DOI:10.32604/csse.2023.025799
| Computer Systems Science & Engineering DOI:10.32604/csse.2023.025799 | |
| Article |
A Smart Room to Promote Autonomy of Disabled People due to Stroke
1Higher Institute of Sciences and Technologies, University of Gafsa, Gafsa, 2100, Tunisia
2AL-Lith Computer College, Umm Al-Qura University, Al-Lith, 28434, Saudi Arabia
*Corresponding Author: Moeiz Miraoui. Email: mfmiraoui@uqu.edu.sa
Received: 05 December 2021; Accepted: 19 January 2022
Abstract: A cerebral vascular accident, known as common language stroke, is one of the main causes of mortality and remains the primary cause of acquired disabilities in adults. Those disabled people spend most of their time at home in their living rooms. In most cases, appliances of a living room (TV, light, cooler/heater, window blinds, etc.) are generally controlled by direct manipulation of a set of remote controls. Handling many remote controls can be disturbing and inappropriate for these people. In addition, in many cases these people could be alone at home and must open the door for visitors after their identification by either moving to the door or using an intercom system which requires in both cases a physical activity. Furthermore, these people need a continuous health monitoring especially blood pressure to avoid a recurrent stroke. Smart spaces and assisted technologies would be beneficial to assist person with disabilities to live independently, enhance their quality of life and empower their autonomy. A complete system which improves and facilitates the daily life and covers all aspects such as appliances automation, appropriate interaction mode and health monitoring of these people is still lacking. The aim of this work is to create a safe and high-quality living environment for persons with disabilities to enable them to live more independently by automating the operation of a living room appliances according to the current context without the need to use remote control devices, the use of a suitable interaction modality with appliances that require direct interaction and a remote health monitoring system which can alert relatives and caregivers in case of an emergency.
Keywords: Adaptation; context-awareness; disability; health monitoring; smart room; stroke
According to the World Stroke Organization (WSO), more than 13 million new stroke patients occur each year, among them 5 million die and 5 million are left permanently disabled [1]. Survival following stroke has improved over the last few years, but it is associated with an increase in the number of severely disabled people. Stroke remains the leading cause of disability (locomotor disability) and is a major cause of death in modern society. Stroke falls within the list of chronic diseases and requires a continuous monitoring of some biological features especially blood pressure, to prevent a recurrent stroke. Stroke patients may die because of a second stroke due to delay in timely intervention. People living with disabilities due to stroke have limited motor ability, require assistance to accomplish their daily life tasks. These people spend most of their time in a living room in most cases alone, and they need to control and interact with some appliances and devices around them such as switching ON/OFF TV, increase/decrease volume, adjustment of light and windows blinds, control heating/cooling/air-conditioning system, interact with intercom system etc. This control and interaction are mainly based on a set of remote controls which is tiring and tedious because the number of remote controls to manipulate or the modality used which essentially manual activity.
Smart home or Ambient assisted living (AAL) technology is considered as the major application domain of IoT technology and could be an efficient tool to facilitate the improvement of autonomy, safety, and social participation of people with disabilities, particularly those living alone. AAL is a term that indicates the use of information and communication technologies to make the living environment adaptable for elderly or people with disability [2]. Currently, there is a broad range of enabling technologies, such as sensor networks, communication techniques, and smart appliances, which provide the necessary functionality required for AAL and smart homes.
Very little work has been done in the literature for assisting people with disability caused by a stroke, except for a few attempts to promote independent living for a person with disabilities in general. Current research on disabled person assistance and AAL has mainly focused on two aspects: home automation and remote health monitoring. Home automation was achieved by learning the user’s daily routines to both detect the conformity of his behavior and foresee his next possible actions. By knowing the routine of the inhabitant, smart home can foresee what activities he/she is likely to do next, and when to adapt appliances accordingly or automate some daily routines. Such approach requires large data sets for training models. It is also difficult to apply modeling and learning results from one person to another. In addition, disabled person may resist having their activities monitored in any way. In addition, there may be a risk that video sequence used for daily routines learning is considered to be strongly privacy violating. Remote health monitoring was achieved either by identifying if the person needs a form of assistance since an unusual activity has been recognized or using wearable sensors to gather physiological and motion information that enables patient’s status monitoring [3,4]. With recent developments in the field of wearable technology, the possibility of accurate, continuous, real-time monitoring of physiological signals has become a reality. Disabled person relatives and caregivers are alerted in case of an emergency and could also be notified in other situations when the patient requires assistance.
In spite of the significant work proposed for both appliance automation and health monitoring there still a missing complete solution for disabled persons from stroke which embed the three major aspects of life assistance for these people namely context-aware appliances adaptation, appropriate modality interaction and health monitoring. The aim of this research paper is to propose a complete system that is a smart room to assist, and take care of, its inhabitants by proactively support people with disabilities caused by stroke in their daily activities and monitor their health to avoid a recurrent stroke. The proposed system consists of the following components: 1) a context-aware adaptation system able to adapt home appliances and devices according to the current context without explicit intervention from the inhabitant or use of remote-control devices; 2) a voice modality system to control devices that need explicit interaction from the inhabitant namely TV and intercom; and 3) a remote monitoring system for health control based on wearable sensors.
The remainder of this paper is organized as follows: Section 2 discusses related work. Section 3 specifies and analyzes the main components of the proposed smart room and outlines its architecture. Section 4 discusses implementation details of the smart room; Section 5 presents a short discussion of the proposed system and Section 6 concludes the paper and presents future work.
In the literature, various studies and systems aimed at monitoring and supporting people that need assistance have been proposed. Reference [5] overviewed various scientific studies done about development of assistive technology and its current application for supporting elderly people to cope at home, with little or no help from formal and informal care givers. They also discussed the role of assistive technology for maintaining self-care and keeping quality of life of elderly people due to aging and disability. They suggested that future research must put into consideration strategies for a smooth transition to technology assisted care provision. Reference [6] have made a survey where they discussed the emergence of ambient intelligence (AmI) techniques in the healthcare domain. They examined the infrastructure and technology required for achieving the vision of AmI, such as smart environments and wearable medical devices. They summarized the artificial intelligence (AI) methodologies used for developing AmI system in the healthcare domain. They also showed how AmI technology can support people affected by various physical or mental disabilities or chronic disease. They concluded that there are still many challenges to be faced in order to complete vision of AmI and its full application in healthcare. Reference [7] conducted a review to determine the levels of technology readiness among older adults and evidence for smart homes and home-based health monitoring technologies that support aging in place for older adults who have complex needs. They concluded that the level of technology readiness for smart homes and home health monitoring technologies is still low. Reference [8] Made a literature review to identify various assistive technologies to assist the elderly. They identified the effectiveness of the proposed technologies. They concluded that, although assistive technologies have been positively evaluated, more studies are needed regarding the outcome and effectiveness of these technologies. Reference [9] made a review to analyze possible impact of information and communication technologies components, typically used in AAL solutions, to the health and quality of life of elderly. They concluded that more research using adequate methods and instruments is needed and there is still a lack of evidence of how subjective quality of life can be influenced. Reference [10] present a sensor-based telemonitoring system that addresses the monitoring of indoor and outdoor activities of elderly and disabled people to detect emergencies, recognize activities, send notifications, and provide a summary of all the relevant information. The overall telemonitoring system is part of the BackHome project. Reference [11] presented their experience in monitoring 9 elderly people for 5 months through eKauri, a sensor based tele-assistance system. The aim of eKauri was helping and supporting elderly people that live alone at home; and constantly providing a feedback to therapists/caregivers about the evolution of the status of each monitored user. Reference [12] Made a review paper to summarize recent developments in wearable sensors with focus on remote monitoring systems based on wearable technology. They discussed key technologies enabling the development and deployment of wearable technologies and remote monitoring systems. They concluded that there are significant challenges ahead before such a system can be utilized on a large scale. Reference [13] Have made a survey on automatic classification of the activities of daily living (ADLs) for elderly persons which is considered as a crucial part of assisted living technologies. The classification involves wearable and nonwearable sensors, deployment options, and signal processing and machine-learning algorithms. They concluded that hybrid generative/discriminative methods, relying on kernel metric distances, are superior to traditional generative methods such as HMM and its variants. They suggested adding several improvements in sensor technologies in several directions including size, accuracy, energy efficiency, and reliability. Reference [14] Proposed a classification of the main activities considered in smart home scenarios targeted to the elderly’s independent living, as well as proposing a general set of guidelines that would help researchers and developers select the sensors and processing techniques best suited to the target activities to detect, focusing on older adults and indoor smart home activities. Reference [15] Proposed a home automation system using gesture modality. Users should wear a special glove in order to control appliances. The system should learn the gesture made by the special glove for each device (resp. appliance). They used a role-based system for the mapping of glove gesture to commands. Reference [16] proposed a smart living room based on hybrid modular application which provides a context-aware services adaption for inhabitants. They have used three modules to make the context-aware adaption of appliances and devices namely climate system, light system, and entertainment system. Different techniques were used to ensure the adaption such as fuzzy logic, case-based reasoning and naïve bayes. Reference [17] Describes a layered model of smart homes for the purpose of delivering health care services and discussed the benefits of smart homes for elderly and disabled person who needs health monitoring. Reference [18] Proposed a voice-controlled Raspberry pi home automation system from cloning with Amazon Alexa Skills Package. Their home automation system was designed basically for either quadriplegia or paraplegia patient to control home appliances using their voices. Reference [19] Proposed a home automation system based on SVM and blockchain technology to ensure identification and authentication of the IoT devices. Their solution was based on Raspberry Pi, 5 V relay circuit which maintains the database of each appliance. Their solution is considered also as an energy-efficient one since it monitors devices power consumption. Reference [20] Proposed a voice-based system to control and operate home appliances using the geeetech voice recognition module and Arduino uno to ease life for handicapped and old aged person. They also used a Bluetooth module for wireless control. Reference [21] Proposed an application for air quality monitoring of a Smart and Healthy Intelligent Room System (SHIRS) which has an Edge-based IoT architecture. The processing air quality data was based on Machine Learning (ML) techniques to infer the number of people currently occupying a room.
