
 Submit a Paper
Submit a Paper Propose a Special lssue
Propose a Special lssue Open Access
Open Access
REVIEW

The Evidenced Effects of Early Childhood Interventions to Promote Mental Health and Parenting in the Nordic Countries: A Systematic Review
1
Faculty of Education and Welfare Studies, Health Sciences, Åbo Akademi University, Vaasa, 65100, Finland
2
Department of Health Sciences, University West, Trollhättan, 46186, Sweden
* Corresponding Author: Maria Dahlberg. Email:
International Journal of Mental Health Promotion 2023, 25(4), 505-537. https://doi.org/10.32604/ijmhp.2023.020833
Received 15 December 2021; Accepted 29 June 2022; Issue published 01 March 2023
 View Full Text
View Full Text Download PDF
Download PDFAbstract
The first years of life and the family context are key to the promotion and protection of children’s health and wellbeing, emphasizing the need for interventions aimed to support families with young children. This review aimed to explore the effectiveness of early childhood interventions developed for promoting mental health and parenting among families with young children in the Nordic countries. Six electronic databases were systematically searched, and 20 articles covering 16 studies applying various quantitative and qualitative methods met the study inclusion criteria. The studied interventions were assessed as universal health-promoting interventions and health-promoting interventions with elements of prevention. Outcomes of interest encompassed mental health, related risk and protective factors among the parents and/or the children, or child-parent interaction. The results from studies applying statistical methods show significant improvements in parents’self-efficacy, self-esteem, and parental satisfaction, while few improvements in parents’ social support or parental relationship were identified. Improvements in social support and parental relationships were however reported in qualitative studies. Most quantitative studies reporting on parents’ mental health problems and stress found a significant decrease, and qualitative studies highlighted experienced positive effects on mental health and well-being. The majority of studies reporting on children’s mental health and/or development as well as strengths and difficulties indicated a statistically significant positive development. No significant changes were however found for existing behavioral problems. The majority of studies examining parenting strategies and/or parent-child interaction found signifi- cant positive changes after the interventions. In sum, although findings are heterogeneous, early childhood interventions show various positive effects on the parenting and mental health of both children and their parents. The fact that different types of initiatives have been developed and implemented can be seen as an advantage, considering the varying needs and expectations of different families.Keywords
The overall population in the Nordic countries (Denmark, Finland, Iceland, Norway, and Sweden) experience a high level of well-being [1,2]. Studies show that this is largely due to the Nordic welfare model’s ability to create good life conditions [3,4]. The welfare model is based on the principles of universalism, meaning equal opportunities for good public health and well-being for the entire population. In practice, this means that the states offer the citizens various forms of welfare services and universal support strategies which are part of a universal insurance system [5,6].
Despite these favorable conditions, and the fact that the majority of the Nordic population has good mental health, 12.3% of the citizens more than 15 years of age show early signs of mental health problems [1]. It has been estimated that half of all mental health problems in adulthood begin during or before adolescence, and there is a high and increasing rate of mental health problems among young people in the European region. Seventeen million children and youth aged 10 to 19 suffer from mental health problems, which means 20% of the population in this age group [7]. This highlights the need for an increased focus on early initiatives and actions to promote and protect mental health in early childhood.
1.1 Promotion and Prevention in Mental Health
In order to improve the population’s mental health, it is pivotal to not only prevent and address mental health problems but to also emphasize mental health promotion in various contexts [8,9]. Even if the terms prevention and promotion are clearly related and overlapping, it is useful to make a theoretical distinction between these concepts. Mental health promotion focuses on positive mental health, and the purpose is to build psychosocial strengths, competencies, and resources, and to create supportive environments while prevention of mental health problems focuses primarily on reducing the incidence, prevalence, or severity of targeted problems [8].
A model, initially developed by Mrazek et al. [10], divides preventive initiatives into three categories: universal, selected, and indicated. Indicated activities are designed for high-risk groups with incipient difficulties, while selective activities are targeted to identified risk groups. The universal initiatives target the whole population, focusing on protective factors rather than risk factors, hence applying a more health-promoting approach [8].
1.2 The Importance of Early Childhood and Parenting
The first years of life are recognized as a particularly sensitive period because they lay the foundation for lifelong physical, mental, and social development [11,12]. Development theorists have emphasized the importance of a safe and secure home environment, a supportive family, and early attachment, along with support from the local community, as protective factors for a child’s positive psychosocial development (e.g., [13–15]). Strengthening family dynamics and the interaction between parents and children is one of the most important protective factors for child development and well-being throughout life [16–18]. Introducing health promotion and prevention efforts during the first five years of life is one important strategy for reducing mental health problems at the population level [19].
In order to support the child, it is recommended to work with the whole family as a unit [20]. Early childhood interventions are designed to reduce risk factors for negative development and to enhance protective factors for positive development. The common emphasis of these interventions is to support parent-child interaction and parenting [16,18]. Various types of structured early childhood interventions have been developed internationally [21,22]. No single intervention can meet the diverse developmental needs of all children, and there is therefore a continuous need for various types of support and services with documented effects [8,23].
The World Health Organization (WHO) has recently collected evidence and published guidelines on improving early childhood development and recommends interventions that strengthen parent-child interaction and support parents in their parenting. Such early childhood interventions encourage stable and healthy family relationships and provide a safe environment for the child which in turn promotes positive child development and mental health [24,25].
1.3 Early Childhood Interventions for Promoting Mental Health
Several international systematic reviews and meta-analyses have evaluated universally offered early childhood interventions and have found significant improvements in mental health and/or parenting outcomes (e.g., [26–35]). The early childhood interventions can be conducted with individual families in their homes (e.g., [32,35]), can be group-based, and delivered at community facilities such as hospitals, social work clinics, preschools, or churches (e.g., [27,29,31]), or be online-based (e.g., [29]). What all these interventions have in common is the aim to improve children’s and parents’ mental health by supporting the parent-child attachment or interaction, focusing on, e.g., the parents’ knowledge, attitudes, and understanding [26,28,29,32–35].
While a narrative review of Nordic interventions focusing on promoting infants’ attachment and parents’ sensitivity has recently been performed [36], to date, no review has been conducted of early childhood interventions in the Nordic countries focusing on universal health-promoting initiatives. The aim of this systematic review was therefore to gather, describe and evaluate early childhood interventions developed for promoting mental health and parenting among families with young children in the Nordic welfare countries.
This systematic review was performed in accordance with the guidelines presented in the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) statement [37]. The selection criteria were defined in accordance with the standard PICOS terminology (Participants, Interventions, Comparisons, Outcomes, and Study design) [37].
Studies were included based on the following inclusion criteria: a) interventions targeted families and/or parents of young children (or parents-to-be), aiming to promote and protect the family’s (parents’ and/or children’s) mental health, with a focus on parental support; b) children were aged 0–6 years, or alternatively, the mean age of the children was ≤7 years; c) interventions were delivered in the Nordic countries; d) articles were published in English, between the years 2000 and 2020.
Intervention studies where the participants were showing early signs or symptoms of mental health problems (but not fulfilling diagnostic criteria) and interventions aimed at identified risks, e.g., parental stress or children’s problem behaviors, were included. Studies could use a randomized controlled or quasi-experimental design, and quantitative or qualitative methods could be applied. Studies were excluded if the intervention was: a) developed to treat mental disorders; b) delivered through schools; c) the participants exhibited severe problems, where, e.g., children were in the care of social services.
