
 Submit a Paper
Submit a Paper Propose a Special lssue
Propose a Special lssue Open Access
Open Access
ARTICLE

Structural Gender Inequality and Mental Health among Chinese Men and Women
1
Department of Sociology, School of Ethnology and Sociology, Minzu University of China, Beijing, 100081, China
2
Department of Interdisciplinary Social Science, Faculty of Social and Behavioral Sciences, Utrecht University, Utrecht, 3508TC, The
Netherlands
3
Shanghai CSW&MSM Center (SCMC), Shanghai, 200023, China
* Corresponding Author: Lei Yang. Email:
International Journal of Mental Health Promotion 2023, 25(1), 31-43. https://doi.org/10.32604/ijmhp.2022.021375
Received 10 January 2022; Accepted 21 February 2022; Issue published 29 November 2022
 View Full Text
View Full Text Download PDF
Download PDFAbstract
Little is known about the association between structural gender inequality and health in patriarchal China. This study employed a sample from the Chinese Women’s Social Status, consisting of 26,139 participants aged 18 and 70 years (13,494 women and 12,645 men). Structural gender inequality was assessed at the macro-, meso-, and micro-levels. Mental health was measured by the summed scores of eight questions on depressive symptoms. Multilevel linear regression was applied for analysis. Results showed that total sex ratio at birth was associated with poorer mental health among women and men but sex ratio at birth of the second-born child predicted better mental health. Gender inequality at meso-level resulted in poorer mental health and gender inequality at microlevel was associated with poorer mental health both for men and women. Eliminating structural gender inequality promotes populations’ mental health in China.Keywords
Gender is a socially constructed concept as related to the internal sense of self, of which is related to behaviors and attributes. It is also a complex social system that structures the life experience as well as social statuses of all human beings [1–4]. As a socially constructed stratification system, gender is an institutionalized system connected to society’s power and resources, whereby women are always globally noted and portrayed as being subordinate to men [3]. The gender system resulting from unequal power relations structures the stratifications and inequalities in societies and shapes ideologies accordingly [5].
Gender systems construct gender roles and norms that determine life opportunities. It affects the social and structural determinants of physical and mental health, as well as the broader well-being, income, employment, and social services of societies, producing various kinds of gender inequality [6]. Gender roles and norms embedded in institutions determine the attributes, expectations, and behaviors valued and considered acceptable for both men and women. Unequal distribution of power and resources lead to inequality among individuals. Thus, gender systems are linked with multidimensional inequality, including employment opportunities, political participation, access to healthcare, and discrimination found across all societies [7,8].
It is well documented that gender inequality is associated with the adverse health of individual’s through multiple potential mechanisms [9]. Great amounts of research have focused on the factors involved at the individual, family, or community levels [10]. Recent studies have also extended prior research by depicting how structural determinant factors influence health outcomes in, for example, the United States [10,11]. Specifically, the structural determinant factors include the socio-economic and political processes that structure hierarchical power relations, stratifying societies based on class, occupational status, education level, and gender, among others arbitrary qualifications. Thus, structural gender inequality refers to the unequal division of power and resources between women and men and these inequalities are assigned through gendered mechanisms, reproduced, and maintained at the individual and societal levels [12]. Therefore, examining the association between structural gender inequality and health outcome is vital to identify the factors that can both undermine and benefit the population’s long-term health, especially in developing societies (e.g., China) where sociocultural gender inequality is much more persistently rooted than in many of their counterparts.
As the largest developing country, China has witnessed remarkable socio-economic development and rapid social transition since the economic reforms and market development in the late 1970s [13]. Simultaneously, there has also been the increasing and widening multidimensional social gaps, including gender inequality across socio-economic, political, and cultural domains [14]. Meanwhile, a large body of studies have discussed the definition and the dimensions of structural gender inequality and their effects on individuals’ health in Western societies [10–11,15]. Yet in light of China’s increasing socio-economic achievements as well as the rooted patriarchal societal system, very scarce attention has been paid to analyzing how structural gender inequality is associated with individual health among Chinese men and women.
Gender inequality has been long existed in China, a patriarchal society where women are subordinate to men [16]. These social, cultural, and political contexts might further exacerbate structural gender inequality. Although there is a remarkable decrease in gender inequality in China in recent decades, there is a lack of understanding of the association between structural gender inequality and health among Chinese women and men. The current study aims to resonate with the recently recognized importance of the macro-level social and political factors in determining an individual’s health [11,17]. We aim to examine how structural gender inequality is associated with self-rated health and depression among Chinese men and women.
2.1 Structural Gender Inequality and Health
Gender inequality results from both individual and social determinants. Structural gender inequality refers to the inequality determined and created by structural social determinants that generate social class inequalities in society [10–11,18]. Socially and culturally constructed gender norms determine roles and opportunities and powerfully shape all aspects of health and well-being [19]. The perspective of the research on gender inequality and health is shifting from an individual-focused to a structural-focused approach. The earlier approach regarded gender as an individual attribute, examining why men and women differ in health outcomes [20]. The health disparity among men and women results from various biological and behavioral factors (e.g., age, chromosomes, smoking, drinking, etc.). These studies generally support women having a longer life expectancy and lower mortality risk than men while having a higher prevalence of chronic diseases or comorbidities [21,22]. Individual-level factors resulted in health differences/disparities rather than inequality which indicates unfairness or structural disadvantage.
Recent studies have investigated the structural determinants of gender inequality and their effects on health [10,11]. The structural factors such as economic systems, political power, and resources that determine material and other assets, labor division, political participation, laws, social norms, and ideology all affect health inequalities. According to Heise and colleagues [7], if examining the structural and social determinants of health from the life course perspective, health inequality originates during childhood when gender socialization plays an essential role in embedding gender norms into individuals [7]. Consequently, the gender system in families, institutions, and communities create and perpetuate gender roles and norms. The gender system also stratifies men and women in gendered social positions, characterized by social class, race, and so on. This may lead to gender differences in hazard exposure, health behaviors, and healthcare access, and can eventually create health inequality over time and generations.
