Republic
3Department of Information Technology, College of Computers and Information Technology, Taif University, P.O. Box 11099, Taif, 21944, Saudi Arabia
4Department of Computer Science, College of Computers and Information Technology, Taif University, P. O. Box 11099, Taif, 21944, Saudi Arabia
5Department of Mathematics, Faculty of Science, Mansoura University, Mansoura, 35516, Egypt
6Department of Computational Mathematics, Science, and Engineering (CMSE), Michigan State University, East Lansing, MI, 48824, USA
*Corresponding Author: Mohamed Abouhawwash. Email: abouhaww@msu.edu
Received: 24 October 2021; Accepted: 24 January 2022
Abstract: Sleep apnea syndrome (SAS) is a breathing disorder while a person is asleep. The traditional method for examining SAS is Polysomnography (PSG). The standard procedure of PSG requires complete overnight observation in a laboratory. PSG typically provides accurate results, but it is expensive and time consuming. However, for people with Sleep apnea (SA), available beds and laboratories are limited. Resultantly, it may produce inaccurate diagnosis. Thus, this paper proposes the Internet of Medical Things (IoMT) framework with a machine learning concept of fully connected neural network (FCNN) with k-nearest neighbor (k-NN) classifier. This paper describes smart monitoring of a patient’s sleeping habit and diagnosis of SA using FCNN-KNN+ average square error (ASE). For diagnosing SA, the Oxygen saturation (SpO2) sensor device is popularly used for monitoring the heart rate and blood oxygen level. This diagnosis information is securely stored in the IoMT fog computing network. Doctors can carefully monitor the SA patient remotely on the basis of sensor values, which are efficiently stored in the fog computing network. The proposed technique takes less than 0.2 s with an accuracy of 95%, which is higher than existing models.
Keywords: Sleep apnea; polysomnography; IOMT; fog node; security; neural network; KNN; signature encryption; sensor
The Internet of Medical Things (IoMT) is the amalgamation of medical applications using sensor devices to connect with health-related information. In this scenario, user health data are sensed by the IoMT and transferred to the chief physician through a modern communication system. Even without the physical presence of the patient, the doctor can naturally view his or her health condition to prescribe medication. Thus, transferring and storing the sensitive data must be secured.
Sleep is one of the fundamental daily needs and is significant for brain function. Any sleep disorder can naturally affect general health and cause serious health problems, such as brain stroke, high blood pressure, complicate daily activities, and risk safety. Experts use Polysomnography (PSG) to study sleep disorders. PSG is a collection of signals recorded from various sensors counting the Electroencephalogram (EEG), Electro oculography (EOG), Electromyogram (EMG), Electrocardiogram (ECG), airflow, thoracic and abdominal movements, and oximetry. Rechtschaffen and Kales standardized the sleep stage classification rules depending on EEG modifications and split Non-Rapid Eye Movement (NREM) in sleep is a natural relief of humans and prevents several diseases. Sleep apnea is a sleep disorder in which breathing problem occurs during sleep states. SA affects our health by decreasing the oxygen blood level, eventually leading to other diseases [1]. SA impacts our health, mentally and physically, causing diseases, such as stroke, cardio problems, and diabetes. Scientifically, based upon the international sleep expert’s key observation, roughly one billion people worldwide have obstructive sleep apnea (OSA) [2].
IoMT collects significant health-related data and helps early diagnosis of diseases using machine learning techniques. Persons health data is considered extremely sensitive and confidential to users. Thus, IoMT must ensure user privacy [3] through a federated learning technique. This learning method trains the device to stop sharing the data outside the device [4]. For SA diagnosis, PSG test is needed, which produces electrical energy signals from sensor devices attached to the human body. The process of sleep monitoring people with SA is highly expensive and beds remain limited. Sometimes, a full night or two nights are required for monitoring in a well-equipped sleep laboratory. PSG-recorded values sometimes misguide health professionals, leading to inaccurate diagnosis.
However, monitoring a person’s health condition continuously is extremely difficult. Nonetheless, IoMT makes this possible. Although data transfer is performed remotely, its security and privacy are not assured. Moreover, data are sensitive, and a need for authentication technology persists, given that various attacks can enter the IoMT environment through the internet. Some attackers easily acquire control over the medical device remotely. Malware in IoMT greatly affects its communication and control on the medical device. Moreover, traditional techniques are insufficient to highly secure IoMT communication. Recent attacks by Mirai botnets create distributed denial of service due to insecurity in the Internet of Things (IoT) environment. Hence, a strong security technique to detect attacks in the sensitive IoMT environment is warranted [5–7].
This research contributes security features as follows:
1. Sleep apnea is monitored using health sensors, such as an oximeter, and stress is monitored on the basis of the heart rate. Data are collected and transmitted to fog nodes using the IoMT framework.
2. IoMT uses forward neural network to train the features and uses KNN to classify SA accurately. The classified data is stored in fog nodes using a signature encryption technique.
The rest of the article is structured as follows. Section 2 presents the survey on IoMT. Section 3 demonstrates the proposed architecture and apnea detection using IoMT. Section 4 discusses the result evaluation. Section 5 concludes.
The information or data is connected and communicated through the internet using the IoT. Smart devices of homes, cars, watches, and so on are connected to the internet to transfer real-time data from user to end user. Moreover, IoT produces Wireless Sensor Networks (WSN), smart technologies, cloud network, and so on [8]. Human to machine communication [9] is abruptly transferred to machine-machine communication. Recently the IoT became promising in smart applications, such as the health industry, smart city, and so on. Thus, this survey focused on intelligent monitoring of SA diagnosis continuously. The Internet of Intelligent Things (IoIT) [10–12] blends the artificial intelligence in the healthcare system to analyze the data logically.
The main disadvantages of using the IoT is limited bandwidth processing, less memory, and small structure, which cause security attacks and privacy threats [13–16]. These factors influence high research interest in IoT security. To address IoT security, various cryptographic frameworks and technology are suggested [17–22]. Especially in the medical system, handling patient data is highly sensitive for the IoT [23,24]. Central cloud server requires high security structure for providing data authentication.
Some studies explored the adaptive architecture for IoMT architecture [25]. This work provides high security for health dataset using public and private key structures. However, the security of the system is not highly adaptive. Thus, this work explores whether the hybrid security system using a cyber security algorithm for the IoMT is implemented [26]. Streaming data is transmitted via nodes using high authentication [27] to secure the IoMT real-time data in networks. Previous research discussed the security of IoMT with different techniques [28].
This study discussed several SA surveys. The novel recurrent neural architecture is used to extract the apnea features from input dataset [29]. Machine learning classifiers, such as the support vector machine (SVM) [30], threshold-based detectors [31], and regression trees with Adaboost are used to classify SA from the input feature set. The health-based smart contracts [32,33] are used for IoMT to transfer health data [34–38].
Although SA syndrome is a common disease, patient diagnosis is difficult. Thus, smart monitoring of the sleeping habit of patients is presented. It monitors the variations in stress and observes the patient’s heart rate and the blood oxygen level while asleep. The architecture of SA syndrome analysis is presented in Fig. 1. The sensor transmits the values to the data analysis section. Here, SA is analyzed on the basis of the input SpO2 value. The forward neural network and KNN classifier is used to detect SA in patients.
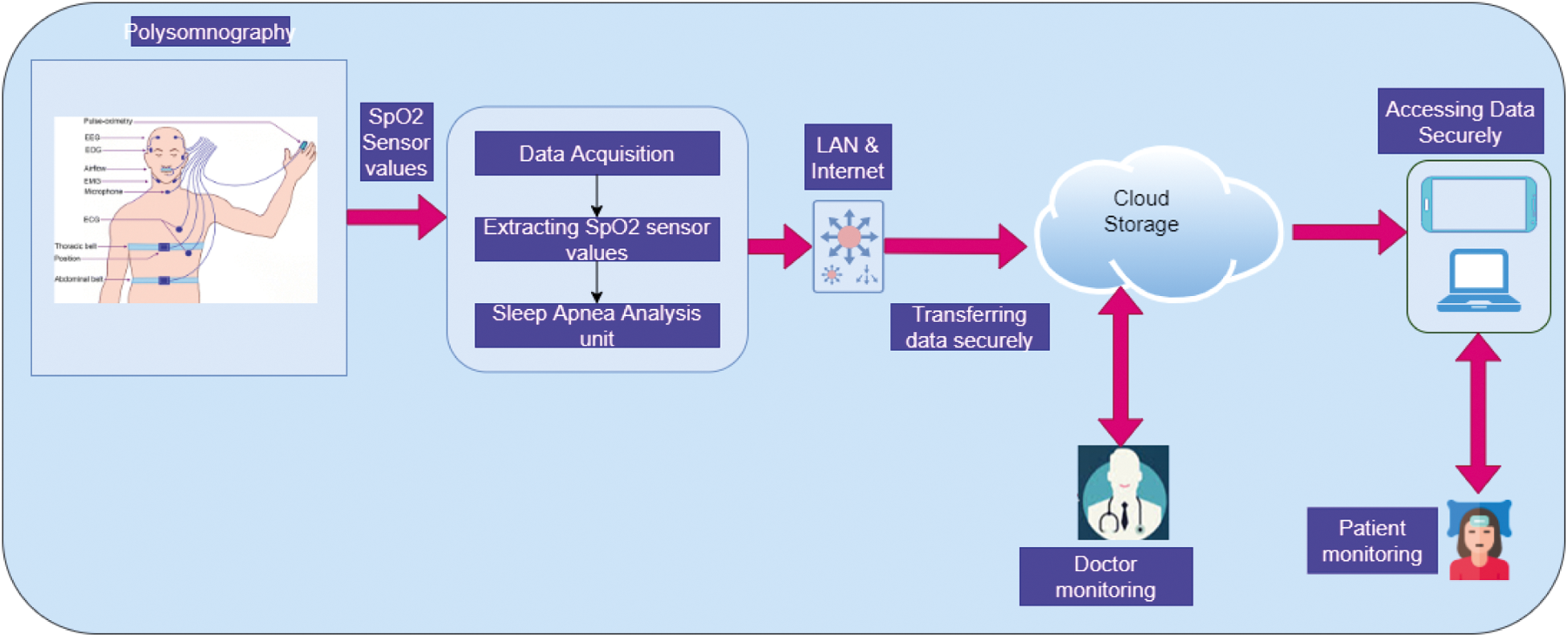
Figure 1: Sleep apnea syndrome analysis
3.1 Visualizing of Sleep Disorder
During sleep state, the nervous system becomes inactive, and the relaxation of muscles forces the eyes to close. It is also associated with low movement, stress less posture, and consciousness becomes suspended involuntarily. To monitor the sleep disorder, patients must undergo five stages, which include rapid eye movement (REM) and non rapid eye movement (NREM). Fig. 2 shows the detailed sleeping stages categorically.
