
 Submit a Paper
Submit a Paper Propose a Special lssue
Propose a Special lssue Open Access
Open Access
ARTICLE

The Moderating Role of Control Strategies on the Relationship between Negative Emotions and QoL in the Elderly: A Longitudinal Study
1 Faculty of Psychology, National Demonstration Center for Experimental Psychology Education, Beijing Key Laboratory of Applied Experimental Psychology, Beijing Normal University, Beijing, 100875, China
2 China Academy of Civil Aviation Science and Technology, Beijing, 100028, China
* Corresponding Author: Wei Xu. Email:
# Ran Ma and Chunyang Zhang are both first authors
International Journal of Mental Health Promotion 2025, 27(4), 469-483. https://doi.org/10.32604/ijmhp.2025.060351
Received 30 October 2024; Accepted 13 March 2025; Issue published 30 April 2025
 View Full Text
View Full Text Download PDF
Download PDFAbstract
Background: Maintaining optimal quality of life (QoL) is a pivotal for “successful aging”. Understanding how the QoL of the elderly develops and what role psychological factors play in its development will help improve QoL from a psychological perspective. Embedded within the lifespan theory of control, this longitudinal study aimed to (1) map the temporal trajectory of QoL among Chinese older adults, (2) examine differential effects of tripartite negative emotions (stress, anxiety, depression), and (3) test the moderating role of control strategies (goal engagement, goal disengagement, self-protection) in emotion-QoL dynamics. Method: A prospective cohort of 345 community-dwelling older adults (Mage = 83.84 ± 8.49 years; 55.1% female) completed validated measures—SF-36 for QoL, DASS-21 for negative emotions, and an adapted Control Strategies Questionnaire (CAS)—at three waves spanning 12 months. Hierarchical linear modeling (HLM) with time-nested structure analyzed intraindividual changes and interindividual differences. Results: QoL exhibited a significant linear decline over time (β = −4.75, p < 0.001). Stress (β = −14.12, p < 0.001) and anxiety (β = −11.24, p < 0.001) robustly predicted QoL decline, whereas depression showed no significant effect. Control strategies had divergent associations: goal engagement (β = 3.51, p < 0.001) and self-protection (β = 2.38, p = 0.015) predicted higher baseline QoL, while goal disengagement accelerated decline (β = −7.00, p < 0.001; interaction with time: β = −2.46, p < 0.001). Contrary to hypotheses, control strategies did not moderate emotion-QoL associations (ΔR2 = 0.02, p = 0.21). Conclusion: The results showed that stress and anxiety played an important role in the QoL of the elderly. At the same time, goal engagement and self-protection were beneficial to the QoL of the elderly, while goal disengagement was not conducive to QoL and its development among the elderly. Meanwhile, the negative effect of anxiety and stress on the QoL of the elderly was not affected by the control strategies.Keywords
China is gradually entering an aging society, and the elderly population will continue to rise and is expected to reach its peak in the middle of the twenty-first century [1]. At the same time, how to achieve “successful aging” has become an important issue for everyone and even at the social level. And how to define “successful aging”? Not only have researchers imagined the general profit of the “successful elderly” from the objective perspective of physical, psychological, and social functions, but also constructed the lifetime control theory to describe the image of the “wise elderly”, who is perfectly balanced between gains and losses [2].
In terms of the performance of successful aging, good quality of life (QoL) is one of the most vital characteristics. QoL was defined as a multidimensional, subjective, and measurable structure that encompassed both physical and psychological states as well as social functioning [3]. Factors affecting the QoL of the elderly included objective health, socioeconomic status, demographic characteristics, and subjective psychological condition [4,5], which contributed to an overall downward trend in the QoL among older adults [6,7]. In order to slow down the declining trend and improve the QoL of the elderly from the psychological perspective, this study further explored the role of negative emotions in the QoL of the elderly and examined the moderating effect of control strategies.
1.1 Negative Emotions and the QoL of the Elderly
The aging process is usually accompanied by an increase in physical illness, a decline in cognitive function, and a continuous loss of social roles [8]. However, older adults also report high levels of QoL, well-being, and life satisfaction [4,9]. Social mood choice theory shed light on the “paradox of aging” from the perspective of “time consciousness”, indicating that when the elderly perceived their left lifetime was limited, they tended to achieve the goals of internal emotion management, namely, preferred to process positive stimulus while avoiding negative stimulus, thus present a positive effect in the process of aging [10]. At the same time, a series of research also showed that depression, anxiety, stress, and other negative emotions were common among the elderly [11,12], and the proportion of older adults with mental disorders in 2016 was even up to 35.2% [13,14]. Considering the evidence presented above, both positive bias and negative emotions existed among the elderly. Therefore, in order to achieve “successful aging”, it’s necessary to pay attention to the consequences of negative emotions among the elderly and find ways to cope with them.