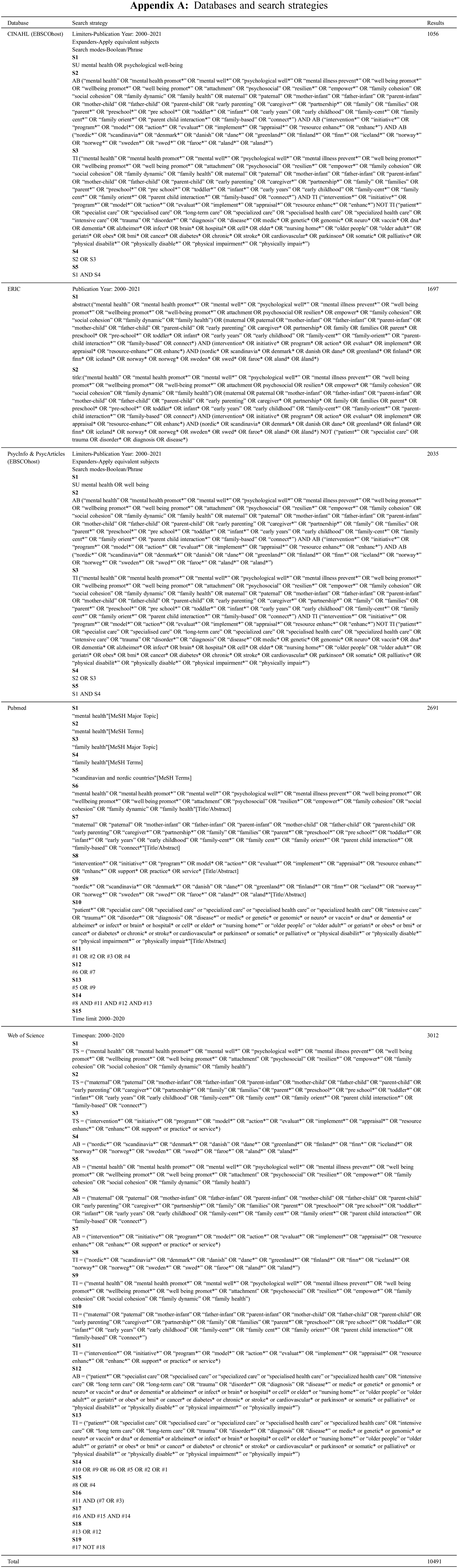
The electronic searches were conducted in October 2020. The following international databases were searched: CINAHL, ERIC, PsycInfo, PsycArticles, Pubmed, and Web of Science using database-tailored search strategies (see Appendix A).
2.4 Screening Procedure and Study Selection
A total of 10531 records were identified (see Fig. 1 for the screening and selection process). After the removal of 768 duplicates, the titles and abstracts of 9763 records were independently screened by four researchers. The full-text screening was performed on 241 articles and their relevance was reevaluated based on the inclusion criteria. Uncertainties concerning the study inclusion were resolved through discussions within the research group. Additionally, the snowballing technique was applied, i.e., the reference lists of the included articles were checked for additional relevant studies, and identified reviews were also checked for relevant original studies. Finally, 20 relevant articles were included in this systematic review.
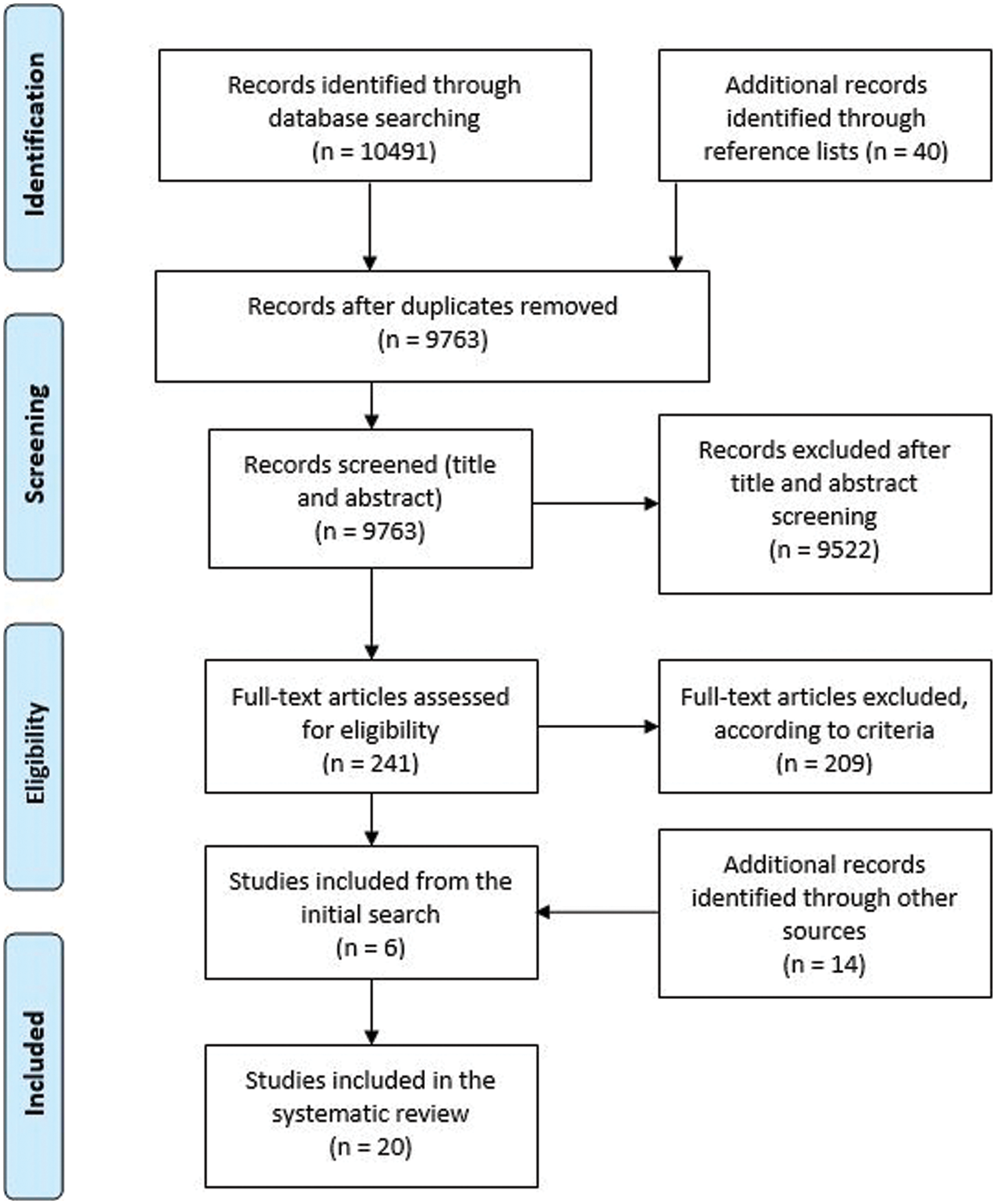
Figure 1: PRISMA Flow Diagram illustrating the screening and selection process
2.5 Data Extraction and Coding
In this review study, outcomes related to mental health in parents and/or children and outcomes related to parenting have been of interest, while outcomes related to, e.g., sociodemographic factors and physical health have been excluded. Information covering, e.g., intervention content and execution, participants, outcome measures, method of analysis, key results, and study limitations was coded from a total of 20 publications, covering 16 studies, using an established coding scheme [37]. Articles reporting on the same study samples were parallel-coded [38–41]. Any uncertainties regarding data coding were discussed among all review authors until a consensus was reached.
3.1 Characteristics of Included Studies
A total of 20 publications covering 16 intervention studies were included in this systematic review (study details are outlined in Appendix B). Ten intervention studies applying quantitative research methods and six studies applying qualitative methods were included. Seven of the quantitative studies had a follow-up period (6 weeks to 24 months after the end of the intervention) and/or a control group design, of which four were randomized-controlled trials (RCTs). The included studies were conducted in Finland (seven), Sweden (six), and Norway (three).