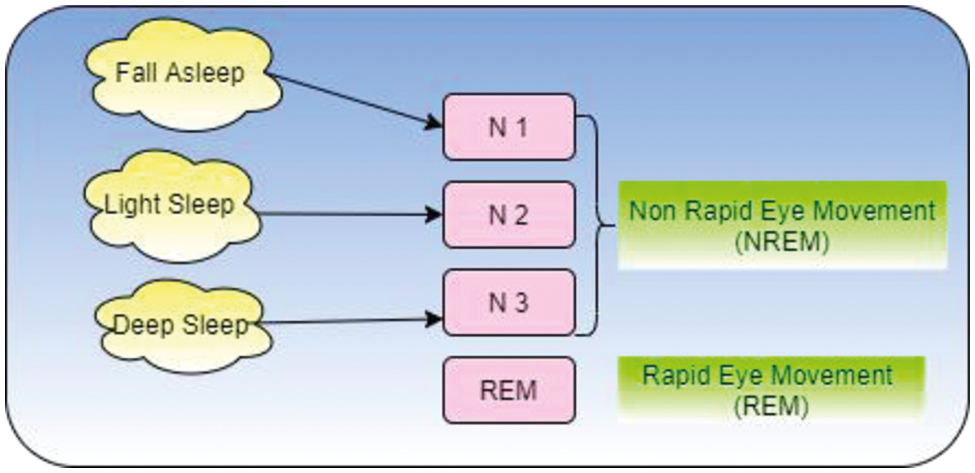
Figure 2: Categorized sleep stages
Human beings have five stages of sleep. Stages 1 and 2 are considered light sleep in which people can be easily awakened. Stage 3 is the deep sleep, Stage 4 represents very deep sleep, and Stage 5 is the REM. Each stage requires 5–15 minutes to complete. After completion of five stages, it starts again from Stage 1. On average, 90 to 110 minutes are needed to complete a sleep cycle. Any irregularity that occurs within the five sleep stages is a sleep disorder. Thus, to maintain a good sound sleep, sufficient sleep in each stage and sleep cycle must be obtained. Fig. 2 presents the sleep stages.
During the sleep state, some breathing-related disorder occurred is called SA. As shown in Fig. 3 for monitoring SA, SpO2 and heart rate variability(HRV) sensor devices are attached in various organs in the body. Electrical energy emitted by the body is collected from these sensors and transmitted as graphical representation and stored in the fog computing network. This procedure is the Polysomnogram diagnosis.
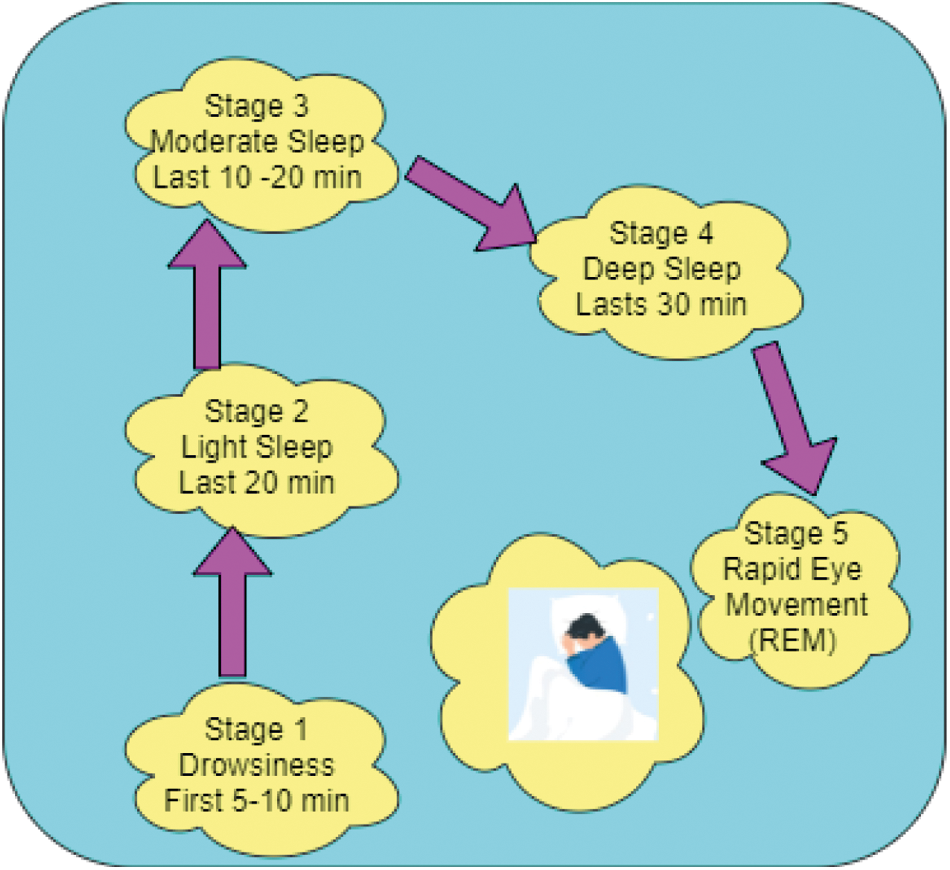
Figure 3: Sleep stages
3.3 Proposed - IoMT-Fog Computing
IoMT sensor values, such as the heart rate, and oximetric values are collected and stored in the fog computing-based network. Fig. 4 shows the IoMT with the fog computing process. Fig. 4 contains two layers, namely, the IoMT section and the fog computing layer. In the IoMT layer, data are collected from sensor