
 Submit a Paper
Submit a Paper Propose a Special lssue
Propose a Special lssue Open Access
Open Access
ARTICLE

An Intervention Study of Language Cognition and Emotional Speech Community Method for Children’s Speech Disorders
Foreign Language College, Guangdong University of Science and Technology, Dongguan, 523000, China
* Corresponding Author: Yali Qiang. Email:
International Journal of Mental Health Promotion 2023, 25(5), 627-637. https://doi.org/10.32604/ijmhp.2023.025746
Received 28 July 2022; Accepted 14 November 2022; Issue published 28 April 2023
 View Full Text
View Full Text Download PDF
Download PDFAbstract
Speech disorders are a common type of childhood disease. Through experimental intervention, this study aims to improve the vocabulary comprehension levels and language ability of children with speech disorders through the language cognition and emotional speech community method. We also conduct a statistical analysis of the interventional effect. Among children with speech disorders in Dongguan City, 224 were selected and grouped according to their receptive language ability and IQ. The 112 children in the experimental group (EG) received speech therapy with language cognitive and emotional speech community, while the 112 children in the control group (CG) only received conventional treatment. After six months of experimental intervention, the Peabody Picture Vocabulary Test-Revised (PPVT-R) was used to test the language ability of the two groups. Overall, we employed a quantitative approach to obtain numerical values, examine the variables identified, and test hypotheses. Furthermore, we used descriptive statistics to explore the research questions related to the study and statistically describe the overall distribution of the demographic variables. The statistical t-test was used to analyze the data. The data shows that after intervention through language cognition and emotional speech community therapy, the PPVT-R score of the EG was significantly higher than that of the CG. Therefore, we conclude that there is a significant difference in language ability between the EG and CG after the therapy. Although both groups improved, the post-therapy language level of EG is significantly higher than that of CG. The total effective rate in EG is higher than CG, and the difference is statistically significant (p < 0.05). Therefore, we conclude that the language cognition and emotional speech community method is effective as an interventional treatment of children’s speech disorders and that it is more effective than traditional treatment methods.Keywords
Language is formed and developed by human beings in the process of social advancement. It refers to the ability to express one’s thoughts or communicate with others by various means or symbols (e.g., gestures, expressions, spoken language, and words). Language is a complex psychological activity that is only acquired by human beings. Speech disorders are a common type of childhood disease; they include all abnormalities in the usage or understanding of spoken language, words, or gestures. In general, child speech disorders refer to deviations and abnormal phenomena that hinder an individual’s ability to understand or express language compared with children of the same age [1].
Language disorders are not physiological diseases but a type of functional disorder, similar to nervous system and motor system disorders [2]. Language disorders are relatively common; according to 2012 U.S. Department of Health statistics, about 7.7 percent of American children are affected by speech disorders. By the time they reach the first grade, about 5 percent of children will have had significant speech disorders, most of which have unknown causes. In comparison to the disorders’ prevalence in the United States, the proportion of children with language disorders in China is estimated to reach 10%–20% [3]. According to an estimate in 2013 by the Hong Kong Speech Therapists Association, about 10% of children in Hong Kong are affected by speech disorders, and 20% of children require speech therapists. These statistics suggest that the number of children affected by speech disorders in China is enormous.
School-aged children affected by language barriers are disadvantaged when faced with competitive pressures from their peers. They can quickly become an especially vulnerable part of this already vulnerable group. Schoolchildren affected by speech disorders may be wrongly perceived as not working hard by their parents and the people around them. They are also easily discriminated against and isolated. These situations should arouse the attention of all of society [4]. We should provide appropriate assistance to those affected by speech disorders (mainly primary and secondary school students), protect them from discrimination, and provide timely and necessary intervention treatment.
Speech community theory is a fundamental theory in sociolinguistics. Contemporary Social Linguistics explains the concept of speech community as follows: “Speech community is a group of speakers. A specific identity within the group constitutes a difference from other similar groups. Speech community theory explains the organizational system of language users [5].” In other words, a speech community is a diverse system of organized speakers bound together by standard norms and desires. This definition shows the following:
1. A speech community is a system of speakers, not a system of language.
2. These speakers share standard norms and attitudes toward language use.
3. There is verbal interaction and communicative intensity among these speakers.
Based on the existing research on speech communities, Daming Xu has further proposed five elements of the speech community: a certain number of speakers (population), a specific range of activity areas (region), frequent speech activities between speakers (interaction), speakers with the same language attitude and language evaluation criteria (identification), and speakers sharing a language symbol system and usage norms (facilities) [6]. The research object of this theory mainly encompasses two main aspects of speech communities. First, it studies the standardization and the consistency of language attitude in language use. Second, it deconstructs the internal structure of the speech community and analyzes whether it has order. Compared with sociology, the “community” of linguistics reflects the ordinary norms of language use, including the interaction and identification of speakers [7].
