
 Submit a Paper
Submit a Paper Propose a Special lssue
Propose a Special lssue Open Access
Open Access
ARTICLE

What Is the Psychosocial Environment of Adolescents with High or Low Internalizing Behavior?
Department of Social Welfare, Inha University, Incheon, 22212, Republic of Korea
* Corresponding Author: Changmin Yoo. Email:
International Journal of Mental Health Promotion 2025, 27(1), 77-88. https://doi.org/10.32604/ijmhp.2025.058577
Received 15 September 2024; Accepted 20 December 2024; Issue published 31 January 2025
 View Full Text
View Full Text Download PDF
Download PDFAbstract
Objective: This study aimed to examine the developmental trajectories of internalizing behaviors among adolescents and to identify key personal and environmental factors associated with these developmental patterns over time. Methods: Data were collected from 2242 adolescents (49.6% girls, aged 13.9–18.9 years) in South Korea. Latent class growth analysis was used to identify distinct developmental patterns of internalizing behaviors. Multinomial logistic regression analyses were conducted to examine the associations between these developmental patterns and various factors including gender, self-esteem, abuse and neglect experiences, peer relationships, and media use. Results: The analysis revealed three latent classes of internalizing behavior trajectories among adolescents. The first group, the “mid decreasing group”, comprised 54.5% of the sample (1221 students), indicating a moderate level of internalizing behavior that declined over time. The second group, the “high decreasing group”, included 19.1% of the sample (429 students), characterized by initially high levels of internalizing behavior that decreased. The third group, the “low maintained group”, represented 26.4% of the sample (592 students), indicating consistently low levels of internalizing behavior. Factors such as gender, self-esteem, experiences of abuse and neglect, peer relationships (trust and alienation), smartphone dependency, and time spent watching TV/videos were significantly associated with these latent groups. Conclusion: Three distinct developmental patterns of internalizing behaviors were identified among adolescents: mid-decreasing (54.5%), high-decreasing (19.1%), and low-maintained (26.4%). Gender, self-esteem, abuse experiences, and peer relationships were significant predictors of these developmental patterns.Keywords
Internalizing refers to a passive, socially internalized, over-controlled condition characterized by symptoms such as anxiety, depression, and social withdrawal [1]. While moderate emotional responses to stress are normal in human development, excessive internalizing behaviors can indicate difficulties in stress management. Previous studies have documented the negative impacts of excessive internalizing behavior [2,3]. These studies demonstrate that internalizing behavior negatively affects mental health [3] and can lead to chronic psychosocial difficulties in adulthood [4]. Such behavior is particularly prominent during adolescence, a transitional period from childhood to adulthood marked by various developmental challenges [5]. Additionally, adolescents may struggle with emotion regulation due to the incomplete development of the frontal lobe [6].
Several studies have examined adolescent internalizing behavior across different cultures [7,8]. Research during the COVID-19 pandemic found that preschool attendance, parental stress levels, and parents’ mental health significantly influenced children’s behavioral problems. Higher parental stress and poorer parental mental health correlated with increased internalizing and externalizing problems in preschool children, while continued preschool attendance showed protective effects [7]. A study of UK adolescents aged 7 to 15 identified various trajectory patterns, with gender and early-life risk factors as significant predictors [8]. Research involving 1298 adolescents aged 8 to 14 from 12 cultural groups revealed that parental warmth and behavioral control influenced externalizing and internalizing symptoms differently across cultures [9]. Gong et al. identified gender-specific developmental trajectories among Chinese youth, finding four distinct patterns for boys and three for girls [10].
These studies indicate that internalizing behavior levels vary across early, middle, and late adolescence. Research tracking children from age 3 through 10, with follow-up assessments at age 19, examined developmental trajectories [11], while Leve et al. observed increased internalizing levels between ages 5 and 17 [12]. Key predictors of these trajectories included gender, self-esteem, parental supervision, and peer relationships [13–17]. Hsieh and colleagues identified adolescent stress as a risk factor for emotional and behavioral problems [18].
While previous research has identified risk and protective factors for internalizing behavior through variable-oriented studies [13–16], this approach may overlook heterogeneous subgroups within the population. Different latent groups may exist beyond the population mean, each requiring distinct intervention methods and goals.
This study examines changes in internalizing behavior among Korean adolescents using a person-centered approach through latent class growth analysis (LCGA), rather than the conventional longitudinal growth model. By identifying subgroup characteristics through LCGA, this research aims to provide practical recommendations for preventing and reducing adolescent internalizing behavior.
Factors related to internalizing behavior
Our research is grounded in ecological systems theory [19], which provides a comprehensive framework for understanding how various environmental systems influence individual development. Within this framework, we focused on the onto-system (individual characteristics) and microsystems, particularly examining how interactions between individuals and their immediate environments (family and school) relate to internalizing behaviors among South Korean adolescents. The factors influencing adolescent internalizing behavior can be categorized into four main domains: individual, family, school/academic, and electronic media factors.
Individual factors encompass gender, self-esteem, and sleep patterns, all of which significantly influence adolescent internalizing behavior [15,20]. Research consistently shows that females exhibit higher levels of internalizing behavior [21], with Olivier et al. documenting notably higher initial scores on internalizing behavior scales among female participants [17]. Self-esteem plays a crucial role, as demonstrated by Mileviciute et al.’s comprehensive study of youth in the Americas, which revealed a significant inverse relationship between self-efficacy and depression levels [15]. Additionally, sleep quality emerges as a critical factor, with Quach et al.’s research establishing that adolescents experiencing sleep difficulties show elevated depression levels [20].
Family factors, particularly household income and experiences of abuse or neglect, significantly impact internalizing behavior [11,13,14,21]. Multiple studies have confirmed that adolescents from low-income households demonstrate markedly higher levels of internalizing behaviors, including depression, social withdrawal, destructive behavior, and hyperactivity, compared to their peers from higher-income families [21,22]. Parenting attitudes also play a crucial role in shaping internalizing behaviors. Lee et al.’s longitudinal research revealed that negative parenting practices at age 6, including negative behavioral appraisals, caregiving inefficacy, unresponsiveness, and physical punishment, predicted higher levels of depression and anxiety symptoms at age 19. These effects persisted even after controlling for prior internalizing symptoms, highlighting the enduring impact of early parenting experiences [7]. This finding is consistently supported by various studies demonstrating the significant relationship between parenting attitudes and children’s internalizing behavior levels [11,13,14].
School and academic factors, encompassing peer relationships, teacher support, and academic stress, form another crucial domain. Adolescents who experience peer rejection [16,23], receive lower teacher support [24], or face higher academic stress [25] show increased probability of developing internalizing behaviors. The significance of peer and teacher relationships is particularly pronounced during adolescence, as students spend substantial time in school environments. Morales et al. [16] and other researchers [23] have documented the substantial impact of peer relationships on both internalizing and externalizing behavior levels. While many studies indicate that higher teacher support correlates with lower problem behaviors [24], some research suggests that teacher support may not significantly affect adolescents’ psychological and psychopathological factors [26]. Högberg et al.’s research revealed a strong negative association between academic achievement and internalizing disorders, with low-achieving students showing disproportionately high risks of anxiety and mood disorders. This relationship may be attributed to educational stressors, including fear, stigma, and shame associated with academic failures, as well as distress from potential educational exclusion. Hsieh et al.’s findings further support this, identifying adolescent stress as a significant risk factor for emotional and behavioral problems [18].