High negative emotions contribute to a lack of sufficient resources and the ability to adapt or regulate one’s own state [15], thus the elderly with high negative emotions might suffer from poor QoL [16]. Many studies have demonstrated the association of negative emotions, such as depression and anxiety, on the QoL of the elderly. Cross-sectional research has shown that older adults with higher levels of depression and anxiety report lower QoL [17]. In addition, older adults with higher levels of depression are associated with worse cognitive function, health status, and social function [18]. However, cross-sectional designs do not establish causality, which has led to growing interest in longitudinal studies to better understand the directional relationship between negative emotions and QoL. For example, the SHARE project provided evidence that depression and anxiety significantly predict QoL decline over time [6]. Moreover, interventions targeting negative emotions, such as emotion-labeling tasks, have been shown to significantly improve subjective QoL among elderly participants, implying that changes in emotions may lead to enhanced subjective QoL [19]. Despite these advancements, psychological stress, as a distinct component of negative emotions, has received less attention in the context of QoL among the elderly.
To address these gaps, the current study used a longitudinal design to clarify the role of negative emotions on QoL among the elderly and then proposed Hypothesis 1: negative emotions (anxiety, depression, and stress) negatively predict QoL in the elderly.
1.2 Control Strategy and the QoL of the Elderly
In the process of “successful aging”, positive control strategies play an important role. Having combined primary and secondary control theories, Reference [20] proposed the life-span theory of control, according to which, an individual’s life is a process of accomplishing a series of goals. While the elderly often encounter various limitations with age, such as the decline of physical and social functions, during the course of choosing, accomplishing, or giving up goals, they constantly adjust and optimize their control strategies. Specifically, there are three kinds of control strategies, i.e., goal engagement, goal disengagement, and self-protection. Goal engagement strategy indicates that when goals are matched with opportunities, individuals tend to take proactive strategies to meet needs, such as continuously increasing the investment of personal resources, including time, effort, and skills, or improving the perceived value of a given goal and using the help of others. Goal disengagement is characterized as the tendency to reduce the value of the goal and quit presupposed investment of resources when the opportunity is limited. Self-protection refers to adapting to life through positive cognitive reappraisal or downward social comparison when opportunities are limited [21,22].
What are the specific effects of the three control strategies on the quality of life of the elderly? Faced with relatively controllable health problems, goal engagement strategies can reduce the prediction of somatic disease symptoms of depression [23] and alleviate the declining trend of health status among the elderly [24]. At the same time, older adults with more positive coping patterns showed better quality of life, a sense of control and pleasure [25]. However, in the context of uncontrollable chronic conditions, excessive goal engagement may lead to frustration and negative health outcomes, as observed in its long-term association with diminished physical health and daily functioning [22]. These findings highlight the importance of aligning engagement strategies with realistic opportunities to avoid adverse effects.
Meanwhile, goal disengagement and self-protection are particularly effective in preserving QoL during periods of significant loss or unattainable goals. These strategies enable older adults to conserve motivational resources, reduce emotional distress, and maintain a sense of control in the face of adversity [26,27]. There are many empirical studies in favor of the theory above. For example, the use of self-protective and goal disengagement strategies can positively predict the physical health and functional status of the elderly after 5 years [22]; self-protective strategies can predict higher levels of well-being among elderly people with visual impairment [28]; goal disengagement strategies can reduce the severity of cold symptoms 6 years later among older adults [29]. These findings underscore the adaptive role of these strategies in slowing the progression of QoL decline by fostering psychological resilience.
As older adults face inevitable aging-related challenges, such as declining physical health, cognitive impairments, and reduced social roles, maintaining QoL becomes increasingly difficult. Control strategies, particularly goal disengagement and self-protection, play a vital role in mitigating the decline of QoL over time. These strategies help older adults adapt to situations where goals become unattainable or resources are insufficient, preserving emotional and motivational stability in the face of losses. Goal disengagement allows individuals to reallocate limited resources, avoiding the frustration and emotional strain that can arise from persistently striving toward unachievable goals [26]. Self-protection strategies, such as cognitive reappraisal and downward social comparison, enable older adults to maintain a positive self-concept and emotional well-being even when faced with significant life changes [28,29]. These mechanisms reduce the psychological toll of aging, thereby slowing the overall decline in QoL.