There was a considerable variation in sample size between the included studies. Some of the studies targeted the whole family or extended family (sample size ranged from 5 to 1300, mean 217.89), while other studies were limited to the parents (sample size ranged from 77 to 759, mean 376). All studies encompassed parents of both genders, with the exception of one study focusing specifically on fathers [42].
Two types of interventions were identified among the included studies; family-focused activities primarily carried out in the participating families’ homes [42–48], and group-based activities carried out at community facilities e.g., social and health care centers, kindergartens, preschools, and club facilities [49–55]. One intervention [56] combined both family-focused and group-based activities, while another [57] intervention was carried out online and consisted of an information database and a discussion forum. The interventions were delivered by a range of professionals, i.e., public health nurses, social workers, family counselors, and preschool teachers, who had also received training prior to the intervention delivery.
In two of the interventions encompassing family-focused sessions, the intervention content was based on larger intervention programs or projects: The extended home visiting program [42], and The European Early Promotion Project (EEPP) [47]. In some of the group-based intervention studies, the intervention content was based on larger intervention programs or projects: The International Child Development Programme (ICDP) [49,53], The ABC parenting group program [50,55], The Short Basic Incredible Years intervention program (S-IY) [52], and The COPE program [54].
3.1.4 Intervention Content and Duration
The family-focused interventions consisted mainly of psychoeducation and discussion activities. Some of the family-focused interventions also encompassed video recording, analysis, and feedback on normal family life situations. In the group-based interventions, the reported group size varied between five and twelve participants, except for The COPE program consisting of a larger group with 25–30 participants. The sessions consisted of, e.g., psychoeducation, different types of assignments and exercises, parental counseling, discussions, and feedback.
Three studies reported the intervention duration in months (1–18), while the remaining studies reported the number of visits or sessions. The number of visits or sessions ranged between 1 and 58; ten studies reported visits or sessions between 1 and 10, and three studies reported an average number of visits or sessions, ranging between 14.1 and 21. Each visit or session lasted between 15 min and 2.5 h.
Half of the included studies had a universal health-promoting approach [42,44,48–50,53,55,57]. These interventions were designed without regard to individual risk factors. The programs were broadly aimed at supporting parenthood and family relationships, as well as recognizing and improving parents’ resources.
The other half of the included studies applied a health-promoting approach with elements of prevention [43,45–47,51,52,54,56]. In these studies, the intervention content was future- and solution-oriented but devoted mostly to problem-solving and targeted families where some form of challenge occurred, e.g., parental stress or children’s problem behaviors.
Three main categories of outcome measures were distinguished (see Table 1). All ten of the included quantitative studies measured outcomes among parents, while nine measured outcomes among children, and six measured outcomes covering the parent-child interaction.
a) Parental outcomes were measured using, e.g., the Satisfaction with Life Scale, Cantril’s Self-Anchoring Ladder of Life Satisfaction Scale, What Being the Parent of a New Baby is Like (WPBL-R), Parental Self-Efficacy Scale (PSE), Parenting Sense of Competence Scale (PSOC), Generalized Self-Efficacy Scale, General Health Questionnaire (GHQ12), Hospital Anxiety and Depression Scale (HADS), Depression Anxiety Stress Scale (DASS-21), UCLA Loneliness Scale, Interview Schedule for Social Interaction (ISSI), Dyadic Adjustment Scale, Parental Locus of Control Instrument (PLOC), Parenting Stress Index (PSI), and Swedish Parenthood Stress Questionnaire (SPSQ).
b) Child outcomes were measured using, e.g., the Child Health and Development (CHD) instrument, Strengths and Difficulties Questionnaire (SDQ), Eyberg Child Behavior Inventory (ECBI), and Behavioral Screening Questionnaire (BSQ).
c) Outcomes related to the parent-child interaction were measured using, e.g., the Relationship Questionnaire (RQ), Conflict Tactics Scale, and Parenting Practices Interview (PPI).
3.1.7 Methodological Quality of the Studies
Quality assessment was performed utilizing the NICE checklists, with separate systematic guidelines for evaluating quantitative and qualitative studies [58,59]. The overall validity of the studies was coded as ++, +, or –. ++ indicated a high-quality score, with all or most checklist criteria fulfilled. + indicated a moderate quality score, where some, but not all, checklist criteria had been met. – indicated a low-quality score, with few or none of the checklist criteria fulfilled. Study quality was assessed by two review authors. The majority (n = 12) of the included studies were rated with a moderate quality score (see Appendix B for listed study limitations).
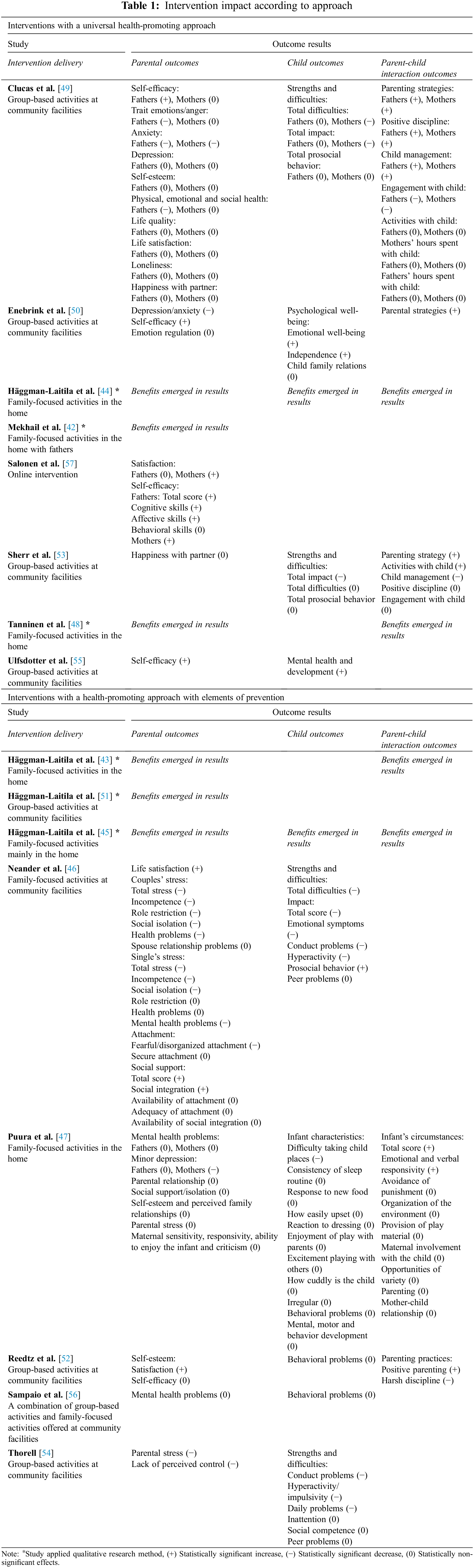
3.2 Evidence on Intervention Impact according to Approach
Table 1 summarizes the intervention impact according to the two approaches: interventions with a universal health-promoting approach and interventions with a health-promoting approach with elements of prevention. The outcome results are divided into parental, child, and parent-child interaction outcomes. Seven of the quantitative studies [46–47,50,52,55–57] had a follow-up period and for these studies, pre- to follow-up-changes are reported. For the studies without a follow-up period [49,53,54], pre- to post-changes are reported. If all the subscales in an instrument showed a change in the same direction, the overall impact is reported.
3.2.1 Intervention Outcomes among Parents
Parental self-efficacy and self-esteem. Four quantitative studies covering interventions with a universal health-promoting approach [49–50,55,57], and one quantitative study classified as a health-promoting intervention with preventive elements [52] evaluated parents’ self-efficacy. All four interventions with a universal health-promoting approach found statistically significant improvement in parents’ self-efficacy, while no statistically significant effect was identified for the intervention with preventive elements. Looking at the studies more in-depth, Clucas et al. [49] found significant improvement in fathers’, but not in mothers’, self-efficacy. Another study [57] found significant improvement in both parents’ total scores, but there were differences in the subscales between the parents. Among the mothers, statistically significant positive changes were found in all the subscales of cognitive, affective, and behavioral skills, while the fathers’ cognitive and affective skills improved statistically, but not their behavioral skills [57]. Furthermore, Clucas et al. [49] and Puura et al. [47] examined parental self-esteem, but no statistically significant effect was found.