The final domain concerns electronic media factors, particularly smartphone dependency and time spent using computers, television, and games [27,28]. Perrino et al.’s analysis of U.S. Hispanic adolescents revealed a positive correlation between sedentary behaviors, especially smartphone use, and internalizing behavior [27]. Multiple studies examining adolescents’ internet and video game usage patterns have established that online gaming and internet addiction significantly predict internalizing behavior [29]. These findings underscore the importance of considering digital media consumption in understanding adolescent behavioral patterns.
The current research aims to discover the change trajectory latent class of the adolescents’ internalizing behavior, as well as identifying the predictors associated with each latent class. The following are the research questions:
Hypothesis 1: The latent group of adolescents exhibits distinct trajectories in internalizing behavior changes over time.
Hypothesis 2: Specific variables significantly influence the latent class of adolescents’ internalizing behavior change trajectories.
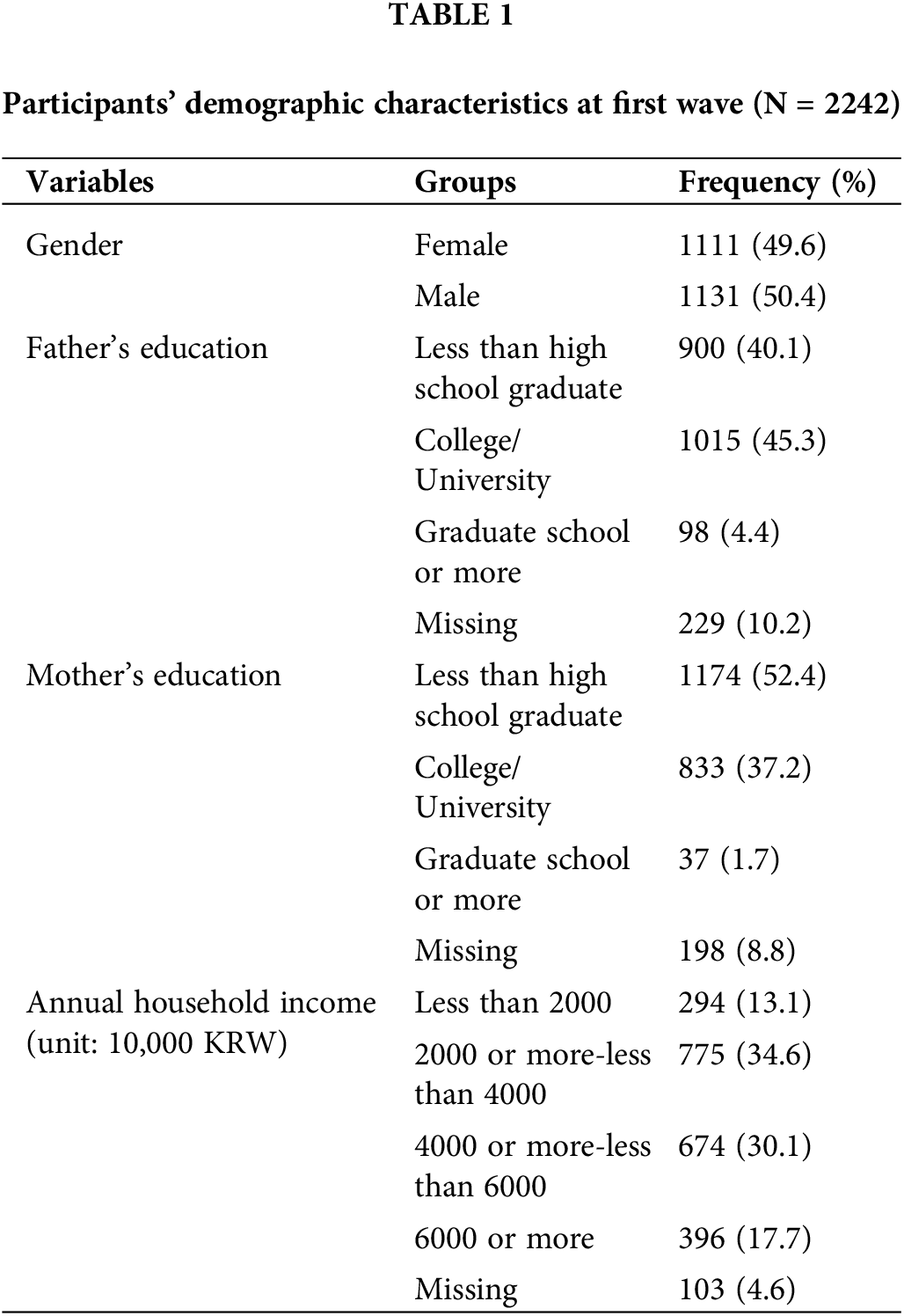
In order to address the main research questions of this study, data from the Korea Children and Youth Panel Survey (KCYPS) collected by the Korea Youth Policy Institute were utilized for the 3rd (2012), 4th (2013), 6th (2015) and 7th (2016) of the seventh-grade cohort. In 2010, the National Youth Policy Institute of South Korea conducted the KCYPS, which is a nationally representative longitudinal panel study. The survey employed a stratified multistage cluster sampling method, collecting data from middle school students across 17 cities and provinces in South Korea. This comprehensive sampling approach covered both urban and rural areas, ensuring proportional representation of different geographic regions and socioeconomic backgrounds. The sampling design supports the generalizability of our findings to the broader population of South Korean adolescents. This study included 2242 adolescent (Mean age = 13.9–18.9 years; 49.6% girls) who responded to the question of internalizing behavior in the third year’s survey. The participants were 9th graders (2012), 10th graders (2013), 12th graders (2015), and first year after graduating high school (2016). The reason why the 11th graders in 2014 (Time 3) wave of the data was not used is that the internalizing behavior was not measured in the wave. The attrition rate of the initial sample was 7.1%, 9.5%, 17.0%, and 20% for each year. Table 1 provides the demographic descriptive statistics of the study participants.
The internalizing behavior was measured using three subscales: physical symptoms, social withdrawal, and depression. Physical symptoms were assessed using eight items (e.g., “My stomach hurts when I study”) from the modified version of the Emotional or Behavioral Problems Scale [30]. Social withdrawal was measured using five items (e.g., “It is uncomfortable if there are many people around”) from Kim S-H and Kim K-Y’s measurement [31]. Depression was assessed using 10 items (e.g., “Feel unhappy or depressed”) from the revised version of psychiatric diagnosis [32]. Each item was scored on a scale of one (never true) to four (always true), with higher scores indicating higher levels of internalizing. The Cronbach’s alpha coefficients in the current study ranged from 0.917 to 0.935. The validation studies [33] of these scales demonstrated good construct validity through confirmatory factor analysis (CFI = 0.907, IFI = 0.907, RMSEA = 0.067).
Individual factors: gender, self-esteem, sleep duration
To measure demographic and individual characteristics, several variables were assessed. Gender was coded dichotomously, with male coded as 0 and female as 1. Self-esteem was measured using the Korean translated version of Rosenberg’s Self-Esteem Scale [34]. The scale consists of 10 items, including statements such as “I am as valuable a person as others,” “I have a lot of talent,” “I am satisfied with myself,” “I felt like a loser,” “I don’t have anything to boast about,” “I often feel useless.” Responses were recorded on a four-point Likert scale ranging from 1 (never true) to 4 (always true). Higher total scores indicate greater levels of self-esteem. This scale has demonstrated strong psychometric properties in previous research [35], and in the current study, showed good internal consistency with a Cronbach’s alpha of 0.815. Sleep duration was calculated by measuring the time difference between reported bedtime and wake time. Participants were asked specific questions about their sleep patterns, including “Exactly at what hour (hours and minutes) do you go to bed and at what hour (hours and minutes) do you get up?” The measure incorporated both weekday and weekend sleep patterns to provide a comprehensive assessment of sleep duration.