In addition, cultural differences may exist in the use of control strategies [26]. Although there is a certain cross-cultural consistency in the association between control strategies and life satisfaction among the elderly in China [30], the relationship between the three control strategies and the QoL of the elderly in China needs to be further evaluated. Given the dynamic and cumulative nature of aging, understanding how control strategies slow the decline of QoL over time is essential. Therefore, the current study further investigated the influence of goal engagement, goal disengagement, and self-protective strategies on the QoL of the elderly in China, and explored the three kinds of control strategies as the protective role in the QoL change of the elderly, thus hypothesizing the Hypothesis 2a: Control strategies (goal engagement, goal disengagement, and self-protection) will have direct positive effects on the QoL of older adults; Hypothesis 2b: Control strategies will alleviate the decline process of QoL.
1.3 The Role of Control Strategies in Negative Emotions and QoL among the Elderly
Reference [31] stated that “people get happier as they get older, but researchers are not sure why?” It has reached many consensuses that the positive effects of older adults resulted from their effective emotional strategies [32,33]. However, even so, negative emotional problems such as anxiety, depression, and stress remain prevalent among older adults [11,12]. This paradox suggests the presence of protective factors that mediate or moderate the impact of negative emotions on well-being, life satisfaction, and QoL. Specifically, it seems possible that in the process of negative emotions affecting QoL, protective factors, such as control strategies, rendered QoL and well-being less sensitive to the negative impact of negative emotions. Given the role of control strategies in maintaining self-esteem and a sense of control, and improving the life satisfaction of the elderly [27,30], control strategies may moderate the association of negative emotions on QoL.
Control strategies have been demonstrated to enhance psychological resilience and mitigate the effects of negative emotions on QoL. In everyday life, where restrictions and stressors are inevitable, these control strategies act as vital moderators in the relationship between negative emotions and QoL. By fostering adaptive responses and promoting psychological resilience, they reduce the vulnerability of QoL to the detrimental effects of emotional challenges, thus supporting successful aging.
For instance, goal engagement—characterized by actively investing time and effort into achieving meaningful goals—has been associated with lower levels of depression [23] and improved physical health among older adults [24]. Studies suggest that older adults who maintain a sense of purpose—through structured activities such as volunteering or goal-directed tasks—experience reduced depression, improved self-reported health, and even lower mortality rates [34,35]. Similarly, research has shown that a positive response to illness perceptions, facilitated by goal engagement, can alleviate the negative effects on QoL [36,37]. Goal disengagement, on the other hand, allows older adults to adapt to unattainable goals by reducing their investment in them and redirecting resources to more feasible objectives. This strategy helps preserve emotional well-being in situations where continued effort would lead to frustration and stress [27]. Complementing this, self-protection strategies—such as cognitive reappraisal and downward social comparison—further shield older adults from the impact of negative emotions. By reframing adverse events in less threatening ways or comparing themselves to others in more challenging circumstances, older adults maintain a sense of control and self-esteem, even in the face of anxiety, depression, or stress [27,30,38].
Despite these insights, the lack of longitudinal evidence regarding the moderating role of control strategies on the relationship between negative emotions and QoL represents a critical gap in the literature. Most existing studies have examined these variables independently or in cross-sectional designs, limiting the ability to infer causality or temporal interactions. Addressing this gap is essential to understanding how control strategies buffer the long-term impact of negative emotions on QoL and how these adaptive mechanisms support successful aging.
Therefore, to test the moderating effect of three kinds of control strategies on the relationship between negative emotions and the QoL among the elderly, the present study applied longitudinal design and put forward Hypothesis 3: three kinds of control strategy can significantly moderate the relationship of negative emotions and the QoL among the elderly. To be specific, all of the control strategies can alleviate the predictive effect of negative emotions on the QoL.
In the current study, data collection was conducted at three-time points among the elderly, who were screened out by cluster sampling method from communities in Nanjing, China. Negative emotions, quality of life, and control strategies were measured at each time.
In November 2020 (T1), a total of 548 elderly people were recruited to complete the questionnaire, aged from 60 to 102 years old (53.5% were female; Mage = 85.34, SD = 7.98).
The follow-up assessments were carried out in May 2021 (T2) and November 2021 (T3), respectively. A total of 68 (12.4%) elderly adults passed away during the follow-up investigation, 24 (4.4%) elderly adults were disabled or hospitalized, and 111 (20.3%) elderly adults did not finish the whole progress due to other reasons. Finally, a total of 345 elderly adults, aged from 60 to 101 years, completed three-time follow-up assessments and were included in the final data analysis (55.1% were female; Mage = 83.84, SD = 8.49). Attrition analyses were performed to evaluate whether participants who dropped out differed significantly from those who completed the study. Comparisons of baseline characteristics, including QoL, DASS, and Control strategy, showed no significant differences (all p > 0.05), suggesting that participant attrition is unlikely to have impacted the study findings.