Based on the theory of speech communities, this study will comprehensively analyze the speech characteristics of children with speech disorders. In addition, it will attempt to treat children with speech disorders using language cognition and emotional speech therapy to explore this approach’s curative effect.
2.1 Foreign Studies on Language Intervention for Speech Disorders
Research on speech disorders can be traced back to Mesopotamian times around 3500 BC. However, the study of language disorders from the linguistics perspective began in the 1920s with the British neuroscientist Head’s systematic linguistic analysis of aphasia caused by local brain injury [8]. Later, Jakobson, a famous linguist, used clinical data to study children’s verbal communication disorders in 1941, pioneering the study of language therapy for speech disorders by European and American scholars. Speech and language disorders remained primarily a medical concern until the 1970s. However, in the late 1970s and early 1980s, a series of studies by Crystal and her team laid the foundation for language therapy for speech disorders [9].
Since the 1980s, more and more studies have examined language therapy for children with speech disorders. Researchers have investigated how children learn to find topics, take turns talking, and repair the ability to prolong the conversation. Fage et al. found that speech-impaired children only directly respond to questions but do not make statements or comments on declarative sentences [10]. Lee and other researchers used a 28-page book of objects to get children with speech disorders to tell a story to a listener who had not heard the story before [11]. In the picture book scenario, children with speech disorders use causal language and internal state vocabulary similar to other children. Still, they needed help to identify the cause of the task’s internal state.
Until the 1990s, researchers focused on the development process of children’s language communication behavior. In particular, they explored how children acquired the necessary knowledge and skills in language development while using language appropriately, effectively, and normatively in interaction. Since the 1990s, speech disorder research in children has focused instead on pragmatic disorders. The main problem of their language development is acquiring the ability to use language effectively in social situations [12]. While much research has investigated the language of children with speech disorders in the international context, the topic is still worthy of further exploration.
2.2 Chinese Studies on Language Intervention for Speech Disorders
Compared with the vigorous development of language therapy for speech disorders abroad, research on Chinese speech disorders in China is just starting. Since the 1990s, scholars in neurolinguistics, language acquisition, pragmatics, and speech rehabilitation have begun to pay attention to language disorders, including via linguistic research on Chinese children’s speech disorders [13].
In terms of treatment and intervention methods, the relevant Chinese literature is as follows:
The researchers evaluate the individual situation of children with speech disorders and then formulate the learning goals and treatment plans according to the children’s individual situations [14]. In the process of treatment, the researchers exercise the articulatory organs of children with speech disorders through massage, oral exercises, and breathing training, and use games to attract children’s interest and promote language learning [15]. Research also suggests that we should fully use children’s visual ability with the Picture Exchange Communication System (PECS) to enhance children’s ability to understand language [16]. When communicating with children with speech disorders, methods such as eye contact should be adopted to fully arouse their attention [17]. At the same time, attention should be paid to the use of existing situations to communicate with children and the creation of environments where children can use language in life situations, thus helping children understand the relationship between language and environment and promoting their language learning [18]. Moreover, researchers should seek to create a highly structured communication environment; as children are more adapted to such environments, they make language development more accessible [19].
A review of the literature on language intervention for children’s speech disorders shows that these studies have produced significant achievements. However, the existing studies have mainly focused on language structure, ignoring children’s natural communicative intentions and emotions. Due to congenital barriers to verbal communication, some children cannot acquire language naturally. They can only express their communicative intentions in alternative ways, such as cards, gestures, imitation repetitions, or stereotyped speech. Therefore, language intervention should respect children’s communicative intentions and emotions, create an environment to stimulate spontaneous expression, and provide opportunities for voluntary expression.
Many studies have explored interventions for children’s language disorders. However, so far, there have been few empirical studies on children’s Chinese language disorders using speech community theory combined with language cognition and emotion to treat children’s language disorders. On the one hand, the language cognition emotional speech community method is targeted and conforms to the characteristics of the community groups of children with speech disorders. On the other hand, considering children’s cognitive and communicative intentions and emotions provides a meaningful, predictable, understandable, and low-pressure expression environment for children with speech disorders, which has obvious advantages for interventions. Therefore, this study endeavors to combine the two perspectives to explore the effectiveness of the combined approach in improving the language ability of children with speech disorders.
