
 Submit a Paper
Submit a Paper Propose a Special lssue
Propose a Special lssue Open Access
Open Access
REVIEW

Effectiveness of manual detorsion in the treatment of testicular torsion: systematic review and meta-analysis
Department of Pediatric Surgery, Faculty of Medicine, Okan University, Istanbul, 34959, Turkiye
* Corresponding Authors: Sinan Kılıç. Email: ,
Canadian Journal of Urology 2026, 33(3), 505-514. https://doi.org/10.32604/cju.2025.072049
Received 18 August 2025; Accepted 16 December 2025; Issue published 29 June 2026
 View Full Text
View Full Text Download PDF
Download PDFAbstract
Objectives: Testicular torsion is the most common surgical cause of an acute scrotum. Manuel detorsion renewed attention as a practical initial treatment, particularly in the COVID-19 pandemic. This study aims to systematically review and meta-analyze the current literature to determine whether manual detorsion offers a viable alternative to immediate surgery in improving testicular salvage rates. Methods: A systematic review and meta-analysis were conducted in accordance with PRISMA guidelines and registered with PROSPERO (CRD420251039489). Studies including ≥30 male patients comparing manual detorsion and surgical exploration were included. Searches were performed in PubMed/MEDLINE, Scopus, TR Index, and Web of Science. Risk of bias was assessed using a predefined scoring system based on methodology, sample size, and follow-up objectivity. Data were synthesized using RevMan 5.4 to calculate pooled risk ratios. Results: Eight retrospective studies involving a total of 670 patients were included. Patients were divided into a manual detorsion group (G1, n = 394) and a surgical exploration group (G2, n = 316). Success rates of manual detorsion ranged from 15% to 76%, while orchiectomy rates were lower in G1 (0% to 10.3%) compared to G2 (0% to 43.8%). The pooled success rate of manual detorsion was 75.7%. Although orchiectomy rates appeared numerically lower in the manual detorsion group (3.8% vs. 29.2%), the pooled analysis did not demonstrate a statistically significant overall difference between the two groups (risk ratio [RR] = 1.23; 95% CI: 0.82–1.84; p = 0.31). Conclusion: Manual detorsion appears time-saving and effective maneuver. To our knowledge, this is the first meta-analysis focused exclusively on manual detorsion, and it supports its consideration as an initial management strategy in selected clinical scenarios.Graphic Abstract
Keywords
Supplementary Material
Supplementary Material FileTesticular torsion (TT) results from twisting of the spermatic cord, leading to interruption of blood flow and subsequent ischemia. It represents a urological emergency with an annual incidence of up to 4.5 cases per 100,000.1 TT accounts for approximately 17%–35% of acute scrotum cases and demonstrates a bimodal age distribution, with peak incidences in the neonatal period and adolescence. The most common age at diagnosis is 13 to 14 years, corresponding to the peripubertal period.2,3 When a patient presents with symptoms of acute scrotum, the foremost clinical priority is to promptly exclude testicular torsion, and Color Doppler ultrasonography plays a central role in this diagnostic process.