As stated before, most proposed solutions were not directly oriented to disabled persons due to stroke who needs home automation system, convenient way for interaction and a health monitoring system. Most of previous work proposed a home automation system either for normal person or disabled (resp. elderly) person without a health monitoring system or an appropriate interaction modality or just a health monitoring system. To the best to our knowledge a complete solution that encompass the aforementioned subsystems required for disabled person from stroke is still inexistant.
The smart room for a disabled person from a stroke is typically like a living room composed of usual appliances and devices. It is made up of three main subsystems namely (1) the interactive subsystem which operation depends on the actions of the person such as TV and intercom system; (2) the reactive subsystem which operates by reacting to stimuli from its environment, it is in continuous interaction with its environment such as the light system (set of light bulbs), heater and cooler system, air conditioner (resp. air purifier) and the window blinds; and (3) the health monitoring subsystem which monitor the blood pressure and heart beat rate of the patient, in addition to a mobile phone which ensure the communication of the measured bio-signals (Fig. 1). The smart room is composed of three independent modules which is a preferred quality criterion that too much demanded for any application. Modular architecture has several advantages such as possibility of reusing any module in other application with minor changes, developers of such architecture can be made simultaneously which reduce the time taken for the whole system development; maintenance of the system becomes easier because the scope of errors is reduced to a simple module not extended in the whole system and finally, the management of separate modules becomes better since independent modules are easier to test, implement or design.

Figure 1: The overall architecture of the smart room
Some appliances of the smart room are reactive which means they are in continuous interaction with the surrounding contextual environment of the smart room and react accordingly. The reactive subsystem may be divided in two main components: the light system and the climate system. This subsystem has a layered architecture as indicated in Fig. 2, where the layers are as follows from bottom to top:
• Sensor layer: contains the basic sensors for raw context information capture especially indoor temperature and outdoor light brightness. This layer sends raw context to the context representation and interpretation layer.
• Context representation and interpretation layer: responsible of putting received raw context from the lower layer on a common format which can be understood by the upper layer. Generally, the format is a vector of values. In addition, the interpretation part of this layer performs interpretation of raw context to useful information such as converting the range of sensed temperature between −50 C and 50 C as a very could temperature (resp. freezing temperature). This layer sends the interpreted context in a suitable format to the adaptation layer.
• Adaptation layer: composed of two subsystems: 1) the light adaptation which perform adaptation of light inside the room according to the current context by controlling the light intensity of the set of light bulbs and the level of window blinds. 2) The climate subsystem which control the overall climate conditions in the room by controlling the operation of the cooler, heater, air conditioner and air purifier based on the current room temperature and degree of air purity. This layer takes as input the meaningful context vector from the context representation and interpretation layer and a set of command signals as output to devices and appliances layer.
• Devices and appliances layer contains a set of appliances and devices namely light bulbs, window blinds, cooler, heater, air conditioner and air purifier. All these devices, and appliances operates according to command signals received from the adaptation layer.

Figure 2: Architecture of the reactive subsystem
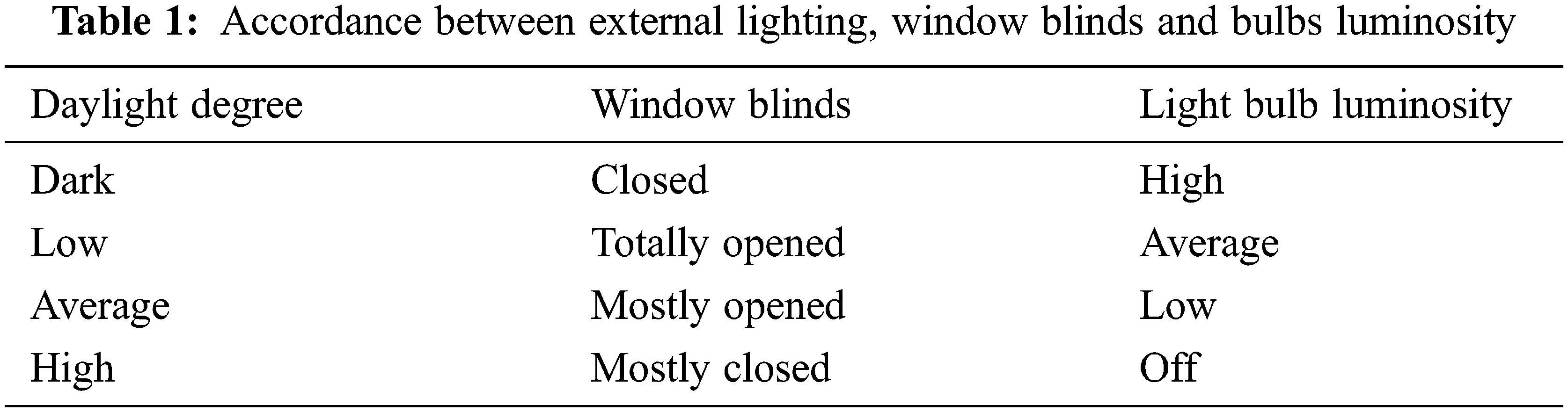
The light system is responsible of the luminosity adjustment inside the smart room using a set of light bulbs and the window blinds of the room. The lighting inside the smart room is adjusted by using the largest possible amount of external lighting from daylight to save energy consumption and turn on the lights in the absence of insufficient external lighting. This requires the window blinds to be opened at different levels according to the degree of external lighting, as well as the operation of lights with different lighting levels. This system will use a light sensor to the Tab. 1 summarizes the accordance between the window blinds opening levels and the light bulbs luminosity degrees according to the external lighting from daylight.