devices and are classified into sensitive data (confidential data) and non-sensitive data (non-confidential data). This classified data is transferred to the fog layer, which contains fog servers. Then, data encryption and authorization are performed by a hashing technique of Advanced Signature-Based Encryption (ASE) of Diffie-Hellman key exchange and digital signature. This algorithm is used to exchange information between IoMT devices securely.
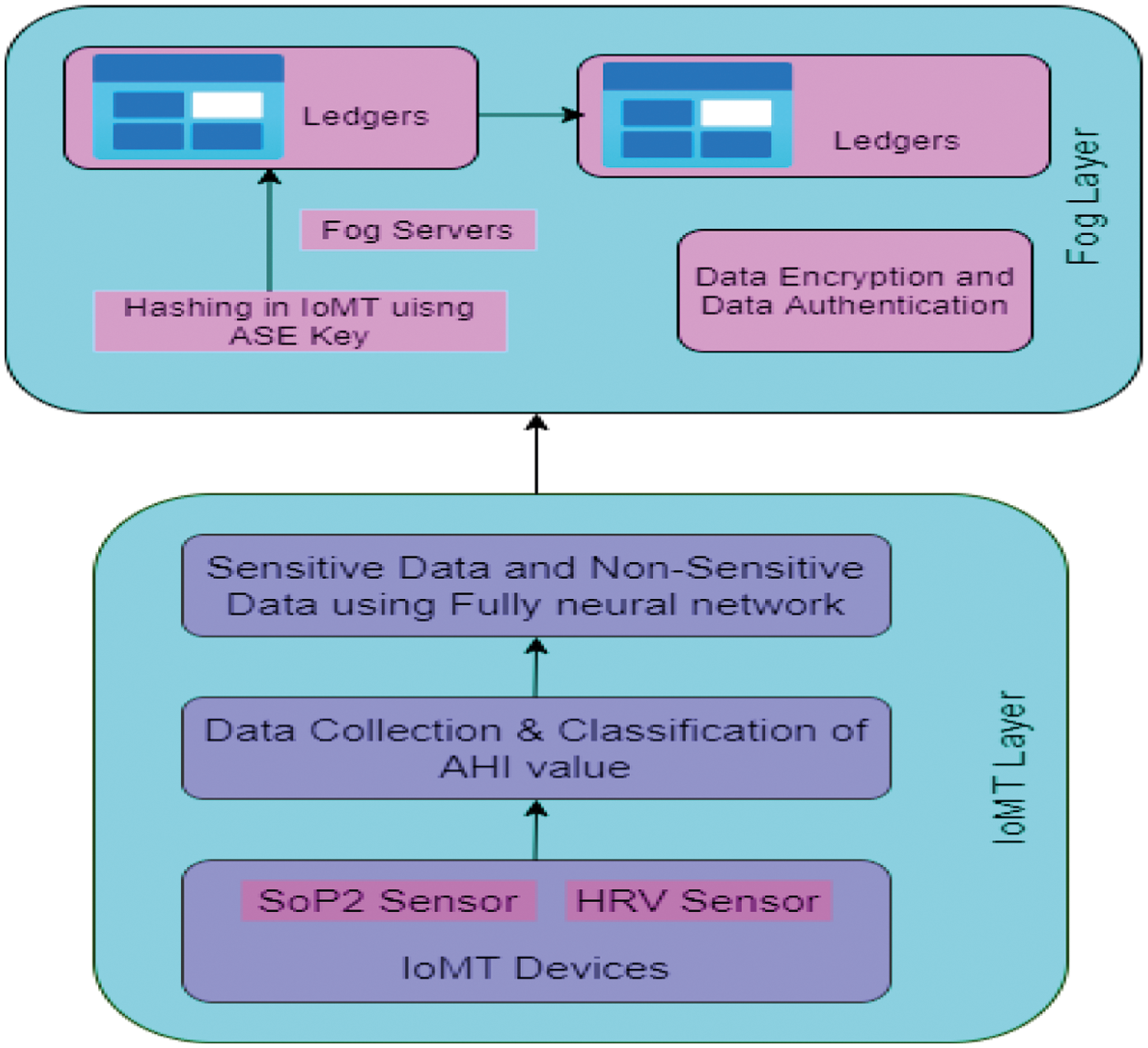
Figure 4: IoMT with fog computing
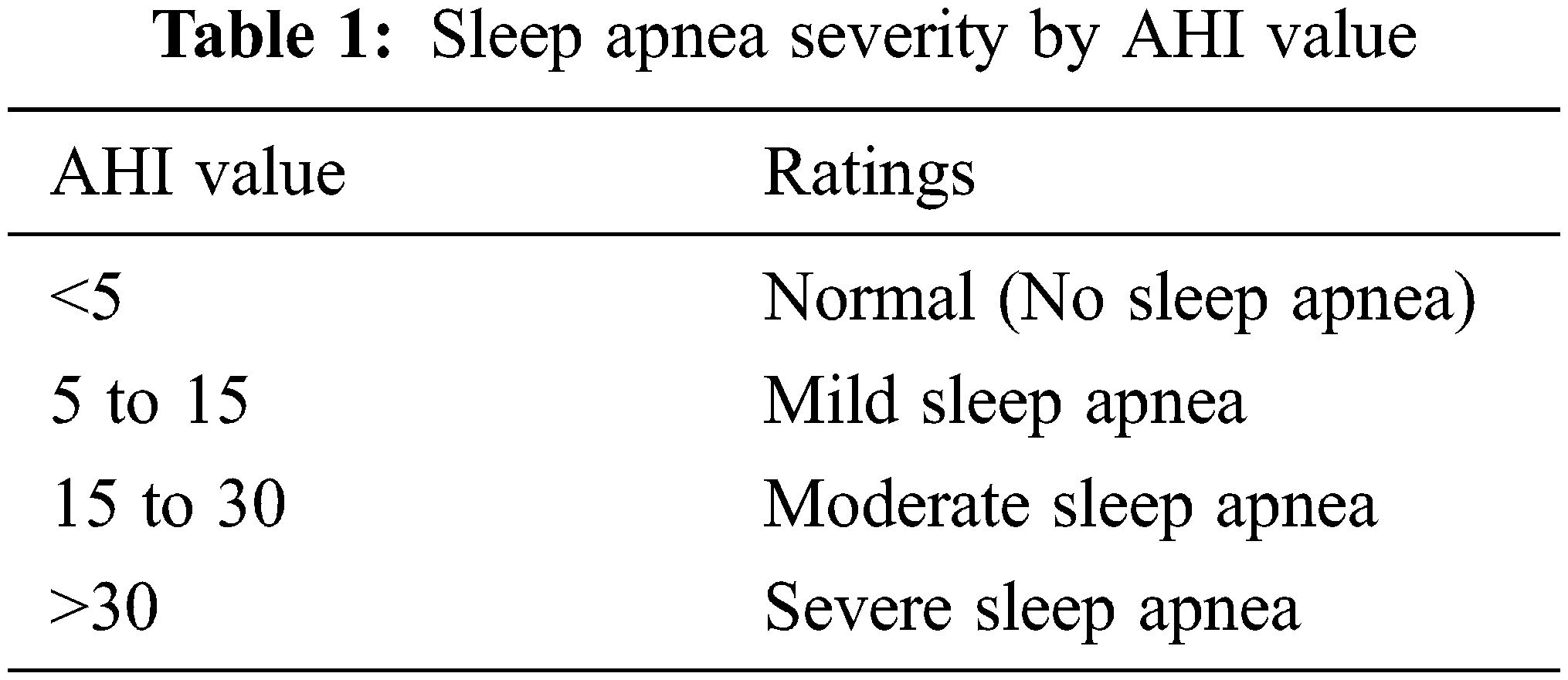
The IoMT layer contains wearable sensor devices of SpO2, which extract the electrical energy signal of SpO2 and HRV. This combination of SpO2 levels and HRV is used to reduce the false detective cases and increases accuracy. This work implementation is focused on monitoring heart rate and oxygen blood level when SA transpires in the sleep state of a patient. When SA happens to the patient, the system will alarm the doctor and observe the readings stored in the fog node securely. The Apnea-Hypopnea Index (AHI) is used to measure SA severity. Tab. 1 displays the AHI value.
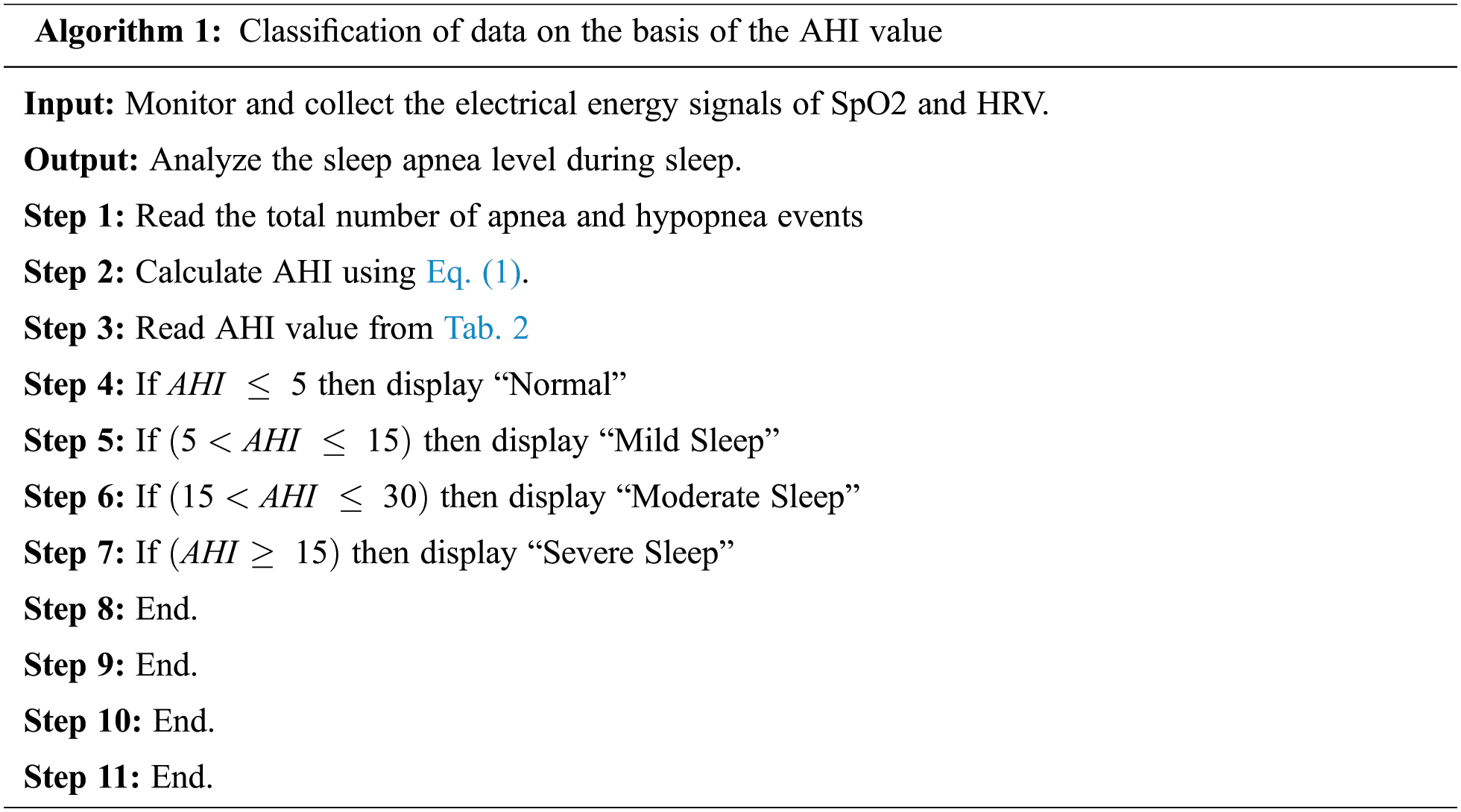
Algorithm 1 represents the patient’s SA severity.
In the IoMT layer, data are collected and classified on the basis of the AHI value. The data are classified as sensitive information and non-sensitive information using FCNN and k-nearest neighbour (k-NN) classifier. Fig. 5 shows the FCNN diagram for SA classification.