When a patient presents with symptoms of acute scrotum, the foremost clinical priority is to promptly exclude testicular torsion. While Color Doppler ultrasonography plays a central role in confirming the diagnosis, TT remains primarily a clinical diagnosis in many cases, and patients with high TWIST scores often proceed directly to surgical exploration without ultrasonic verification. In addition, power Doppler ultrasonography is more sensitive than conventional color Doppler in detecting testicular perfusion and may further aid in diagnosis.4
Color Doppler ultrasonography enhances the diagnostic accuracy in suspected torsion cases.5 Before its widespread clinical use, a suspected acute scrotum often necessitated surgical exploration. Despite improved diagnostic modalities, delays in intervention may still occur and may exceed the critical ischemic window.6 To address this, manual detorsion has gained attention as a rapid, non-invasive treatment alternative. Manual detorsion was first introduced by Nash as a clinically based blind procedure. Following the widespread use of ultrasonography, it has become the preferred initial approach in selected centers due to its ease of application.7
However, disappointing testicular salvage rates persist in the literature and are closely associated with delayed treatment and the extent of cord twisting.8 Manual detorsion functions as a temporizing measure aimed at minimizing ischemic injury. Although it may not fully resolve torsion, partial reversal of cord twisting can restore perfusion to some extent. Studies have suggested a correlation between the number of rotations and the severity of ischemic damage. While much of the current evidence is limited to case reports and small observational series, manual detorsion appears to hold therapeutic potential in select cases.9,10
Manual detorsion can be easily attempted without anesthesia in suitable patients. It involves gently rotating the testicle outward, much like opening a book, while checking for pain relief and ensuring that there is no resistance or worsening of symptoms. Successful detorsion is suggested by rapid clinical improvement and normalization of examination findings. Doppler ultrasonography should be used to confirm both the diagnosis and the effectiveness of the procedure.11 In the event of failure, emergency surgical exploration becomes mandatory. Published success rates for manual detorsion vary between 61.5% and 91%. Manual detorsion is increasingly considered as a rapid, interim management strategy for TT. Despite the growing body of literature on the subject, no comprehensive meta-analysis or systematic review evaluating the efficacy of this approach has been published to date. Hence, the present study aims to conduct a meta-analysis to assess the effectiveness of manual detorsion and to evaluate its clinical implications more broadly.
This systematic review and meta-analysis strictly adhered to the rigorous standards set forth by the PRISMA (2020 current version) statement (Supplementary Material S1)12 and SEDATE guidelines.13 All procedures, encompassing inclusion/exclusion criteria, data extraction, and quality assessment, were meticulously defined a priori and outlined in detail in Figure 1. The research methodology was meticulously registered in PROSPERO (CRD420251039489) before the commencement of the study, with no subsequent alterations post-registration. Institutional review board approval was intentionally waived, given the distinctive nature and design of the study.

FIGURE 1. Study the algorithm and flowchart
A comprehensive and systematic search was conducted across four major electronic databases (PubMed/MEDLINE, Scopus, TR Index, and Web of Science) to identify potentially eligible studies published between January 2000 and March 2025. The search strategy utilized specific keywords, including “torsion”, “detorsion”, “testicular torsion”, “manual detorsion”, and “Color Doppler”, to ensure a thorough exploration of the relevant literature. Duplicate documents retrieved from different databases were identified and excluded before screening, as also illustrated in the PRISMA flow diagram. The last search for all databases was completed on 31 March 2025. Strict inclusion criteria were applied, restricting the selection to articles published in English. This meticulous and multilateral search process was designed to capture a broad range of studies while maintaining adherence to the predefined language criterion.
The author systematically investigated identified articles by thoroughly scrutinizing titles and abstracts. Their primary objective was to eliminate irrelevant content, including duplicates, studies unrelated to the review’s topic, case reports, reviews, meta-analyses, and letters to the editor. Following this initial screening, the authors obtained the full texts of relevant articles and independently applied the specified inclusion criteria. These inclusion criteria mandated that eligible studies be either prospective or retrospective cohort or case-control studies, with a minimum of 30 male subjects included. Torsion confirmation was conducted through color Doppler ultrasound assessment for at least one of the following ultrasound signs: edema, the whirlpool sign, and Doppler assessment of testicular blood flow. Studies involving fetuses and/or neonates were explicitly excluded from consideration (Figure 1).
The author autonomously employed Microsoft Excel spreadsheets (Version 15.24) to extract data. For every study, pertinent information such as the overall sample size, distribution of subjects within each patient cohort, mean age at presentation, incidence of torsion per group, average symptom duration, prevalence of delayed presentation among children, frequency of manual detorsion procedures, and the rate of orchiectomy necessity among children were gathered. Furthermore, details regarding the primary author’s name, publication year, and study design classification were duly documented.14–21
Success was defined as restored testicular blood flow on Doppler ultrasound, resolution of pain, and avoidance of subsequent orchiectomy. This definition captures both immediate procedural outcomes and short-term testicular viability, ensuring a comprehensive assessment of manual detorsion effectiveness.
Methodological quality assessment
A scale for assessing study quality was developed, wherein study methodology, participant numbers, and objectivity of follow-up at 12 months were assigned scoring points as outlined in Table 1.