This research was approved by the Institutional Review Board and Ethics Committee of the Faculty of Psychology, authors’ university. The handwritten informed consent was received by from all individual participants included in the study.
2.2 The MOS Item Short Form Health Survey (SF-36)
The QoL was measured by the MOS 36-item short-form health survey (SF-36) developed by McHorney et al. [39]. The Chinese version of the scale was revised by Li et al. [40]. The scale consists of 36 items, with different ratings from each subscale. The scale includes 8 subscales: physical functioning (PF), role physical (RP), role emotional (RE), vitality (VT), bodily pain (BP), social functioning (SF), mental health (MH), and general health (GH). A higher total score indicates a higher level of quality of life. The scale demonstrated good internal consistency (T1: α = 0.95; T2: α = 0.93; T3: α = 0.95).
2.3 The Depression Anxiety Stress Scale (DASS)
The Depression Anxiety Stress Scale (DASS) developed by Lovibond et al. [41] was used to evaluate negative emotions. Gong et al. [42] revised the scale, which has good reliability and validity. The DASS-21 contains 21 items and 3 subscales, each containing 7 items, to assess stress, anxiety, and depression. On a 4-point scale (0 = extremely disagree; 3 = extremely agree), higher scores indicate higher levels of stress, anxiety, and depression. The internal consistency coefficients of the three subscales were 0.73, 0.77 and 0.76 at T1, 0.62, 0.66 and 0.75 at T2, and 0.69, 0.77 and 0.74 at T3, respectively.
The control strategy questionnaire developed by Chipperfield and Perry [21] was used in the present study. The questionnaire consisted of nine items and contained three dimensions, namely goal engagement, goal disengagement, and self-protection. There were five items for goal engagement (e.g., “Keep doing it as usual”), two items for goal disengagement (e.g., “Tell yourself that it’s not that necessary to do these things”), and two items for self-protection (e.g., “Tell yourself that other peers have worse problems”). Since there’s no Chinese version of this questionnaire at present, the original English version was translated and back-translated in the current study by two graduate students in psychology. When evaluating control strategies, researchers emphasized the limitations experienced by the elderly and added the guiding words: “As age increases, you can’t avoid finding limitations on what you want to accomplish. When you encounter problems with what you want to do, here’s what you might normally do to determine how well it fits your situation”. A 5-point scale was used (0 = extremely disagree; 4 = extremely agree), with higher scores indicating that the elderly were more aligned with the corresponding control strategy. The internal consistency coefficients of the three subscales were 0.83, 0.67, and −0.11 at T1; 0.94, 0.92, and 0.46 at T2; 0.67, 0.89, and 0.10 at T3, respectively.
The self-protection domain showed low internal consistency reliability, which was consistent with previous studies [43]. The two items in the self-protection dimension respectively measured positive cognitive reappraisal and downward social comparison. Chances are that they are functionally complementary and interchangeable across individuals, thus making internal consistency reliability low. To follow suit as the analysis of previous studies [21], in the present study, items in the self-protection dimension were used as independent predictors to examine their role in the QoL of older adults.
2.5 Procedures and Data Analysis
After obtaining the informed consent from the participants, the trained community staff handed out and collected the paper questionnaires. Since some participants were found to have some difficulties in reading and filling out the questionnaire in the previous investigation, the trained community staff were arranged to read the questions to acquire the answers of these particular participants. After the initial test, the follow-up assessments were conducted every six months for a total of 2 times.
In this study, we analyzed the direct effects of control strategies on QoL to understand their immediate contribution to psychological well-being. Additionally, we explored how control strategies mitigate QoL decline over time, which can be conceptualized as moderating the relationship between time and QoL. Lastly, we investigate the role of control strategies (goal engagement, goal disengagement, and self-protection) as moderating variables. Moderation was tested by creating interaction terms between control strategies and negative emotions (stress, anxiety, and depression) to examine their conditional effects on QoL.
To test the moderating effects of control strategies on the relationship between negative emotions and QoL, interaction terms (e.g., negative emotions × control strategies) were created and included in hierarchical linear models (HLM). HLM was chosen for its ability to account for longitudinal data, capturing both within-subject changes and between-subject variability over time. This approach allows for a robust analysis of how control strategies influence the strength and direction of the relationship between negative emotions and QoL.
Firstly, SPSS 26.0 was used for descriptive statistics and correlation analysis of the vital variables measured at three time points. Second, MPLUS 6.0 was applied to build the hierarchical linear model.