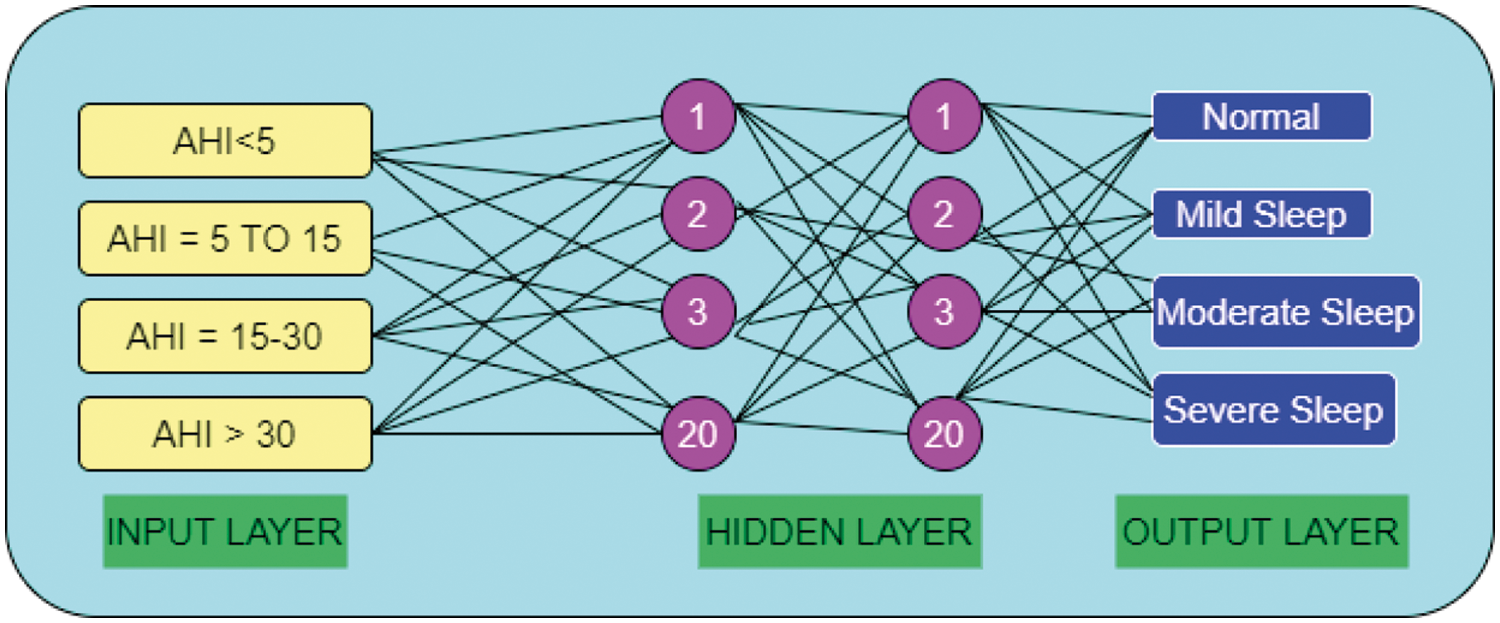
Figure 5: FCNN of SA
This FCNN has one input layer, two hidden layers, and one output layer with 20 neurons. This model is used to develop a relationship between AHI value and sleep stages. To obtain accurate classification after applying FCNN, KNN is implemented. In the KNN classification, the input value is the k-nearest neighbor, and the output value assigns the feature vector class membership. In the classification of KNN, Euclidean distance metric measures are used,
In Eq. (2), classification is done by the majority votes of neighbourhood values that are grouped together. Here the value of k should be assigned only an odd number. That is, 1-NN, 3-NN, 5NN, and so on.
In the fog layer, the classification of data is stored for promoting accuracy, security, and scalability. Fog servers are used to generate data encryption and decryption using Diffie-Hellman encryption in the fog node. Algorithms 2 and 3 are used to encrypt and decrypt the information.
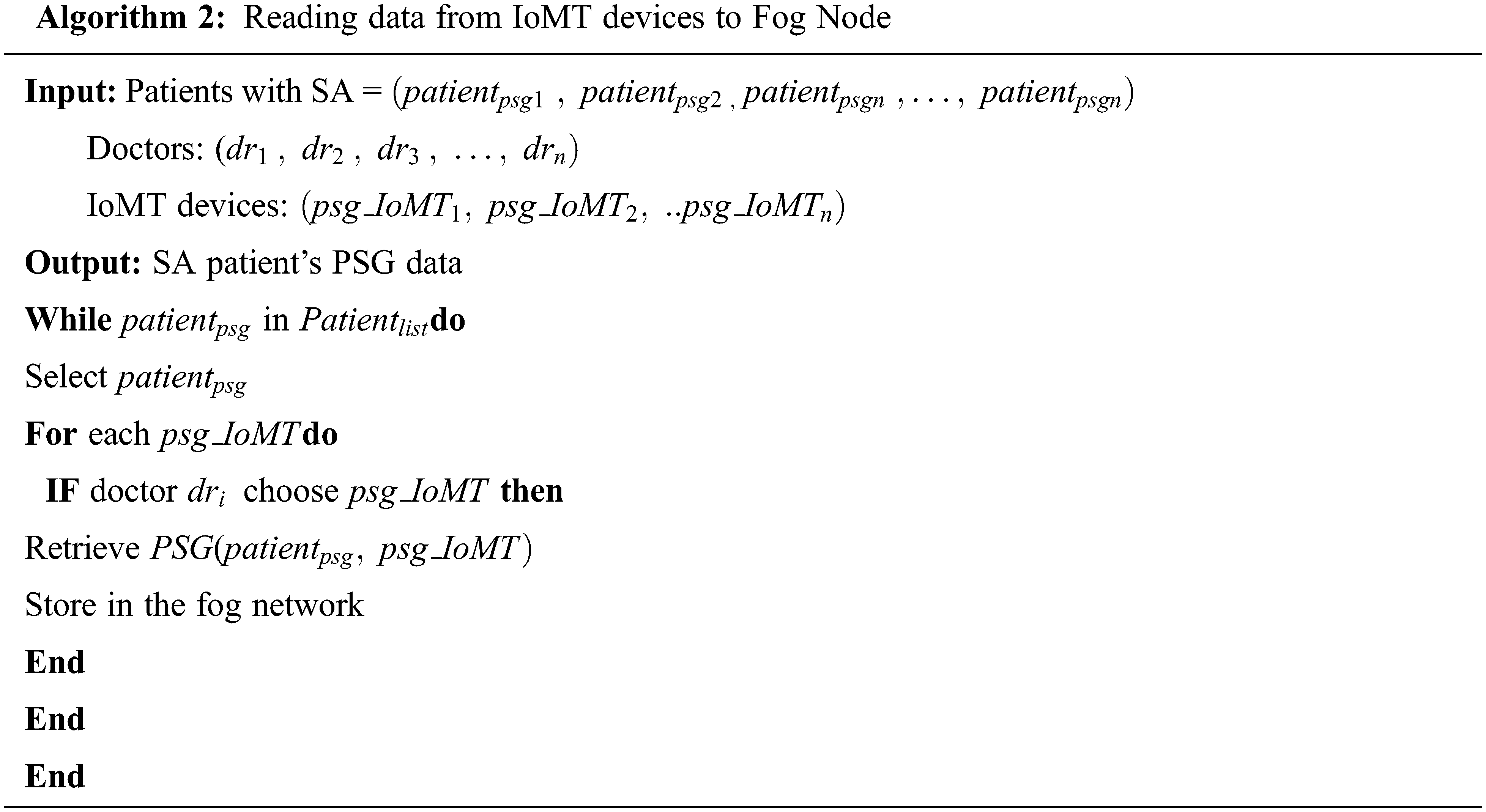
Algorithm 1 retrieves data from IoMT devices and transfers to fog nodes. In the fog node data from sensor devices of SoP2, HRV are stored securely. Algorithm 2 describes the data encryption and decryption using the Diffie-Hellman encryption during fog computation. ASE algorithm comprises asymmetric cryptographic operations, such as the Diffie-Hellman key exchange and digital signature.