Family factors: household income, abuse, neglect
Household income was measured as the average annual household income was used for the analysis. Parental abuse (e.g., “My parent (or caregiver) frequently leaves me with scratches and injuries”) and neglect (e.g., “My parent (or caregiver) gives suitable medical attention when I am very sick”) were both measured as continuous variables, with each scored as the mean of four items evaluated on a four-point Likert scale ranging from one (never true) to four (always true) based on measures developed by Huh [36] and Kim [37]. High scores suggest greater degree concerning abuse as well as neglect. The Cronbach’s alpha for abuse was 0.854, whereas neglect was 0.758.
School factors: peer trust and alienation, teacher-student relationship, time spent on after-school classes, homework, and other study
Peer trust (e.g., “I can express my inner sentiments with my buddies”) and alienation (e.g., “I want to create new friends rather than my present ones”) were evaluated as constant variables. Each was assessed as the mean of three questions derived from the Inventory of Parent and Peer Attachment (IPPA) scale developed by Armsden et al. [38], which has been translated into Korean. Teacher-student relationship was measured using the five items (e.g., “I feel pleased when I meet an instructor”) established by Min [39]. Each item was evaluated on a scale of One (never true) to Four (always true). A higher rating suggests a greater degree of peer trust, alienation, and teacher connection. The Cronbach’s alpha for peer trust was 0.787, peer alienation was 0.768, and teacher relationship was 0.840. In the case of study time, we asked how much time each day was allocated to after-school classes, after-school homework, and other studies.
Electronic media factors: smartphone dependency, time spent on using computers, watching TV/video, and playing games
Smartphone dependency (e.g., “I am anxious if I don’t have my cell phone”) was measured using continuous variables, and evaluated as the average of seven items adapted from Lee et al.’s measurements [29,40]. Each item was assigned a rating ranging from 1 (never true) to 4 (always true). The Cronbach’s alpha was 0.895. A greater rating suggests a higher level of smartphone reliance. In terms of time spent using electronic devices, we asked how much time each day they allocate to computers, TV/video, and games.
LCGA was utilized to address our main research question ‘identifying sub-group trajectories of internalizing behavior over the five-time point.’ Determining the number of latent classes for internalizing behavior, the k and k−1 class models were assessed using Akaike’s information criterion (AIC) [41], Bayesian information criterion (BIC) [42], the Lo, Mendell, Rubin likelihood ratio test (LMR-LRT) [43], and the entropy value [44]. Lower AIC and BIC values, higher entropy, and a significant LMR-LRT p value (<0.05) indicate a better model. The entropy index, closer to 1, shows clear class differentiation.
A logistic regression analysis was carried out using the r3 step method [45]. When analyzing latent groups, the r3 step technique considers mistakes caused by the effect of predicting variables. To compare the mean differences of crucial variables across latent classes, the Bolck, Croon, and Hagenaars (BCH) approach was utilized. Mplus 8.7 software was used for analysis.
Identifying internalizing behavior trajectory latent classes
Before determining the number of unobservable groups based on internalizing behavior changes, we performed a chi-square difference test on a linear change (chi-square = 37.489 (df = 5), CFI = 0.985, RMSEA = 0.054) and quadratic curve model (chi-square = 34.290 (df = 2), CFI = 0.985, RMSEA = 0.085) for the complete group. The null hypothesis was not rejected (chi-square difference = 3.199 (df = 3), p > 0.362), which means that there is no difference concerning the linear model as well as the quadratic model. Above all, the linear model was selected as the final model because it is simpler, has better model fit, and is more effective [46].
As the number of latent classes increased by one, both the AIC and BIC values decreased, and the LMR-LRT test was significant as well. However, in the case of class four, the LMR-LRT test was not significant (p > 0.1307). Therefore, classification into three classes (AIC = 10,060.247, BIC = 10,128.829, Entropy = 0.656, LMRT = p < 0.05, BLRT = p < 0.05) was ultimately selected. Therefore, three trajectories of perceived levels of internalizing behavior were identified.
The three identified internalizing behavior is shown in Table 2 and Fig. 1. The initial value of internalizing behavior for the whole sample (N = 2242) was 2.059 (p < 0.001) as well as linear rate of change was −0.035 (p < 0.001). The whole sample revealed a moderate level of internalizing behavior as well as a change trajectory that gradually decreased over time. Class 1 comprised 54.5% of the sample (n = 1221). The initial value of internalizing behavior for class 1 was 2.133 (p < 0.001) and the linear rate of change was −0.051 (p < 0.001). Class 1 showed a moderate level of internalizing behavior and showed a change trajectory that gradually decreased over time. Therefore, it was named “mid decreasing.” Class 2 comprised 19.1% of the sample (n = 429). The initial value of internalizing behavior for class 2 was 2.549 (p < 0.001) and the linear rate of change was −0.036 (p < 0.001). Class 2 showed a high level of internalizing behavior and showed a change trajectory that gradually decreased over time. Therefore, it was named “high decreasing.” Class 3 comprised 26.4% of the sample (n = 592). The initial value of internalizing behavior for class 3 was 1.527 (p < 0.001) and the linear rate of change was −0.004 (p > 0.05). Class 3 showed a low level of internalizing behavior and showed a change trajectory that remained the same over time. Therefore, it was named “low maintaining.”