Structural gender inequality could be conceptualized as inequality at the micro-, meso-, and macro-levels [11]. Micro-level inequality usually indicates internalized gender norms and roles, which symbolize individually embodied gender inequality created through socialization, internalization, and self-construction [3]. Although micro gender inequality is expressed at the individual level, it can be regarded as structural because it reproduces discriminatory gender structures [11], which may disproportionately affect the health between men and women. A large body of literature has previously assessed how masculinity norms link with men’s health, but little research has examined the association between femininity and women’s health. Previous studies found that men are more likely to engage in unhealthy and risky behaviours to conform to hegemonic masculine ideals, which leads to worse health [23].
Meso-structural gender inequality refers to the inequality in power and resources between men and women brought by gender interactions within families, the workplace, and other social settings shaped by hegemonic cultural gender norms [11,24]. Gender norms and cultural expectations require women to do more undesirable work or overloaded work (e.g., caring for the family) and to face more work-family conflict, which may induce increased levels of long-term stress [25]. For example, previous studies have suggested that the spouse with the higher relative income reports higher levels of life satisfaction regardless of the respondent’s sex in the US and Hungary [26,27] while some studies found that men reported a lower level of well-being when their wives’ relative income increase [28]; changes in proportional earnings had no effect on life satisfaction for women [29].
Gender inequality at the macro-level indicates systematic gender inequality in power and resources that could be global, national, or state in scale, favoring men within political, economic, and cultural institutions [11]. Extensive studies have examined the association between macro-socioeconomic factors and individual health in Western societies. For example, several studies found a significant correlation between national income inequality and mortality risk [9,30]. One study documented significant positive associations between the gender inequality index (measured by macro-structural factors, e.g., parliamentary representation of women, labor force participation by women, and maternal mortality rate) and child mortality rates [31].
Three hypothetical empirical associations between structural gender inequality and health among men and women were proposed by Homan [11]. First, that structural gender inequality harms men’s and women’s health equally, which means that it does not affect individual health. Thus, the observed gender gaps in health outcomes may result from other non-social factors. Second is the zero-sum effect, which means one person’s gain would be another’s loss. That is, structural gender inequality is beneficial to men’s health while being harmful to women. Third, the hypothesis argues that both men’s and women’s health are negatively affected by structural gender inequality, suggesting that the patriarchal system fosters a toxic culture harming men and women [24].
2.2 Structural Gender Inequality in China
While research in developed countries has extensively demonstrated the relevance of structural gender inequality to health status [11,17], the association between structural gender inequality and individual health is still scant in China. Chinese women’s social status has seen unprecedented change as China has shifted from a traditional to a modern society. Massive gender inequality was reported in the traditional Chinese culture characterized by patriarchy, where women were considered subordinate to men [32]. In this patriarchal society of decades ago, Chinese women were confined to the home, taking the major responsibilities of feeding family members, taking care of children, running the household, and caring for the elderly [33,34]. Most women received no schooling and were illiterate. However, men were considered to be the primary sources of the labor force, and the breadwinners. Thus, most of the Chinese people preferred sons rather than daughters. Son preference symbolized gender discrimination and cultural norms in traditional Chinese society [35]. This differentiated gender value further reinforced women’s subordination to men.
After the foundation of the People’s Republic of China in 1949, the socialist revolution and development led to Chinese women’s emancipation in the country. Gender equality became the mainstream ideology of the country, and an increasing number of women participated in the workforce with men [36]. The rights and interests of women were institutionally and legally protected by national laws, regulations, and policies set up by the Chinese central governments. Women became the real owners of society and made significant contributions to China’s social and economic development. Notably, during the planned economy era, Chinese women’s labor participation was relatively high as they were exempt from the burden of caring for children or older adults, and employers in the planned economy mainly provided this welfare [36].
After the economy shifted from planned to market-oriented in the late 1970s, gender inequality started to come back across Chinese society in multiple dimensions [37]. This could be demonstrated in several spheres. Economically, as market economy reform paid a considerable amount of attention to efficiency while ignoring fairness, exacerbating social polarization, and widening the gap between the rich and the poor, as well as men and women. There was a significant cut-down of the state-owned or community-owned social services in the market-oriented Chinese reform period. Thus, women were at a disadvantage because they had to balance family and work under the embedded traditional gender norms as homemakers while men acted as the breadwinners, resulting in long-term stress for women [38].
Additionally, rapid modernization in China has yielded uneven gains between men and women. The widening wage gap between women and men resulted from the increased labour market discrimination [39], where women were rejected from some occupations because of their assumed physical performance and potential maternity leave. Politically, for example, although women in China accounted for more than 20 percent of all National People’s Congress (NPC) delegates, they are still under-represented at all levels of the Chinese Communist Party or governmental hierarchies [40]. Culturally, the persistently rooted and dominate patriarchal culture [41] as well as the related practices, still influence Chinese women’s social status within the family and the society in many aspects, which are embedded in many patriarchal cultural norms. For example, the son preference and sex ratio at birth [42,43], the use of contraception [44], women’s housework time and care work [45], and intra-household power concerning the marital matching [46], which somehow reflect the women’s bargaining power with men and gender inequality.
To sum up, while China has achieved significant improvement in women’s health during the past four decades, far less has been achieved on gender equality in general [47]. Although women’s social status has made considerable progress in recent decades, structural gender inequality remains in the current Chinese society. Previous studies have examined different social factors affecting health disparity in China [48,49]; nonetheless, there is a lack of research on structural gender inequality and mental health in China. The aim of the study is to examine the association of structural gender inequality with womens’ and men’s mental health.
The data used in this study were retrieved from the third survey of the Chinese Women’s Social Status (CWSS), a nationwide decennial representative survey jointly conducted by the China Women’s Federation and National Bureau of Statistics in 1990, 2000, and 2010. Data was collected using structured questionnaires, and informed consent was obtained from all participants. The survey employed a multi-stage stratified random sampling method and the aim of the survey was to review gender equality and women’s development in China over the past 10 years. The CWSS collected plentiful information on individuals and families covering demographic factors, health, socio-economic status, social security and welfare, marriage and family, gender roles, etc.