In language learning, there are two types of psychological processes involved in speech activities. The first is cognition (intellectual factors), such as perception, understanding, imagination, thinking, and memory. The second is emotion (non-intellectual factors), such as motivation, attitude, interest, emotion, and will. Both factors play a positive role in children’s word context creation or scene processing—that is, in strengthening the unity of word cognition and emotion activation cognition [20]. The creation of perceptual scenes enables the repetition and reuse of language knowledge and activates cognition with the processed language scene. Moreover, cognition and emotion interact with each other during learning, and emotion strengthens cognition and promotes the development of cognitive ability. Suppose language therapy for children with speech disorders can achieve the mutual promotion, complementation and infiltration of cognition and emotion and the unification of emotion and cognition. In that case, language therapy will be more effective. Therefore, this study uses the language cognitive emotion method based on speech community theory to treat children with speech disorders.
The research design of the present study includes the research objective, hypotheses, subjects, methods, instruments, and process.
Through experimental intervention, this study aims to improve the vocabulary comprehension levels and language ability of children with speech disorders through the language cognition and emotional speech community method. It also aims to provide a statistical analysis of the interventional effect.
In this study, the researcher will test the following null hypotheses at the 0.05 level of significance:
1. There is no significant difference in pre-test scores of PPVT-R between the experimental group (EG) and the control group (CG) before the treatment.
2. There is no significant difference in post-test scores of PPVT-R between the EG and CG after the treatment.
The researchers selected and grouped 224 children (aged 3–6 years) with speech disorders from the Xiangrihua Rehabilitation and Training Center in Dongguan City according to their receptive language ability and IQ. The S-S method diagnosed all the children with language development disorders; this method met the diagnostic criteria for delayed language development. The researchers informed the children’s families of the study.
In this study, the researchers selected and grouped 224 children with speech disorders according to their receptive language ability and operation IQ, including 112 in the EG and 112 in the CG. In the CG, the mean age is (3.1 ± 0.6) years, and there are 75 males and 37 females. In the EG, the mean age is (3.0 ± 0.8) years, and there are 72 males and 40 females. There is no significant difference in the general data between the two groups (p > 0.05), indicating that they are comparable.
CG received traditional primary treatment, including motion treatment, massage, cognitive function rehabilitation training, orthosis, brain circulation, nerve-muscle electric stimulation, and percutaneous nerve electric stimulation. In EG, the researchers applied language cognitive and emotional therapy based on speech community theory; this treatment mainly included language cognitive rehabilitation training and emotional intervention. All treatments took place from January to August 2019.
3.4.1 Language Cognitive Rehabilitation Training
Schell language training stimulation therapy was adopted to conduct one-to-one rehabilitation training for children’s hearing, speech, language expression, and daily communication skills. This treatment mainly included the following training:
Auditory stimuli: By listening to the radio, watching TV, reading newspapers, and listening to music and other forms of media, children with speech disorders focus their attention, stimulate thinking, and train their listening comprehension and ability to understand text. They are repeatedly provided language signals and given auditory language stimulation and feedback of generated responses, thereby strengthening the correct response to promote listening comprehension and reading comprehension ability.
Speech construction training: In this training type, children with speech disorders control the movements of the tongue, lips, teeth, soft palate, throat, and mouth muscles through sound and mouth shape and observe the position of the construction organs by looking at the shape of the mouth. Language trainers correct the children’s pronunciation movement and train their volume, pitch, language clarity, and speed; they coordinate with the body movement and correct unclear pronunciation whenever it occurs. In addition, the researchers instruct children to clear their throat, drum their cheeks, flex their tongue and whistle, and use their mouth muscles to perform pronunciation transformation training, prolong the pronunciation time, and increase rhythm and volume. Language trainers also train children to follow or read aloud characters, phrases, and short and long sentences.
Language expression training: This type of training stimulates children’s vision through toys, pictures, or videos and reminds children through mouth movements to improve their language expression ability. At the same time, the researchers also instruct children to imitate the mouth shape of pronunciation.
Daily communication skills training: For eating, drinking, sleeping, walking, and other phrases in daily life, language trainers help children with language-assisted gesture training, deepening the children’s understanding of the phrases and their pronunciation. Communicating more with children increases their vocabulary and memory and improves their language expression ability. Moreover, offering children complete patience and support encourages them to take the initiative to participate in language training. Furthermore, trainers seek to encourage the progress made and give children the confidence to persist in training.