The initial dataset was presented using various metrics, including numerical values, proportions, and measures of central tendency, such as mean or median, alongside their respective ranges. Orchiectomy rates in the manual detorsion and surgical exploration groups were analyzed using the chi-square (χ2) test. Meta-analysis was conducted using RevMan 5.4 from the Cochrane Collaboration in London, UK. Risk ratios (RRs) with 95% confidence intervals (CIs) and mean differences with 95% CI were calculated for dichotomous and continuous outcomes, respectively, for each study. The pooled risk ratio and weighted mean difference were then determined using Mantel-Haenszel and inverse variance methods, respectively. Heterogeneity among the studies was assessed using I2 statistics, with a random-effects model chosen for substantial heterogeneity (I2 > 50%). Statistical significance was set at a p-value of <0.05.
Database screening identified a total of 87 articles. After the removal of 46 duplicates, 41 articles remained for eligibility assessment. Following abstract screening, 8 studies were selected to ensure homogeneity across groups (Figure 1). Three of the included studies were conducted in Turkey, while the others originated from Portugal, Italy, Greece, Brazil, and Spain. All studies used retrospective designs, with study durations ranging from 1 to 13 years. Sample sizes varied from 26 to 133 cases per study, and the total number of patients across all studies was 670. The included studies enrolled either both pediatric and adult patients or exclusively one age group14–21 (Table 1).
Patients were categorized into two groups: Group 1 (G1) comprised individuals who underwent manual detorsion, and Group 2 (G2) included those who received surgical exploration. Mean ages in both groups were similar, ranging between 11.5 and 24.7 years. A total of 394 patients underwent manual detorsion, while 316 patients received surgical exploration. Success rates for G1 ranged between 15% and 76%, whereas G2 showed rates between 9% and 64% (Table 2).

Meta-analysis using the Random Effects Model was conducted to assess the success rates in each group. Table 3 presents the success outcomes for manual detorsion and surgical exploration.

All eight studies reported orchiectomy rates following both interventions. In G1, orchiectomy rates ranged from 0% to 10.3%. In G2, rates ranged from 0% to 43.8%. In general, orchiectomy was more frequently required after surgical exploration compared to manual detorsion (Table 4).

Pooled success rates and comparisons were calculated using a Random Effects Model. High heterogeneity was noted across the studies (I2 = 95.2%). The pooled success rate was found to be 75.7%, with a 95% CI of 60.5% to 90.9%.
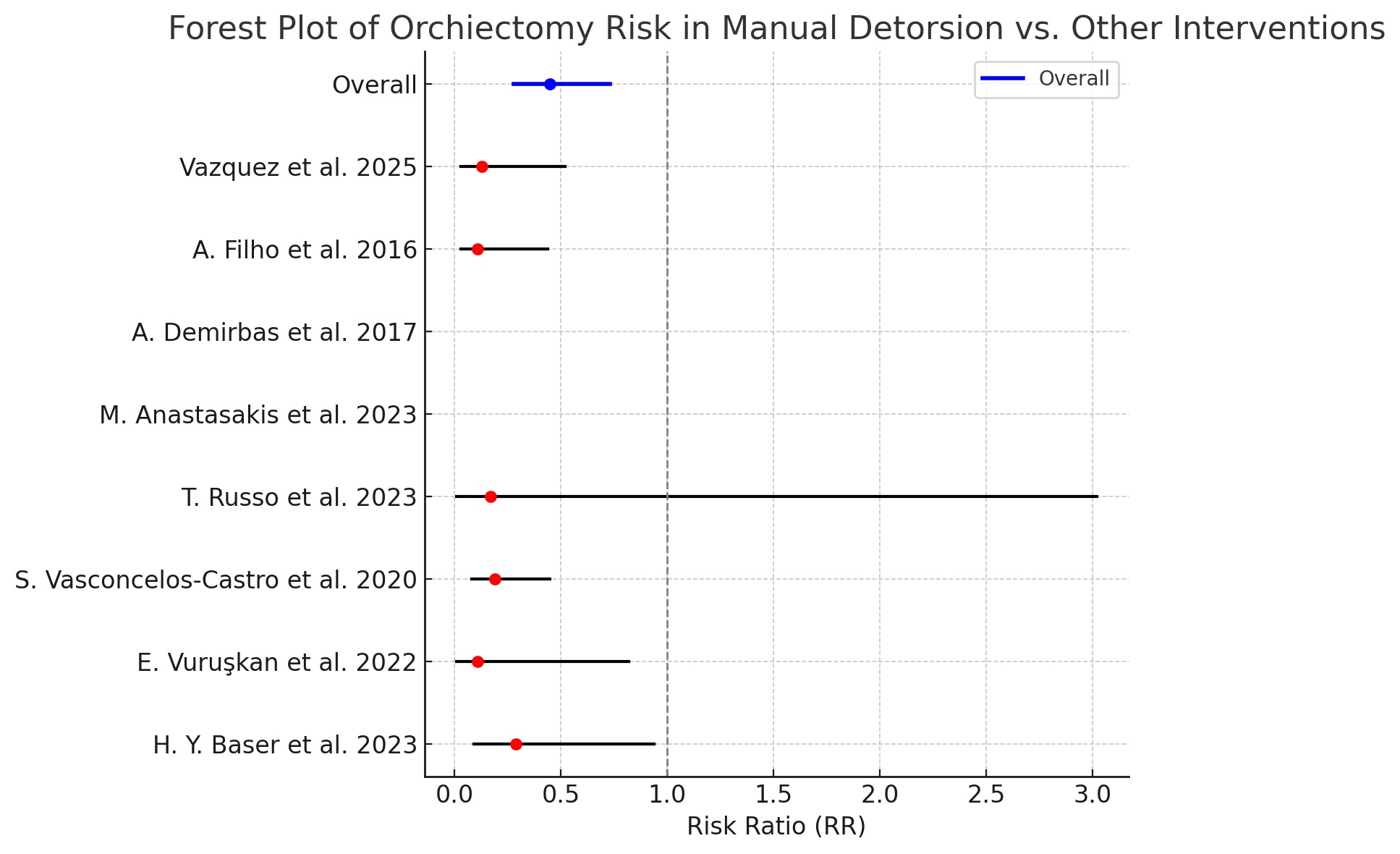
Although orchiectomy rates appeared numerically lower in the manual detorsion group (3.8% vs. 29.2%), the pooled analysis did not demonstrate a statistically significant overall difference between the two groups (risk ratio [RR] = 1.23; 95% CI: 0.82–1.84; p = 0.31).
Statistical heterogeneity remained significant (p = 0.01; I2 = 66%) (Tables 5 and 6, Figure 2).



FIGURE 2. Forest plot of orchiectomy risk in manual detorsion versus surgical exploration14–21