Using the CWSS has certain advantages. Firstly, it is a representative survey on women’s development in China. Secondly, it contains information on health and gender inequality at meso- and micro levels. Thirdly, the data has a two-level hierarchical structure with individuals from 31 provinces where they are exposed to different levels of structural gender inequality, which is suitable for studying the association between structural gender inequality and health status. The third survey conducted in 2010 was used in this study, and the final sample size was 26,139 participants aged 18 and 70 years (13,494 women and 12,645 men).
Mental health was measured by eight questions about depressive symptoms. The respondents were asked whether they had the following eight circumstances in recent 30 days: insomnia, physical and mental exhaustion, irritability, wanting to cry, disinterest, feelings of loneliness, feelings of uselessness and feelings of meaningless. The response for each question was on a four-scale metric: rarely, in some days, occasionally, and most of the time, coded from 0 to 3, respectively. The Cronbach’s alpha is 0.85, indicating higher reliability of the items. The eight responses were summed up to derive mental health scores (0–24, a higher score indicating worse mental health).
The structural gender inequality in this study was assessed at the macro-, meso-, and micro levels, as suggested by Homan [11] and Risman [3]. Due to the unavailability of certain data concerning the political representation and labor participation of women in each province of China, gender inequality at the macro level was measured by four variables in cultural domains in each province: total sex ratio at birth, the sex ratio at the birth of the second child, percentage of tubectomies, and percentage of vasectomies.
The sex ratio at birth (i.e., the number of boys divided by that of girls at birth), particularly for the sex ratio of the second-born child, is the most prominent external demonstration of gender inequality. Under the ‘One-Child Policy’ and the long history of ‘son preference’ in Chinese history, more boys than girls were given birth to, and the sex ratio at birth has been distorted since the 1980s, which worsened discrimination against women and girls, especially in rural China. Son preference demonstrates the discriminatory ‘value’ of males over females, which can be traced back to thousands of years in Chinese history [50,51].
Contraceptive behavior is a social practice shaped by complex interactions between males and females on the gendered roles and responsibilities [52]. Contraceptive use depends on women’s ability to make decisions. Women with more significant resources (e.g., the highest education or income) have a more significant influence on the couple’s choice of contraceptive methods [44,53]. Previous studies suggested that women’s bargaining power significantly increases the probability of contraceptive use [54,55]. Hence, contraception among men and women may reflect gender inequality concerning the negotiation or bargaining power. Chinese women take responsibility for giving birth and the main risk of reproductive health, which depends on different contraceptive methods. The higher percentage of vasectomies in men and lower percentages of tubectomies in the population of women reflect gender equality in China. In this study, the percentage of vasectomies or tubectomies in each province, to some extent, indicates how men and women negotiate with each other, and a higher percentage of vasectomies or lower percentage of tubectomies in each province indicates more gender equality [56].
The total sex ratio at birth and the sex ratio of the second-born child in 2010 were selected from the 2010 census data conducted by the National Bureau of Statistics. The percentage of tubectomy or vasectomy in 2010 was selected from the China Health Statistical Yearbook of 2011 [57].
Structural gender inequality at the meso level was measured in households from the dataset directly, including relative education within a couple (equivalent, husband < wife, husband > wife) and relative income within a couple (equivalent, husband < wife, husband > wife). These two variables represented inter-spousal inequality within the family [11], and the partner wage gap was an adequate measure of enduring gender inequality within modern coupledom [29].
Micro-level gender inequality was measured by internalized gender norms (measured directly from the dataset), which symbolized individually embodied gender inequality created through socialization, internalization, and self-construction [3]. The extent to which respondents agreed to the following five statements was used to construct traditional or egalitarian gender norms (Cronbach’s alpha = 0.73). The statements were: ‘A man’s place is in the office, while a woman’s place is in the home’, ‘Breadwinner is a man’s main responsibility’, ‘For women, a good marriage is better than a good job’, ‘Boys should behave as boys, and girls should behave as girls do’, and ‘The development of the husband is more important than that of the wife’. Each question’s answer was 5-scale categories: 1 = strongly agree, 2 = agree, 3 = disagree, and 4 = strongly disagree. The five statements were summed up (1–20), and higher scores indicated more egalitarian gender roles and gender equality.
Covariates included age (18–70 years), years of education (0–13 years), area of residence (rural or urban), frequency of physical activity in the last year (never, occasionally, sometimes, often), marital status (married or unmarried), and GDP of each province in 2010 from the China Statistical Yearbook [58].
Since the dataset had a hierarchical structure (individuals nested within provinces), we used two-level hierarchical linear regression modeling to examine the association between structural gender inequality and mental health. Hierarchical regression allows the data’s hierarchical nature to be incorporated into the analyses and measuring the variables at different levels. The ordered hierarchical logistic model is as follows:
Yij is the individual’s mental health, γ00 is the constant, Xij is a vector of independent variables, β0j is a vector of coefficients for Xij, and eij is an error term or unobserved heterogeneities. i and j denote persons and provinces, respectively. uij and αj capture provincial and individual heterogeneities, which are assumed to be uncorrelated.
Random-effects models stratified by gender were estimated using STATA 15.1 (Stata Corp. 2017. College Station, TX). We modeled the full sample (married + unmarried) and married sample separately as the meso-levels were measured within the family. Missing data made up less than 1% for any given variable except for the married sample (8%) in the dataset. Thus, the listwise deletion strategy was used to deal with missing data, as it may be less biased than standard multiple imputations when missing data are not random for income, as people with higher income are less likely to report their income information [59]. Robust checks indicates that there were not significant differences between age or cohort.