Emotional support enables children to establish confidence in learning. Therefore, researchers analyze children’s psychological and emotional characteristics to carry out the targeted intervention.
In the process of language training, researchers adopt encouragement strategies. No matter how weak a child’s ability, he or she also has a “strong point.” Accordingly, language trainers give timely affirmation and encouragement and constantly strengthen their identification with the psychological rewards of discovery. No action is too small to be rewarded. As long as the behavior is positive, trainers should praise children with phrases like “good job!” “you’re good at this!” or “you’re great!”
For children with delayed language development, language trainers appropriately lower the standards so that children can succeed and gain confidence from successful experiences that are not difficult to achieve. When a child makes a small amount of progress, language trainers must exaggerate their response because it takes work for the child to progress. The trainer’s praise can mobilize positive factors in the child’s psychology so that the child expects excellent progress.
In addition, this treatment group fully mobilizes the emotional care of the family to understand the children, mobilize communication between them, encourage effective treatment of children to exchange experiences, enhance confidence in the treatment, and apply games and music therapy to relax the treatment atmosphere and make it comfortable and pleasant.
The main instruments used in the study comprise the Wechsler Preschool and Primary Scale of Intelligence (WPPSI) and Peabody Picture Vocabulary Test-Revised (PPVT-R).
3.5.1 Emotional Intervention Wechsler Preschool and Primary Scale of Intelligence (WPPSI)
The Wechsler Preschool and Primary Scale of Intelligence (WPPSI), developed by Wechsler, is one of the world’s most widely used scales of individual intelligence. It is suitable for children aged 3–7. The researchers design the measurement’s selected materials, project arrangement, and measurement methods according to the corresponding age norms.
Professor Zhang Houcan of Beijing Normal University revised the Chinese version of the WPPSI used in this study. It consists of language and operation tests, and the intelligence quotient is converted from the original score to a scaled score. WPPSI comprises three intelligence quotients: Verbal IQ (VIQ), Performance IQ (PIQ), and Full IQ (FIQ). In the context of speech disorders, researchers mainly use operational intelligence (PIQ) [21].
Relevant studies have shown that IQ significantly impacts children’s language disorders, and children with different IQ levels will present different levels and types of speech disorders. Therefore, in this study, children with speech disorders were matched and grouped according to their cognitive level and language status in cognition to avoid interference caused by IQ differences in the effect of speech therapy.
3.5.2 Peabody Picture Vocabulary Test-Revised (PPVT-R)
The Peabody Picture Vocabulary Test (PPVT) is one of the most influential tests for assessing children’s language ability. L. M. Dunn, an adjunct professor of special education at the University of Hawaii, initially compiled it. A revised version of the scale, PPVT-R, was published in 1981. Peabody Picture Vocabulary Test-Revised (PPVT-R) contains 175 sets of pictures and 350 words. Then, it forms two sets, each with 175 pairs (picture–vocabulary). Due to the limited form of picture–word matching, these are mainly nouns, verbs, and descriptive words. PPVT-R tests children’s receptive vocabulary ability in the form of finger-pointing to reflect their language ability.
Relevant studies have shown that children’s language level significantly correlates with their receptive language ability. In the present study, the revised Chinese PPVT-R, which the scholar Biao Sang revised in 1990, was used to measure the receptive language ability of children with speech disorders, and the test results were statistically analyzed. Biao Sang revised PPVT-R according to formula L and formulated the trial norm for normal children in the Shanghai urban area. In terms of vocabulary, the revised Chinese version of PPVT-R maintains the meanings and parts of the original English words while trying to conform to the language habits of Chinese children [22]. In terms of picture matching, screening was performed mainly by redrawing the pictures that Chinese children had never seen, which were easily confused with Chinese words or with foreign features.
In PPVT-R, there are four pictures in each group, and the tester must present the pictures in turn and say a matching word to determine the test’s starting point. The subject must point out a picture with the same meaning as the word from the four pictures. If the picture that the subject points out is consistent with the answer, the score is 1; otherwise, the score is 0. The test is simple and engaging, and it is often used to test the language ability of children with speech disorders. In addition, the test score is objective and fast, and it has high reliability and validity [23].