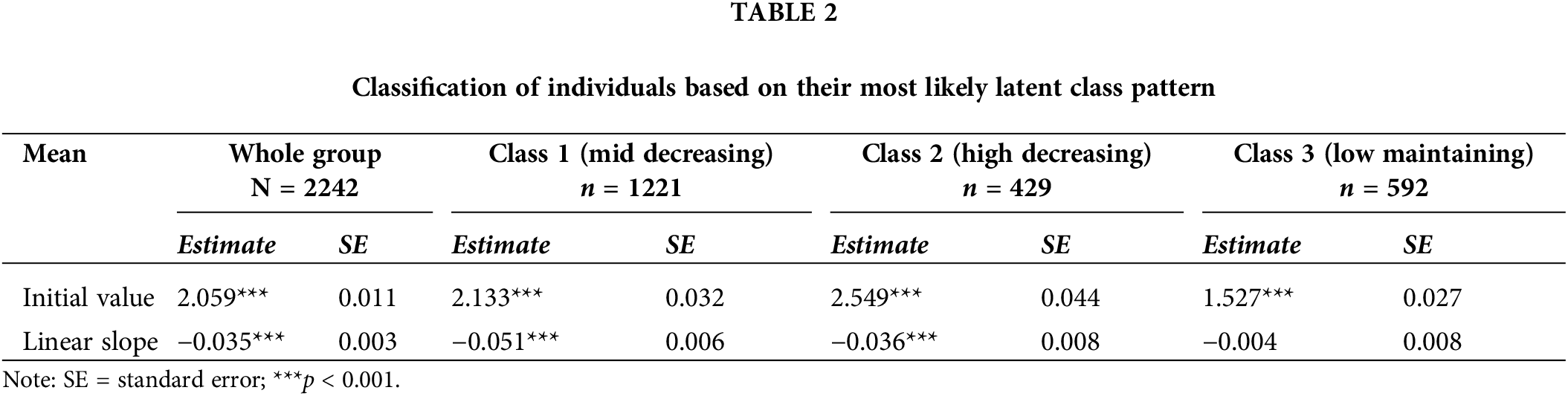
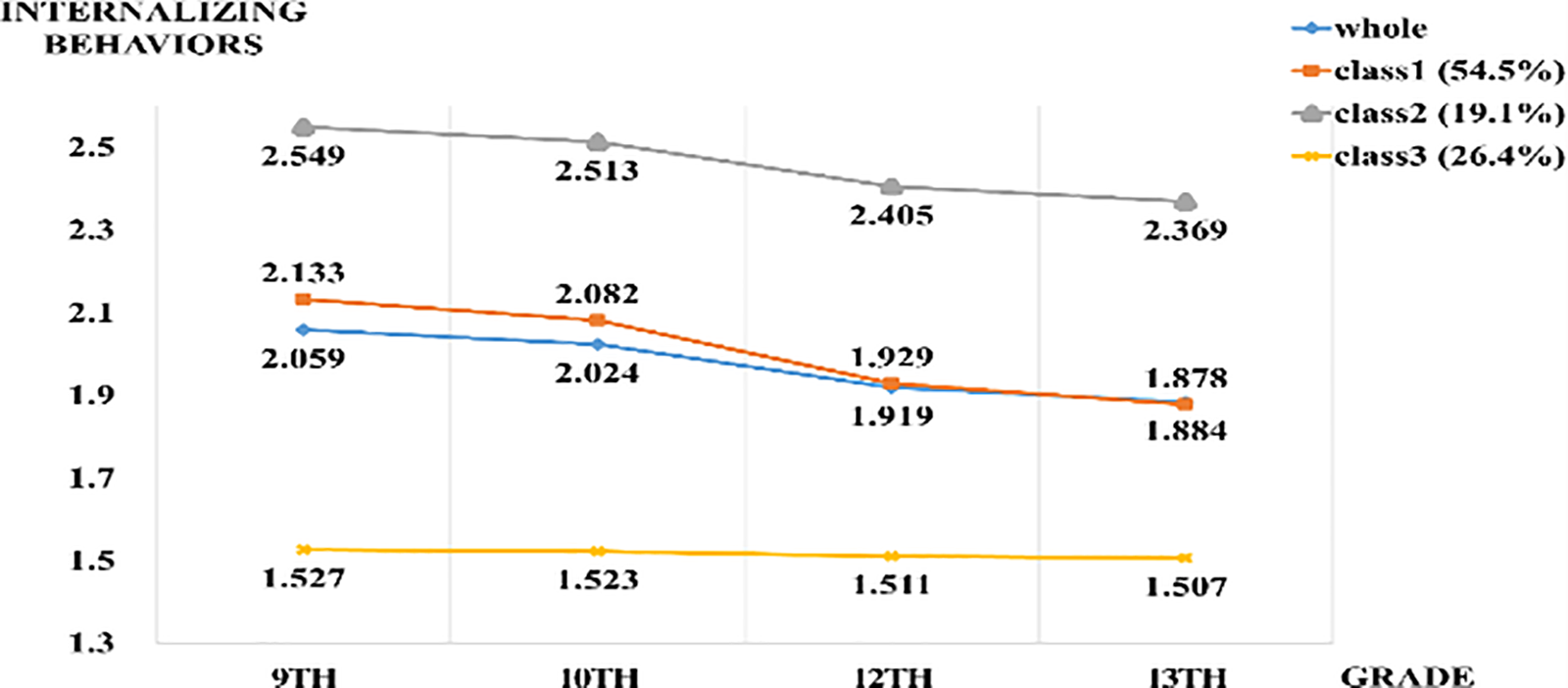
Figure 1: Trajectories of internalizing behavior.
Descriptive statistics of main factors according to latent classes
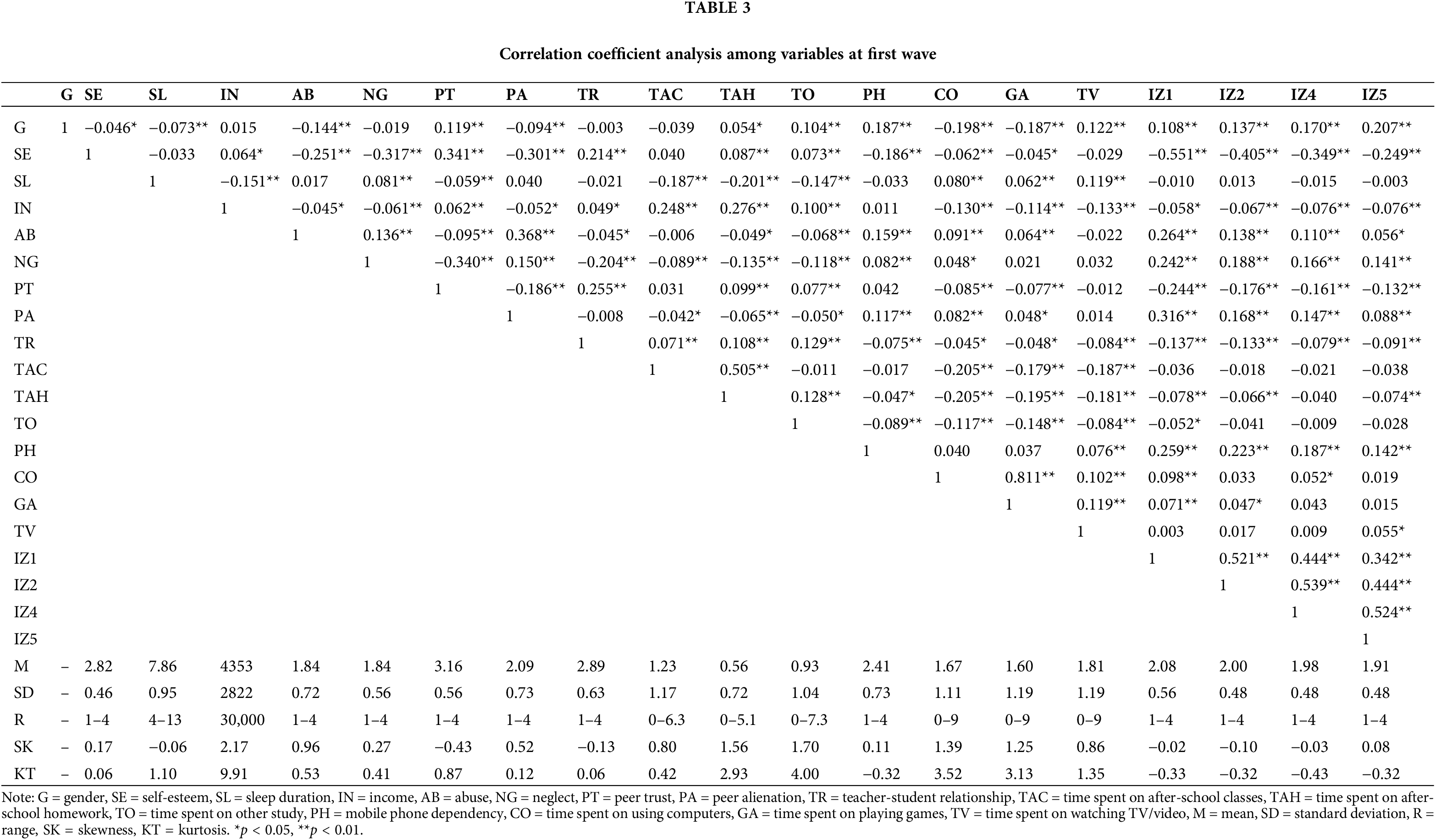
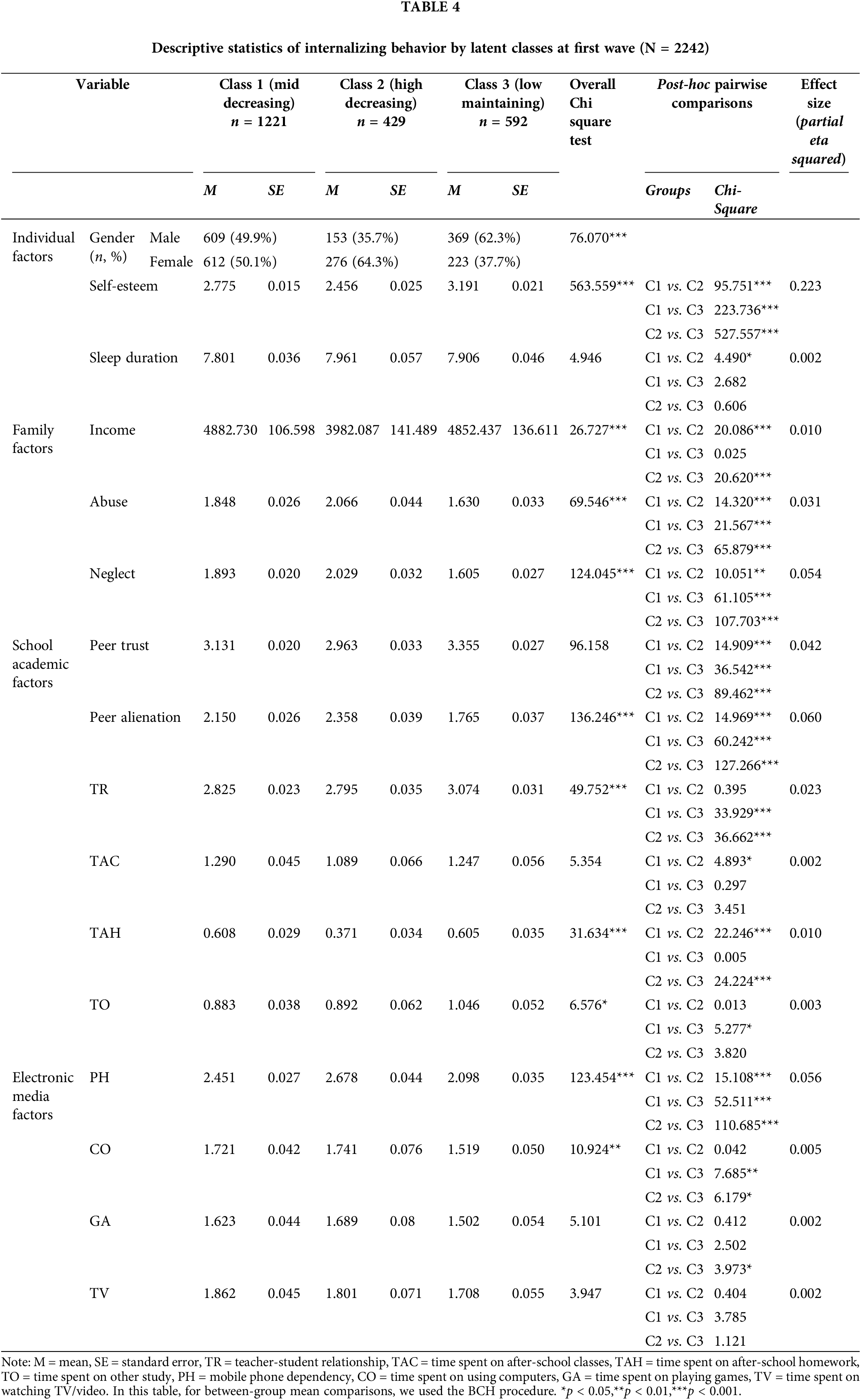
Table 3 shows the correlation coefficients for the main variables. Table 4 gives the sociodemographic characteristics of the research participants, as well as descriptive statistics for each latent class group’s main factors. BCH techniques analysis was also used to test for variations in the mean values of important variables across each latent class. As a consequence, most variables differed significantly between classes.
Factors associated with the internalizing behavior
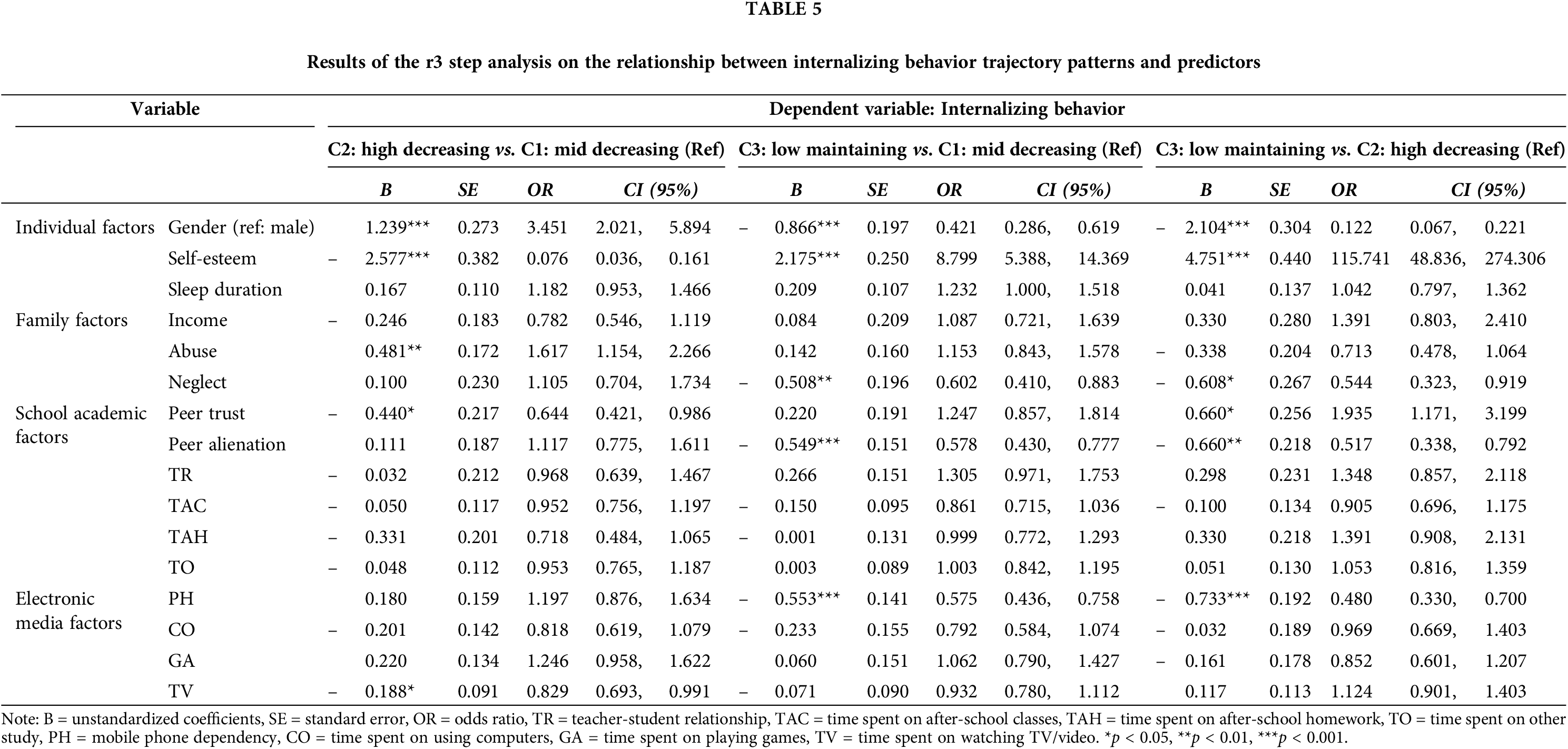
Table 5 shows the relations between predictors associated to the internalizing behavior and the latent group classification. First, the ‘C1: mid decreasing’ was used as reference and when compared with ‘C2: high decreasing,’ female (B = 1.239, p < 0.001), adolescents with lower self-esteem (B = –2.577, p < 0.001), higher abuse (B = 0.481, p < 0.01), lower peer trust (B = –0.440, p < 0.05), and lower time spent on watching TV/video (B = –0.188, p < 0.05) were more likely to belong to the ‘C2: high decreasing.’ Second, the ‘C1: mid decreasing’ was used as reference and when compared with ‘C3: low maintaining,’ female (B = –0.866, p < 0.001), adolescents with lower self-esteem (B = 2.175, p < 0.001), higher neglect (B = –0.508, p < 0.01), higher peer alienation (B = –0.549, p < 0.001), and higher smartphone dependency (B = –0.553, p < 0.001) were more likely to belong to the ‘C1: mid decreasing.’ Finally, the ‘C2: high decreasing’ was used as reference and when compared with ‘C3: low maintaining,’ female (B = –2.104, p < 0.001), adolescents with lower self-esteem (B = 4.752, p < 0.001), higher neglect (B = –0.608, p < 0.05), lower peer trust (B = 0.660, p < 0.05), higher peer alienation (B = –0.660, p < 0.01), and higher smartphone dependency (B = –0.733, p < 0.001) that was part of the ‘C2: high decreasing.’