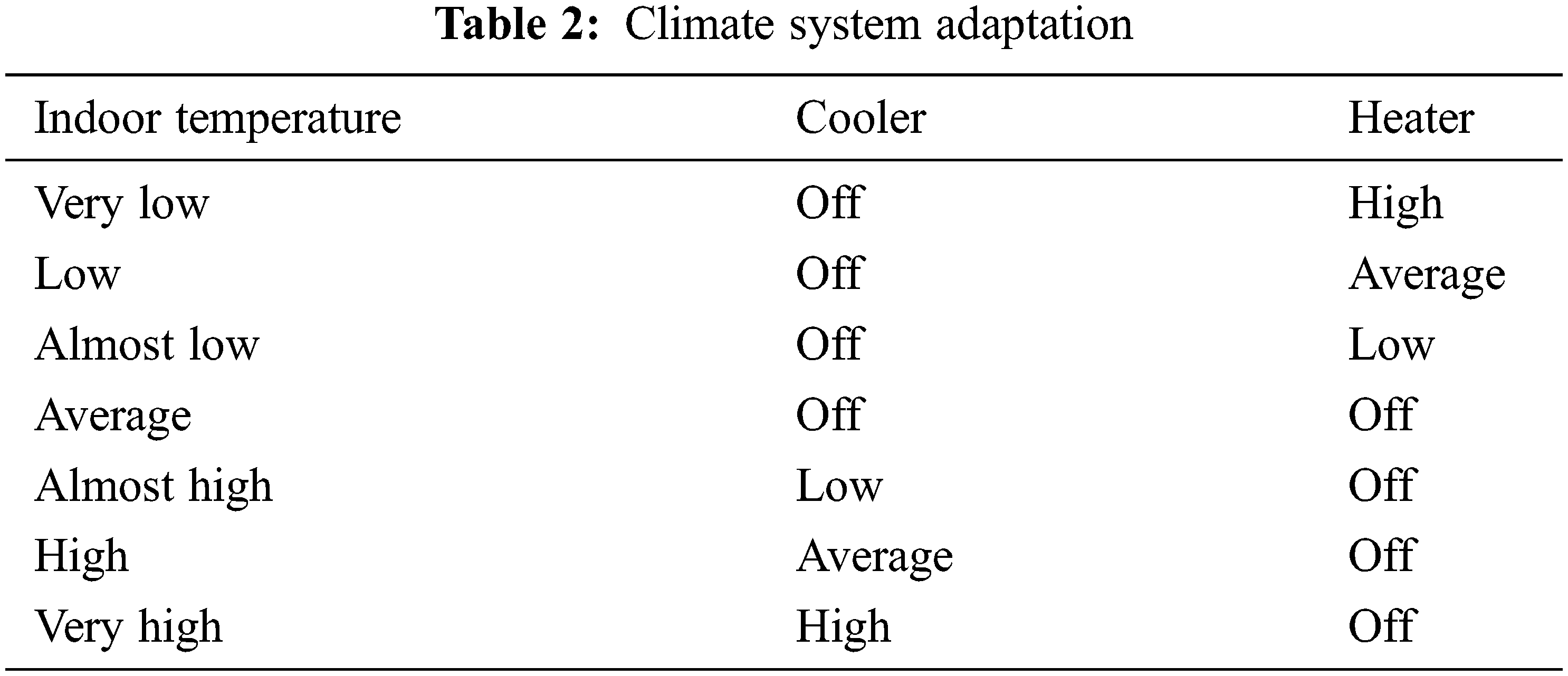
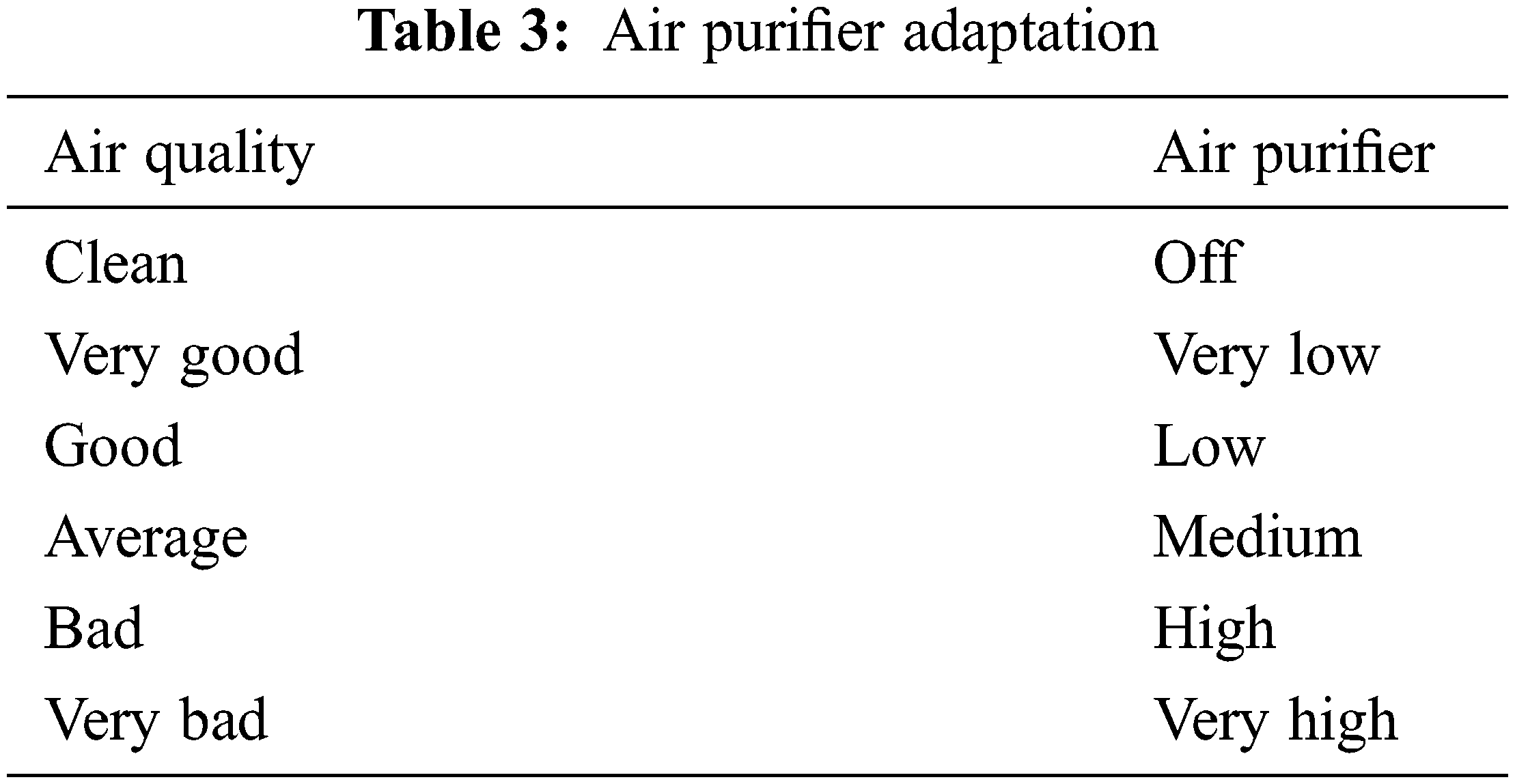
In the same way the climate system which is composed of the heater/cooler and the air conditioner (resp. air purifier) will adjust the temperature inside the smart room as well as the air quality which could affect the health of stroke patients. This system will use both a temperature sensor and air quality sensor to adapt to the desired temperature and air quality level. The temperature automatically adjustment to an average temperature which fixed previously, and the air quality level is adjusted according to CO2 and smoke threshold. Tabs. 2 and 3 show the climate system adaptation mechanism.