TT is the most common cause of acute scrotum and represents the primary condition requiring urgent intervention.1 Currently, TT can be diagnosed with almost 100% accuracy through physical examination and color Doppler ultrasonography.2,3 The typical age distribution of testicular torsion, a frequent cause of acute scrotum, follows a bimodal pattern, with peaks in the neonatal period and during adolescence.4,5
A direct relationship exists between the timing of intervention and the salvage rate of the testis in cases of torsion. A systematic review analyzing 30 studies and a total of 2166 cases demonstrated that surgical intervention within the first “golden” 6 h from symptom onset resulted in a 97.2% testicular salvage rate. In contrast, when torsion persisted for 24 to 48 h, testicular survival decreased to 24.4%.22
The conventional approach involves surgical exploration and detorsion via an inguinal or scrotal incision. Delays between diagnosis and operative intervention may prolong testicular ischemia and lead to testicular loss.23,24 During the COVID-19 pandemic, reduced access to hospitals led to an increase in cases managed with manual detorsion, highlighting the potential of this method as an effective alternative.25 Fixation is generally recommended in testicular torsion associated with undescended testes. However, in cases of spontaneous testicular torsion the necessity of fixation remains controversial. Contralateral fixation is especially debated in patients with anatomical abnormalities such as the bell clapper deformity.26,27
Manual detorsion is a simple, non-invasive technique used to preserve testicular viability in torsion cases. Historical studies investigating its effectiveness have reported widely variable success rates across different authors and periods. Early reports from the late 19th century through the 1990s describe high success rates, even in studies involving small patient groups. Collectively, these publications provide valuable insight into the early use and clinical impact of manual detorsion as a treatment for testicular torsion.28 This approach alone may not be sufficient to prevent recurrence or reduce the risk of torsion in the contralateral testis. Hosokawa reported that in a cohort of 27 patients undergoing successful manual detorsion without immediate orchiopexy, 11% experienced recurrence several months later, emphasizing the importance of timely orchiopexy following manual detorsion.29
In clinical practice, manual detorsion is often performed blindly, since the degree and direction of torsion are not always known. The immediate relief of scrotal pain and restoration of blood flow following the maneuver supports its effectiveness. Performing manual detorsion under ultrasonographic guidance may improve success rates in such “blind” procedures.21 Ultrasound guidance provides real-time visualization of testicular blood flow and the degree and direction of torsion, allowing clinicians to confirm successful detorsion immediately. Several studies have reported higher success rates when ultrasonography was used to guide the maneuver, particularly in cases where the degree or direction of torsion was uncertain. Therefore, incorporating ultrasound guidance may be considered a valuable adjunct, especially in settings where rapid and precise intervention is critical, enhancing both the safety and effectiveness of manual detorsion.21