Six studies applying qualitative methods indicated improved parental self-efficacy and self-esteem, e.g., parents reported that their confidence, self-knowledge, and childcaring skills had improved [44], that they had discovered their own hidden skills and felt successful and able to support their children’s development [43], that their awareness of personal resources and reliance on their ability to cope was strengthened and improved [51], and that they had become better at coping with everyday life [48]. Häggman-Laitila et al. [45] reported that the parent’s need for support regarding coping with parenthood decreased drastically from 77% to 3% after the intervention, and Mekhail et al. [42] reported that the intervention met the participating father’s need for support regarding knowledge and parental confidence.
Parental satisfaction. Parental satisfaction was measured in four quantitative studies. Three interventions [46,52,57] significantly improved parental satisfaction, while one study [49] found no significant changes associated with parental satisfaction or life quality. Analyzing men and women separately, Salonen et al. [57] found significant improvement in mothers’, but not fathers’, satisfaction.
Three of the qualitative studies also indicate improved life satisfaction, e.g., parents reported that they had made positive discoveries about everyday life [43] and that their recreation, such as rest, joy, and company, had improved [51]. Tanninen et al. [48] reported that the participating parents evaluated that their overall living conditions had improved.
Parental social support. Three studies applying quantitative methods reported on outcomes related to the parents’ social support. Neander et al. [46] found that the total score of social support and the subscale of social integration had significantly increased, while no significant changes were found for the availability and adequacy of attachment, or availability of social integration. Clucas et al. [49] reported no significant changes in parents’ experienced loneliness and Puura et al. [47] found no significant changes in parents’ experienced social support, isolation, or family relationships.
Also, four studies where interview methods were applied indicated improved social support, e.g., parents reported that their social support networks were strengthened [51], that they gained information about channels of support [42], and that their need for support regarding social relations decreased from 43% to 17% [45]. Tanninen et al. [48] reported that 85% of the participating parents felt that the intervention benefitted them with regard to getting support to raise children and handle tasks of parenting.
Parental relationship. Outcomes related to the relationship between the parents or spouses were evaluated in three quantitative studies. No statistically significant changes were found in parental relationships [47] nor happiness with a partner [49,53].
However, three qualitative studies reported improvements in parental relationships, e.g., that the relationship between parents was perceived to be strengthened [44], and that the intervention was experienced as beneficial for the parent’s relationship as a couple [48]. Häggman-Laitila et al. [45] reported that the participants’ need for support regarding the parents’ relationship decreased slightly from 53% to 43% and that 73% of those who wanted the intervention to support the parent’s relationship achieved this goal.
Parental mental health and well-being. Five quantitative studies evaluated parental mental health problems. Neander et al. [46] reported that the participating parents’ mental health problems significantly decreased. Furthermore, they found that the parents’ fearful/disorganized attachment significantly decreased, but no significant changes in secure attachment were reported. Enebrink et al. [50] found that the participating parents’ depression and anxiety had significantly decreased at the post-intervention measurement, but they found no significant changes in emotion regulation at the follow-up measurement. Clucas et al. [49] found that both parents’ anxiety decreased significantly but found no significant changes in the participating parents’ depressive symptoms. Furthermore, the study [49] found that the participating fathers’, but not the mothers’, emotional, and social health and also anger decreased significantly. Puura et al. [47] and Sampaio et al. [56] found no significant changes in parents’ overall mental health problems. However, Puura et al. [47] did find that mothers’, but not fathers’, symptoms of minor depression significantly decreased. Finally, no significant changes in maternal sensitivity, responsivity, ability to enjoy the infant, and criticism were identified in the study by Puura et al. [47].
Three qualitative studies reported an improvement in participants’ well-being. Parents reported e.g., improved health and coping ability [44], and that the need for support associated with parents’ health and well-being decreased from 87% to 23%, and that 83% of those who wanted the intervention to improve well-being felt that this goal was achieved [45]. Also, Häggman-Laitila et al. [43] reported on statements that may indicate increased well-being, e.g., the parents gaining distance from their own lives, learning to observe family life from the outside and free from emotions, and seeing their children and themselves in a new way.
Parental stress. Three of the quantitative studies of health-promoting interventions with preventive elements examined parental stress. Thorell [54] found that parental stress and parents’ lack of perceived control significantly decreased. Neander et al. [46] evaluated couples’ and single parents’ stress separately and found that the couples’ total stress and subscales covering incompetence, role restriction, social isolation, and health problems significantly decreased, while no significant changes were found in the subscale for spouse relationship problems. Single parents’ total stress, incompetence, and social isolation scores significantly decreased, but no significant changes were found in the subscales for role restriction and health problems. Puura et al. [47] found no statistically significant changes in parental stress.
3.2.2 Intervention Outcomes among Children
Children’s mental health and development. Three quantitative studies examined children’s mental health and development. Enebrink et al. [50] found that the children’s emotional well-being and independence significantly improved but found no significant changes in child family relations. Ulfsdotter et al. [55] found that the children’s mental health and development significantly improved. Puura et al. [47] on the other hand, found no significant changes in children’s mental, and behavioral development nor in infant characteristics (with the exception of one subscale, difficulties taking child places significantly decreased).
Two of the studies applying interview methods reported on children’s outcomes. Häggman-Laitila et al. [44] reported that the children’s health and conditions were improved, and Häggman-Laitila et al. [45] reported that 27% of the participating parents hoped the intervention would support their children’s health and development and that this goal was achieved by 33% of participants.
Children’s strengths, difficulties, and behavioral problems. Seven studies applying quantitative methods examined children’s strengths and difficulties or behavioral problems. Four studies measured children’s strengths and difficulties with the Strengths and Difficulties Questionnaire (SDQ). Clucas et al. [49], Neander et al. [46] and Sherr et al. [53] reported that the SDQ total impact score (parental reported overall distress and social impairment resulting from child difficulties) significantly decreased. Clucas et al. [49] found a significant decrease in mothers’ total impact scores, but no statistically significant changes in fathers’ scores. Neander et al. [46] reported separately for each subscale; emotional symptoms, conduct problems and hyperactivity significantly decreased, while prosocial behavior significantly increased, and no significant changes were reported in peer problems. Clucas et al. [49] and Neander et al. [46] also reported a significant decrease in SDQ total difficulties, meaning e.g., a decrease in children’s emotional symptoms and conduct problems reported by the parents. Here, Clucas et al. [49] found a significant decrease in mothers’, but not fathers’, reports. Sherr et al. [53] found no statistically significant changes in child difficulties. Furthermore, Clucas et al. [49] and Sherr et al. [53] found no statistically significant changes in SDQ prosocial behavior, meaning positive changes in children’s prosocial behavior. In another study [54] where the SDQ outcomes were reported in a slightly different way, children’s conduct and daily problems, and hyperactivity and impulsivity significantly decreased, but no significant changes in inattention, social competence, and peer problems were identified. Three of the studies [47,52,56] examining health-promoting interventions with preventive elements assessed children’s problem behaviors with instruments other than the SDQ. These studies identified no significant changes in children’s behavioral problems.