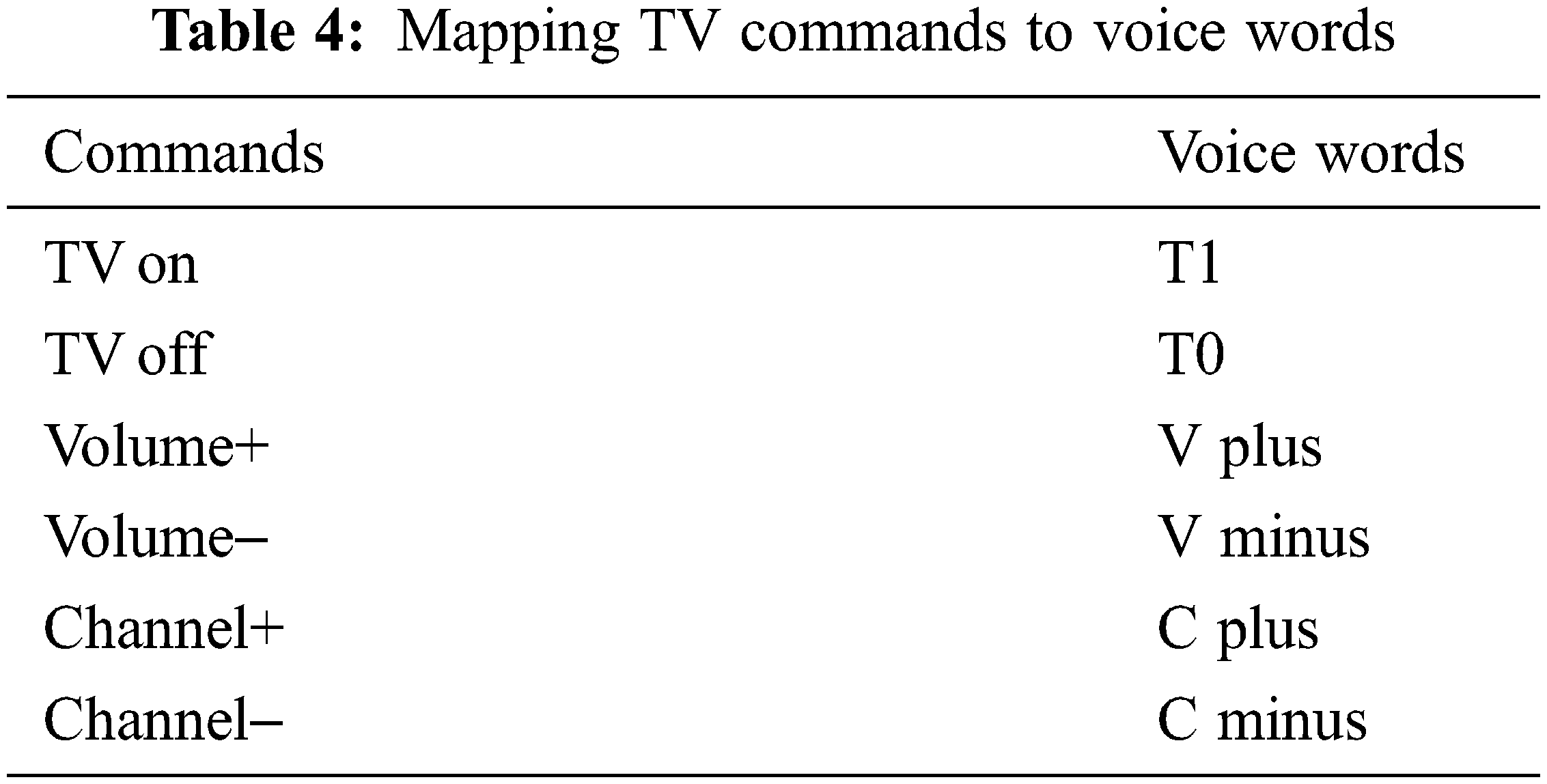
There are two main devices in the smart room that could be considered as interactive systems which respond according to the patient actions: TV and intercom system. The patient needs to execute three basic operations on TV namely put TV ON/OFF, up and down the volume and channels. For this and to avoid fatigue of the patient by using manual manipulation of the TV remote control, an appropriate method of interaction based on voice will be used. It consists of associating the remote-control commands to voice words as shown in Tab. 4.
For the intercom system, the patient needs just to command the door opening using the voice modality to avoid moving to the door and open it manually. The door closure is done automatically without the need to command it. The patient communicates with visitors using the intercom monitor which should be place close to him. The voice word used to open the door is D1.
The general architecture of the interactive subsystem is given by Fig. 3 where patient issues commands to both TV and door using voice commands as mentioned before via a close microphone. These voice commands will then be interpreted by the voice to IR waves module using a correspondence table to select the correspondent IR signal related to the voice command and finally send it to either the TV or the intercom which in its turn command the opening of the door.

Figure 3: General architecture of the interactive subsystem
3.3 The Health Monitoring Subsystem
High blood pressure is the biggest cause of strokes especially when it is 140/90 or higher. Control of high blood pressure (hypertension) is one of the most important things we can do to reduce the risk of stroke. If a person had a previous stroke, it is possible to halve the risk of stroke recurrence, if blood pressure is constantly monitored. In our case the patient blood pressure is monitored using a wearable device (sensor) to continuously measure the blood pressure and communicate it to a mobile phone which send alerts to relatives or caregivers in case of emergency. In addition, the patient mobile phone will save the blood pressure measures for a certain period for further check and analysis (Fig. 4). Currently, several types of heath bracelets which provide nearly accurate measure of bio-signals such as blood pressure or heartbeat rate are available in the market. Even current smart watches are very useful in this case.
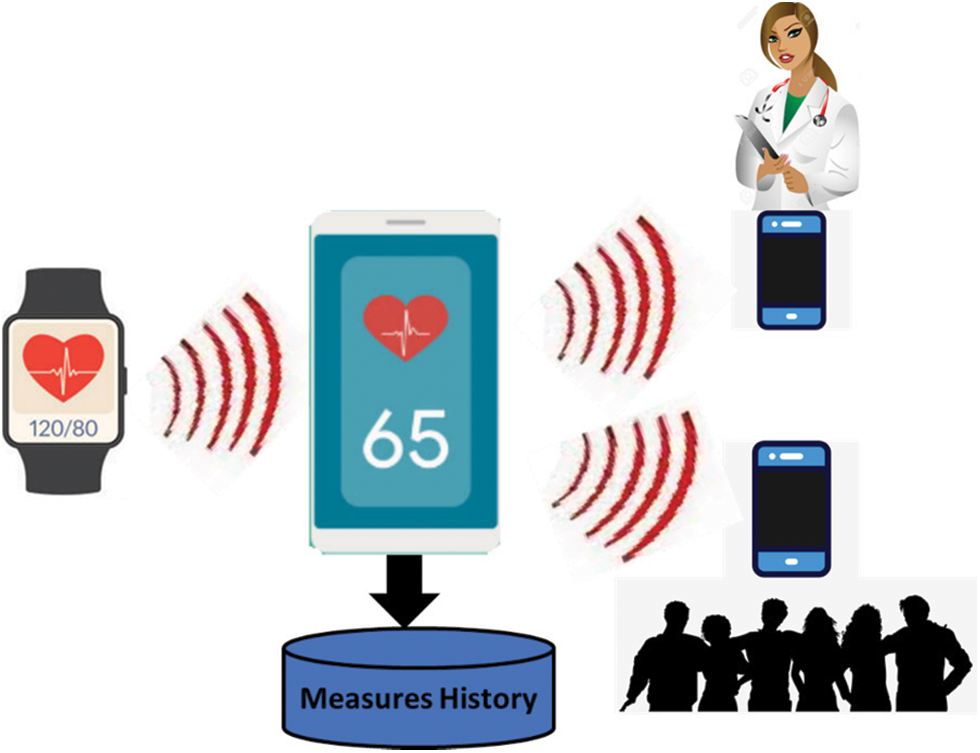
Figure 4: General architecture of the health monitoring subsystem
The smart room is implemented using Arduino as a central hub. Arduino is open-source electronics prototyping platform based on flexible, easy-to-use hardware and software [22]. The implementation schema of the smart room is given by Fig. 5.

Figure 5: Implementation schema of the smart room
All the appliances (resp. devices) of the light subsystem are commanded using remote controls. The light bulb has two commands: ON and OFF, in addition to three level of luminance namely low (default on ON command), average and high. The window blinds have two commands: up and down. Whenever the user keeps pressing one of these buttons the store will continue the action either up or down depending on the pressed button. The subsystem will sense the outdoor light (daylight degree) using a light sensor and reacts accordingly to adjust the indoor light. This task will be done automatically without explicit intervention from the patient. To accomplish this task, a simple Infra-Red receiver is used to learn the different codes of the remote control for each command. This is done for both window blinds remote control and light bulb remote control. To learn the codes commands of the remote control we should place the remote control in front of the IR receiver and press the desired button; then using the appropriate Arduino IDE for IR remote controls we will get the hexadecimal code of the button. Fig. 6 shows the general Arduino-based system for learning IR remote control codes using the Tinkercad simulator [23].