Based on speech community theory, we examined the speech used in the group of children with speech disorders and comprehensively analyzed their speech characteristics as follows. Children’s speech disorders manifest as abnormal pronunciation—that is, unclear speech. Specifically, disorders cause abnormal tone and fluency problems related to loudness, tone quality, and resonance. Pauses, repetitions, prolongations, and obstacles characterize oral fluency problems in children with speech disorders. Such children understand language correctly but express it with incredible difficulty.
According to the language characteristics of the children with speech disorders, we selected 224 children with speech disorders for this study. Based on their receptive language ability and operational intelligence quotient, 112 children were in the experimental group and 112 in the control group. The intervention objectives of this experiment were language cognitive rehabilitation training and emotional intervention. The research procedure comprises five stages:
1. The researchers selected and grouped 224 children with speech disorders according to their actual physiological age, IQ, and receptive speech ability.
2. During the pre-test period, the researchers conducted language assessment tests for the experimental and control groups to verify whether the children in the two groups had the same level of linguistic ability.
3. In the experimental period, the children in the experimental group were given speech therapy with language cognition, emotional, and speech community treatments, while the control group only received conventional primary therapy.
4. Post-test period: After the end of the treatment, the language assessment test was conducted again for the two groups. The researchers designed the post-test to test whether there was a significant difference in language ability between the experimental and control groups after the 8-month language therapy experiment.
5. Data analysis: A statistical t-test was conducted to analyze the data.
After the measurement of the Performance IQ and receptive speech ability of children, all 224 children with speech disorders were tested through PPVT-R to evaluate the children’s vocabulary, which responded to language ability. We compared the PPVT-R scores of all 112 children in the experimental group and 112 children in the control group with a two-sample t-test. The results of the t-test of the PPVT-R pre-test scores of the EG and CG are as follows (Table 1):
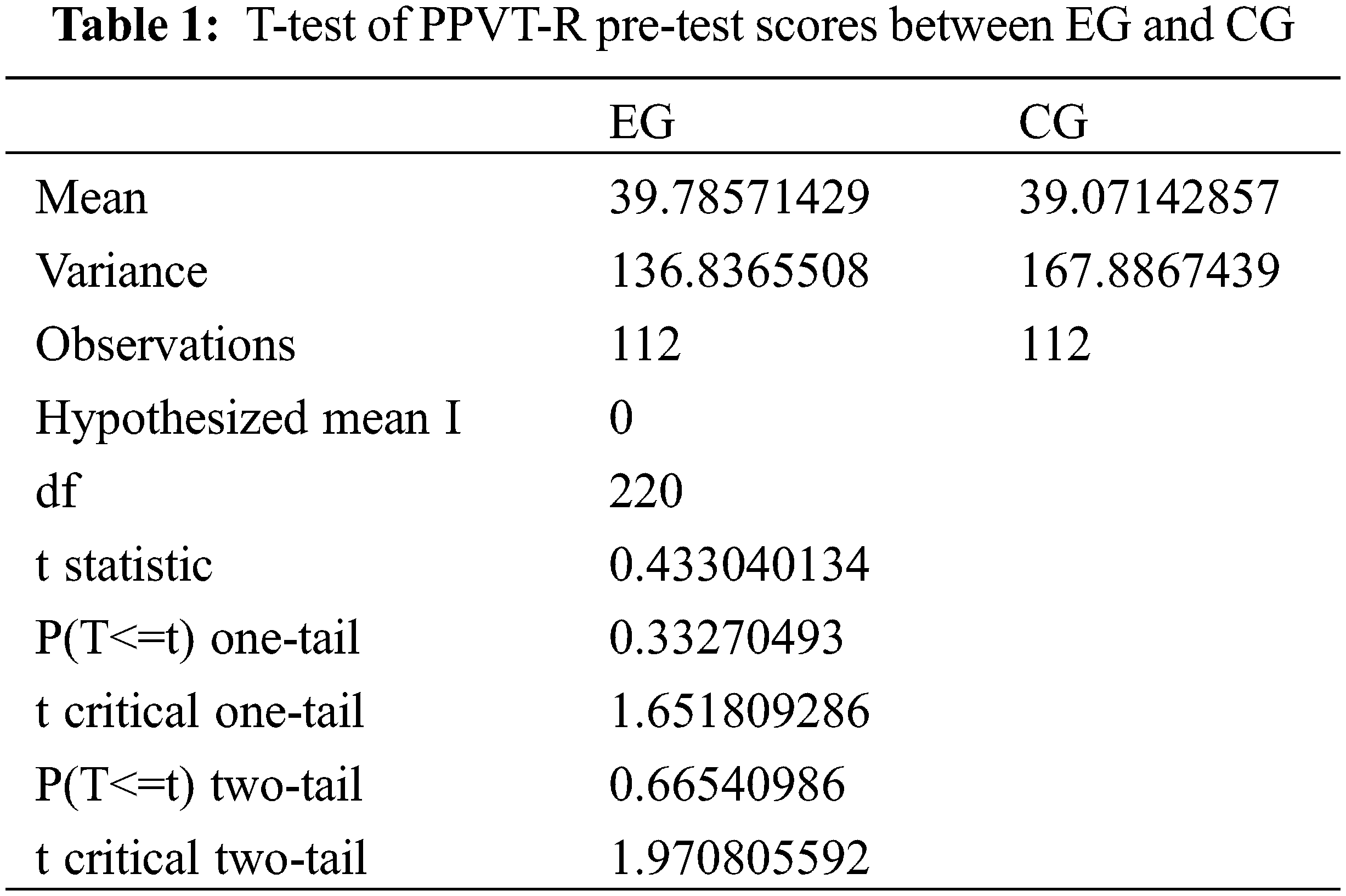
From Table 1, we can perform the following data analysis with significance level alpha = .05.