3.2.3 Intervention Outcomes Related to Parent-Child Interaction
Parenting strategies and parent-child interaction. Outcomes related to parenting strategies and parent-child interaction were examined in five of the quantitative studies. Clucas et al. [49], Enebrink et al. [50], and Sherr et al. [53] found significant changes in parenting strategies, while Puura et al. [47] found no significant changes in parenting. Additionally, Clucas et al. [49] found significant improvement in both parents’ positive discipline and child management, while the engagement with the child significantly decreased. No significant changes were found in activities with the child nor hours spent with the child [49]. In the study by Sherr et al. [53] no significant improvement in activities with the child was identified, while child management significantly decreased. In the same study, no significant changes were found in positive discipline nor engagement with the child. Reedtz et al. [52] found that positive parenting significantly increased, while harsh discipline significantly decreased. Finally, the study by Puura et al. [47] examining infants’ circumstances found that the subscales for total score and emotional and verbal responsivity significantly improved, while no significant changes in the mother-child relationship were found.
Four of the studies applying qualitative research methods reported an improvement in parenting and interaction. Häggman-Laitila et al. [43] reported, e.g., that the parents had gained new perspectives on parenthood, that they were interacting more positively with their children, and that they had become more sensitively able to identify their children’s needs. Häggman-Laitila et al. [44] reported, e.g., that the participating parents’ interactive skills were improved, and that they spent more time with the children. Häggman-Laitila et al. [45] reported, e.g., that the participating parents’ need for support regarding upbringing and childcare decreased from 70% to 30%, and that 93% of the parents who were hoping that the intervention would strengthen parenthood, and 67% of those who wanted the intervention to develop their skills in raising and caring for their children, achieved these goals. Additionally, another study [48], reported that almost all participants (96%) reported increased interaction within the family.
As the first systematic review of early childhood interventions in the Nordic countries, the goal was to gather, describe and evaluate the interventions developed for promoting mental health and parenting among families with young children in the region. Previous intervention research from the Nordic countries has mainly evaluated selected (e.g., [36,60,61]), and indicated activities targeting identified risk groups (e.g., [62–65]), but our intention was to focus on health-promoting interventions on a universal level. After a comprehensive screening procedure, the intervention studies meeting the eligibility criteria were nevertheless categorized as interventions with a universal health-promoting approach or interventions with a health-promoting approach with elements of prevention. Theoretically, while there is a distinction between universal, selective, and indicated initiatives, the differentiation in practice is naturally more fluid.
Interestingly, no Danish or Icelandic studies were identified that met the inclusion criteria of this review study. Previous studies (e.g., [66]) have identified different approaches to health-promoting initiatives in the five Nordic countries and have found that the universal health-promoting focus is least prominent in the Danish and Icelandic contexts. Further, other researchers have highlighted that the welfare systems and public health programs do vary between the Nordic countries (e.g., [67]), and the fact that this review study did not identify any Danish or Icelandic studies may reflect these variations with regard to early childhood interventions. When discussing the Nordic welfare model, it is relevant to note the importance of the sociodemographic position of families and how this may affect family mental health and well-being and related prerequisites. Several of the included studies looked at sociodemographic factors, such as parents’ level of education and employment status, and highlighted the need to take these into consideration in both intervention delivery and the interpretation of intervention effects. While it was not the aim of this review study to analyze how these factors might impact the effect of the interventions, we acknowledge the increasing importance of socioeconomic status in relation to health and well-being also in the Nordic countries and the need to consider these in future family-focused research.
When analyzing the key results of the included studies, three main outcome categories were identified in the studies applying statistical methods. The outcomes were divided into effects related to the parents, children, or parent-child interaction. The qualitative studies deepened the understanding of participants’ experiences’, which may reflect the mechanisms involved in the findings that emerged in the studies applying statistical methods. As presented in the results, almost all of the studies reporting on parents’ self-efficacy and/or self-esteem and parents’ satisfaction found a significant increase as a result of the interventions. This is in line with previous international systematic reviews evaluating parenting programs, which have found similar improvements in parental self-efficacy (e.g., [26]) and confidence (e.g., [29]).
On the other hand, most of the quantitative studies that reported on parents’ social support and the parental relationship did not find any significant changes after the interventions. Here the findings between the quantitative and qualitative studies differed, as qualitative studies reported on the participants’ experienced improvements in social support and parental relationships. Significant statistical improvements in satisfaction with the relationship with one’s partner have, however, been found in a previous systematic review by Bennett et al. [29]. Interestingly, in another review study, Bennett et al. [30] found that the majority of the included literature related to parenting programs does not consider the development of social connections as an important outcome, concluding that social connectivity should be valued as a primary goal of any parenting program.
There were challenges in analyzing the gathered evidence on interventions focusing on positive mental health and well-being outcomes among parents. Unlike the number of validated scales for measuring mental health problems, there are relatively few scales that are designed to measure mental health [8]. The WHO defines mental health as more than the absence of symptoms of mental health problems [68]. Therefore, the appropriateness of making conclusions about mental health by assessing mental health problems (such as anxiety, depression, and stress) can be questioned. Despite the definition and the questioned appropriateness, a common approach when statistically studying mental health is to investigate the absence of or decrease in mental health problems. A majority of the quantitative studies included in this systematic review found a significant decrease in parents’ mental health problems and stress. Previous review studies have reported varying results in relation to parental mental health problems. For example, Bennett et al. [29] reported a significant decrease in parental depression, anxiety, stress, anger, and guilt, while Jeong et al. [33] did not find any significant reductions in depressive symptoms. To investigate the subjective nature of positive mental health and well-being, qualitative methods may be better suited. Three of the qualitative studies in this review concluded that parents experience the interventions as positively impacting their health and well-being.
Most of the quantitative studies that examined children’s mental health and/or development found significant improvements, and all four studies that examined children’s strengths and difficulties found some significant changes that indicate a positive development. Positive results reflecting these findings also emerged in two of the qualitative studies. When it comes to children’s mental health and development, previous review studies have come to different conclusions. For instance, Barlow et al. [27] and Jeong et al. [33] found significant improvement in children’s socioemotional development while Pontoppidan et al. [69] found no statistically significant effects on child development. Notably, none of the studies included in this review found significant changes in existing behavioral problems, while Jeong et al. [33] have found significant reductions in child behavior problems.
Almost all of the studies that examined parenting strategies and/or parent-child interaction found significant positive changes after the interventions. This favorable development also emerged in four qualitative studies. With regard to these outcomes, previous research has come to different conclusions, e.g., Filene et al. [32] and Jeong et al. [33] found improved parenting knowledge, skills, practices, and parent-child interaction, while Pontoppidan et al. [69] found no statistically significant effects on parent-child relationships.
A strength of our review study is the mixed-method design, i.e., the inclusion of intervention studies applying quantitative or qualitative methods. Even if the results of studies applying qualitative methods are not generalizable, they can increase the understanding of the subjective experiences of mental health, family dynamics, and the perceived benefits of the interventions.
The included studies reported several limitations, including, e.g., participants being self-selected, small sample size, lack of control group, no randomization, self-report data, and lack of follow-up period. The overall quality of the included studies varied, and mainly due to the reported limitations most of the studies were rated with a moderate quality score. The variation in follow-up periods (and the fact that some studies merely reported pre- and post-intervention measurements), a wide range of measuring instruments, and different intervention content made the studies difficult to compare and prevented data pooling, meaning that a statistical meta-analysis was not possible.
There are some limitations to this review study as well. The first limitation concerns the screening and selection process. Even if we searched a relatively large number of databases and applied broad search terms, there is always a risk of missing relevant Nordic studies. Some interventions targeted at a specific risk group were included, e.g., families with children with behavioral problems, while others risk groups, e.g., families where domestic violence may have occurred, were excluded.
Another limitation to be discussed is our attempt to make a distinction between interventions with a universal health-promoting approach and a health-promoting approach with preventive elements. Although the results were separated according to interventions in these two categories, there was no clear overarching difference in the outcomes between the two types of interventions. Selective and indicated interventions may not always be adaptable on a universal level for the general public, since the initiatives are developed for certain risk or high-risk groups [26,70].