3.1 Descriptive Statistics and Correlation Analysis
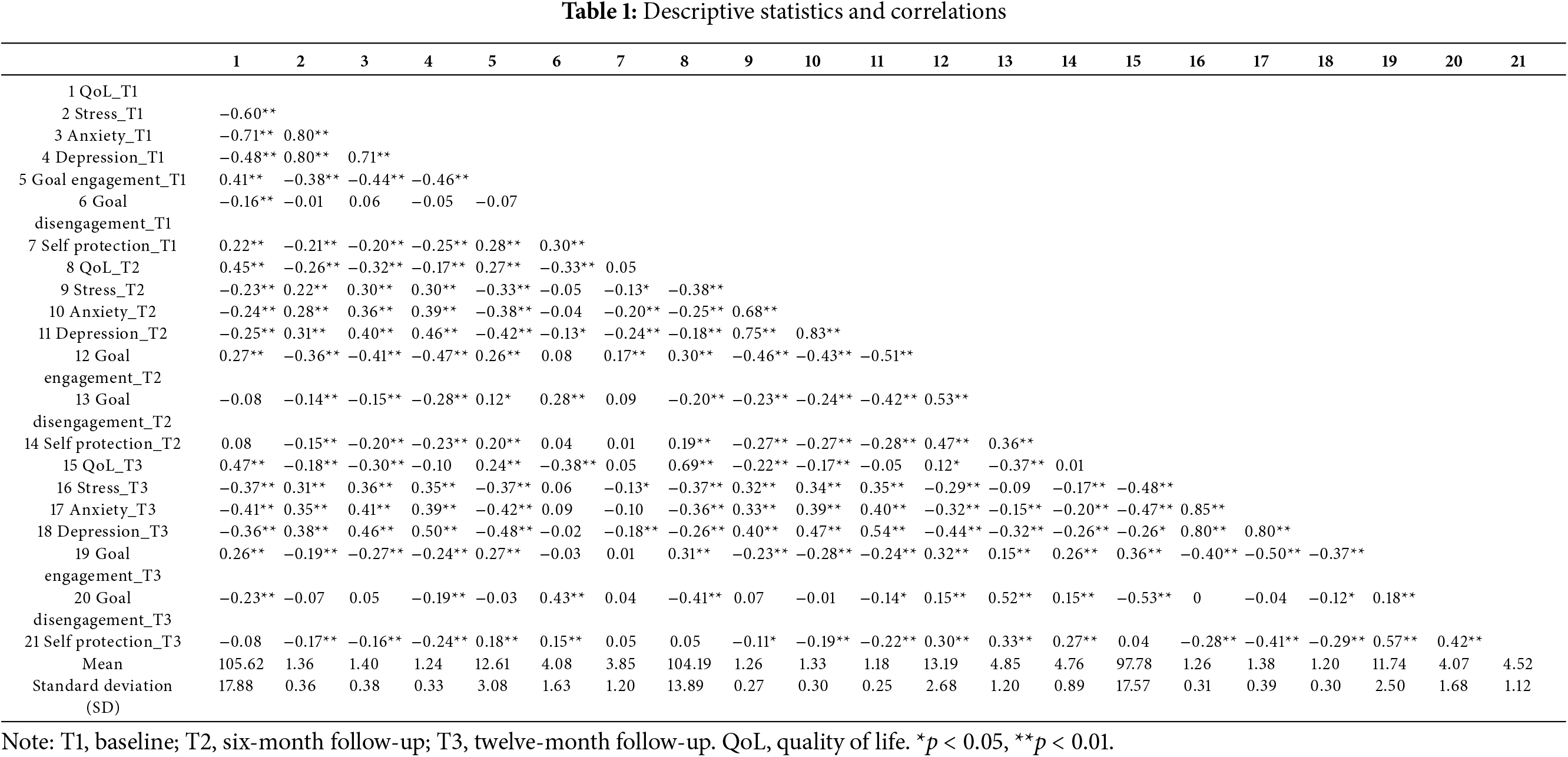
The descriptive statistics and correlation analysis of each variable were shown in Table 1. The results showed that QoL was negatively correlated with negative emotions (r = −0.71~−0.18, all p < 0.01) and positively correlated with goal engagement (r = 0.26~0.41, all p < 0.01). Aside from that QoL at T1 was not significantly associated with T2 goal disengagement, QoL at other time points was negatively correlated with goal disengagement (r = −0.53~−0.16, all p < 0.01). Except for the relationships between QoL at T1 and self-protection at T1 (r = 0.22, p < 0.01), and QoL at T2 and self-protection at T2 (r = 0.19, p < 0.01), the relationship between QoL and self-protection at other time points were all not significant. In addition, negative emotion was negatively correlated with goal engagement (r = −0.51~−0.19, all p < 0.01) and self-protection (r = −0.41~−0.18, all p < 0.01), but its correlation with goal disengagement was not stable.