Because the t statistic (0.43) < T critical two-tail (1.97), T is not significant. Therefore, the null hypothesis is accepted, and there is no significant difference in pre-test scores of PPVT-R between the EG and CG before the treatment. Therefore, before the experiment, the language abilities of the EG and CG were at essentially the same level, which met the requirements of the experimental design of the peer group in this study.
After an eight-month language therapy experiment, we compared the PPVT-R post-test scores of EG and CG to analyze whether there was a significant difference in language ability. Table 2 shows the t-test of the PPVT-R post-test scores of the EG and CG:
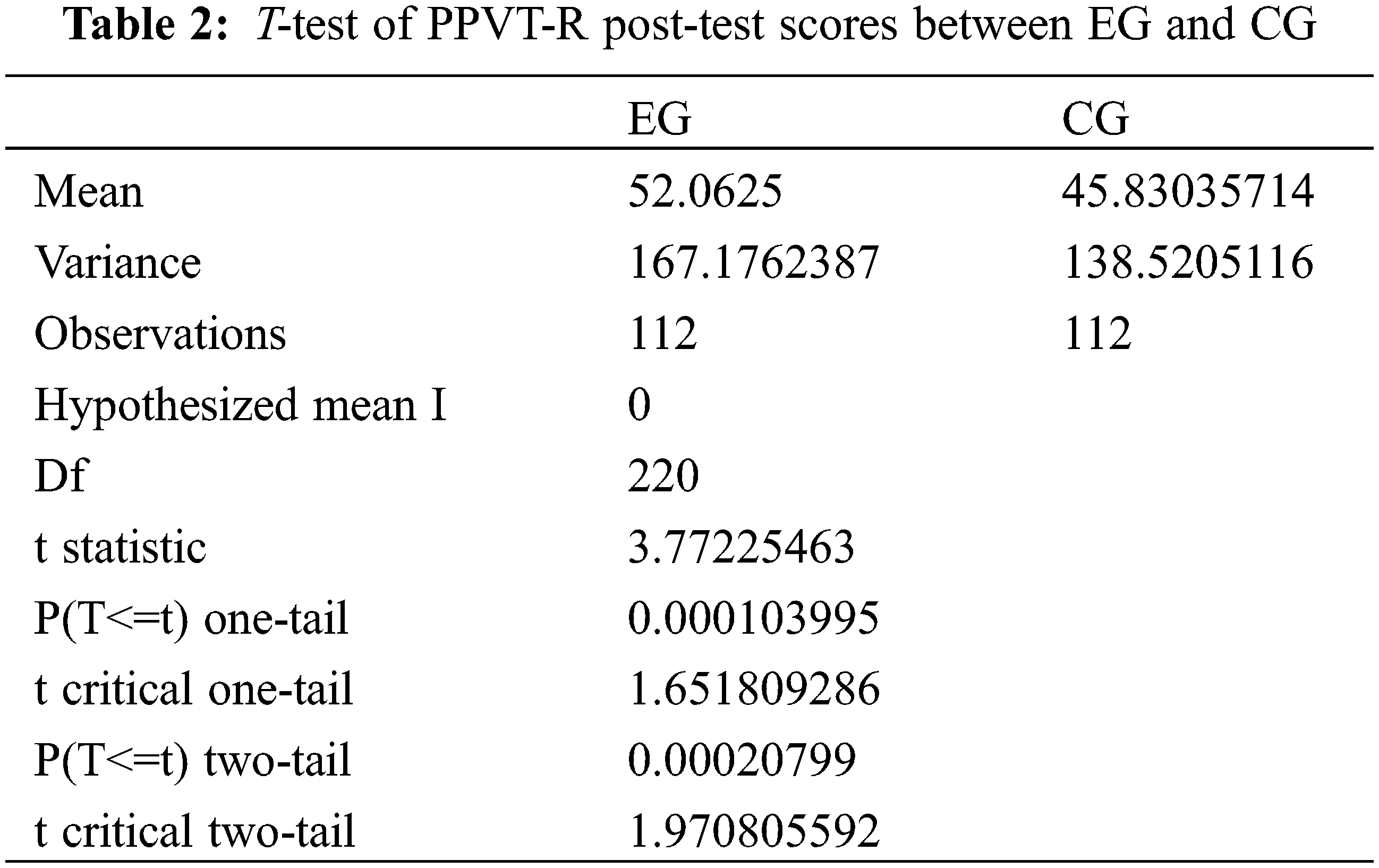
From the above table, we can perform the following analysis with significance level alpha = .05.