This study aimed to compare the effectiveness and success rates of manual detorsion and surgical exploration, seeking to identify which method offers superior outcomes in the management of testicular torsion. The retrospective data analyzed in eight studies from diverse regions (Turkey, Portugal, Italy, Greece, Brazil, and Spain) allowed for a comparative assessment of both approaches. The concentration of studies in European countries may be viewed as a limitation.
Success rates varied across studies between the manual detorsion (G1) and surgical exploration (G2) groups. In G1, success ranged from 15% to 76%, while G2 showed rates between 9% and 64%. These findings suggest that manual detorsion may be more effective, particularly in cases where early intervention is possible. However, this method may not be ideal for all patients. Several studies noted reduced effectiveness of manual detorsion as the duration of torsion increased, suggesting a growing need for more invasive approaches such as surgical exploration.
Orchiectomy rates ranged from 0% to 10.3% in the manual detorsion group and from 0% to 43.8% in the surgical exploration group. This difference indicates that manual detorsion may better prevent testicular loss, while the invasive nature of exploration may contribute to higher orchiectomy rates. Timely manual detorsion appears to offer an important option for reducing testicular loss. Nonetheless, the relatively high orchiectomy rates observed in both groups suggest that factors beyond the procedure itself—such as timing of intervention and degree of torsion—also influence outcomes.
Although the meta-analysis revealed significantly lower orchiectomy rates in the manual detorsion group, the overall difference in orchiectomy requirement between the two groups did not reach statistical significance. This result suggests that both treatment approaches may offer similar effectiveness in preserving the testis. Given its minimally invasive and rapid nature, manual detorsion is generally more favorable.28 A possible explanation for the numerically lower orchiectomy rates observed in patients undergoing manual detorsion is that these cases do not always undergo direct surgical exploration. As a result, ischemic testicles may occasionally go unrecognized, potentially contributing to the lower reported orchiectomy rates. Although speculative, this observation highlights a limitation of relying solely on manual detorsion and underscores the importance of careful follow-up and assessment to ensure testicular viability.
Considerable heterogeneity was observed across the included studies (I2 = 95.2%), primarily due to differences in patient characteristics (e.g., age, duration of torsion prior to presentation), variations in study design, sample sizes, follow-up durations, and differences in how manual detorsion was performed and confirmed (with or without post-detorsion ultrasonography). These factors likely contributed to the variability in success and orchiectomy rates across studies. Although this heterogeneity limits the precision and generalizability of the pooled estimates, it highlights important clinical considerations: manual detorsion may be more or less effective depending on patient age, symptom duration, and procedural confirmation. Therefore, the findings should be interpreted with caution, but they still provide valuable insights into the potential role of manual detorsion as an initial management strategy, particularly in situations where immediate surgical intervention is delayed, such as during the COVID-19 pandemic.