The data in this study had the characteristics of nested data, so a hierarchical linear model was used for statistical analysis. First, a null model was constructed, and the total variance of QoL was divided into within-person and between-person variance. The results showed that the within-person variance (σ002 = 148.25, p < 0.001) and between-person variance (τ00 = 136.57, p < 0.001) of quality of life were significant. The ratio of between-person variance to total variance was 47.95% (ICC = τ00/(τ00 + σ002) = 0.48 > 0.25). According to the classification criteria of LeBreton et al. [44], when there were large between-person differences in the QoL of the elderly, it was suitable for hierarchical linear model analysis.
Second, a hierarchical linear model was constructed. The first layer is the within-person level where the independent variables were evaluation time and negative emotions (including stress, anxiety, and depression), and the dependent variable was QoL. In the second layer, gender and control strategies (including goal engagement, goal disengagement, and self-protection) were set as the independent variables, and the dependent variable was QoL. Among them, negative emotions and assessment time were taken as within-person variables, and centralized processing was carried out within individuals while gender, goal engagement, goal disengagement, and self-protection served as between-person variables. In this study, we used mean values of the control strategies across time points to simplify data analysis and focus on overall trends. This approach aligns with the scope of the research and is supported by prior literature suggesting moderate temporal stability in similar contexts (Hall et al., 2010). The control strategies in the three-time evaluations were included in the equation after mean transformation, and gender and control strategies were respectively centralized among individuals. The final model is as follows:
The level-1 equation:
The level-2 equation:
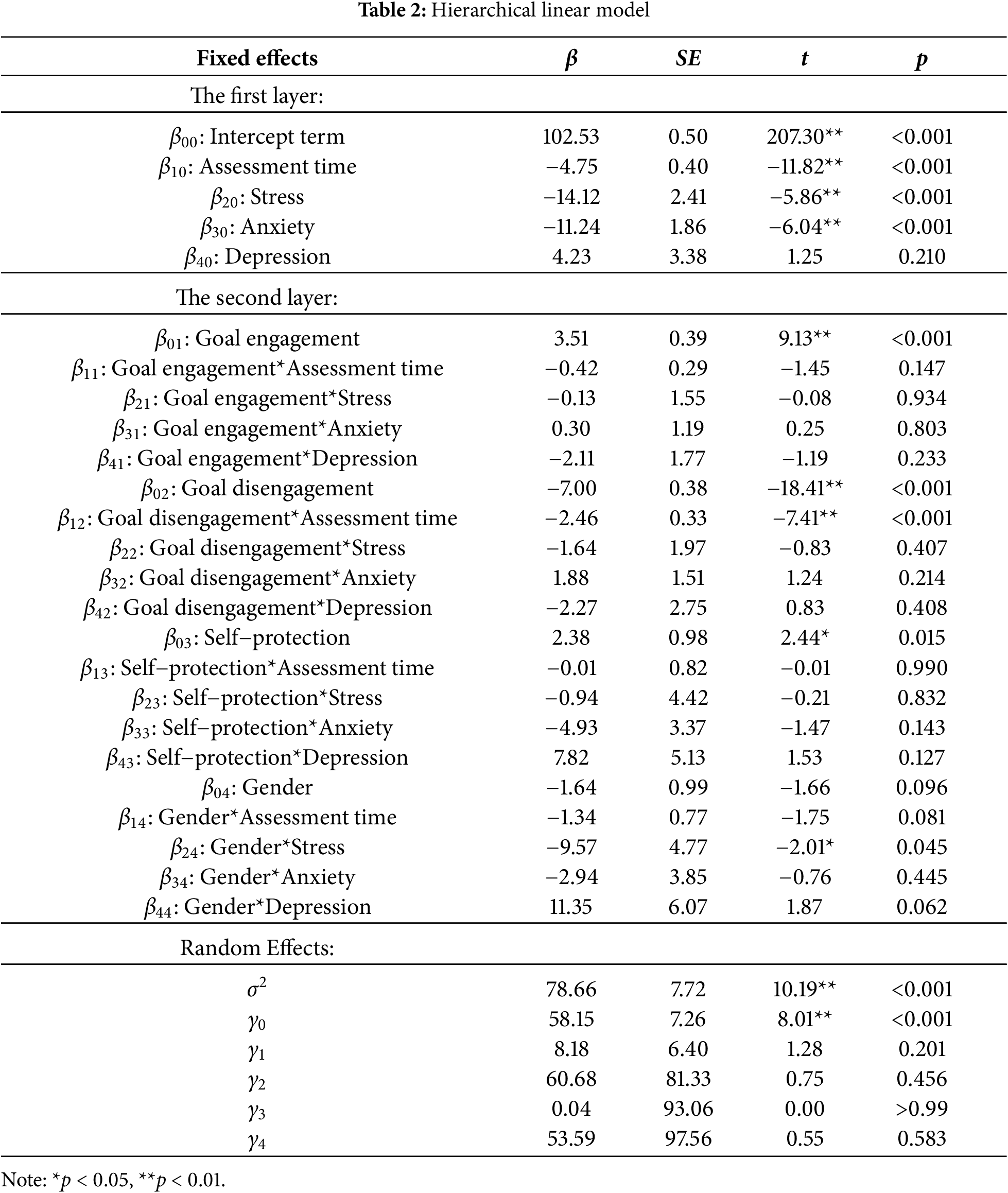
The specific results of the model are shown in Table 2, and the analysis of the model results is divided into three parts below.