Since the t statistic (3.77) > T critical two-tail (1.97), T is significant. We reject the null hypothesis and accept the alternative hypothesis: there is a significant difference in PPVT-R post-test scores between EG and CG. The test mean of EG is 52.06, while the mean score of CG is 45.83. The test accuracy of EG is 87.4%, while the accuracy of CG is 73.2%. This shows that after the language cognition and emotional speech community therapy, the PPVT-R score of EG is significantly higher than that of CG. Therefore, there is a significant difference in language ability between EG and CG after the therapy. Although both groups improved, the language level of EG is significantly higher than that of CG. The total effective rate in EG was higher than in CG, and the difference is statistically significant (p < 0.05).
Therefore, we can apply the language cognition and emotional speech community method in treating children’s speech disorders, and it is more effective than the traditional treatment.
Speech disorders mainly include articulation, speech fluency, affective communication, and hearing disorders. The main clinical manifestations of speech disorders are respiratory abnormalities, heavily nasal pronunciation, abnormal pronunciation rhythm, abnormal pronunciation speed, abnormal tone, unclear pronunciation, inaccurate pronunciation, and phonation difficulty. Salivation and mastication difficulties can also occur. Speech disorders cause children to lose their primary communication function and severely affect their future life and learning [24].
This study’s results show a significant difference between EG and CG in the language ability of the PPVT-R post-test after the treatment. The accuracy rate of EG is 87.4%, while that of CG is 73.2%. The total effective rate of the EG is higher than that of the CG, and the difference is statistically significant (p < 0.05). These results suggest that language cognition and emotional speech community therapy can significantly improve children’s language ability.
It is difficult for children with speech disorders to express their ideas and needs due to their particularity, and these children’s emotional needs are often ignored. Accordingly, emotional intervention can improve the symptoms of children’s speech disorders. This, in turn, can improve children’s confidence in treatment by understanding patients’ psychological demands and ideas, adjusting destructive psychological emotions, and giving positive feedback.
Overall, the present study’s language cognition and emotional speech community therapy method has achieved good results. Based on the speech community theory, it comprehensively analyzes the speech characteristics of children with language disorders and, on this basis, implements language cognitive rehabilitation training combined with emotional intervention for the children [25]. The reason is that language cognition and emotional speech community therapy can fully stimulate children’s sensory organs while coordinating with the implementation of staged symbolic language understanding and expression. This improves the children’s communication ability and attitude, enhancing their language expression, understanding, and cognitive ability.
In conclusion, we can adopt the language cognition and emotional speech community method in treating children’s speech disorders, and its curative effect is stronger than traditional treatment methods.
However, some areas for improvement still exist, including the practical intervention ability of the researchers. Before the intervention, although the researchers had carefully prepared the intervention process and possible treatment measures, there were some obstacles in the actual intervention process due to the researchers’ limited intervention experience and ability. Based on these issues, the following recommendations may be helpful for future studies:
1. Before the intervention, the researchers should contact the subjects more, understand the characteristics of the subjects in detail, and increase the types of intervention content.
2. The interveners should focus on lively intonation and easy-to-understand, vivid, and enjoyable language.
3. The interveners should maintain positive emotions, use more encouraging language, and recognize and interact positively with the children.
Funding Statement: The author received no specific funding for this study.