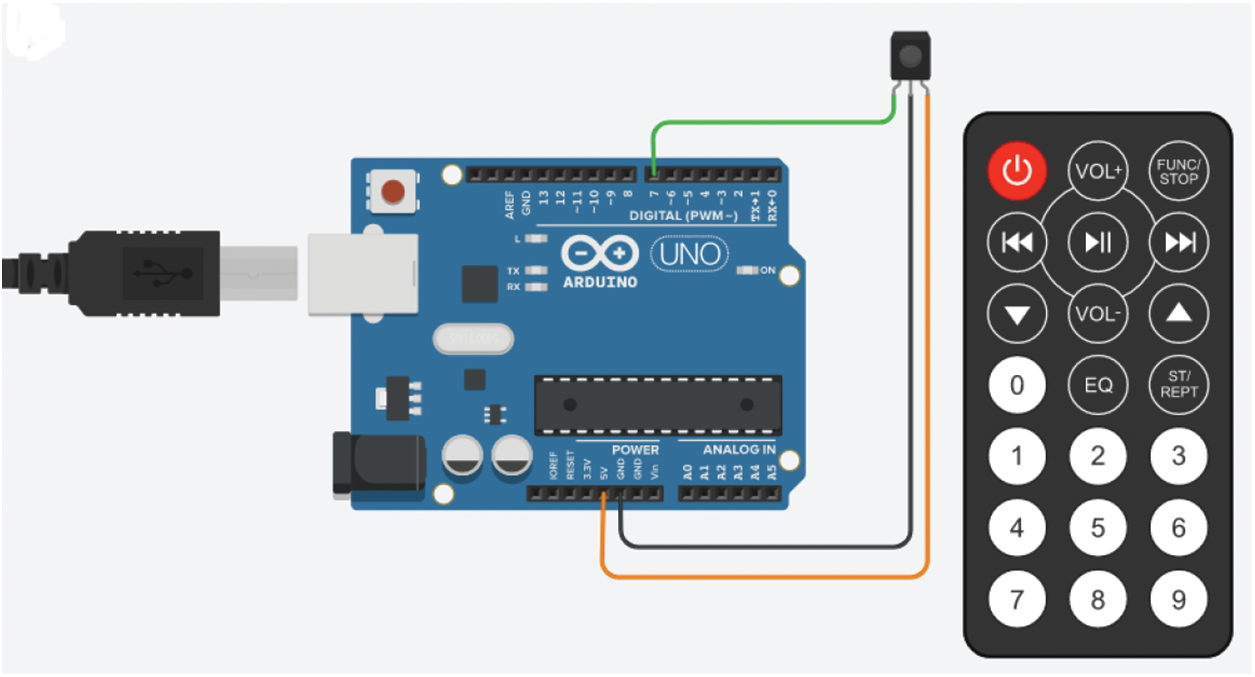
Figure 6: Arduino-based circuit for IR code learning
As an application, the system has learnt the following IR commands of a TV remote control:
• FD00FF >>>> ON/OFF
• FD807F >>>> Vol+
• FD906F >>>> Vol−
• FD50AF >>>> Ch+
• FD10EF >>>> Ch−
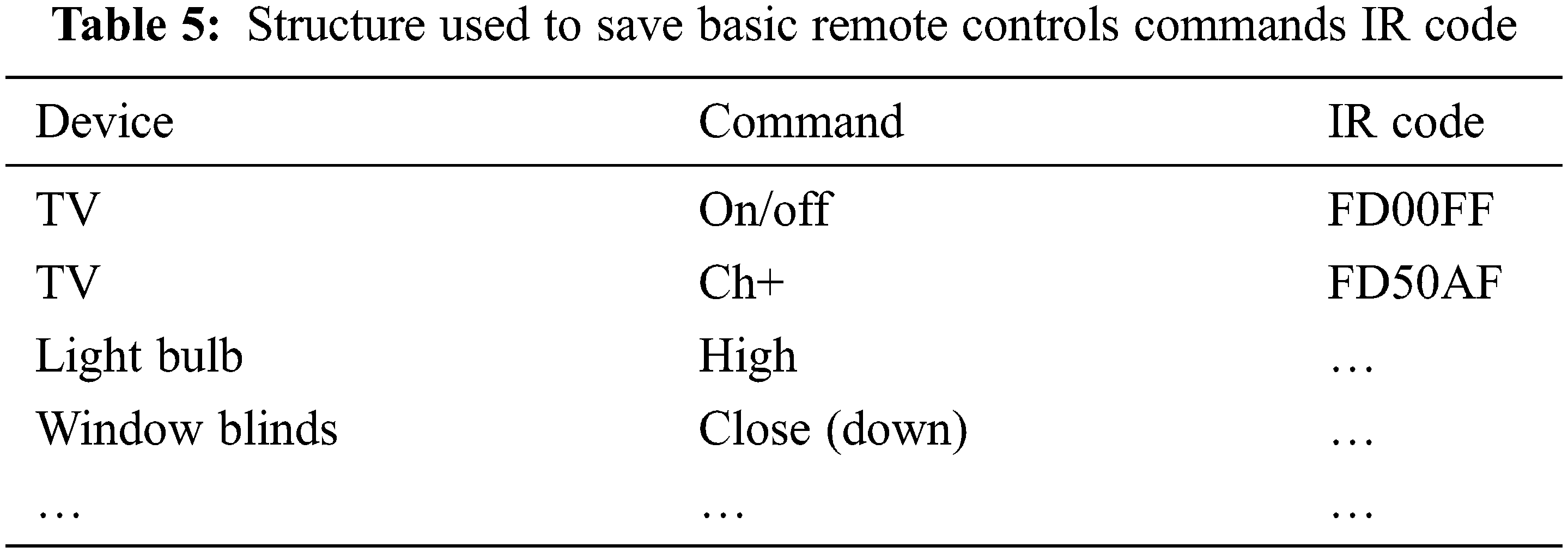
The IR codes of basic commands for each remote control of the following devices had been learnt TV, air purifier, cooler/heater, window blinds, light bulbs, and door lock opening (via intercom system). All the learnt codes were saved in a table with the structure shown in Tab. 5.
4.1 Implementation of the Light System Adaptation
The adaptation of the light system is based on the external lighting. For that reason, a light sensor (LDR: Light Dependent Resistor or simply photoresistor) is required to sense it. As mentioned before, the light system is composed of light bulb and window blind with the following states:
• Light bulb:
o Off
o On low
o On Average
o On High
• Window blind:
o Closed
o Totally opened.
o Mostly opened.
o Mostly closed.
The IR signals of the light bulb remote control are already learnt in the previous step. The window blind remote control has only two commands: down and up. To totally open (resp. close) the window blind, the down (resp. up) button should be continuously pressed during T seconds. For the state mostly opened (resp. mostly closed), the up (resp down) button should be continuously pressed during (T*3/4) (resp. T/4) seconds. An IR receiver was used for simulation purpose only because both light bulb and window blind have their own IR receiver already installed. In addition, three LEDs with different colors (red, green, and blue) are used. Each color combination is associated to one state of the light bulb and the window blind as shown in Fig. 7.
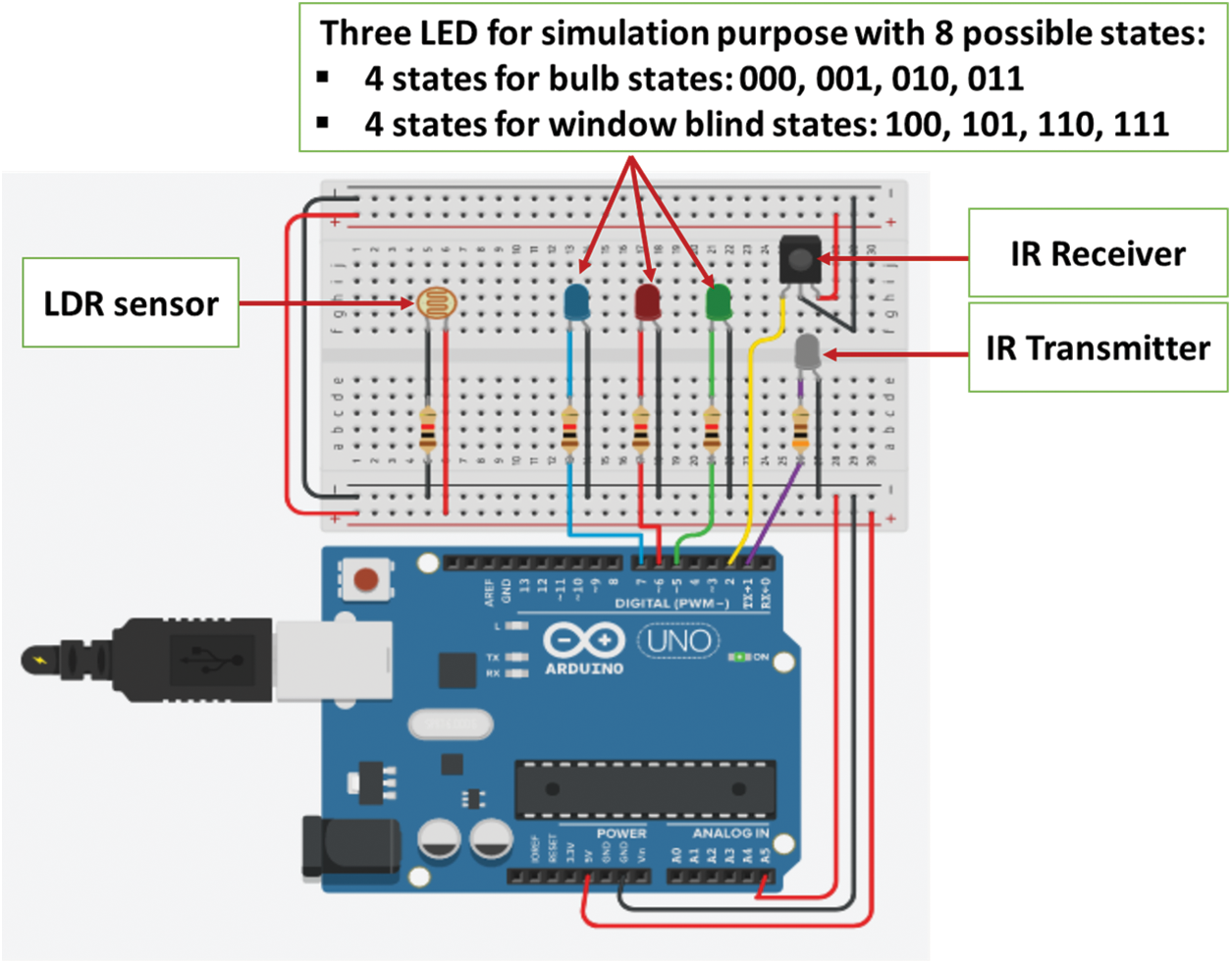
Figure 7: Arduino-based circuit for light system adaptation
The simulation of the light system adaptation was performed successfully and for each level of the external light the desired states of both the light bulb and the window blind were reached.