3.3 The Association between Negative Emotions and the QoL
The results of the level-1 equation of the hierarchical linear model showed that the assessment time (β10 = −4.75, t = −11.82, p < 0.001) negatively predicted the QoL of the elderly. Stress (β20 = −14.12, t = −5.86, p < 0.001) and anxiety (β30 = −11.24, t = −6.04, p < 0.001) could negatively predict the quality of life in the elderly. In addition, stress and anxiety negatively predicted the QoL, while depression had no significant predictive effect on the QoL.
3.4 The Role of Control Strategy in the Development of the QoL among the Elderly
The results of the level-2 equation of the hierarchical linear model showed that the prediction of gender on the intercept of QoL was not significant (β04 = −1.64, t = −1.66, p > 0.05), and the interaction effect between gender and assessment time on QoL was also not significant (β14 = −1.34, t = −1.75, p > 0.05). It indicated that not only was there no significant difference in the QoL between male and female elderly, but also in the declining trend of QoL between both genders.
Goal engagement (β01 = 3.51, t = 9.13, p < 0.001) and self-protection (β03 = 2.38, t = 2.44, p < 0.05) significantly positively predicted QoL, and goal disengagement (β02 = −7.00, t = −18.41, p < 0.001) significantly negatively predicted QoL. This demonstrated that the elderly with higher levels of goal-engagement and self-protective strategies have better QoL. However, the higher the goal-disengagement strategy, the worse the QoL of the elderly. At the same time, the interaction between goal disengagement and assessment time negatively predicted the QoL of the elderly (β12 = −2.46, t = −7.41, p < 0.001). The interaction between goal engagement, self-protection, and assessment time was not significant in the prediction of the QoL of the elderly, indicating that the higher degree of goal-engagement strategy the elderly held, the faster their QoL declined. Meanwhile, goal engagement and self-protection have no effect on alleviating the decline of QoL in the elderly.
3.5 The Moderating Role of Control Strategies in the Prediction of Negative Emotions on QoL in the Elderly
None of the interaction effects between negative emotions and control strategies were significant in predicting QoL in the elderly, indicating that the predictive effect of negative emotions on the QoL of the elderly was not moderated by control strategies. In addition, the results of the level-2 equation of the hierarchical linear model presented that the interaction between gender and anxiety (β34 = −2.94, t = −0.76, p > 0.05) and depression (β44 = 11.35, t = 1.87, p > 0.05) was not significant in predicting the QoL of the elderly. However, the interaction between gender and stress negatively predicted the QoL of the elderly (β24 = −9.57, t = −2.01, p < 0.05), indicating that stress was a stronger negative predictor of QoL in the male elderly than in the female elderly.
Findings presented that the QoL of the elderly showed an overall downward trend during the one-year follow-up investigation. Consistent with previous studies [6,7], the QoL of the elderly gradually deteriorated with the aging process. However, when the elderly evaluated their overall QoL with a one-item, 5-point scored method, their QoL presented a more positive and stable state during the 12 years [4]. This suggested that when researchers asked older people to evaluate their own QoL by different assessments, it might appear to be completely inconsistent results.
The current study partially verified Hypothesis 1 that anxiety and stress had negative predictive effects on QoL in the elderly, while depression had no significant effect on that. Reference [6] and reference [17] found that both anxiety and depression can predict the QoL of the elderly. However, when stress was included as a predictor in this study, the predictive effect of depression on the QoL of the elderly was no longer significant. It was possible due to the fact that perceived stress played a key role in the QoL of older adults [45,46], and internal sensitivity, unease, and other stress reactions would make the QoL of the elderly more vulnerable.