Types of internalizing behavior trajectories
Our latent class analysis of internalizing behavior trajectories, spanning from ninth grade through one-year post-high school graduation, revealed three distinct developmental patterns: ‘mid decreasing’ (54.5%, 1221 cases), ‘high decreasing’ (19.1%, 429 cases), and ‘low maintaining’ (26.4%, 592 cases). These findings provide valuable insights into the developmental pathways of adolescent mental health.
These results both complement and diverge from previous longitudinal research [11,12]. The literature has shown mixed findings regarding adolescent internalizing behavior trajectories, with some studies documenting decreasing patterns among Korean adolescents while others identified increasing trends [12]. Our research extends this understanding by identifying distinct subgroups with unique developmental trajectories [8–12]. Particularly significant is how our findings illuminate the role of cultural context in shaping these developmental patterns. Research conducted across Europe, the United States, and Asia has demonstrated that adolescent internalizing behavior is influenced by various social, familial, and environmental factors that differ substantially across cultural settings. Studies consistently show that cultural norms and parenting practices are crucial in shaping these developmental pathways, with no universal patterns emerging across diverse societies [8–10].
The South Korean context provides particularly valuable insights due to its unique sociocultural characteristics. Specific cultural elements—including intense academic pressure, strong familial expectations, and societal norms governing emotional expression—appear to influence these developmental trajectories in ways that may differ significantly from Western contexts. This cultural specificity offers an essential framework for understanding the patterns observed in our study.
The identification of multiple trajectory groups suggests that internalizing behavior development follows a more complex pattern than simple linear increases or decreases. These findings are especially significant as they reveal distinct subgroups with varying levels and patterns of internalizing behavior, moving beyond traditional population-wide trend analyses. This heterogeneity carries important implications for intervention strategies, suggesting the need for targeted approaches based on trajectory group membership.
The ‘high decreasing’ group merits particular attention, given the well-documented negative effects of internalizing behavior on child development [2,4]. Understanding this high-risk group’s characteristics and needs is crucial for developing effective interventions. Equally important are the insights gained from the ‘low maintaining’ group, as understanding the factors contributing to their sustained lower levels of internalizing behavior could inform prevention strategies and interventions for other groups.
These distinct trajectories strongly suggest that interventions should be tailored to specific developmental pathways rather than applying a uniform approach. Such targeted interventions are likely to be more effective in addressing the unique needs and challenges faced by adolescents in each trajectory group. This understanding enables the development of more nuanced and effective intervention strategies, potentially leading to better outcomes for adolescents across different trajectory groups.
Key factors influencing internalizing behavior
Our analysis identified several critical factors associated with internalizing behavior trajectory patterns. Regarding individual factors, gender emerged as a significant predictor, with male students demonstrating consistently lower levels of internalizing behavior compared to female students. This gender difference, well-documented in previous research [21], was further elaborated in Liu et al.’s study, which highlighted that certain risk factors, such as marital conflict and family deficits, were unique to female students, suggesting the necessity for gender-specific intervention approaches.
Self-esteem emerged as another crucial individual factor influencing internalizing behavior trajectories. Higher self-esteem significantly increased the likelihood of belonging to groups with lower internalizing behavior levels. This finding aligns with previous research [15], particularly Mileviciute et al.’s comprehensive analysis of youth in the Americas, which demonstrated strong correlations between higher self-efficacy and lower depression levels. These findings emphasize the potential value of self-esteem enhancement interventions in preventing or reducing internalizing behavior.
Family factors, particularly parenting attitudes and experiences of abuse and neglect, showed strong associations with trajectory group membership. Higher levels of abuse and neglect significantly increased the likelihood of belonging to groups with elevated internalizing behavior. These findings correspond with Jwa’s research, which demonstrated that excessive interference and abuse correlate with higher levels of internalizing behavior in children. This suggests the importance of examining family environment factors when addressing adolescent internalizing behaviors, rather than viewing them solely as individual behavioral issues.
In the domain of school and academic factors, peer trust and alienation emerged as significant predictors of trajectory group membership. Lower peer trust and higher peer alienation increased the probability of belonging to groups with elevated internalizing behavior, supporting previous research findings [16,23]. Morales et al.’s study particularly highlighted that children experiencing peer rejection demonstrated higher internalizing levels compared to their non-rejected peers [16], emphasizing the crucial role of positive peer relationships in school settings.
Electronic media factors, particularly smartphone dependency, showed significant associations with internalizing behavior trajectories, aligning with research from both Korea and the U.S. [27,47]. Perrino et al.’s analysis of U.S. Hispanic adolescents demonstrated that increased smartphone use correlated with higher levels of internalizing behavior [27]. This finding has particular relevance in South Korea, where smartphone penetration rates reach approximately 95% [48].
Interestingly, the relationship between electronic media use and internalizing behavior revealed complex patterns. While smartphone dependency showed a clear positive association with internalizing behavior, time spent watching TV or videos demonstrated an inverse relationship, with higher consumption associated with lower likelihood of belonging to groups with elevated internalizing behavior. This unexpected finding suggests that certain forms of media consumption might serve as stress-relief mechanisms, though this requires further investigation.
Our findings emphasize the interconnected nature of these various factors. The relationship between peer relationships and internalizing behavior may be moderated by self-esteem, while family factors could simultaneously influence both self-esteem and peer relationships. This intricate web of relationships suggests the need for comprehensive intervention approaches that address multiple risk and protective factors concurrently.
These findings significantly advance our understanding of internalizing behavior by highlighting the relative importance of different factors across developmental trajectories. They indicate that intervention strategies should be multifaceted, addressing individual, family, school, and technological factors while considering the unique characteristics of different trajectory groups. The identification of these key factors provides a robust foundation for developing more targeted and effective interventions for adolescent mental health.
This study has three main limitations. First, we treated predictive factors as time-invariant, while future research should consider time-varying characteristics. Second, although we focused on adolescents aged 14.9–18.9 years, further research should examine internalizing behavior in childhood and early adolescence, as these are crucial developmental periods. Third, while we tracked a cohort longitudinally, we did not divide participants into specific age groups (e.g., early vs. mid-adolescence), which could reveal important developmental differences in internalizing behavior trajectories. Future studies addressing these limitations would enhance our understanding of age-related differences in adolescent internalizing behavior.