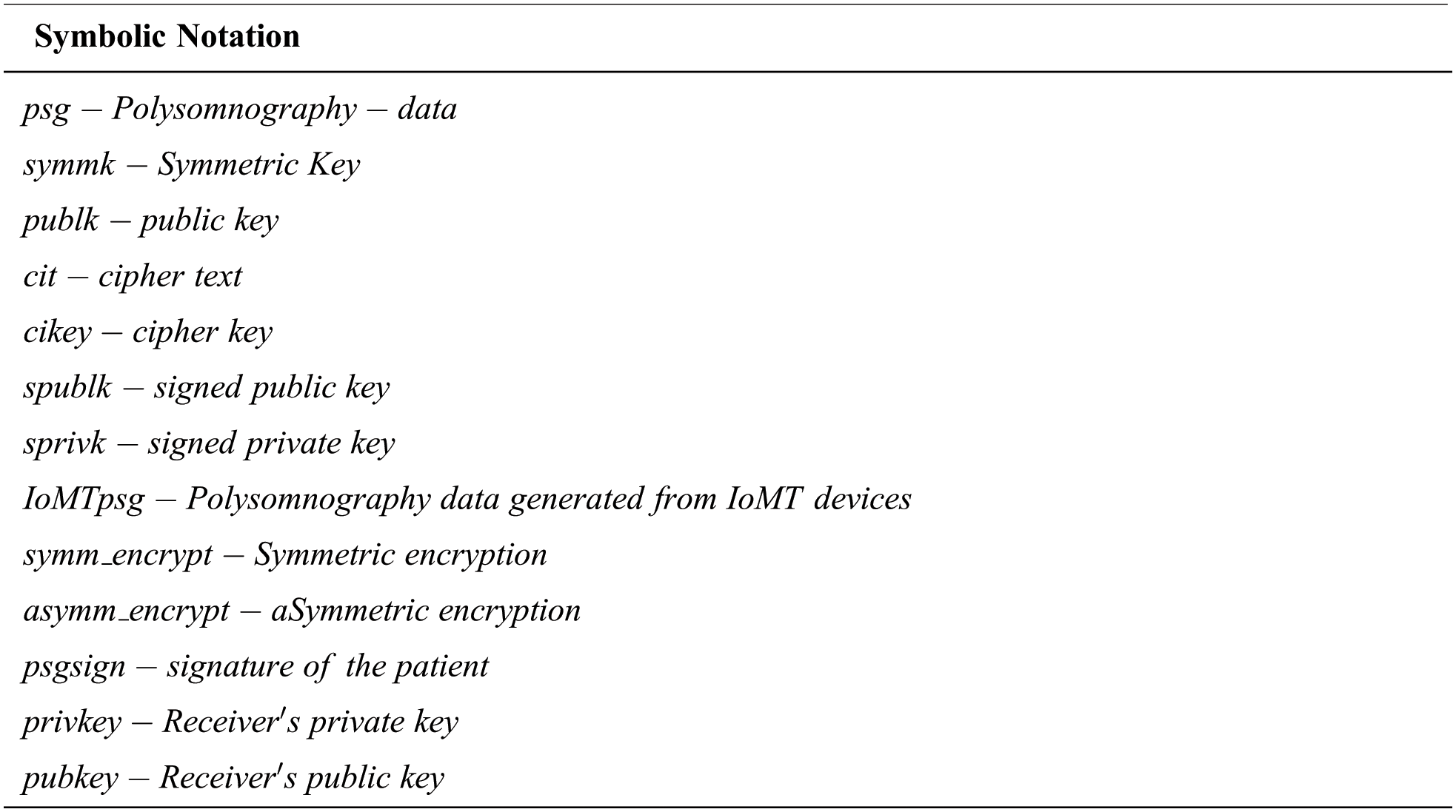
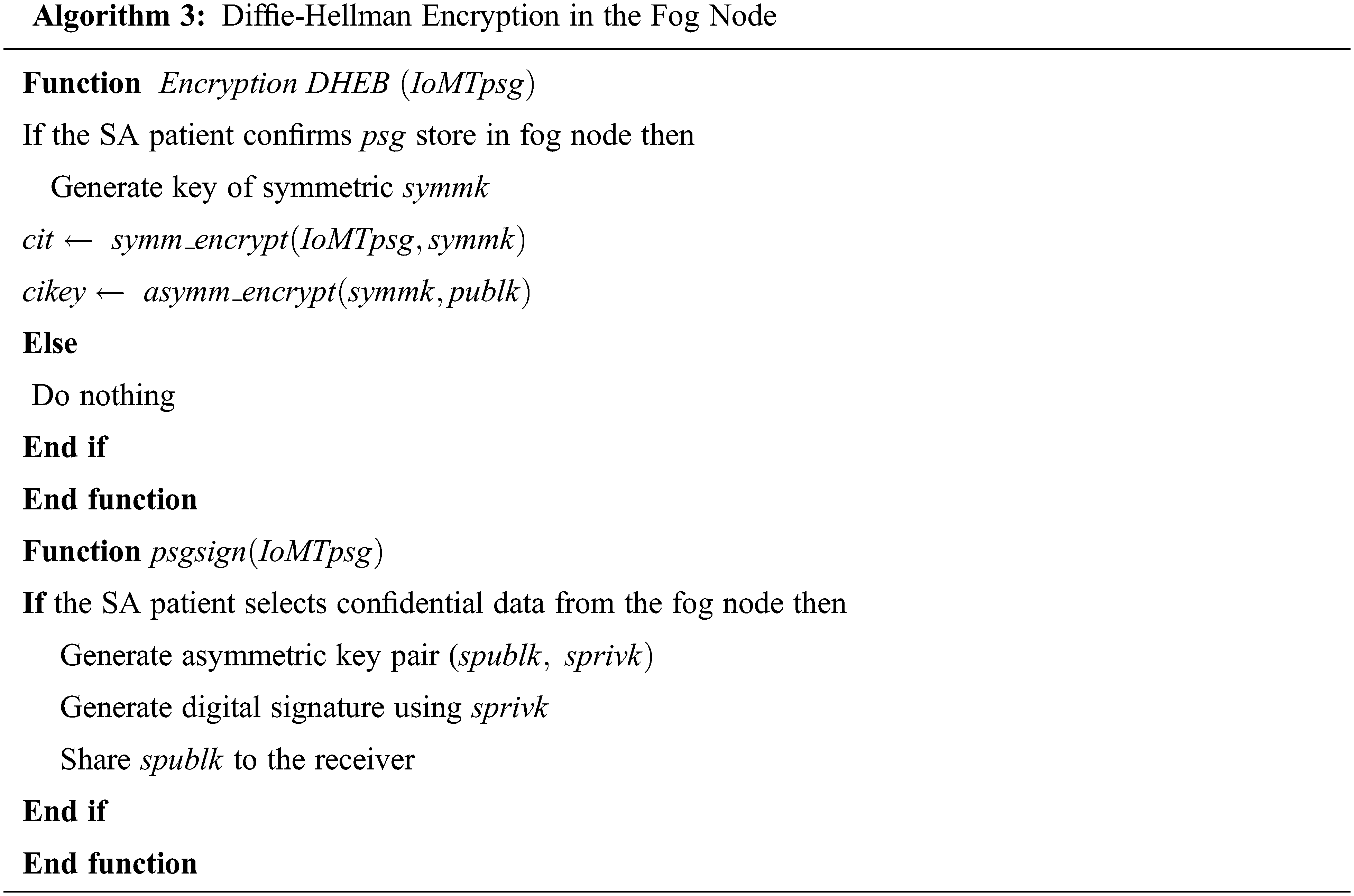
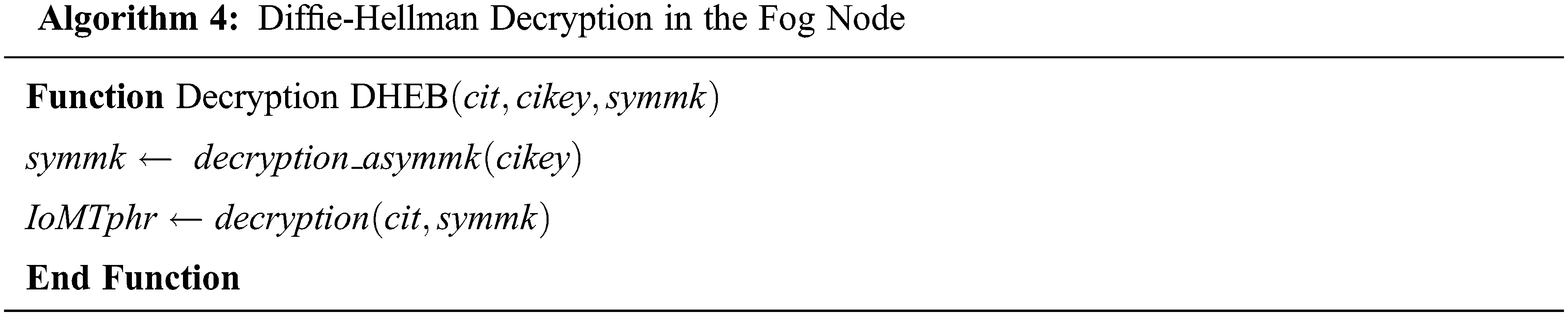
Algorithms 3 and 4 typically perform the encryption and decryption of the SA patient’s data by using the digital signature of hash, and private key produces the Diffie-Hellman method for the exchange of the key among various mobile IoMT devices and fog nodes.
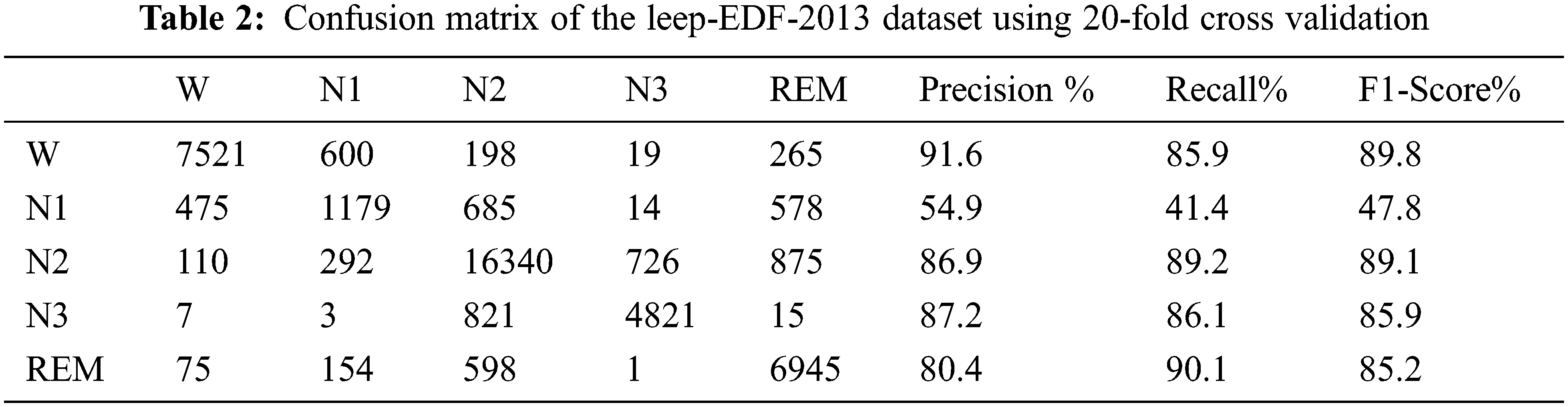
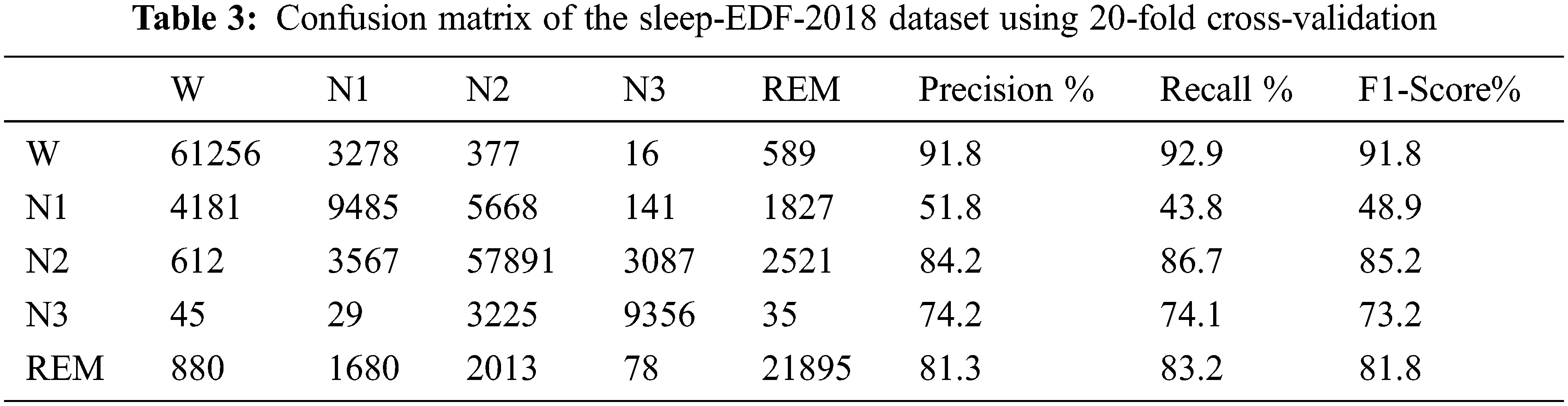
Independent analysis of SA is a breathing disorder that occurs during a person’s sleep state. In this work, FCNN-KNN+ASE uses two public datasets of Sleep-EDF-2013 and Sleep-EDF-2018. For evaluation, a 20-fold cross validation was applied to all 250 PSG data values of the dataset. The sleeping stages of R & K standard of W, N1, N2, N3, N4, and REM are used to evaluate FCNN-KNN+ASE. The parametric measures are given below.