This review must be interpreted in light of several limitations. First, all included comparative studies carry a moderate risk of bias and have limited sample sizes. Second, the retrospective design of the studies introduces variability in reporting. Third, the meta-analysis involves the combination of heterogeneous data. A key contributor to this heterogeneity (I2 = 95.2%) is the incomplete reporting of important clinical factors, particularly patient age and the duration of torsion prior to intervention. These variables are known to influence the success of manual detorsion and testicular salvage rates; however, only a few of the included studies provided this information, which limited our ability to analyze their impact on outcomes. Additionally, the literature screening and data extraction in this review were performed by a single reviewer, which may introduce a potential selection bias. Although every effort was made to adhere strictly to PRISMA guidelines and to minimize subjectivity, the absence of multiple independent reviewers could have influenced the selection or interpretation of some studies. Future systematic reviews and meta-analyses using independent reviewers and a predefined consensus protocol would enhance the methodological rigor and reliability of findings.
Finally, most patients undergoing manual detorsion in the included studies were adults, while testicular torsion is more common in children and adolescents. Anatomical differences, smaller testicular size, and limited cooperation may make the procedure more challenging in younger patients. Adults generally tolerate the maneuver better, which can increase procedural success. These differences suggest that creating separate clinical groups for infants, adolescents, and adults would be beneficial for future studies. However, due to insufficient age-specific reporting in the included studies, we were unable to perform separate analyses for adults and children. Future studies creating distinct clinical groups for infants, adolescents, and adults would help clarify age-specific outcomes and enhance the applicability of results across different populations.
More prospective studies are needed to better evaluate the effectiveness of manual detorsion in the management of testicular torsion. Increasing its success rate and reducing time to intervention could help lower testicular loss. Manual detorsion, when applied promptly, represents an important option in testicular torsion management. Still, it must be recognized that this method may not suffice on its own in all cases.
To our knowledge, this systematic review and meta-analysis represents the first study comparing outcomes of manual detorsion in patients presenting with acute testicular torsion. While the strength of this analysis lies in its comprehensive reporting and external validity, the moderate risk of bias in the included studies limits the overall level of evidence. Additionally, internal validity and statistical power remain important limitations.
Manual detorsion is a non-invasive method for treating testicular torsion and is recommended as a first-line option in selected cases. Performing the procedure under ultrasonographic (US) guidance improves reliability and allows monitoring of testicular perfusion. Whether applied alone or followed by surgical exploration, it serves as a temporizing measure to reduce ischemia duration and increase testicular preservation. Manual detorsion should not replace definitive surgical repair. Its primary role is to gain time, particularly when immediate surgery is delayed, such as during the COVID-19 pandemic or in resource-limited settings. Surgical exploration and orchiopexy is the gold standard, and timely surgical intervention after detorsion is essential to ensure optimal testicular salvage.
Acknowledgement
Not applicable.
Funding Statement
The authors received no specific funding for this study.
Availability of Data and Materials
All data analysed in this meta-analysis were obtained from previously published studies and are publicly available in the respective articles. No individual patient data were used in this study.
Ethics Approval
Not applicable.
Conflicts of Interest
The author declares no conflicts of interest to report regarding the present study.
Supplementary Materials: The supplementary material is available online at https://www.techscience.com/doi/10.32604/cju.2025.072049/s1.