Table 1 presents the descriptive statistics of the sample at different levels by men and women. The mean values of mental health scores were 2.7 for men and 4.0 for women, respectively. On average, the respondents received 9 or 10 years of education. Nearly 46%–49% lived in rural areas, and 83%–85% were married. Regarding structural gender inequality, the total sex ratio at birth and the sex ratio at birth for the second child were approximately 120 and 130, higher than the normal (101–107). On average, 0.9% of the men underwent vasectomies in all provinces. At the meso level, men are better educated and earned a higher income than their wives.
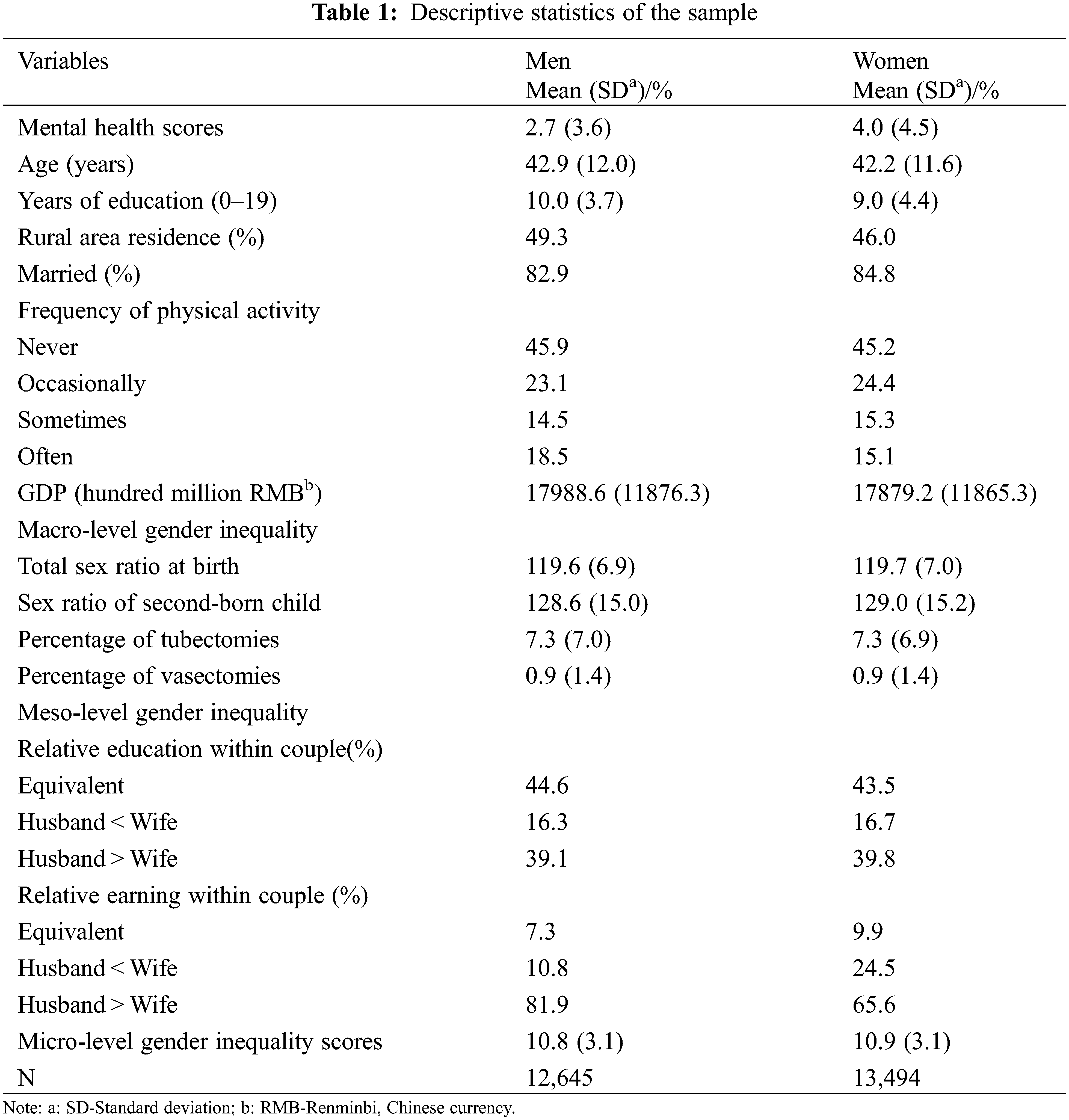
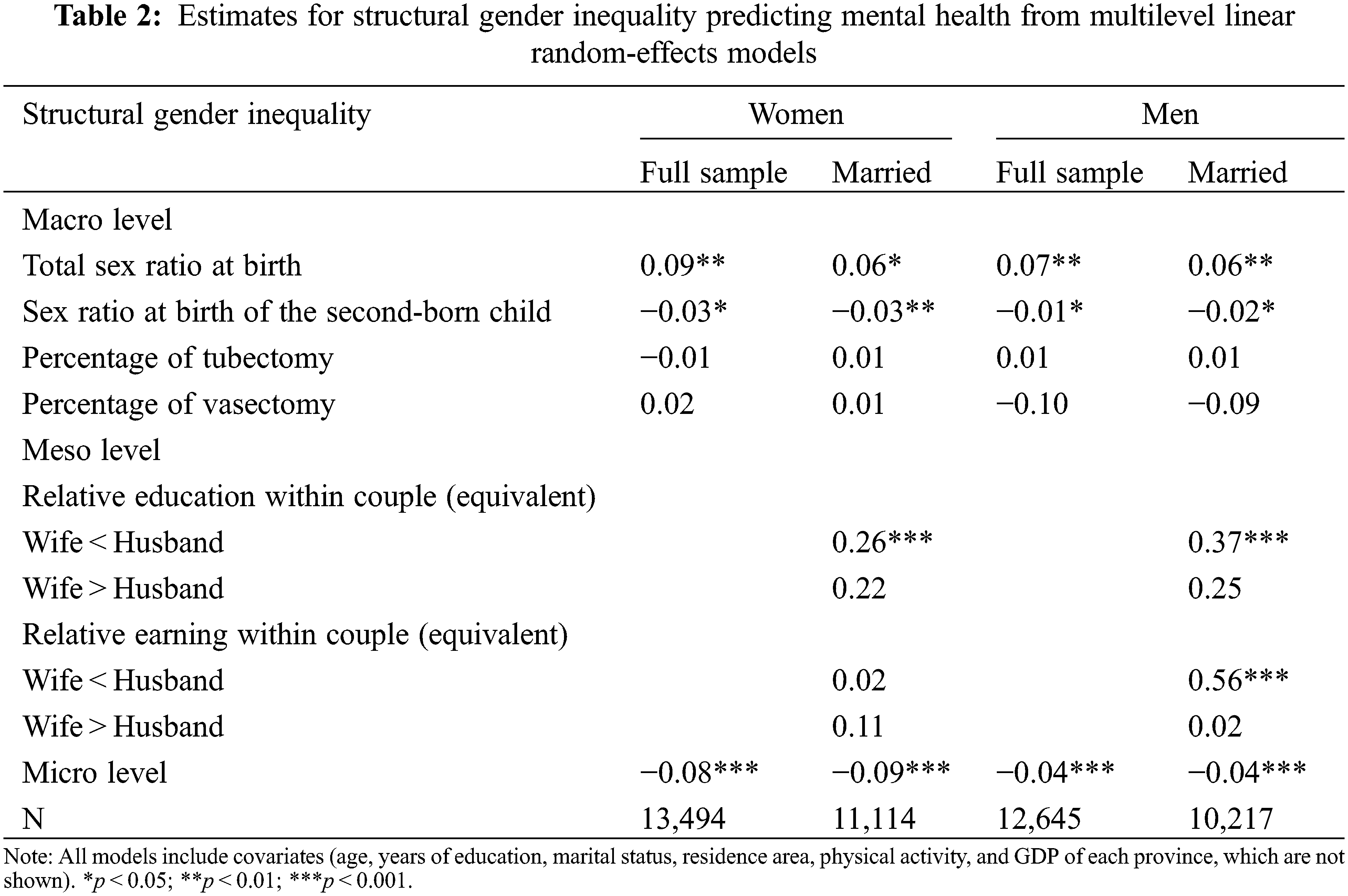
Table 2 presents the coefficients for structural gender inequality, predicting mental health using multilevel linear random-effects models for women and men, respectively. The results suggested that the total sex ratio at birth was associated with poorer mental health among women and men but the sex ratio at birth of the second-born child predicted better mental health. The percentage of tubectomies and vasectomies were not associated with mental health regarding both for women and men, while gender equality (higher scores at micro-level) predicted better mental health. At meso-level, women reported worse mental health if their education was lower than that of their husbands. Similarly, men reported worse mental health if their education or income was lower than that of their wives.
For the sensitivity test, no significant interaction effects were found between meso-and micro-level predictors. We also analyzed the sample aged 45 and over (middle-aged and older adults), and the results were comparable.
This study examined the association of structural gender inequality with mental health among Chinese men and women based on nationally representative data—CWSS. We systematically assessed the relationship between the structural gender system at the macro-, meso-, and micro levels, as well as mental health among men and women in China. The results suggested that the total sex ratio at birth was associated with poorer mental health among women and men, but that the sex ratio at birth of the second-born child predicted better mental health. Structural gender inequality at meso-and micro-level harmed both women’s and men’s mental health in China.
Specifically, structural gender inequality at the macro-level (the total sex ratio at birth) was associated with more depression, which is in line with a previous study in the USA [11]. However, we also found the heterogeneous effects of macro gender inequality in particular in the Chinese context. We found that the sex ratio at birth of the second-born child was associated with better mental health for Chinese men and women. The higher sex ratio at birth of the second-born child means more boys were born which brings more happiness to their parents. This may indicate the spillover effects of the child on their parents’ mental health if the second-born is a boy in China. Previous studies demonstrated that structural gender inequality harmed women’s health through multiple pathways, including perceived gender discrimination, healthcare access, long-term stress, and unsafe working conditions [60,61]. As a previous study noted, the distorted sex ratio at birth reflects the patriarchal culture, son preference, and women’s subordination [62]. Hence, long-term exposure to this discriminated culture leads to psychological stress for women during their socialization process.