where TP-True Positive, TN-True Negative, FP-False Positive, FN-False Negative, and
Tab. 4 shows the comparison of our proposed work with other machine learning algorithms in the parametric metric measures of kappa and MF1 score values using two different datasets of Sleep-EDF-2013 and Sleep-EDF-2018.
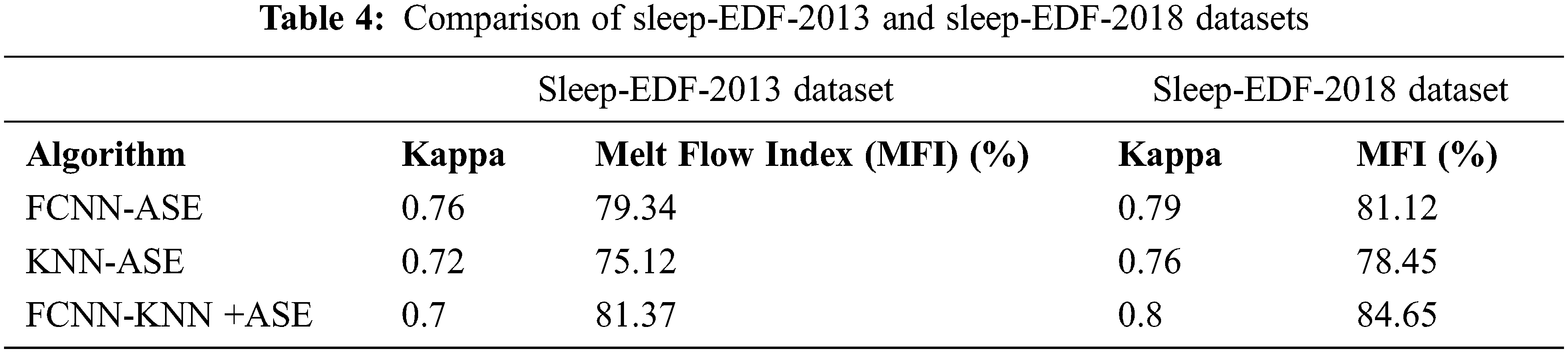
Tab. 5 unveils that the evaluation of FCNN-KNN+ASE was compared with FCNN-ASE and KNN-ASE. Our proposed work obtained better value in kappa of 0.7 in the Sleep-EDF-2013 dataset and obtained a kappa value of 0.8 in the Sleep-EDF-2018 dataset. Similarly, for the MF1 score value of the Sleep-EDF-2013 dataset obtained 81.37% and the Sleep-EDF-2018 dataset obtained 84.65% in our proposed work, FCNN-KNN+ASE. Tabs. 6 and 7 show the calculating error rate of the Sleep-EDF-2013 and Sleep-EDF-2018 datasets.
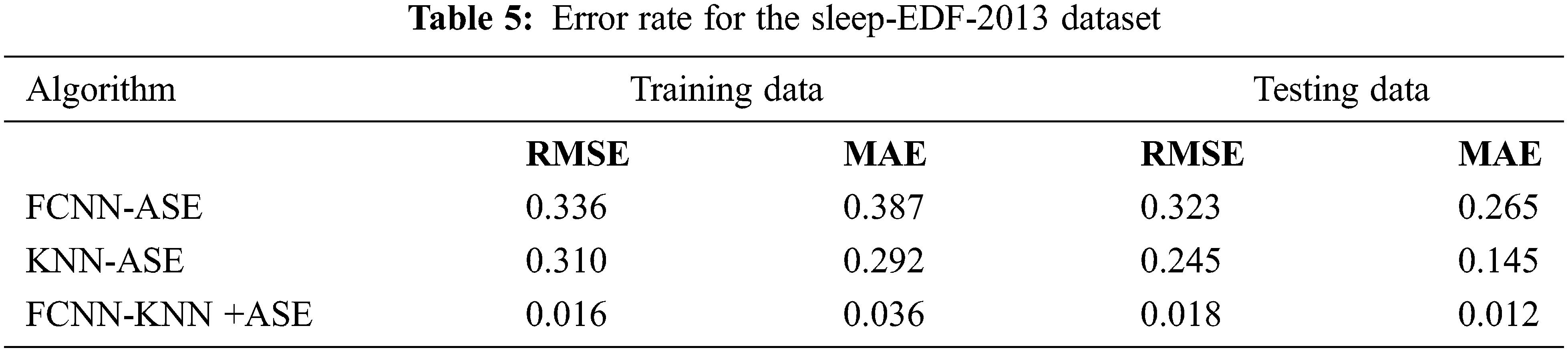
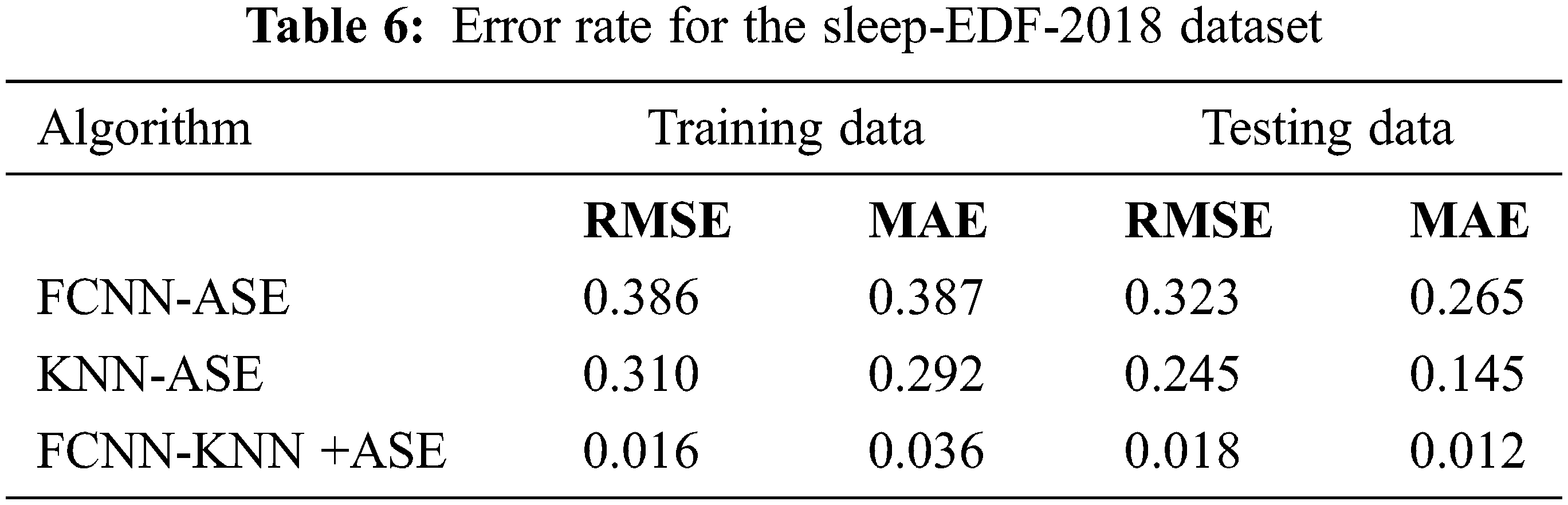
Tabs. 6 and 7 present tthat the error rate for our proposed work produces minimum error rate using two different datasets. Tabs. 8 and 9 unveil that cost of communication and storage cost in bits of different algorithm with two different datasets are given.

Tab. 8 demonstrates that our proposed technique obtains minimum communication cost and storage cost compared with other techniques.

Tab. 9 presents that our proposed technique obtains minimum communication cost and storage cost compared with other techniques. Tabs. 9 and 10 reveal that time analysis for encryption of PSG information with various file sizes and stored it in fog-node.