References
1. Coles V, Elagami H, Bhandarker K et al. The acute scrotum in infancy: a retrospective regional study. J Pediatr Urol 2022;18(2):226–231. doi:10.1016/j.jpurol.2021.08.008. [Google Scholar] [PubMed] [CrossRef]
2. Greear GM, Romano MF, Katz MH, Munarriz R, Rague JT. Testicular torsion: epidemiological risk factors for orchiectomy in pediatric and adult patients. Int J Impot Res 2021;33(2):184–190. doi:10.1038/s41443-020-0331-8. [Google Scholar] [PubMed] [CrossRef]
3. Yen CW, Chang YJ, Ming YC, Gau CC, Wu CT, Lee J. Factors determining testicular torsion and consequent orchiectomy in pediatric patients presenting with scrotal pain. Pediatr Emerg Care 2023;39(10):744–750. doi:10.1097/PEC.0000000000003037. [Google Scholar] [PubMed] [CrossRef]
4. Qin KR, Qu LG. Diagnosing with a TWIST: systematic review and meta-analysis of a testicular torsion risk score. J Urol 2022;208(1):62–70. doi:10.1097/JU.0000000000002496. [Google Scholar] [PubMed] [CrossRef]
5. Gunther P, Schenk JP, Wunsch R et al. Acute testicular torsion in children: the role of sonography in the diagnostic workup. Eur Radiol 2006;16(11):2527–2532. doi:10.1007/s00330-006-0287-1. [Google Scholar] [PubMed] [CrossRef]
6. Bandarkar AN, Blask AR. Testicular torsion with preserved flow: key sonographic features and value-added approach to diagnosis. Pediatr Radiol 2018;48(5):735–744. doi:10.1007/s00247-018-4093-0. [Google Scholar] [PubMed] [CrossRef]
7. Nash WG. Acute torsion of the spermatic cord: reduction: immediate relief. Br Med J 1893;1:742. [Google Scholar]
8. Törzsök P, Steiner C, Pallauf M et al. Long-term follow-up after testicular torsion: prospective evaluation of endocrine and exocrine testicular function, fertility, oxidative stress and erectile function. J Clin Med 2022;11(21):6507. doi:10.3390/jcm11216507. [Google Scholar] [PubMed] [CrossRef]
9. Smith WT, Midgley S, Kummer T. Real-time ultrasound-guided manual testicular detorsion: a case report. Clin Pract Cases Emerg Med 2022;6(3):248–251. doi:10.5811/cpcem2022.6.57256. [Google Scholar] [PubMed] [CrossRef]
10. Yığman M, Ekenci BY, Durak HM, Karakoyunlu AN. Predictive factors for manual detorsion success in testicular torsion. Int Urol Nephrol 2024;56(12):3797–3804. doi:10.1007/s11255-024-04151-0. [Google Scholar] [PubMed] [CrossRef]
11. Beher A, Moreno-Alfonso JC, Garnier H, Darici D, Salö MJ, Aubert O. A survey of preoperative, perioperative, and postoperative management practices for testicular torsion in pediatric patients among European surgeons. Eur J Pediatr Surg 2025;35(1):36–42. doi:10.1055/s-0044-1790244. [Google Scholar] [PubMed] [CrossRef]
12. Page MJ, McKenzie JE, Bossuyt PM et al. The PRISMA, 2020 statement: an updated guideline for reporting systematic reviews. Syst Rev 2021;10(1):89. doi:10.1186/s13643-021-01626-4. [Google Scholar] [PubMed] [CrossRef]
13. Sotiriadis A, Papatheodorou SI, Martins WP. Synthesizing evidence from diagnostic accuracy TEsts: the SEDATE guideline. Ultrasound Obstet Gynecol 2016;47(3):386–395. doi:10.1002/uog.15762. [Google Scholar] [PubMed] [CrossRef]
14. Yılmaz Başer H, Küçüker K. The effectiveness of manual detorsion applied in the emergency department in testicular torsion: a single-center experience of 13 years. Grand J Urol 2023;3(3):70–74. doi:10.5505/gju.2023.81300. [Google Scholar] [CrossRef]
15. Vuruşkan E, Erçil H, Karkin K et al. The effect of manual detorsion on testicular salvage rates in adult testicular torsion patients: single center experience. Duzce Med J 2022;24(2):101–104. doi:10.18678/dtfd.1073586. [Google Scholar] [CrossRef]