4.2 Implementation of the Climate System Adaptation
The climate system is composed of the heater and cooler where each of them has four states namely:
• OFF
• ON Low
• ON Average
• ON High
The ambient temperature of the smart room is sensed by a temperature sensor and according to this value the heater and cooler are set to the appropriate configuration as mentioned in Tab. 2. In all there are seven possible configurations. After sensing the indoor temperature (noted T in degree Celsius), the sensed value should be interpreted as follows:
1. Very low: 1T < 0
2. Low: 0 <= T < 10
3. Almost low: 10 <= T < 15
4. Medium: 15 <= T < 20
5. Almost high: 20 <= T < 25
6. High: 25 <= T < 35
7. Very high: 35 < T
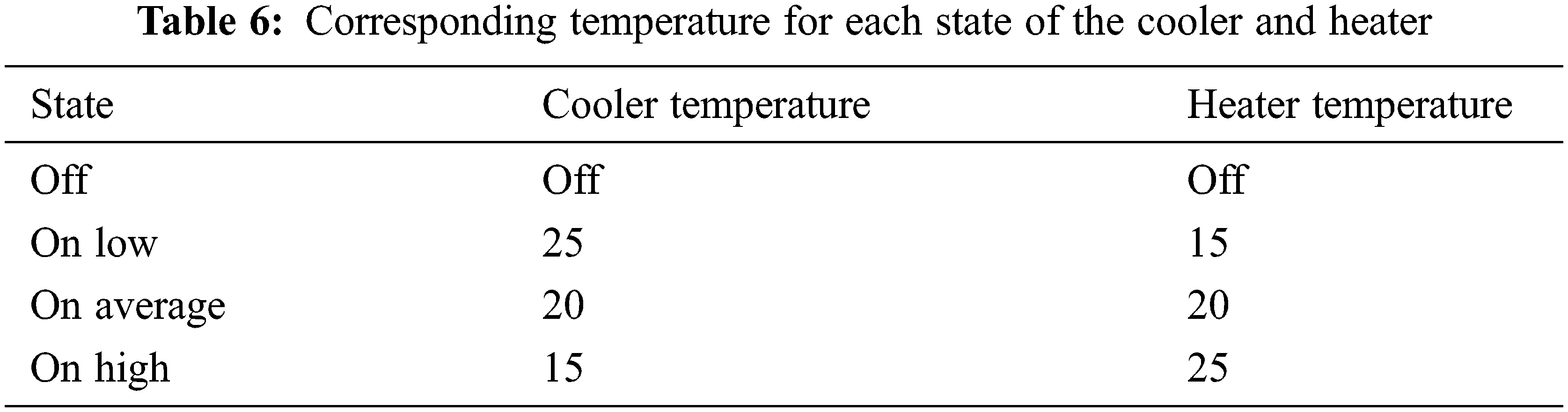
The Adaptation task consists of remotely set the both the heater and the cooler to the appropriate state according to the sensed temperature of the smart room and the mapping in Tab. 6. As mentioned before, each climate equipment has four states: OFF, ON Low, ON Average and ON High. The adaptation to each state is as shown in Tab. 6. Fig. 8 shows the Arduino-based circuit for climate system adaptation.
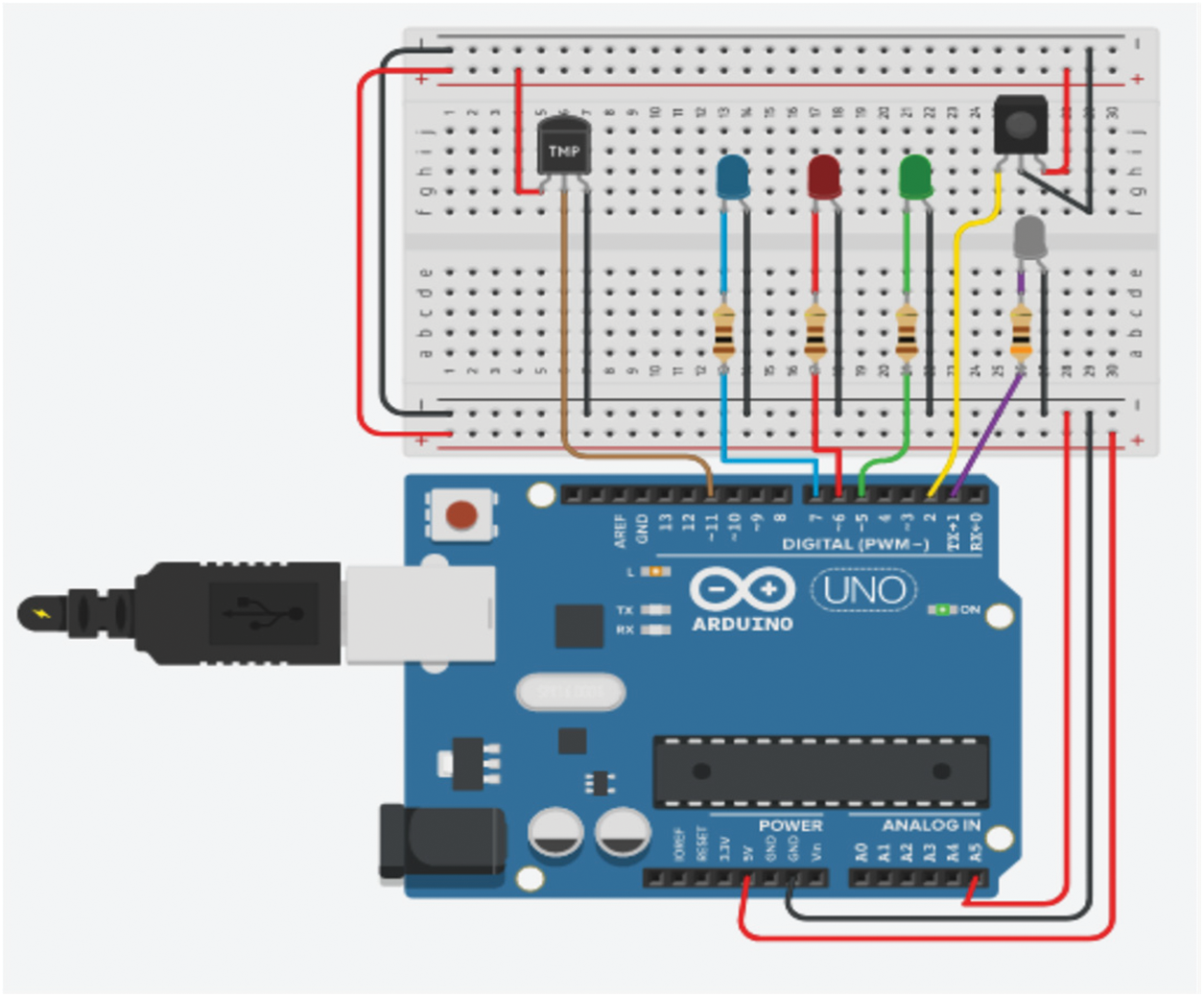
Figure 8: Arduino-based circuit for climate system adaptation
4.3 Implementation of the Air Purifier Adaptation
Similarly, to the climate and light systems adaptation, the air purifier adaptation system consists of sensing the air quality inside the smart room and setting the air purifier in one of its states as shown in Tab. 3. The used sensor can sense level of poisons gas such as butane, methane, CO2, smoke, etc. The Arduino-based circuit is almost like climate and light systems adaptations.