4.2 Implications for Research and Practice
This review shows that early childhood interventions encompassing various forms of parenting support can have positive effects on mental health and well-being and related outcomes among both parents and children and thus should be considered a feasible health-promoting activity. However, more studies covering the effects of existing intervention programs and longer follow-up periods evaluating the long-term effects of the specific interventions would strengthen the evidence base. When it comes to complex phenomena such as mental health, parenting strategies, and family dynamics, it might not be purposeful to attempt to identify a one-size-fits-all model early childhood intervention, rather the interventions need to be flexible and adapted to the participants’ individual situations and needs. The implementation and realization of an intervention is a compound of several interacting components. Health-promoting interventions are characterized by a participatory approach, and previous research highlights that actively engaged parents are of great importance for the effect of the intervention [71]. In addition to participant attitudes, the practitioners and group leaders influence the implementation success and intervention sustainability [64].
As previous systematic reviews (e.g., [26–27,29,33]) of the international evidence have shown, this Nordic study also found that early childhood interventions improve the short-term mental health of both parents and children, but the long-term effectiveness of the interventions need to be further investigated preferably through longitudinal prospective studies.
In conclusion, this Nordic systematic review of quantitative and qualitative evidence highlights that early childhood interventions seem to be promising, the limited number of studies synthesized showed various positive effects on mental health and well-being of both children and their parents. The fact that different types of initiatives have been developed and implemented can be seen as an advantage, considering the varying needs and expectations of different families.
Acknowledgement: The authors thank Ronja Hagberg for her assistance in screening and coding publications in the initial stage of the systematic review study process.
Funding Statement: The study was funded by Högskolestiftelsen i Österbotten and Svensk-Österbottniska samfundet. These funding bodies had no role in the design of the study, the collection, analysis, and interpretation of data, or the composition of the manuscript.
Conflicts of Interest: The authors declare that they have no conflicts of interest to report regarding the present study.
References
*) Studies included in the systematic review are marked with an asterisk sign
1. Nordic Council of Ministers (2018). In the shadow of happiness (Analysis no. 01/2018). http://norden.diva-portal.org/smash/get/diva2:1236906/FULLTEXT02.pdf. [Google Scholar]
2. Helliwell, J. F., Layard, R., Sachs, J. D., de Neve, J. E., Aknin, L. B. et al. (2021). World Happiness Report. https://happiness-report.s3.amazonaws.com/2021/WHR + 21.pdf. [Google Scholar]
3. Organisation for Economic Co-Operation and Development (OECD) (2017). How’s life? 2017: Measuring well-being. Paris: OECD Publishing. DOI 10.1787/how_life-2017-en. [Google Scholar] [CrossRef]
4. Organisation for Economic Co-Operation and Development (OECD) (2020). How’s life? 2020: Measuring well-being. Paris: OECD Publishing. DOI 10.1787/9870c393-en. [Google Scholar] [CrossRef]
5. Esping-Andersen, G. (1990). The three worlds of welfare capitalism. Princeton, New Jersey: Princeton University Press. [Google Scholar]
6. Vihriälä, V., Valkonen, T.(2014). The nordic model-challenged but capable of reform. Copenhagen: Nordic council of ministers. http://norden.diva-portal.org/smash/get/diva2:715939/FULLTEXT02.pdf. [Google Scholar]
7. World Health Organization (WHO) (2018). Adolescent mental health in the European Region. https://www.euro.who.int/__data/assets/pdf_file/0005/383891/adolescent-mh-fs-eng.pdf. [Google Scholar]
8. Barry, M. M., Clarke, A. M., Petersen, I., Jenkins, R. (2019). Implementing mental health promotion. 2nd edition. Cham: Springer International Publishing. [Google Scholar]
9. World Health Organization (WHO) (2004). Prevention of mental disorders: Effective interventions and policy options: Summary report. http://www.mentalhealthpromotion.net/resources/prevention_of_mental_disorders_bluebooklet.pdf. [Google Scholar]
10. Mrazek, P. J., Haggerty, R. J. (Eds.). (1994). Reducing risks for mental disorders: Frontiers for preventive intervention research. Washington DC: National Academy Press. [Google Scholar]
11. Center on the Developing Child at Harvard University (2010). The foundations of lifelong health are built in early childhood. https://developingchild.harvard.edu/wp-content/uploads/2010/05/Foundations-of-Lifelong-Health.pdf. [Google Scholar]
12. Center on the Developing Child at Harvard University (2016). From best practices to breakthrough impacts: A science-based approach to building a more promising future for young children and families. https://developingchild.harvard.edu/wp-content/uploads/2016/05/From_Best_Practices_to_Breakthrough_Impacts-4.pdf. [Google Scholar]
13. Bronfenbrenner, U. (1979). Contexts of child rearing: Problems and prospects. American Psychologist, 34(10), 844–850. DOI 10.1037/0003-066X.34.10.844. [Google Scholar] [CrossRef]
14. Lamb, M. E., Lerner, R. M. (2015). Handbook of child psychology and developmental science: Socioemotional processes, vol. 3, 7th edition. Hoboken, NJ: John Wiley & Sons Inc. [Google Scholar]
15. Rutter, M. E. (1988). Studies of psychosocial risk: The power of longitudinal data. New York: Cambridge University Press. [Google Scholar]
16. Morgan, Z., Brugha, T., Fryers, T., Stewart-Brown, S. (2012). The effects of parent-child relationships on later life mental health status in two national birth cohorts. Social Psychiatry and Psychiatric Epidemiology, 47(11), 1707–1715. DOI 10.1007/s00127-012-0481-1. [Google Scholar] [CrossRef]
17. Stewart-Brown, S. (2008). Improving parenting: The why and the how. Archives of Disease in Childhood, 93(2), 102–104. DOI 10.1136/adc.2006.113522. [Google Scholar] [CrossRef]
18. Stewart-Brown, S. L., Schrader-Mcmillan, A. (2011). Parenting for mental health: What does the evidence say we need to do? Report of Workpackage 2 of the DataPrev project. Health Promotion International, 26(suppl_1), i10–i28. DOI 10.1093/heapro/dar056. [Google Scholar] [CrossRef]
19. Mistry, K. B., Minkovitz, C. S., Riley, A. W., Johnson, S. B., Grason, H. A. et al. (2012). A new framework for childhood health promotion: The role of policies and programs in building capacity and foundations of early childhood health. American Journal of Public Health, 102(9), 1688–1696. DOI 10.2105/AJPH.2012.300687. [Google Scholar] [CrossRef]
20. Britto, P. R., Lye, S. J., Proulx, K., Yousafzai, A. K., Matthews, S. G. et al. (2017). Nurturing care: Promoting early childhood development. The Lancet, 389(10064), 91–102. DOI 10.1016/S0140-6736(16)31390-3. [Google Scholar] [CrossRef]
21. Clarke, A. M. (2019). Promoting the mental health of children and families in the early years. In Barry, M., Clarke, A., Petersen, I., Jenkins R. (Eds.). Implementing mental health promotion. Cham: Springer. DOI 10.1007/978-3-030-23455-3_8. [Google Scholar] [CrossRef]