This study examined the latent groups of internalizing behavior trajectories among adolescents from ninth grade through one-year post-high school graduation using KCYPS data. Unlike previous variable-centered approaches that treated the population as homogeneous, our research identified distinct subgroups with varying trajectories. The identification of high, medium, and low internalizing behavior groups, along with their characteristic features, provides an important foundation for targeted interventions. Our findings revealed several key factors influencing internalizing behavior: gender, self-esteem, abuse, neglect, peer relationships, smartphone addiction, and time spent watching TV or videos. These results suggest that effective reduction of adolescent internalizing behavior requires comprehensive interventions addressing multiple domains-interpersonal, family, school, and environmental factors. This multifaceted understanding enables the development of more targeted and effective interventions for different subgroups of adolescents experiencing internalizing behaviors.
Acknowledgement: The author thanks research participants for their participation in this study.
Funding Statement: The author received no specific funding for this study.
Availability of Data and Materials: The data that support the findings of this study are available from the Korean National Youth Policy Institute at (https://www.nypi.re.kr/archive/eps) (accessed on 19 December 2024).
Ethics Approval: Not applicable.
Conflicts of Interest: The author declares no conflicts of interest to report regarding the present study.
References
1. Achenbach TM. Integrative guide for the 1991 CBCL/4-18, YSR, and TRF profiles. Burlington: Department of Psychiatry, University of Vermont; 1991. [Google Scholar]
2. Meier MH, Beardslee J, Pardini D. Associations between recent and cumulative cannabis use and internalizing problems in boys from adolescence to young adulthood. J Abnorm Child Psychol. 2020;48(6):771–82. doi:10.1007/s10802-020-00641-8. [Google Scholar] [PubMed] [CrossRef]
3. Arslan İB, Lucassen N, Van Lier PA, De Haan AD, Prinzie P. Early childhood internalizing problems, externalizing problems and their co-occurrence and (mal) adaptive functioning in emerging adulthood: a 16-year follow-up study. Soc Psychiat Psychiatr Epidemiol. 2021;56(2):193–206. doi:10.1007/s00127-020-01959-w. [Google Scholar] [PubMed] [CrossRef]
4. Essau CA, de la Torre-Luque A. Comorbidity between internalising and externalising disorders among adolescents: symptom connectivity features and psychosocial outcome. Child Psychiat Hum Dev. 2023;54(2):493–507. doi:10.1007/s10578-021-01264-w. [Google Scholar] [PubMed] [CrossRef]
5. Morneau-Vaillancourt G, Voronin I, Ouellet-Morin I. Polygenic predictions of internalizing problems and suicidal behaviors in youth. Eur Neuropsychopharmacol. 2023;75:S36. doi:10.1016/j.euroneuro.2023.08.074. [Google Scholar] [CrossRef]
6. Yap MB, Allen NB, Ladouceur CD. Maternal socialization of positive affect: the impact of invalidation on adolescent emotion regulation and depressive symptomatology. Child Dev. 2008;79(5):1415–31. doi:10.1111/j.1467-8624.2008.01196.x. [Google Scholar] [PubMed] [CrossRef]
7. Jarvers I, Ecker A, Schleicher D, Brunner R, Kandsperger S. Impact of preschool attendance, parental stress, and parental mental health on internalizing and externalizing problems during COVID-19 lockdown measures in preschool children. PLoS One. 2023;18(2):e0281627. doi:10.1371/journal.pone.0281627. [Google Scholar] [PubMed] [CrossRef]
8. Nivard MG, Lubke GH, Dolan CV, Evans DM, Pourcain BS, Munafò MR, et al. Joint developmental trajectories of internalizing and externalizing disorders between childhood and adolescence. Dev Psychopathol. 2017;29(3):919–28. doi:10.1017/S0954579416000572. [Google Scholar] [PubMed] [CrossRef]
9. Rothenberg WA, Lansford JE, Bornstein MH, Chang L, Deater-Deckard K, Di Giunta L, et al. Effects of parental warmth and behavioral control on adolescent externalizing and internalizing trajectories across cultures. J Res Adolesc. 2020;30(4):835–55. doi:10.1111/jora.12566. [Google Scholar] [PubMed] [CrossRef]
10. Gong X, Guo N, Huebner ES, Tian L. Gender-specific co-developmental trajectories of internalizing and externalizing problems from middle childhood to early adolescence: environmental and individual predictors. Dev Psychopathol. 2023;35(3):1468–83. doi:10.1017/S0954579422000207. [Google Scholar] [PubMed] [CrossRef]
11. Lee S, Bernstein R, Ip KI, Olson SL. Developmental cascade models linking contextual risks, parenting, and internalizing symptoms: a 17-year longitudinal study from early childhood to emerging adulthood. Dev Psychopathol. 2024;36(1):144–60. doi:10.1017/S0954579422001043. [Google Scholar] [PubMed] [CrossRef]
12. Leve LD, Kim HK, Pears KC. Childhood temperament and family environment as predictors of internalizing and externalizing trajectories from ages 5 to 17. J Abnorm Child Psychol. 2005;33(5):505–20. doi:10.1007/s10802-005-6734-7. [Google Scholar] [PubMed] [CrossRef]
13. Gorostiaga A, Aliri J, Balluerka N, Lameirinhas J. Parenting styles and internalizing symptoms in adolescence: a systematic literature review. Int J Environ Res Public Health. 2019;16(17):3192. doi:10.3390/ijerph16173192. [Google Scholar] [PubMed] [CrossRef]
14. Martinez I, Garcia F, Veiga F, Garcia OF, Rodrigues Y, Serra E. Parenting styles, internalization of values and self-esteem: a cross-cultural study in Spain, Portugal and Brazil. Int J Environ Res Public Health. 2020;17(7):2370. doi:10.3390/ijerph17072370. [Google Scholar] [PubMed] [CrossRef]
15. Mileviciute I, Scott WD, Mousseau AC. Alcohol use, externalizing problems, and depressive symptoms among American Indian youth: the role of self-efficacy. Am J Drug Alcohol Abuse. 2014;40(4):342–8. doi:10.3109/00952990.2014.910518. [Google Scholar] [PubMed] [CrossRef]
16. Morales S, Vallorani A, Pérez-Edgar K. Young children’s behavioral and neural responses to peer feedback relate to internalizing problems. Dev Cogn Neurosci. 2019;36(3):100610. doi:10.1016/j.dcn.2018.12.008. [Google Scholar] [PubMed] [CrossRef]
17. Olivier E, Morin AJ, Langlois J, Tardif-Grenier K, Archambault I. Internalizing and externalizing behavior problems and student engagement in elementary and secondary school students. J Youth Adolesc. 2020;49(11):2327–46. doi:10.1007/s10964-020-01295-x. [Google Scholar] [PubMed] [CrossRef]
18. Hsieh H-F, Zimmerman MA, Xue Y, Bauermeister JA, Caldwell CH, Wang Z, et al. Stress, active coping, and problem behaviors among Chinese adolescents. Am J Orthopsychiat. 2014;84(4):364. doi:10.1037/h0099845. [Google Scholar] [PubMed] [CrossRef]
19. Bronfenbrenner U. Toward an experimental ecology of human development. Am Psychol. 1977;32(7):513. doi:10.1037/0003-066X.32.7.513. [Google Scholar] [CrossRef]