4.4 Implementation of the Interactive Subsystem Adaptation
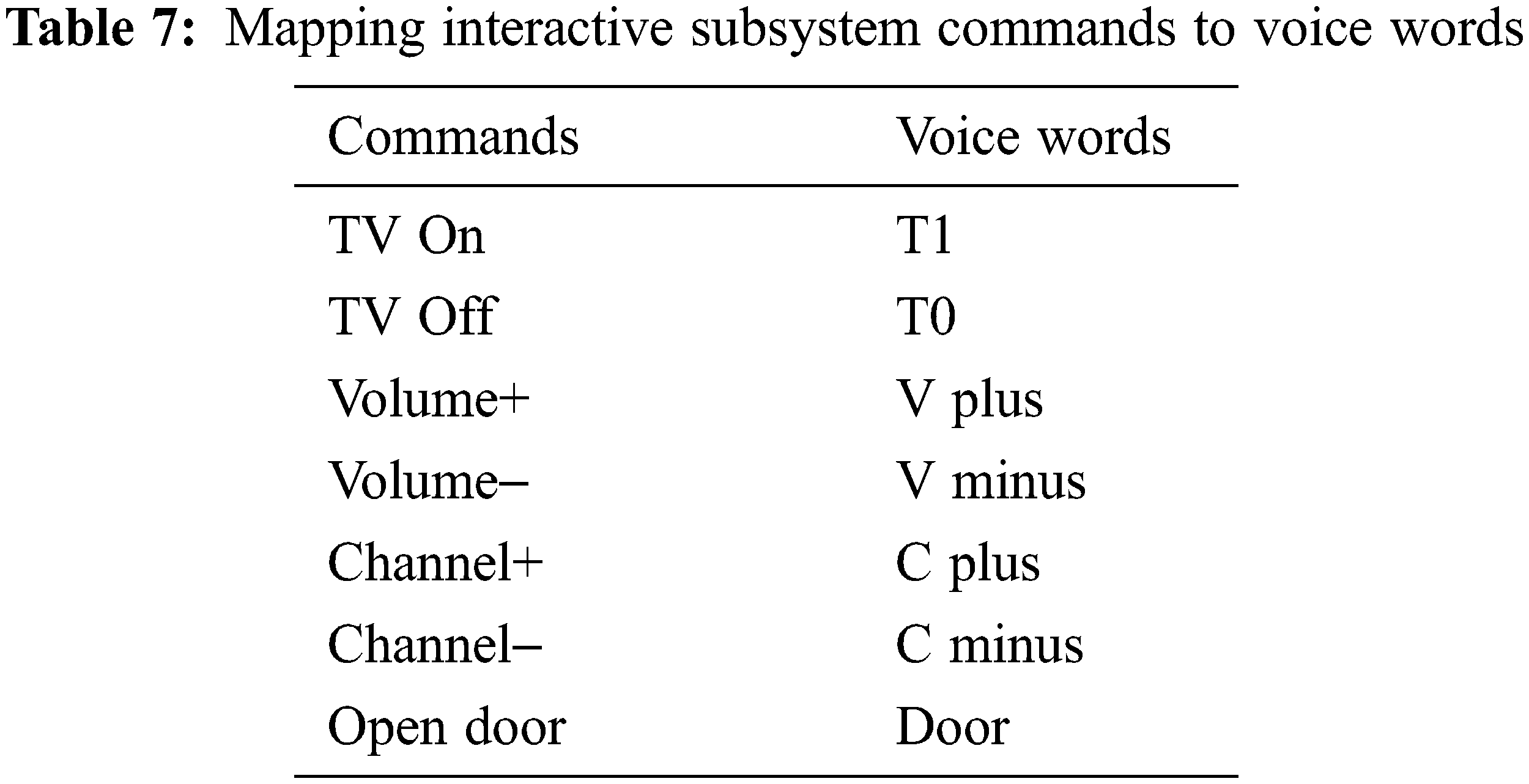
The interactive subsystem has two components namely the smart TV and the intercom. This subsystem will be controlled using voice commands in adaptation to the physical condition of people with disabilities. As mentioned before in this paper, there will be mainly eight voice commands where seven of them are related to the operation of the smart TV and one for the opening of the door which is closed automatically and do not need a command for its closure. Tab. 7 shows the mapping of interactive system commands to voice words.
In this project, we used the Geeetech speech (Module 3) recognition module [24] to record the voice commands of the interactive system devices, make the hardware connection and uploading the relative code to Arduino Uno for translating them to the corresponding infrared commands.
For the simulation of the interactive subsystem, a set of three colored LED (red, green, blue) were used with each combination of lighted led correspond to one of the eight voice command of the interactive system (e.g., the combination (red = on, green = on, blue = off) correspond to the command TV ON and the voice word T1). In addition to be more realistic an infra-red transmitter and an infra-red receiver were used in the circuit to simulate the remote controls of both the smart TV and the intercom. Fig. 9 shows the Arduino-based circuit for the interactive subsystem.
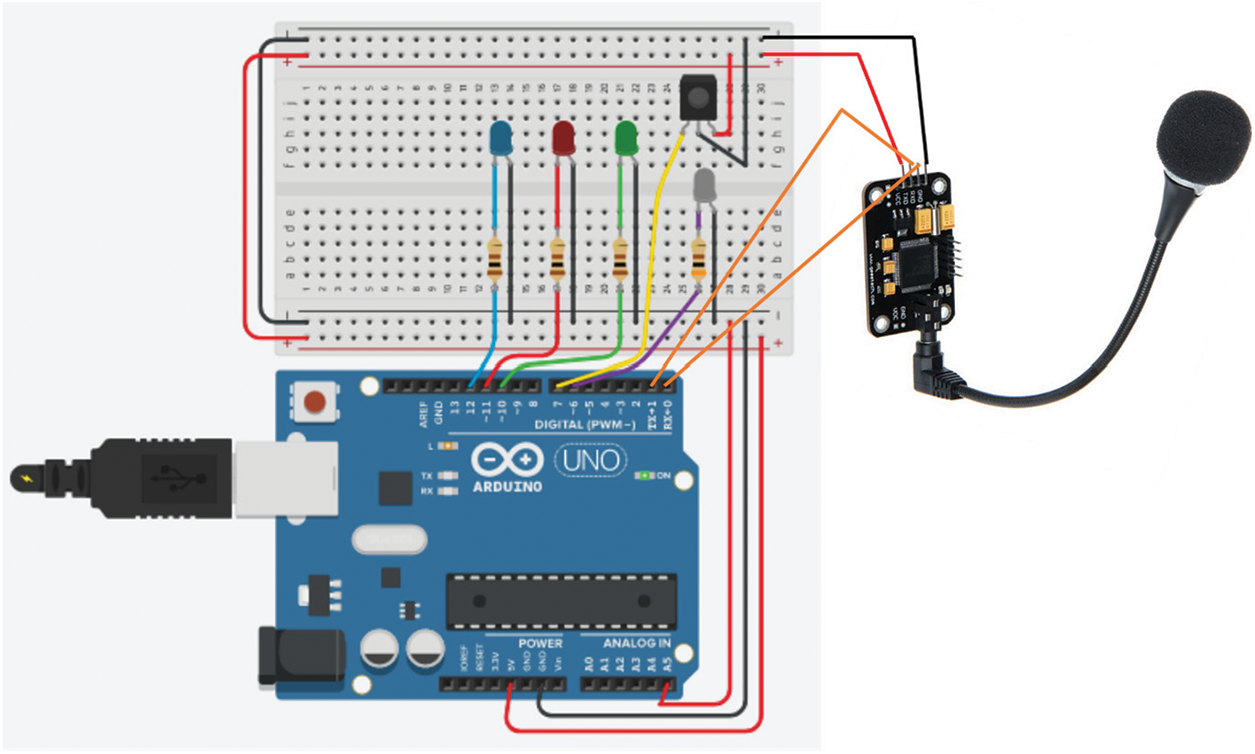
Figure 9: Arduino-based circuit for the interactive subsystem
To the best of our knowledge, the proposed smart room is a complete solution to both health monitoring and comfort improvement for person with stroke living alone. Most proposed solutions focus either on health monitoring or home automation but not both. The proposed system has a modular architecture which enhance its modification, extension, reusability, and maintenance. It encompasses both hardware and software components using IoT technologies with reduced cost which promote its manufacturing on large scale. Some components of the system are ready-made IoT devices especially those used for health monitoring. Adaptation of the reactive system is done according to the current context of the room without explicit intervention from the inhabitant which enhance its intelligence, contributes to the economy of energy consumption, improve the autonomy of disabled inhabitant helps to get rid of the large number of remote-control devices that we use nowadays. The reactive system used a voice-based command method which appropriate for disabled people living alone. The main inconvenient of using such command system is voice interference which is not really present in our case because the disabled person is most the time alone and even though he is surrounded, those present can help by the explicit use of remote controls instead of the voice-based method. In addition, the microphone of the voice-based command system is place close to the disabled person’s mouth to avoid voice interference with TV volume. The health monitoring system is made up of existing IoT devices (mainly smart phone) which promotes continuous health monitoring since all IoT devices should be connected to the internet permanently. The smart watch or health bracelet is also connected permanently to the smart phone and any deviation of biometric values especially blood pressure is immediately noticed and send to patient physician or parents.