22. Clarke, A. M. (2019). Implementing parenting and preschool programmes. In: Barry, M., Clarke, A., Petersen, I., Jenkins, R. (Eds.). Implementing mental health promotion. Cham: Springer. DOI 10.1007/978-3-030-23455-3_9. [Google Scholar] [CrossRef]
23. Karoly, L. A., Kilburn, M. R., Cannon, J. S. (2005). Early childhood interventions: Proven results, future promise. Santa Monica: Rand Corporation. [Google Scholar]
24. Jeong, J., Franchette, E., Yousafzai, A. (2020). World Health Organization recommendations on caregiving interventions to support early child development in the first three years of life: Report on the systematic review of evidence. https://cdn.who.int/media/docs/default-source/mca-documents/child/ecd/sr_caregivin_interventions__ecd___jeong___final____05mar2020___rev.pdf?sfvrsn=5d74c5ac_7. [Google Scholar]
25. World Health Organization (WHO) (2020). Improving early childhood development: WHO guideline. Geneva: World Health Organization. https://apps.who.int/iris/bitstream/handle/10665/331306/9789240002098-eng.pdf. [Google Scholar]
26. Amin, N. A. L., Tam, W. W., Shorey, S. (2018). Enhancing first-time parents’ self-efficacy: A systematic review and meta-analysis of universal parent education interventions’ efficacy. International Journal of Nursing Studies, 82, 149–162. DOI 10.1016/j.ijnurstu.2018.03.021. [Google Scholar] [CrossRef]
27. Barlow, J., Bergman, H., Kornør, H., Wei, Y., Bennett, C. (2016). Group-based parent training programmes for improving emotional and behavioural adjustment in young children. Cochrane Database of Systematic Reviews, 2016(8). DOI 10.1002/14651858.CD003680.pub3. [Google Scholar] [CrossRef]
28. Barlow, J., Schrader-McMillan, A., Axford, N., Wrigley, Z., Sonthalia, S. et al. (2016). Attachment and attachment-related outcomes in preschool children–A review of recent evidence. Child and Adolescent Mental Health, 21(1), 11–20. DOI 10.1111/camh.12138. [Google Scholar] [CrossRef]
29. Bennett, C., Barlow, J., Huband, N., Smailagic, N., Roloff, V. (2013). Group-based parenting programs for improving parenting and psychosocial functioning: A systematic review. Journal of the Society for Social Work and Research, 4(4), 300–332. DOI 10.5243/jsswr.2013.20. [Google Scholar] [CrossRef]
30. Bennett, C. T., Buchan, J. L., Letourneau, N., Shanker, S. G., Fenwick, A. et al. (2017). A realist synthesis of social connectivity interventions during transition to parenthood: The value of relationships. Applied Nursing Research, 34, 12–23. DOI 10.1016/j.apnr.2016.11.004. [Google Scholar] [CrossRef]
31. Branco, M. S. S., Altafim, E. R. P., Linhares, M. B. M. (2021). Universal intervention to strengthen parenting and prevent child maltreatment: Updated systematic review. Trauma, Violence, & Abuse, 23(5). DOI 10.1177/15248380211013131. [Google Scholar] [CrossRef]
32. Filene, J. H., Kaminski, J. W., Valle, L. A., Cachat, P. (2013). Components associated with home visiting program outcomes: A meta-analysis. Pediatrics, 132(Supplement 2), S100–S109. DOI 10.1542/peds.2013-1021H. [Google Scholar] [CrossRef]
33. Jeong, J., Franchett, E. E., Ramos de Oliveira, C. V., Rehmani, K., Yousafzai, A. K. (2021). Parenting interventions to promote early child development in the first three years of life: A global systematic review and meta-analysis. PLoS Medicine, 18(5), e1003602. DOI 10.1371/journal.pmed.1003602. [Google Scholar] [CrossRef]
34. Morrison, J., Pikhart, H., Ruiz, M., Goldblatt, P. (2014). Systematic review of parenting interventions in European countries aiming to reduce social inequalities in children’s health and development. BMC Public Health, 14(1), 1–13. DOI 10.1186/1471-2458-14-1040. [Google Scholar] [CrossRef]
35. Munns, A., Watts, R., Hegney, D., Walker, R. (2016). Effectiveness and experiences of families and support workers participating in peer-led parenting support programs delivered as home visiting programs: A comprehensive systematic review. JBI Evidence Synthesis, 14(10), 167–208. DOI 10.11124/JBISRIR-2016-003166. [Google Scholar] [CrossRef]
36. Bergström, M., Gebreslassie, M., Hedqvist, M., Lindberg, L., Sarkadi, A. et al. (2020). Narrative review of interventions suitable for well-baby clinics to promote infant attachment security and parents’ sensitivity. Acta Paediatrica, 109(9), 1745–1757. DOI 10.1111/apa.15212. [Google Scholar] [CrossRef]
37. Moher, D., Liberati, A., Tetzlaff, J., Altman, D. G., Group, P. (2009). Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Medicine, 6(7), e1000097. DOI 10.1371/journal.pmed.1000097. [Google Scholar] [CrossRef]
38. *Davis, H., Dusoir, T., Papadopoulou, K., Dimitrakaki, C., Cox, A. et al. (2005). Child and family outcomes of the European Early Promotion Project. International Journal of Mental Health Promotion, 7(1), 63–81. DOI 10.1080/14623730.2005.9721951. [Google Scholar] [CrossRef]
39. *Lindberg, L., Ulfsdotter, M., Jalling, C., Skärstrand, E., Lalouni, M. et al. (2013). The effects and costs of the universal parent group program–all children in focus: A study protocol for a randomized wait-list controlled trial. BMC Public Health, 13(1), 1–12. DOI 10.1186/1471-2458-13-688. [Google Scholar] [CrossRef]
40. *Puura, K., Davis, H., Cox, A., Tsiantis, J., Tamminen, T. et al. (2005). The European Early Promotion Project: Description of the service and evaluation study. International Journal of Mental Health Promotion, 7(1), 17–31. DOI 10.1080/14623730.2005.9721947. [Google Scholar] [CrossRef]
41. *Salonen, A. H., Kaunonen, M., Åstedt-Kurki, P., Järvenpää, A. L., Tarkka, M. T. (2008). Development of an internet-based intervention for parents of infants. Journal of Advanced Nursing, 64(1), 60–72. DOI 10.1111/j.1365-2648.2008.04759.x. [Google Scholar] [CrossRef]
42. *Mekhail, K. T., Lindberg, L., Burström, B., Marttila, A. (2019). Strengthening resilience through an extended postnatal home visiting program in a multicultural suburb in Sweden: Fathers striving for stability. BMC Public Health, 19(1), 1–12. DOI 10.1186/s12889-019-6440-y. [Google Scholar] [CrossRef]
43. *Häggman-Laitila, A., Pietilä, A. M., Friis, L., Vehviläinen-Julkunen, K. (2003). Video home training as a method of supporting family life control. Journal of Clinical Nursing, 12(1), 93–106. DOI 10.1046/j.1365-2702.2003.00696.x. [Google Scholar] [CrossRef]
44. *Häggman-Laitila, A., Seppänen, R., Vehviläinen-Julkunen, K., Pietilä, A. M. (2010). Benefits of video home training on families’ health and interaction: Evaluation based on follow-up visits. Journal of Clinical Nursing, 19(23–24), 3504–3515. DOI 10.1111/j.1365-2702.2010.03241.x. [Google Scholar] [CrossRef]
45. *Häggman-Laitila, A., Tanninen, H. M., Pietilä, A. M. (2010). Effectiveness of resource-enhancing family-oriented intervention. Journal of Clinical Nursing, 19(17–18), 2500–2510. DOI 10.1111/j.1365-2702.2010.03288.x. [Google Scholar] [CrossRef]
46. *Neander, K., Engstrom, I. (2009). Parents’ assessment of parent-child interaction interventions – A longitudinal study in 101 families. Child and Adolescent Psychiatry and Mental Health, 3(8). DOI 10.1186/1753-2000-3-8. [Google Scholar] [CrossRef]