For men and women, structural gender inequality at meso levels was associated with poorer mental health, although numerous studies have demonstrated that men benefit more from marriage than women do, in particular those with higher spousal socio-economic status [63,64]. Consistent with a US study [11], the findings in this study suggested higher meso-level gender inequality was associated with worse mental health. Usually, when husbands earned lower than that of their wives, the former reported worse health status because of males’ social norms as breadwinners [29]. As a study noted, the traditional gender norms of the male breadwinner are challenged when the percentage of wives out-earning their husbands and the ‘gender role reversals in marriage’ are associated with adverse physical and mental health [65]. Therefore, this study’s findings suggest a universal harmful effect of higher structural gender inequality at the meso-level on women’s and men’s health in China. At the meso-level, greater exposure to structural gender inequality was associated with worse mental health among women and men.
In this study, structural gender inequality at the micro-level was associated with worse mental health for both Chinese women and men, which is consistent with a prior study suggesting that young Chinese people with egalitarian views were associated with a lower level of depression, anxiety, and stress [66]. Men or women with more traditional gender roles may be associated with more undesirable work or overloaded work (e.g., caring for the family) and facing more work-family conflict, which may induce long-term stress [25].
The study’s aims were to systemically examine the association between structural gender inequality at different levels and mental health among Chinese women and men. Specifically, multiple measurements were adopted to assess structural gender inequality at three levels: macro-, meso-, and micro-. Nationally representative survey data and multilevel linear regression were both used. However, the study has some limitations. First, some factors (e.g., perceived gender discrimination or sexual harassment) and health behaviors (smoking or drinking status) could not be controlled in the models because of the unavailability of information, although physical activity has been adjusted. Second, the study’s dataset is cross-sectional, limiting the possibility of examining the causality of structural gender inequality to health. Future studies using longitudinal data covering a longer period are needed to study the long-term effects and structural gender inequality changes on the health statuses of all Chinese women and men (e.g., reproductive health).