20. Quach JL, Nguyen CD, Williams KE, Sciberras E. Bidirectional associations between child sleep problems and internalizing and externalizing difficulties from preschool to early adolescence. JAMA Pediatr. 2018;172(2):e174363. doi:10.1001/jamapediatrics.2017.4363. [Google Scholar] [PubMed] [CrossRef]
21. Liu K, Thompson RC, Watson J, Montena AL, Warren SL. Developmental trajectories of internalizing and externalizing symptoms in youth and associated gender differences: a directed network perspective. Res Child Adolesc Psychopathol. 2023;51(11):1627–39. doi:10.1007/s10802-023-01106-4. [Google Scholar] [PubMed] [CrossRef]
22. Anderson AS, Siciliano RE, Henry LM, Watson KH, Gruhn MA, Kuhn TM, et al. Adverse childhood experiences, parenting, and socioeconomic status: associations with internalizing and externalizing symptoms in adolescence. Child Abuse Negl. 2022;125(9):105493. doi:10.1016/j.chiabu.2022.105493. [Google Scholar] [PubMed] [CrossRef]
23. Tambelli R, Laghi F, Odorisio F, Notari V. Attachment relationships and internalizing and externalizing problems among Italian adolescents. Child Youth Serv Rev. 2012;34(8):1465–71. doi:10.1016/j.childyouth.2012.04.004. [Google Scholar] [CrossRef]
24. Baker JA, Grant S, Morlock L. The teacher-student relationship as a developmental context for children with internalizing or externalizing behavior problems. Sch Psychol Q. 2008;23(1):3–15. doi:10.1037/1045-3830.23.1.3. [Google Scholar] [CrossRef]
25. Högberg B, Strandh M, Petersen S, Nilsson K. Associations between academic achievement and internalizing disorders in Swedish students aged 16 years between 1990 and 2018. Eur Child Adolesc Psychiat. 2024;22(3):1–11. doi:10.1007/s00787-024-02597-2. [Google Scholar] [PubMed] [CrossRef]
26. Dhital R, Shibanuma A, Miyaguchi M, Kiriya J, Jimba M. Effect of psycho-social support by teachers on improving mental health and hope of adolescents in an earthquake-affected district in Nepal: a cluster randomized controlled trial. PLoS One. 2019;14(10):e0223046. doi:10.1371/journal.pone.0223046. [Google Scholar] [PubMed] [CrossRef]
27. Perrino T, Brincks A, Lee TK, Quintana K, Prado G. Screen-based sedentary behaviors and internalizing symptoms across time among US Hispanic adolescents. J Adolesc. 2019;72(1):91–100. doi:10.1016/j.adolescence.2019.02.014. [Google Scholar] [PubMed] [CrossRef]
28. Yoo C. Problematic smartphone use and adolescent’s depression trajectory patterns. Asia Pac J Soc Work Dev. 2024;22(5):1–17. doi:10.1080/29949769.2024.2397982. [Google Scholar] [CrossRef]
29. Lee S, Kim H, En Y. A study on the use of cell phones and their influence on the utilization of youth. Samsung Life Institute for Public Health and Mental Health Science l. 2002 [cited 2024 Oct 21]. Available from: https://www.samsunghospital.com. [Google Scholar]
30. Cho B, Lim K. Development and validation of emotional or behavioral problems scale. Korean J Couns Psychother. 2003;15(4):729–46. [Google Scholar]
31. Kim S-H, Kim K-Y. Development of behavior problem scale for children and adolescence. J Korean Home Manag Assoc. 1998;16(4):155–66. [Google Scholar]
32. Kim JH, Kim K. The standardization study of symptom checklist-90-revision in Korea III. Ment Health Res. 1984;2:278–311. [Google Scholar]
33. Ban J, Oh I. Mediating effects of teacher and peer relationships between parental abuse/neglect and emotional/behavioral problems. Child Abuse Negl. 2016;61(1):35–42. doi:10.1016/j.chiabu.2016.09.010. [Google Scholar] [PubMed] [CrossRef]
34. Rosenberg M. Society and the adolescent self-image. Princeton, New Jersey, NJ, USA: Princeton University Press; 1965. [Google Scholar]
35. Greenberger E, Chen C, Dmitrieva J, Farruggia SP. Item-wording and the dimensionality of the Rosenberg self-esteem scale: do they matter? Pers Individ Dif. 2003;35(6):1241–54. doi:10.1016/S0191-8869(02)00331-8. [Google Scholar] [CrossRef]
36. Huh MY. The study for the development and validation of ‘parenting behavior inventory’ perceived by adolescent (Ph.D. Thesis). Ewha Womans University: Seoul, Republic of Korea; 2000. [Google Scholar]
37. Kim S. The effect of social support on abused children’s adjustment (Master Thesis). Seoul National University: Seoul, Republic of Korea; 2003. [Google Scholar]
38. Armsden GC, Greenberg MT. The inventory of parent and peer attachment: individual differences and their relationship to psychological well-being in adolescence. J Youth Adolesc. 1987;16(5):427–54. doi:10.1007/BF02202939. [Google Scholar] [PubMed] [CrossRef]
39. Min B. The effects of school adaptation and self-concept on academic achievement (Master Thesis). Hongik University: Seoul, Republic of Korea; 1991. [Google Scholar]
40. Fontana A, Benzi IMA, Cipresso P. Problematic internet use as a moderator between personality dimensions and internalizing and externalizing symptoms in adolescence. Curr Psychol. 2023;42(22):19419–28. doi:10.1007/s12144-021-02409-9. [Google Scholar] [PubMed] [CrossRef]
41. Akaike H. A new look at the statistical model identification. IEEE Trans Autom Control. 1974;19(6):716–23. doi:10.1109/TAC.1974.1100705. [Google Scholar] [CrossRef]
42. Schwarz G. Estimating the dimension of a model. Ann Stat. 1978;6:461–4. [Google Scholar]
43. Lo Y, Mendell NR, Rubin DB. Testing the number of components in a normal mixture. Biometrika. 2001;88(3):767–78. doi:10.1093/biomet/88.3.767. [Google Scholar] [CrossRef]
44. Dias JG, Vermunt JK. Bootstrap methods for measuring classification uncertainty in latent class analysis. In: Rizzi A, Vichi M, editors. Proceedings in computational statistics; 2006. p. 31–41. doi:10.1007/978-3-7908-1709-6_3. [Google Scholar] [CrossRef]
45. Asparouhov T, Muthén B. Auxiliary variables in mixture modeling: three-step approaches using M plus. Struct Equ Model. 2014;21(3):329–41. doi:10.1080/10705511.2014.915181. [Google Scholar] [CrossRef]
46. Coffman DL, Millsap RE. Evaluating latent growth curve models using individual fit statistics. Struct Equ Model. 2006;13(1):1–27. doi:10.1207/s15328007. [Google Scholar] [CrossRef]
47. Deng X, Li X, Xiang Y. Smartphone addiction and internalized and externalized aggression among adolescents: evidence from longitudinal study and weekly diary study. Comput Human Behav. 2024;150(3):107988. doi:10.1016/j.chb.2023.107988. [Google Scholar] [CrossRef]
48. Yoo C. What makes children aged 10 to 13 engage in problematic smartphone use? A longitudinal study of changing patterns considering individual, parental, and school factors. J Behav Addict. 2024;13(1):76–87. doi:10.1556/2006.2024.00002. [Google Scholar] [PubMed] [CrossRef]
Cite This Article
 Copyright © 2025 The Author(s). Published by Tech Science Press.
Copyright © 2025 The Author(s). Published by Tech Science Press.This work is licensed under a Creative Commons Attribution 4.0 International License , which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
 Downloads
Downloads
 Citation Tools
Citation Tools