IoT is a quantum leap in technological development. One of the most prominent applications of the IoT is smart spaces that are able to interact with inhabitants in order to provide smart services to the user to improve comfort, life quality, energy savings, security and tremendous benefits for the elderly who live alone as well as people with disabilities that are sometimes the result of stroke. Among the valuable uses of IoT is the continuous and real-time health monitoring remotely, especially for people who have a stroke, to avoid having another stroke by following up on blood pressure measurements and some other biological measurements. In this paper, we propose to integrate the advantages of smart spaces and the use of IoT for health monitoring of persons with disabilities due to stroke by developing a smart room which promote the autonomy of disabled people due to stroke by the context-aware dynamic adaptation of devices and equipment. Also, the use of a voice-based command system for interactive devices which is very appropriate for disabled people. These two modules will help to get rid of remote-control devices that require tedious and annoying manual work for people with disabilities, in addition to disposing of a good number of these devices. The third module of the smart room consists of a real-time, permanent health monitoring system based on IoT devices for monitoring among others the blood pressure to avoid the risk of stroke recurrence. The proposed solution has a modular architecture which enhance its extensibility, reusability, and maintenance. As a future improvement to this work, it is possible to add a unit to monitor and track medication doses and remind the times of taking medications.
Funding Statement: The author received no specific funding for this study.
Conflicts of Interest: The authors declare that they have no conflicts of interest to report regarding the present study.
1. M. P. Lindsay, B. Norrving, R. L. Sacco, M. Brainin, W. Hacke et al., “World stroke organization (WSOGlobal stroke fact sheet 2019,” International Journal of Stroke, Sage Publications, vol. 14, no. 8, pp. 806–817, 2019. [Google Scholar]
2. R. Andrich, N. Mathiassen, E. Hoogerwerf and G. Gelderblom, “Service delivery systems for assistive technology in Europe: An AAATE/EASTIN position paper,” Technology and Disability, IOS press, vol. 25, no. 3, pp. 127–146, 2013. [Google Scholar]
3. S. Patel, H. Park, P. Bonato, L. Chan and M. Rodgers, “A review of wearable sensors and systems with application in rehabilitation,” Journal of NeuroEngineering and Rehabilitation, vol. 9, no. 12, pp. 1–17, 2012. [Google Scholar]
4. F. Sadri, “Ambient intelligence: A survey,” ACM Computing Surveys, vol. 43, no. 4, pp. 1–66, 2011. [Google Scholar]
5. M. Sisay, “The use of assistive technology to support selfcare of elderly people at home,” B. S. thesis, Nursing Degree Program, Arcadia University, Finland, 2017. [Google Scholar]
6. G. Acampora, J. D. Cook, P. Rashidi and A. V. Vasilakos, “A survey on ambient intelligence in healthcare,” Proceedings of the IEEE, vol. 101, no. 12, pp. 2470–2494, 2013. [Google Scholar]
7. L. Liu, E. Stroulia, I. Nikolaidis, A. Miguel-Cruz and A. Rios Rincon, “Smart homes and home health monitoring technologies for older adults: A systematic review,” International Journal of Medical Informatics, ScienceDirect, vol. 91, pp. 44–59, 2016. [Google Scholar]
8. P. Khosravi and A. H. Ghapanchi, “Investigating the effectiveness of technologies applied to assist seniors: A systematic literature review,” International Journal of Medical Informatics, ScienceDirect, vol. 85, pp. 17–26, 2016. [Google Scholar]
9. C. Siegel and T. E. Dorner, “Information technologies for active and assisted living influences to the quality of life of an ageing society,” International Journal of Medical Informatics, ScienceDirect, vol. 100, pp. 32–45, 2017. [Google Scholar]
10. X. Rafael-Palou, E. Vargiu, S. Dauwalder and F. Miralles, “Monitoring and supporting people that need assistance: The backhome experience,” in Information Filtering and Retrieval. Studies in Computational Intelligence, C. Lai, A. Giuliani and G. Semerao (Ed.vol. 668, pp. 79–96, Springer, Berlin, 2017. [Google Scholar]
11. E. Vargiu, S. Dauwalder, X. Rafael-Palou, F. Miralles, A. M. Pi-Figueres et al., “Monitoring elderly people at home: Results and lessons learned,” International Journal of Integrated Care, vol. 16, no 6, pp. 1–8, 2016. [Google Scholar]
12. S. Patel, H. Park, P. Bonato, L. Chan and M. A. Rodgers, “A review of wearable sensors and systems with application in rehabilitation,” Journal of NeuroEngineering and Rehabilitation, vol. 9, no. 21, pp. 1–17, 2012. [Google Scholar]
13. C. Debes, A. Merentitis, S. Sukhanov, M. Niessen, N. Frangiadakis et al., “Monitoring activities of daily living in smart homes: Understanding human behavior,” IEEE Signal Processing Magazine, vol. 33, no. 2, pp. 81–94, 2016. [Google Scholar]
14. Q. Ni, A. B. G. Hernando and P. Pau de la Cruz, “The elderly’s independent living in smart homes: A characterization of activities and sensing infrastructure survey to facilitate services development,” Sensors, vol. 15, no. 5, pp. 11312–11362, 2015. [Google Scholar]
15. M. Miraoui, S. El-etriby, C. Tadj and A. Z. Abid, “A hybrid modular context-aware services adaptation for a smart living room,” Intelligent Automation & Soft Computing, vol. 24, no. 2, pp. 299–308, 2018. [Google Scholar]
16. S. Kashirsagar, S. Sachdev, N. Singh, A. Tiwari and S. Sahu, “IoT enabled gesture-controlled home automation for disabled and eldery,” in Proc. ICCMC 2020, Erode, India, pp. 821–826, 2020. [Google Scholar]
17. C. Zhirui Li and E. M. Borycki, “Smart homes for healthcare,” in Improving Usability, Safety and Patient Outcomes with Health Information Technology, F. Lau et al., (Ed.IOS press, Amsterdam, pp. 283–287, 2019. [Google Scholar]
18. A. Chandini and P. V. Bhaskar Reddy, “Smart home automation using a voice-bot,” International Journal of Advanced Research in Computer Science, vol. 11, no. Special Issue I, pp. 194–200, 2020. [Google Scholar]
19. M. Rizwan, A. Nurul Azma, A. Imran, Y. Ben Zikria, M. F. Mushtaq et al., “An intelligent, secure, and smart horme automation system,” Scientific Programming, vol. 2020, Article ID 4579291, pp. 14, 2020. [Google Scholar]
20. M. W. Shan and K. V. Vardhana Reddy, “Voice based controlling system for home appliances,” International Journal of Innovative Science and Research Technology, vol. 4, no. 12, pp. 693–701, 2019. [Google Scholar]
21. G. Cicceri, C. Scaffidi, Z. Benomar, S. Distefano, A. Puliafito et al., “Smart healthy intelligent room: Headcount through air quality monitoring,” in IEEE SMARTCOMP, 2020, Bologna, Italy, pp. 320–325. [Google Scholar]
22. [Online]. Available: https://www.arduino.cc/ (visited 9/15/2021). [Google Scholar]
23. [Online]. Available: https://www.tinkercad.com/ (visited 8/31/2021). [Google Scholar]
24. [Online]. Available: https://www.geeetech.com/wiki/index.php/Arduino_Voice_Recognition_Module (visited 8/25/2021). [Google Scholar]
 | This work is licensed under a Creative Commons Attribution 4.0 International License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. |