This study demonstrates that structural gender inequality harms both women’s and men’s health status in China. Chinese society has been characterized by a patriarchal system where women were subordinated to men, although they have achieved significant social status progress in recent decades. Traditional gender norms and roles are emerging to be seemingly and increasingly equal amid China’s modernization process, and feminism is arising in academia, grassroots organizations, and some coastal and cosmopolitan cities [67]. However, structural gender inequality may still exist in the long run, especially in rural areas where women always acquire fewer educational opportunities. Numerous hidden and invisible institutional, and cultural barriers exist in Chinese society and are continuously producing structural gender inequality (e.g., gender discrimination, family-work conflict, sexual harassment). Women’s participation in political and other decision-making processes from family to national levels should be increased to speak and represent their voice and agency. This study could inform future policies (centered on women issues, family, marriage, work, care, etc.) by raising the awareness of structural gender inequality in particular for male policy-makers, while advocating for attempts to eliminate all aspects of structural gender inequality and improve women’s social status.
Funding Statement: The authors received no specific funding for this study.
Conflicts of Interest: The authors declare that they have no conflicts of interest to report regarding the present study.
References
1. Marchbank, J., Letherby, G. (2014). Introduction to gender: Social science perspectives. London: Routledge. [Google Scholar]
2. Ridgeway, C. L., Smith-Lovin, L. (1999). The gender system and interaction. Annual Review of Sociology, 25, 191–216. DOI 10.1146/annurev.soc.25.1.191. [Google Scholar] [CrossRef]
3. Risman, B. J. (2004). Gender as a social structure: Theory wrestling with activism. Gender & Society, 18(4), 429–450. DOI 10.1177/0891243204265349. [Google Scholar] [CrossRef]
4. Lorber, J., Farrell, S. A. (1991). The social construction of gender. USA: Sage Publications, Inc. [Google Scholar]
5. Ridgeway, C. L., Correll, S. J. (2004). Unpacking the gender system: A theoretical perspective on gender beliefs and social relations. Gender and Society, 18(4), 510–531. DOI 10.1177/0891243204265269. [Google Scholar] [CrossRef]
6. Pincus, F. L. (1996). Discrimination comes in many forms: Individual, institutional, and structural. American Behavioral Scientist, 40(2), 186–194. DOI 10.1177/0002764296040002009. [Google Scholar] [CrossRef]
7. Heise, L., Greene, M. E., Opper, N., Stavropoulou, M., Harper, C. et al. (2019). Gender inequality and restrictive gender norms: Framing the challenges to health. Lancet, 393(10189), 2440–2454. DOI 10.1016/S0140-6736(19)30652-X. [Google Scholar] [CrossRef]
8. Lorber, J. (2018). Paradoxes of gender redux. In: Naples, N. A. (Ed.Gender reckonings: New social theory and research, pp. 297–313. New York: New York University Press. [Google Scholar]
9. Pickett, K. E., Wilkinson, R. G. (2015). Income inequality and health: A causal review. Social Science & Medicine, 128, 316–326. DOI 10.1016/j.socscimed.2014.12.031. [Google Scholar] [CrossRef]
10. George, A. S., Amin, A., de Abreu Lopes, C. M., Ravindran, T. S. (2020). Structural determinants of gender inequality: Why they matter for adolescent girls’ sexual and reproductive health. British Medical Journal, 368(l6985), 19–23. DOI 10.1136/bmj.l6985. [Google Scholar] [CrossRef]
11. Homan, P. (2019). Structural sexism and health in the United States: A new perspective on health inequality and the gender system. American Sociological Review, 84(3), 486–516. DOI 10.1177/0003122419848723. [Google Scholar] [CrossRef]
12. Okin, S. M. (1989). Justice, gender, and the family. New York: Basic Books. [Google Scholar]
13. Rawski, T. G. (1995). Implications of China’s reform experience. The China Quarterly, 144, 1150–1173. DOI 10.1017/S030574100000477X. [Google Scholar] [CrossRef]
14. Ji, Y., Wu, X. (2018). New gender dynamics in post-reform China: Family, education, and labor market. Chinese Sociological Review, 50(3), 231–239. DOI 10.1080/21620555.2018.1452609. [Google Scholar] [CrossRef]
15. Denton, M., Prus, S., Walters, V. (2004). Gender differences in health: A Canadian study of the psychosocial, structural and behavioural determinants of health. Social Science & Medicine, 58(12), 2585–2600. DOI 10.1016/j.socscimed.2003.09.008. [Google Scholar] [CrossRef]
16. Jaschok, M., Miers, S. (1994). Women and Chinese patriarchy: Submission, servitude, and escape. London and New Jersey: Zed Books. [Google Scholar]
17. van de Velde, S., Huijts, T., Bracke, P., Bambra, C. (2013). Macro-level gender equality and depression in men and women in Europe. Sociology of Health & Illness, 35(5), 682–698. DOI 10.1111/j.1467-9566.2012.01521.x. [Google Scholar] [CrossRef]
18. Sen, G., Östlin, P. (2008). Gender inequity in health: Why it exists and how we can change it. Global Public Health, 3(S1), 1–12. DOI 10.1080/17441690801900795. [Google Scholar] [CrossRef]
19. Kennedy, E., Binder, G., Humphries-Waa, K., Tidhar, T., Cini, K. et al. (2020). Gender inequalities in health and wellbeing across the first two decades of life: An analysis of 40 low-income and middle-income countries in the Asia-pacific region. The Lancet Global Health, 8(12), e1473–e1488. DOI 10.1016/S2214-109X(20)30354-5. [Google Scholar] [CrossRef]