16. Vasconcelos-Castro S, Flor-De-Lima B, Campos JM, Soares-Oliveira M. Manual detorsion in testicular torsion: 5 years of experience at a single center. J Pediatr Surg 2020;55(12):2728–2731. doi:10.1016/j.jpedsurg.2020.02.026. [Google Scholar] [PubMed] [CrossRef]
17. Russo T, Cozzi DA, Gaglione G, Ceccanti S. The role of manual detorsion in pediatric testicular torsion during the global COVID-19 pandemic: experience from 2 centres. Urology 2023;180(3 Pt 1):227–234. doi:10.1016/j.urology.2023.04.025. [Google Scholar] [PubMed] [CrossRef]
18. Anastasakis M, Gkalonaki I, Doitsidis C, Michou P, Patoulias I. The importance of manual detorsion in intravaginal testicular torsion. Acta Med Bulg 2023;50(1):41–47. doi:10.2478/amb-2023-0006. [Google Scholar] [CrossRef]
19. Demirbas A, Demir DO, Ersoy E et al. Should manual detorsion be a routine part of treatment in testicular torsion? BMC Urol 2017;17(1):84. doi:10.1186/s12894-017-0276-5. [Google Scholar] [PubMed] [CrossRef]
20. Dias Filho AC, Oliveira Rodrigues R, Riccetto CLZ, Oliveira PG. Improving organ salvage in testicular torsion: comparative study of patients undergoing vs not undergoing preoperative manual detorsion. J Urol 2017;197(3Pt1):811–817. doi:10.1016/j.juro.2016.09.087. [Google Scholar] [PubMed] [CrossRef]
21. Vazquez JL, Fernandez MJ, Comendador-Morales A, Prada-Arias M. Testicular torsion and ultrasound-assisted manual detorsion. Pediatr Radiol 2025;55(4):674–681. doi:10.1007/s00247-024-06008-1. [Google Scholar] [PubMed] [CrossRef]
22. Mellick LB, Sinex JE, Gibson RW, Mears K. A systematic review of testicle survival time after a torsion event. Pediatr Emerg Care 2019;35(12):821–825. doi:10.1097/PEC.0000000000001287. [Google Scholar] [PubMed] [CrossRef]
23. MacDonald C, Kronfli R, Carachi R, O’Toole S. A systematic review and meta-analysis revealing realistic outcomes following paediatric torsion of testes. J Pediatr Urol 2018;14(6):503–509. doi:10.1016/j.jpurol.2018.09.017. [Google Scholar] [PubMed] [CrossRef]
24. Van Doeveren T, Somani BK, T Hoen LA, Haensel SM. Real-world management of testicular torsion: level of adherence to the EAU Pediatric Urology guidelines. J Pediatr Urol 2023;19(1):117–124. doi:10.1016/j.jpurol.2022.09.020. [Google Scholar] [PubMed] [CrossRef]
25. Pogorelić Z, Anand S, Artuković L, Krishnan N. Comparison of the outcomes of testicular torsion among children presenting during the Coronavirus Disease 2019 (COVID-19) pandemic versus the pre-pandemic period: a systematic review and meta-analysis. J Pediatr Urol 2022;18(2):202–209. doi:10.1016/j.jpurol.2022.01.005. [Google Scholar] [PubMed] [CrossRef]
26. Bowlin PR, Gatti JM, Murphy JP. Pediatric testicular torsion. Surg Clin North Am 2017;97(1):161–172. doi:10.1016/j.suc.2016.08.012. [Google Scholar] [PubMed] [CrossRef]
27. Moore SL, Chebbout R, Cumberbatch M et al. Orchidopexy for testicular torsion: a systematic review of surgical technique. Eur Urol Focus 2021;7(6):1493–1503. doi:10.1016/j.euf.2020.07.006. [Google Scholar] [PubMed] [CrossRef]
28. Scheier E. Manual detorsion in pediatric testicular torsion: a narrative review of the literature. Urologia 2024;91(3):628–631. doi:10.1177/03915603241229800. [Google Scholar] [PubMed] [CrossRef]
29. Hosokawa T. Recurrences of testicular torsion after manual detorsion: a single institution experience. Pediatr Emerg Med J. 2025;12(2):83–86. doi:10.22470/pemj.2025.01228. [Google Scholar] [CrossRef]
Cite This Article
 Copyright © 2026 The Author(s). Published by Tech Science Press.
Copyright © 2026 The Author(s). Published by Tech Science Press.This work is licensed under a Creative Commons Attribution 4.0 International License , which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
 Downloads
Downloads
 Citation Tools
Citation Tools