Conflicts of Interest: The author declares that they have no conflicts of interest to report regarding the present study.
References
1. Zhou, H., Xiong, C. (2019). Etiology analysis of 515 children with speech and language disorders. Journal of Audiology and Speech Diseases, 27(5), 477–481. [Google Scholar]
2. Lin, B. (2014). Intervention therapy for speech disorders. China: Science Press. [Google Scholar]
3. Black, L. I., Vahratian, A., Hoffman, H. J. (2015). Communication disorders and use of intervention services among children aged 3–17 years: United States, 2012. NCHS Data Brief. Number 205. Hyattsville, MD: National Center for Health Statistics. [Google Scholar]
4. Liang, D. (2017). An introduction to language disorders of children. Beijing, China: The Commercial Press. [Google Scholar]
5. Taylor, L., Whitehouse, J. J, A. (2017). Autism spectrum disorder, language disorder, and social (pragmatic) communication disorder: Overlaps, distinguishing features, and clinical implications. Australian Psychologist, 51(4), 287–295. https://doi.org/10.1111/ap.12222 [Google Scholar] [CrossRef]
6. Wan, P. (2012). Speech therapy. China: People’s Medical Publishing House. [Google Scholar]
7. Liang, D. (2018). Research on language disorders and acquisition of children. China: Nanjing Normal University Press. [Google Scholar]
8. Zhou, T. (2014). A study on language theory and language disorder. China: China Social Sciences Press. [Google Scholar]
9. Guo, T. (2015). Intervention research on communication ability of autistic children (Master Thesis). Shanghai Normal University, China. [Google Scholar]
10. Zheng, Q., Shen, M., Wu, Y. (2018). Effect of individual training combined with group games on speech disorders in children with cerebral palsy. Journal of Audiology and Speech Diseases, 26(4), 379–382. [Google Scholar]
11. Li, S. (2018). Research on the intervention in the lexical comprehension disorders of autistic children by semantic and context matching design (Master Thesis). Nanjing Normal University, China. [Google Scholar]
12. Zhang, J. (2018). Clinical intervention of expressive language disorder in children. Journal of Chinese Practical Neuropathy, 11(24), 18–20. [Google Scholar]
13. Phan, T. (2018). Out of loneliness: A study on the classification, assessment and rehabilitation of language disorders in children (Ph.D. Thesis). Jilin University, China. [Google Scholar]
14. Cui, G. (2015). Neurolinguistics. China: Tsinghua University Press. [Google Scholar]
15. Li, X. (2016). A review of language development in children with autism. Special Education in China, 14(12), 38–43. [Google Scholar]
16. Li, H., Du, Z. (2016). The intervention study on picture exchange communication system on the active communication behavior of preschool autistic children. Special Education in China, 17(3), 68–72. [Google Scholar]
17. Yuan, H. (2017). A review of structured teaching for children with language disorders. Modern Special Education, 10(7), 54–59. [Google Scholar]
18. Tan, X. (2018). Chines communication development manual. China: Peking University Medical Press. [Google Scholar]
19. Liang, D. (2018). Language disorders and acquisition in children (Master Thesis). Nanjing Normal University, China. [Google Scholar]
20. Fromkin, V., Rodman, R., Hyams, N. (2014). An introduction to language. 10th edition USA: Cengage Learning. [Google Scholar]
21. Korkiakangas, T. (2018). Communication, gaze, and autism: A multimodal interaction perspective. UK: Psychology Press. [Google Scholar]
22. American Psychiatric Association (2013). Diagnostic and statistical manual of mental disorders. 5th edition USA: American Psychiatric Pub. [Google Scholar]
23. Du, Q., He, H. (2019). Problems related to language and social communication in children with autism spectrum disorders. Chinese Journal of Practical Pediatrics, 34(8), 632–637. [Google Scholar]
24. Liu, X. (2019). Language disorders and language assessment in children. Chinese Journal of Hearing and Speech Rehabilitation, 17(3), 161–165. [Google Scholar]
25. Cheng, Y. (2016). The effectiveness of the lego therapy intervention in promoting the social interaction of children with autism spectrum condition in the playground: An evaluation study (Master Thesis). UK University College London, UK. [Google Scholar]
Cite This Article
 Copyright © 2023 The Author(s). Published by Tech Science Press.
Copyright © 2023 The Author(s). Published by Tech Science Press.This work is licensed under a Creative Commons Attribution 4.0 International License , which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
 Downloads
Downloads
 Citation Tools
Citation Tools