20. Read, J. N. G., Gorman, B. K. (2010). Gender and health inequality. Annual Review of Sociology, 36, 371–386. DOI 10.1146/annurev.soc.012809.102535. [Google Scholar] [CrossRef]
21. Arber, S., Cooper, H. (1999). Gender differences in health in later life: The new paradox? Social Science & Medicine, 48(1), 61–76. DOI 10.1016/S0277-9536(98)00289-5. [Google Scholar] [CrossRef]
22. Murtagh, K. N., Hubert, H. B. (2004). Gender differences in physical disability among an elderly cohort. American Journal of Public Health, 94(8), 1406–1411. DOI 10.2105/AJPH.94.8.1406. [Google Scholar] [CrossRef]
23. Courtenay, W. H. (2000). Constructions of masculinity and their influence on men’s well-being: A theory of gender and health. Social Science & Medicine, 50, 1385–1401. DOI 10.1016/S0277-9536(99)00390-1. [Google Scholar] [CrossRef]
24. Connell, R. (2012). Gender, health and theory: Conceptualizing the issue, in local and world perspective. Social Science & Medicine, 74(11), 1675–1683. DOI 10.1016/j.socscimed.2011.06.006. [Google Scholar] [CrossRef]
25. Cerrato, J., Cifre, E. (2018). Gender inequality in household chores and work-family conflict. Frontiers in Psychology, 9(1330), 1–11. DOI 10.3389/fpsyg.2018.01330. [Google Scholar] [CrossRef]
26. Eirich, G. M., Robinson, J. H. (2017). Does earning more than your spouse increase your financial satisfaction? A comparison of men and women in the United States, 1982 to 2012. Journal of Family Issues, 38(17), 2371–2399. DOI 10.1177/0192513X16638384. [Google Scholar] [CrossRef]
27. Hajdu, G., Hajdu, T. (2018). Intra-couple income distribution and subjective well-being: The moderating effect of gender norms. European Sociological Review, 34(2), 138–156. DOI 10.1093/esr/jcy006. [Google Scholar] [CrossRef]
28. Rogers, S. J., DeBoer, D. D. (2001). Changes in wives’ income: Effects on marital happiness, psychological well-being, and the risk of divorce. Journal of Marriage and Family, 63(2), 458–472. DOI 10.1111/j.1741-3737.2001.00458.x. [Google Scholar] [CrossRef]
29. Gash, V., Plagnol, A. C. (2021). The partner pay gap: Associations between spouses’ relative earnings and life satisfaction among couples in the UK. Work, Employment and Society, 35(3), 566–583. DOI 10.1177/0950017020946657. [Google Scholar] [CrossRef]
30. Babones, S. J. (2008). Income inequality and population health: Correlation and causality. Social Science & Medicine, 66(7), 1614–1626. DOI 10.1016/j.socscimed.2007.12.012. [Google Scholar] [CrossRef]
31. Brinda, E. M., Rajkumar, A. P., Enemark, U. (2015). Association between gender inequality index and child mortality rates: A cross-national study of 138 countries. BMC Public Health, 15(1), 1–6. DOI 10.1186/s12889-015-1449-3. [Google Scholar] [CrossRef]
32. Bauer, J., Wang, F., Riley, N. E., Zhao, X. H. (1992). Gender inequality in urban China: Education and employment. Modern China, 18(3), 333–370. DOI 10.1177/009770049201800304. [Google Scholar] [CrossRef]
33. Lee, S. W. (1999). The patriarchy in China: An investigation of public and private spheres. Asian Journal of Women’s Studies, 5(1), 9–49. DOI 10.1080/12259276.1999.11665840. [Google Scholar] [CrossRef]
34. Cook, S., Dong, X. Y. (2011). Harsh choices: Chinese women’s paid work and unpaid care responsibilities under economic reform. Development and Change, 42(4), 947–965. DOI 10.1111/j.1467-7660.2011.01721.x. [Google Scholar] [CrossRef]
35. Das Gupta, M., Jiang, Z. H., Li, B. H., Xie, Z. M., Chung, W. J. et al. (2003). Why is son preference so persistent in East and South Asia? A cross-country study of China, India and the Republic of Korea. The Journal of Development Studies, 40(2), 153–187. DOI 10.1080/00220380412331293807. [Google Scholar] [CrossRef]
36. Wang, Q., Min, D. C., Sørensen, B. Æ. (2016). Revisiting gender inequality: Perspectives from the People’s Republic of China. New York: Palgrave Macmillan. [Google Scholar]
37. Sun, W. N., Guo, Y. J. (2013). Unequal China: The political economy and cultural politics of inequality. USA and Canada: Routledge. [Google Scholar]
38. Shui, Y., Xu, D., Liu, Y., Liu, S. (2020). Work-family balance and the subjective well-being of rural women in Sichuan, China. BMC Women’s Health, 20(1), 1–10. DOI 10.1186/s12905-019-0871-6 [Google Scholar] [CrossRef]
39. Lee, J. W., Wie, D. (2017). Wage structure and gender earnings differentials in China and India. World Development, 97, 313–329. DOI 10.1016/j.worlddev.2017.04.016. [Google Scholar] [CrossRef]
40. Iwanaga, K. (2008). Women’s political participation and representation in Asia: Obstacles and challenges. Denmark: NIAS Press. [Google Scholar]
41. Shen, Y. F. (2011). China in the “Post-patriarchal Era” changes in the power relationships in urban households and an analysis of the course of gender inequality in society. Chinese Sociology & Anthropology, 43(4), 5–23. DOI 10.2753/CSA0009-4625430401. [Google Scholar] [CrossRef]
42. Li, L., Wu, X. (2011). Gender of children, bargaining power, and intrahousehold resource allocation in China. Journal of Human Resources, 46(2), 295–316. DOI 10.1353/jhr.2011.0014. [Google Scholar] [CrossRef]
43. Bulte, E., Tu, Q., List, J. (2015). Battle of the sexes: How sex ratios affect female bargaining power. Economic Development and Cultural Change, 64(1), 143–161. DOI 10.1086/682706. [Google Scholar] [CrossRef]