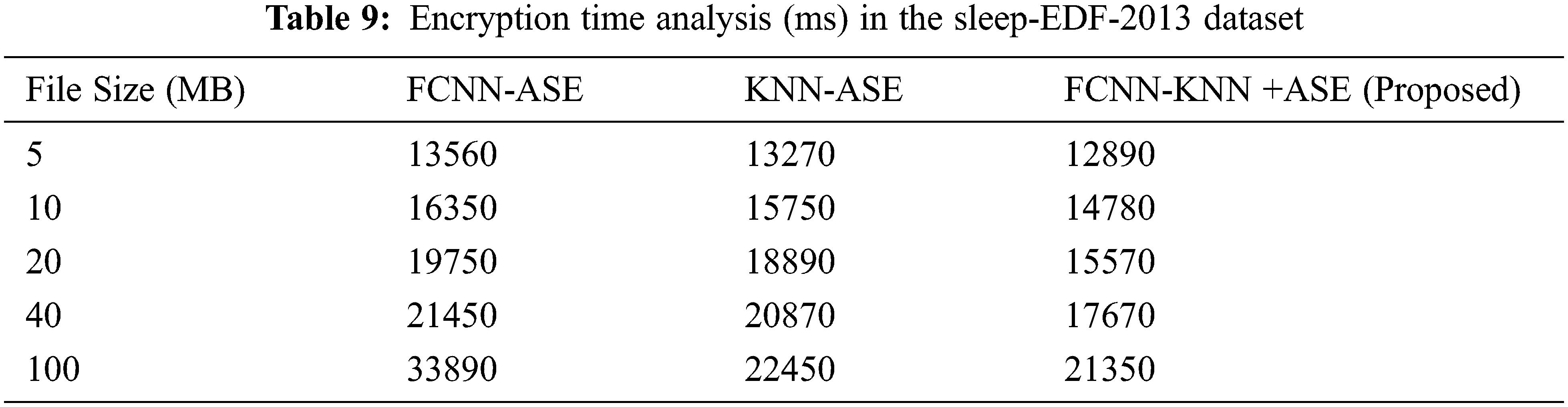
Tab. 10 shows that our proposed work obtained minimum time analysis for encryption using the Sleep-EDF-2013 dataset and the PSG information, which are collected from SoP2 and HRV sensor devices for diagnosis of SAS.
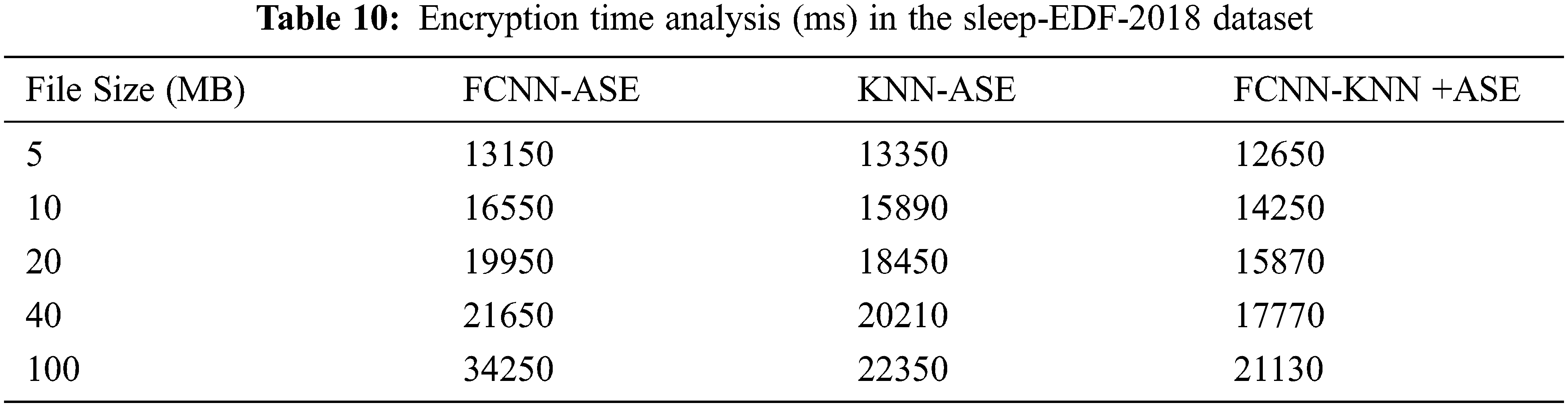
Tab. 10 demonstrates that our proposed work obtained minimum time analysis for encryption using the Sleep-EDF-2018 dataset and the PSG information, which are collected from SoP2 and HRV sensor devices for SAS diagnosis.
Our proposed work obtained minimum time analysis for decryption using the Sleep-EDF-2018 dataset and the PSG information, which are collected from SoP2 and HRV sensor devices for SAS diagnosis. Fig. 6 shows the average accuracy rate for FCNN-KNN+ASE in the two datasets.
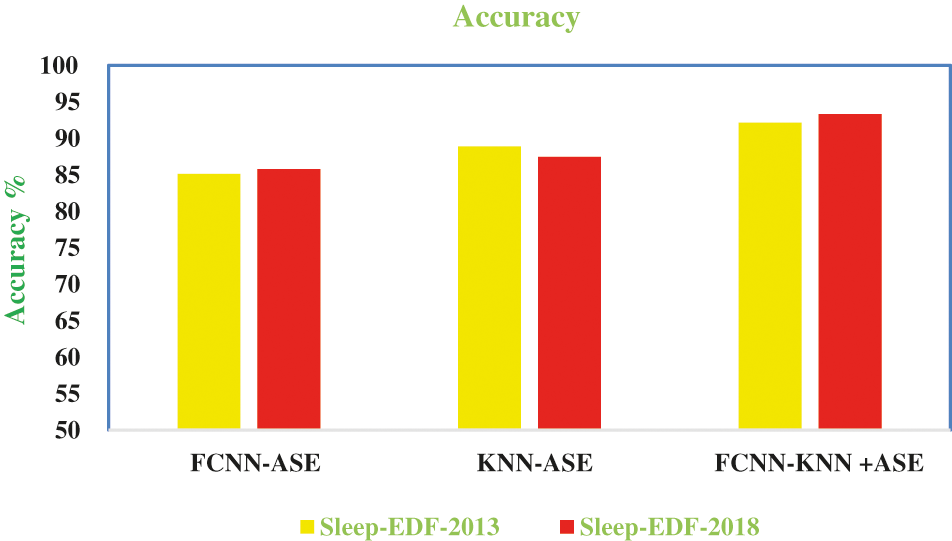
Figure 6: Accuracy
Fig. 6 presents that our proposed work gives high accuracy rate compared with other algorithms. Fig. 7 shows the computation time of our proposed work.
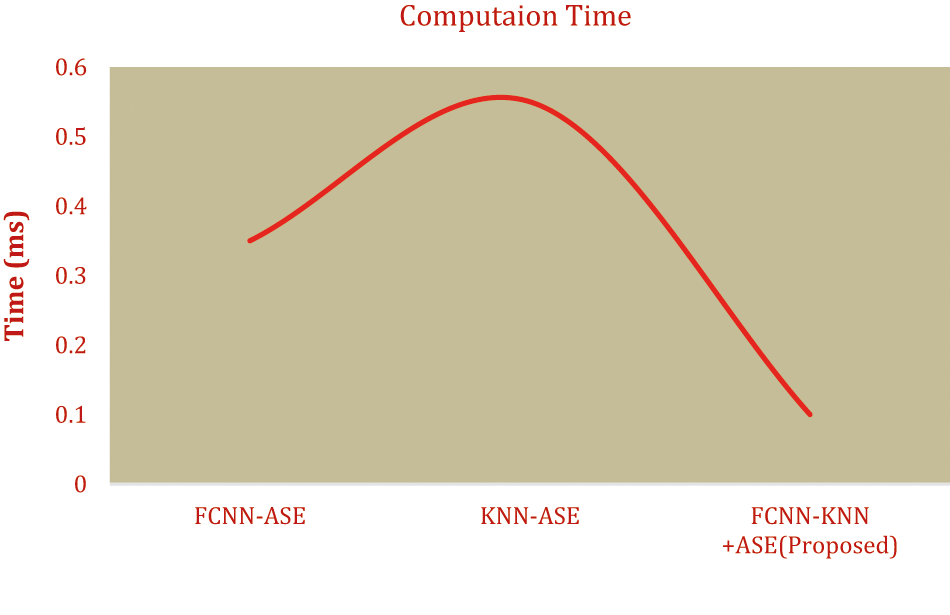
Figure 7: Computation time
The figure shows that the computation of our proposed work obtained minimum time. It produces minimum execution time and minimum error rate.
This work provides reference for SA diagnosis using a fog computing-based IoMT in machine learning algorithms. It uses electrical energy signals that are carefully collected from SpO2 and HRV sensor devices and collected data stored in fog computing network. Thereafter, we implement a complex ASE algorithm for encryption and decryption for PSG values, which cannot be accessed by unauthorized users. This work uses two different public datasets of Sleep-EDF-2013and Sleep-EDF-2018. The advantages of the proposed work, FCNN-KNN +ASE, are better security, faster access, minimal time execution, higher accuracy, more flexible, and more reliable compared with other existing algorithms. The overall accuracy performance of this work obtained 92.13% in the Sleep-EDF-2013 dataset and 93.32% in the Sleep-EDF-2018 dataset. Finally, our proposed work analysis provides effective monitoring for diagnosing people with the SA based on PSG values. Future work is upgraded by using various machine learning algorithms with edge computing. Energy efficiency must be calculated in future work to widely enhance fog computing the IoMT.
Acknowledgement: We would like to give special thanks to Taif University Research supporting Project Number (TURSP-2020/98), Taif University, Taif, Saudi Arabia.
Funding Statement: Taif University Researchers Supporting Project Number (TURSP-2020/98), Taif University, Taif, Saudi Arabia.
Conflicts of Interest: The authors declare that they have no conflicts of interest to report regarding the present study.