47. *Puura, K., Davis, H., Mäntymaa, M., Tamminen, T., Roberts, R. et al. (2005). The outcome of the European Early Promotion Project: Mother-child interaction. International Journal of Mental Health Promotion, 7(1), 82–94. DOI 10.1080/14623730.2005.9721952. [Google Scholar] [CrossRef]
48. *Tanninen, H. M., Häggman-Laitila, A., Kangasniemi, M., Pietilä, A. M. (2014). How resource-enhancing family nursing is realized by Finnish parents? An intervention study. International Journal of Caring Sciences, 7(2), 520–529. [Google Scholar]
49. *Clucas, C., Skar, A. M. S., Sherr, L., Tetzchner, S. V. (2014). Mothers and fathers attending the international child development programme in Norway. The Family Journal, 22(4), 409–418. DOI 10.1177/1066480714533640. [Google Scholar] [CrossRef]
50. *Enebrink, P., Danneman, M., Mattsson, V. B., Ulfsdotter, M., Jalling, C. et al. (2015). ABC for parents: Pilot study of a universal 4-session program shows increased parenting skills, self-efficacy and child well-being. Journal of Child and Family Studies, 24(7), 1917–1931. DOI 10.1007/s10826-014-9992-6. [Google Scholar] [CrossRef]
51. *Häggman-Laitila, A., Pietilä, A. M. (2007). Perceived benefits on family health of small groups for families with children. Public Health Nursing, 24(3), 205–216. DOI 10.1111/j.1525-1446.2007.00627.x. [Google Scholar] [CrossRef]
52. *Reedtz, C., Handegård, B. H., Mørch, W. T. (2011). Promoting positive parenting practices in primary pare: Outcomes and mechanisms of change in a randomized controlled risk reduction trial. Scandinavian Journal of Psychology, 52(2), 131–137. DOI 10.1111/j.1467-9450.2010.00854.x. [Google Scholar] [CrossRef]
53. *Sherr, L., Skar, A. M. S., Clucas, C., Tetzchner, S. V., Hundeide, K. (2014). Evaluation of the International Child Development Programme (ICDP) as a community-wide parenting programme. European Journal of Developmental Psychology, 11(1), 1–17. DOI 10.1080/17405629.2013.793597. [Google Scholar] [CrossRef]
54. *Thorell, L. B. (2009). The Community Parent Education Program (COPETreatment effects in a clinical and a community-based sample. Clinical Child Psychology and Psychiatry, 14(3), 373–387. DOI 10.1177/1359104509104047. [Google Scholar] [CrossRef]
55. *Ulfsdotter, M., Enebrink, P., Lindberg, L. (2014). Effectiveness of a universal health-promoting parenting program: A randomized waitlist-controlled trial of all children in focus. BMC Public Health, 14(1), 1–11. DOI 10.1186/1471-2458-14-1083. [Google Scholar] [CrossRef]
56. *Sampaio, F., Sarkadi, A., Salari, R., Zethraeus, N., Feldman, I. (2015). Cost and effects of a universal parenting programme delivered to parents of preschoolers. The European Journal of Public Health, 25(6), 1035–1042. DOI 10.1093/eurpub/ckv106. [Google Scholar] [CrossRef]
57. *Salonen, A. H., Kaunonen, M., Åstedt-Kurki, P., Järvenpää, A. L., Isoaho, H. et al. (2011). Effectiveness of an internet-based intervention enhancing Finnish parents’ parenting satisfaction and parenting self-efficacy during the postpartum period. Midwifery, 27(6), 832–841. DOI 10.1016/j.midw.2010.08.010. [Google Scholar] [CrossRef]
58. National Institute for Health and Care Excellence (2012). Methods for the Development of NICE Public Health Guidance. Appendix F Quality Appraisal Checklist–Quantitative Intervention Studies. Third editionhttps://www.nice.org.uk/process/pmg4/chapter/appendix-f-quality-appraisal-checklist-quantitative-intervention-studies. [Google Scholar]
59. National Institute for Health and Care Excellence (2012). Methods for the Development of NICE Public Health Guidance. Appendix F Quality Appraisal Checklist–Qualitative Studies. Third editionhttps://www.nice.org.uk/process/pmg4/chapter/appendix-h-quality-appraisal-checklist-qualitative-studies#ftn.footnote_17. [Google Scholar]
60. Barboza, M., Kulane, A., Burström, B., Marttila, A. (2018). A better start for health equity? Qualitative content analysis of implementation of extended postnatal home visiting in a disadvantaged area in Sweden. International Journal for Equity in Health, 17(1), 1–9. DOI 10.1186/s12939-018-0756-6. [Google Scholar] [CrossRef]
61. Landsem, I. P., Handegård, B. H., Tunby, J., Ulvund, S. E., Rønning, J. A. (2014). Early intervention program reduces stress in parents of preterms during childhood, a randomized controlled trial. Trials, 15(1), 1–13. DOI 10.1186/1745-6215-15-387. [Google Scholar] [CrossRef]
62. Axberg, U., Hansson, K., Broberg, A. G. (2007). Evaluation of the Incredible Years Series–An open study of its effects when first introduced in Sweden. Nordic Journal of Psychiatry, 61(2), 143–151. DOI 10.1080/08039480701226120. [Google Scholar] [CrossRef]
63. Karjalainen, P., Kiviruusu, O., Aronen, E. T., Santalahti, P. (2019). Group-based parenting program to improve parenting and children’s behavioral problems in families using special services: A randomized controlled trial in a real-life setting. Children and Youth Services Review, 96, 420–429. DOI 10.1016/j.childyouth.2018.12.004. [Google Scholar] [CrossRef]
64. Olofsson, V., Skoog, T., Tillfors, M. (2016). Implementing group based parenting programs: A narrative review. Children and Youth Services Review, 69, 67–81. DOI 10.1016/j.childyouth.2016.07.004. [Google Scholar] [CrossRef]
65. Sigmarsdóttir, M., Forgatch, M. S., Guðmundsdóttir, E. V., Thorlacius, Ö., Svendsen, G. T. et al. (2019). Implementing an evidence-based intervention for children in Europe: Evaluating the full-transfer approach. Journal of Clinical Child & Adolescent Psychology, 48(sup1), S312–S325. DOI 10.1080/15374416.2018.1466305. [Google Scholar] [CrossRef]
66. Raphael, D. (2014). Challenges to promoting health in the modern welfare state: The case of the Nordic nations. Scandinavian Journal of Public Health, 42(1), 7–17. DOI 10.1177/1403494813506522. [Google Scholar] [CrossRef]
67. Vallgårda, S. (2011). Addressing individual behaviours and living conditions: Four Nordic public health policies. Scandinavian Journal of Public Health, 39(6_suppl), 6–10. DOI 10.1177/1403494810378922. [Google Scholar] [CrossRef]
68. World Health Organization (WHO) (2002). Prevention and promotion in mental health. https://apps.who.int/iris/bitstream/handle/10665/42539/9241562161.pdf. [Google Scholar]
69. Pontoppidan, M., Klest, S. K., Patras, J., Rayce, S. B. (2016). Effects of universally offered parenting interventions for parents with infants: A systematic review. BMJ Open, 6(9), e011706. DOI 10.1136/bmjopen-2016-011706. [Google Scholar] [CrossRef]
70. Furlong, M., McGilloway, S., Bywater, T., Hutchings, J., Smith, S. M. et al. (2013). Cochrane review: Behavioural and cognitive-behavioural group-based parenting programmes for early-onset conduct problems in children aged 3 to 12 years. Evidence-Based Child Health: A Cochrane Review Journal, 8(2), 318–692. DOI 10.1002/ebch.1905. [Google Scholar] [CrossRef]
71. Giannotta, F., Özdemir, M., Stattin, H. (2019). The implementation integrity of parenting programs: Which aspects are most important? Child & Youth Care Forum, 48(6), 917–933. DOI 10.1007/s10566-019-09514-8. [Google Scholar] [CrossRef]

Cite This Article
 Copyright © 2023 The Author(s). Published by Tech Science Press.
Copyright © 2023 The Author(s). Published by Tech Science Press.This work is licensed under a Creative Commons Attribution 4.0 International License , which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
 Downloads
Downloads
 Citation Tools
Citation Tools