44. Xu, Y., Bentley, R. J., Kavanagh, A. M. (2011). Gender equity and contraceptive use in China: An ecological analysis. Women & Health, 51(8), 739–758. DOI 10.1080/03630242.2011.623221. [Google Scholar] [CrossRef]
45. Kan, M. Y., He, G. (2018). Resource bargaining and gender display in housework and care work in modern China. Chinese Sociological Review, 50(2), 188–230. DOI 10.1080/21620555.2018.1430506. [Google Scholar] [CrossRef]
46. Du, J., Wang, Y., Zhang, Y. (2015). Sex imbalance, marital matching and intra-household bargaining: Evidence from China. China Economic Review, 35, 197–218. DOI 10.1016/j.chieco.2014.11.002. [Google Scholar] [CrossRef]
47. Yu, M. Y., Sarri, R. (1997). Women’s health status and gender inequality in China. Social Science & Medicine, 45(12), 1885–1898. DOI 10.1016/S0277-9536(97)00127-5. [Google Scholar] [CrossRef]
48. Tang, S., Meng, Q., Chen, L., Bekedam, H., Evans, T. et al. (2008). Tackling the challenges to health equity in China. The Lancet, 372(9648), 1493–1501. DOI 10.1016/S0140-6736(08)61364-1. [Google Scholar] [CrossRef]
49. Yip, W., Subramanian, S. V., Mitchell, A. D., Lee, D. T., Wang, J. et al. (2007). Does social capital enhance health and well-being? Evidence from rural China. Social Science & Medicine, 64(1), 35–49. DOI 10.1016/j.socscimed.2006.08.027. [Google Scholar] [CrossRef]
50. Greenhalgh, S. (2003). Science, modernity, and the making of China’s one-child policy. Population and Development Review, 29(2), 163–196. DOI 10.1111/j.1728-4457.2003.00163.x. [Google Scholar] [CrossRef]
51. Li, J., Cooney, R. S. (1993). Son preference and the one-child policy in China: 1979–1988. Population Research and Policy Review, 12(3), 277–296. DOI 10.1007/BF01074389. [Google Scholar] [CrossRef]
52. Gribaldo, A., Judd, M. D., Kertzer, D. I. (2009). An imperfect contraceptive society: Fertility and contraception in Italy. Population and Development Review, 35(3), 551–584. DOI 10.1111/j.1728-4457.2009.00296.x. [Google Scholar] [CrossRef]
53. Grady, W. R., Klepinger, D. H., Billy, J. O., Cubbins, L. A. (2010). The role of relationship power in couple decisions about contraception in the US. Journal of Biosocial Science, 42(3), 307–323. DOI 10.1017/S0021932009990575. [Google Scholar] [CrossRef]
54. Tchakounté Tchuimi, D., Kamga, B. (2020). The effect of women? Bargaining power within couples on contraceptive use in Cameroon. Gates Open Research, 4, 20. DOI 10.12688/gatesopenres. [Google Scholar] [CrossRef]
55. Juraqulova, Z. H., Henry, E. B. (2020). Women’s bargaining power and contraception use in post-soviet Tajikistan. Central Asian Survey, 39(4), 520–539. DOI 10.1080/02634937.2020.1806202. [Google Scholar] [CrossRef]
56. Mathur, K. (2008). Gender hierarchies and inequalities: Taking stock of women’s sexual and reproductive health. Economic and Political Weekly, 43(49), 54–61. [Google Scholar]
57. Ministry of People’s Republic of China (2011). China health statistical yearbook. Beijing, China: Peking Union Medical College Press. [Google Scholar]
58. National Bureau of Statistics of China (2011). China statistical yearbook. Beijing, China: China Statistics Press. [Google Scholar]
59. Allison, P. (2014). Listwise deletion: It’s NOT evil. https://statisticalhorizons.com/listwise-deletion-its-not-evil. [Google Scholar]
60. Adler, N. E. (2009). Health disparities through a psychological lens. American Psychologist, 64(8), 663–673. DOI 10.1037/0003-066X.64.8.663. [Google Scholar] [CrossRef]
61. Marmot, M. (2005). Social determinants of health inequalities. The Lancet, 365(9464), 1099–1104. DOI 10.1016/S0140-6736(05)71146-6. [Google Scholar] [CrossRef]
62. Guilmoto, C. Z. (2009). The sex ratio transition in Asia. Population and Development Review, 35(3), 519–549. DOI 10.1111/j.1728-4457.2009.00295.x. [Google Scholar] [CrossRef]
63. Torssander, J., Erikson, R. (2009). Marital partner and mortality: The effects of the social positions of both spouses. Journal of Epidemiology & Community Health, 63(12), 992–998. DOI 10.1136/jech.2009.089623. [Google Scholar] [CrossRef]
64. Jaffe, D. H., Eisenbach, Z., Neumark, Y. D., Manor, O. (2005). Does one’s own and one’s spouse’s education affect overall and cause-specific mortality in the elderly? International Journal of Epidemiology, 34(6), 1409–1416. DOI 10.1093/ije/dyi185. [Google Scholar] [CrossRef]
65. Syrda, J. (2020). Spousal relative income and male psychological distress. Personality and Social Psychology Bulletin, 46(6), 976–992. DOI 10.1177/0146167219883611. [Google Scholar] [CrossRef]
66. Koo, A., Hui, B. P., Pun, N. (2020). Gender ideologies of youth in post-socialist China: Their gender-role attitudes, antecedents, and socio-psychological impacts. Chinese Sociological Review, 52(5), 487–514. DOI 10.1080/21620555.2020.1768366. [Google Scholar] [CrossRef]
67. Leung, A. S. (2003). Feminism in transition: Chinese culture, ideology and the development of the women’s movement in China. Asia Pacific Journal of Management, 20(3), 359–374. DOI 10.1023/A:1024049516797. [Google Scholar] [CrossRef]
Cite This Article
 Copyright © 2023 The Author(s). Published by Tech Science Press.
Copyright © 2023 The Author(s). Published by Tech Science Press.This work is licensed under a Creative Commons Attribution 4.0 International License , which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
 Downloads
Downloads
 Citation Tools
Citation Tools