1. R. W. Mcarley, “Neurobiology of REM and NREM sleep,” Sleep Medicine, vol. 8, no. 4, pp. 302–330, 2017. [Google Scholar]
2. S. Chokroverty, “Overview of sleep & sleep disorders,” Indian Journal of Medical Research, vol. 131, no. 2, pp. 126–140, 2010. [Google Scholar]
3. C. Della Monica, S. Johnsen, G. Atzori, J. A. Groeger and J. Dijk, “Rapid eye movement sleep, sleep continuity and slow wave sleep as predictors of cognition, mood and subjective sleep quality in healthy men and women, aged 20-84 years,” Frontiers in Psychiatry, vol. 9, no. 255, pp. 23–34, 2018. [Google Scholar]
4. C. A. Kushida, M. R. Littner, T. Morgenthaler, C. A. Alessi Bailey and J. Coleman, “Practice parameters for the indications for PSG, AASM practice parameters practice parameters for the indications for polysomnography and related procedures: An update for 2005,” Journal of Sleep Research, vol. 28, no. 4, pp. 24–36, 2005. [Google Scholar]
5. Z. Liu, L. Zhang, Q. Ni, J. Chen, J. Wang et al., “An integrated architecture for IoT malware analysis and detection,” in Proc. Int. Conf. on Internet of Things as a Service, Patna, India, pp. 127–137, 2018. [Google Scholar]
6. J. Su, D. V. Vasconcellos, S. Prasad, D. Sgandurra, Y. Feng et al., “Lightweight classification of IoT malware based on image recognition,” in Proc. IEEE 42Nd Annual Computer Software and Applications Conf. (COMPSAC), Tokyo, Japan, vol.2, pp. 664–669, 2018. [Google Scholar]
7. V. Clincy and H. Shahriar, “IoT malware analysis,” in Proc. 2018 IEEE 42Nd Annual Computer Software and Applications Conf. (COMPSAC), USA, vol. 1, pp. 920–921, 2019. [Google Scholar]
8. T. H. Tran and C. Pham, “The internet-of-things based hand gestures using wearable sensors for human machine interaction,” in Proc. 2019 Int. Conf. on Multimedia Analysis and Pattern Recognition (MAPR), Hwaseong, Korea, pp. 1–6, 2019. [Google Scholar]
9. S. Hu and T. Jiang, “Artificial intelligence technology challenges patent laws,” in Proc. 2019 Int. Conf. on Intelligent Transportation, Big Data & Smart City (ICITBS), India, pp. 241–244, 2019. [Google Scholar]
10. T. E. Weaver, M. W. Calik, S. S. Farabi, A. M. Fink, M. C. Kapella et al., “Innovative treatments for adults with obstructive sleep apnea,” Nature and Science of Sleep, vol. 6, no. 137, pp. 1–12, 2014. http://dx.doi.org/10.2147/NSS. [Google Scholar]
11. L. Cai, J. Jiang, X. Liu, M. Zhu, K. Cheng et al., “OSA patient monitoring system based on the internet of things framework,” in Proc. 4th Int. Conf. on Smart and Sustainable Technologies (SpliTech), India, pp. 1–4, 2019. [Google Scholar]
12. J. Lin, W. Yu, N. Zhang, X. Yang, H. Zhang et al., “A survey on internet of things: Architecture, enabling technologies, security and privacy, and applications,” IEEE Internet of Things Journal, vol. 4, no. 5, pp. 1125–1142, 2017. [Google Scholar]
13. I. Lee and K. Lee, “The Internet of Things (IoTApplications, investments, and challenges for enterprises,” Business Horizons, vol. 58, no. 4, pp. 431–440, 2015. [Google Scholar]
14. M. Khomh, F. Haoues, M. Quintero and S. Yacout, “Enforcing security in internet of things frameworks: A systematic literature review,” Internet of Things, vol. 6, no. 3, pp. 100050, 2019. [Google Scholar]
15. J. Ahamed and A. V. Rajan, “Internet of Things (IoTApplication systems and security vulnerabilities,” in Proc. 2016 5th Int. Conf. on Electronic Devices, Systems and Applications (ICEDSA), Ras Al Khaimah, United Arab Emirates, pp. 1–5, 2016. [Google Scholar]
16. C. Hosmer and M. Dermott, Defending IoT Infrastructures with the Raspberry Pi. Germany: Apress, Springer, 2018. [Google Scholar]
17. A. Tekeoglu and A. S. Tosun, “An experimental framework for investigating security and privacy of IoT devices,” in Proc. Int. Conf. on Intelligent, Secure, and Dependable Systems in Distributed and Cloud Environments, Vancouver, BC, Canada, pp. 63–83, 2017. [Google Scholar]
18. M. Frustaci, P. Pace, G. Aloi and G. Fortino, “Evaluating critical security issues of the IoT world: Present and future challenges,” IEEE Internet of Things Journal, vol. 5, no. 4, pp. 2483–2495, 2018. [Google Scholar]
19. O. Alrawi, C. Lever, M. Antonakakis and F. Monrose, “Sok: Security evaluation of home-based IOT deployments,” in Proc. Sym. on Security and Privacy (sp), San Francisco, CA, USA, pp. 1362–1380, 2019. [Google Scholar]
20. M. Chernyshev and H. Peter, “Security assessment of IoT devices: The case of two smart TVs,” in Proc. Conf.: 13th Australian Digital Forensics Conf., Australia, 2015. [Google Scholar]
21. B. Ali and A. Awad, “Cyber and physical security vulnerability assessment for IoT-based smart homes,” Sensors, vol. 18, no. 3, pp. 817, 2018. [Google Scholar]
22. O. Mazhelis and P. Tyrväinen, “A framework for evaluating internet-of-things platforms: Application provider viewpoint,” in Proc. IEEE World Forum on Internet of Things (WF-IoT), Louisiana, USA, pp. 147–152, 2014. [Google Scholar]
23. W. Xi and L. Ling, “Research on IoT privacy security risks,” in Proc. Intelligent Technology, Industrial Information Integration (ICIICII), Wuhan, China, pp. 259–262, 2016. [Google Scholar]
24. S. S. Rani, J. A. Alzubi, S. K. Lakshmanaprabu, D. Gupta and R. Manikandan, “Optimal users based secure data transmission on the internet of healthcare things (IoHT) with lightweight blockciphers,” Multimedia Tools Application, vol. 18, no. 3, pp. 1–20, 2019. [Google Scholar]
25. W. Leister, M. Hamdi, H. Abie, S. Poslad and A. Torjusen, “An evaluation framework for adaptive security for the IoT in ehealth,” International Journal of Information Security, vol. 7, no. 3, pp. 93–109, 2014. [Google Scholar]
26. D. Nkomo and R. Brown, “Hybrid cybersecurity framework for the Internet of medical things (IOMT),” in Proc. 2019 IEEE 12th Int. Conf. on Global Security, Safety and Sustainability (ICGS3), Chennai, India, 2019. [Google Scholar]
27. M. A. Jan, M. Usman, X. He and A. U. Rehman, “SAMS: A seamless and authorized multimedia streaming framework for WMSN-based IoMT,” IEEE Internet of Things, vol. 6, no. 2, pp. 1576–1583, 2019. [Google Scholar]
28. M. Usman, M. A. Jan, X. He and J. Chen, “P2DCA: A privacy-preserving based data collection and analysis framework for IoMT applications,” IEEE Journal on Selected Areas in Communications, vol. 37, no. 6, pp. 1222–1230, 2019. [Google Scholar]
29. J. Cecil, A. Gupta, M. Pirelacruz and P. Ramanathan, “An IoMT based cyber training framework for orthopedic surgery using next generation Internet technologies,” Informatics in Medicine Unlocked, vol. 12, no. 3, pp. 128–137, 2018. [Google Scholar]
30. S. Liaqat, A. Akhunzada, F. S. Shaikh, A. Giannetsos and M. A. Jan, “SDN orchestration to combat evolving cyber threats in internet of medical things (IoMT),” Computer Communications, vol. 160, no. 4, pp. 697–705, 2020. [Google Scholar]
31. B. L. Koley and D. Dey, “Real-time adaptive apnea and hypopnea event detection methodology for portable sleep apnea monitoring devices,” IEEE Transactions on Biomedical Engineering, vol. 60, no. 12, pp. 3354–3363, 2013. [Google Scholar]
32. M. Abdel Basset, N. Moustafa, R. Mohamed, O. Elkomy and M. Abouhawwash, “Multi-objective task scheduling approach for fog computing,” IEEE Access, vol. 9, no. 3, pp. 126988–127009, 2021. [Google Scholar]
33. M. Abouhawwash and A. Alessio, “Develop a multi-objective evolutionary algorithm for pet image reconstruction: Concept,” IEEE Transactions on Medical Imaging, vol. 40, no. 8, pp. 2142–2151, 2021. [Google Scholar]
34. B. L. Koley and D. Dey, “Real-time adaptive apnea and hypopnea event detection methodology for portable sleep apnea monitoring devices,” IEEE Transactions on Biomedical Engineering, vol. 60, no. 12, pp. 3354–3363, 2013. [Google Scholar]
35. A. Lakhan, M. A. Mohammed, A. N. Rashid, S. Kadry, S. Panityakul et al., “Smart contract aware ethereum and client- fog-cloud healthcare system,” Sensors, vol. 21, no. 12, pp. 4093, 2021. [Google Scholar]
36. M. Abdel Basset, R. Mohamed, M. Abouhawwash, R. K. Chakrabortty and M. J. Ryan, “EA MSCA: An effective energy aware mult objective modified sine-cosine algorithm for real-time task scheduling in multiprocessor systems: Methods and Analysis,” Expert Systems with Applications, vol. 173, no. 4, pp. 114699, 2021. [Google Scholar]
37. M. Abouhawwash, “Hybrid evolutionary multi-objective optimization algorithm for helping multi-criterion decision makers,” International Journal of Management Science and Engineering Management, Taylor& Francis, vol. 16, no. 2, pp. 94–106, 2021. [Google Scholar]
38. A. Lakhan, M. A. Mohammed, S. Kozlov and J. J. Rodrigues, “Mobile-fog-cloud assisted deep reinforcement learning and blockchain-enable IoMT system for healthcare workflows,” Transactions on Emerging Telecommunications Technologies, vol. 12, no. 4, pp. e4363, 2021. [Google Scholar]
 | This work is licensed under a Creative Commons Attribution 4.0 International License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. |