Inconsistent with Hypotheses 2a and 2b, in terms of the association of the three control strategies to the QoL of the elderly, the results of the current study showed that the goal engagement and self-protective strategy could positively predict the intercept of the QoL of the elderly, but neither of them could attenuate the declining trend of the QoL of the elderly. However, goal disengagement negatively predicted the intercept of QoL in older adults, and those elderly with higher levels of possessing goal-disengagement strategies experienced a faster decline in QoL. Aligned with existing research findings, goal engagement and self-protection benefited QoL in older adults [25,28]. Although this study presented that goal-engagement and self-protective strategies did not alleviate the decline in QoL in older adults over a period of 1 year, chances were that active control strategies might mitigate the decline over a longer period. The negative associations of goal-disengagement strategies to QoL and its development in older adults didn’t cohere with previous studies [29]. Specifically, although reducing the importance of goals could protect self-esteem from being damaged, a series of negative effects on QoL cannot be ignored for the problem has not been solved. Overreliance on disengagement may result in passivity or reduced agency, which could exacerbate feelings of helplessness and accelerate QoL decline in some cases. Conversely, a balanced use of disengagement and engagement—where older adults disengage from unattainable goals while re-engaging with new, feasible ones—has been shown to foster better long-term outcomes [47]. Therefore, the combination of goal disengagement and goal reengagement strategies may be beneficial to physical health and subjective well-being [47]. In the meantime, there were cultural differences in the choice of control strategies [48]. Therefore, cultural differences may also exist in the impact of goal disengagement on QoL. Under Chinese cultural space, goal disengagement is more similar to the criticized “Ah Q spirit”, which is the approach of helpless self-consolation and may therefore not play a positive role in the QoL of the elderly in China.
The current study did not find any moderating effects of the three control strategies on the relationship between negative emotions and QoL in the elderly, which cannot confirm Hypothesis 3. As a vital adaptive function in the aging process, different control strategies can be selected alternately to achieve “successful aging” [20]. Among them, both goal-engagement strategies and self-protective strategies were beneficial to the alleviation of negative emotions in the elderly and the promotion of the health status [25,49]. Therefore, it was probable that as a regulatory strategy for psychological and physiological functions, control strategies can directly act on negative emotions and QoL of the elderly, but cannot regulate the effect of negative emotions on their QoL.
In addition, this study did not find gender differences in the QoL of the elderly. Nor did it find gender differences in the downward trend of the QoL of the elderly, which was inconsistent with the results of previous studies [50–52]. This may be due to the fact that although female elderly has a relatively low level of education, under the influence of China’s traditional culture of “men outside the home, women inside”, female elderly are better than men in terms of self-care such as diet and housework, and also have higher levels of mental resilience and active coping remedies [53]. These factors can be used as a compensation strategy to improve the QoL. Therefore, the present study did not show male superiority in the development of QoL but found that the association of female elderly’s stress to the QoL was weaker than that of male elderly.
Our study still had some limitations. First of all, the sample was only selected from the elderly group from a community in Nanjing, China, which could not represent the overall situation of the elderly. In addition, the average age of the elderly in this study was 85 years old, which was relatively older among the elderly. Therefore, whether the conclusions can be extended to the elderly in other regions or other age groups needs to be investigated. Secondly, the internal consistency of the self-protection dimension of the control strategy is low, and the evaluation tools of the control strategy need to be further optimized in the future. In addition to that, it is important to note that our use of mean values assumes a certain level of temporal stability in control strategies, which was not explicitly tested in this study. While this approach is consistent with prior literature and serves the purpose of examining general trends, future research could address this limitation by employing higher-frequency data collection or dynamic modeling methods to capture potential temporal variability. Finally, although this study used a longitudinal design with three assessments administered 6 months apart, the overall follow-up period was only 1 year, and whether the findings ensure consistency over a longer period needs to be verified. Therefore, researchers can further explore the relationship between control strategies, negative emotions, gender, and QoL in larger samples and longer tracing studies, so as to provide a clearer basis for improving the QoL of the elderly from a psychological perspective.
In conclusion, the QoL of the elderly is closely related to their anxiety and stress levels. Alleviating the anxiety and stress levels of the elderly may help to improve their QoL. Moreover, despite the range of life limitations, illnesses, and functional decline that older adults are facing, QoL can be enhanced by using positive and proactive strategies, investing resources and efforts to meet their own needs, and being able to see the positive aspects of themselves and events in the face of obstacles.
Acknowledgement: Not applicable.
Funding Statement: The authors received no specific funding for this study.
Author Contributions: Study conception and design: Chunyang Zhang, Wei Xu; data collection: Chunyang Zhang; analysis and interpretation of results: Chunyang Zhang, Ran Ma; draft manuscript preparation: Ran Ma, Wei Xu. All authors reviewed the results and approved the final version of the manuscript.
Availability of Data and Materials: The data that support the findings of this study are available from the corresponding author, Wei Xu, upon reasonable request.
Ethics Approval: All human studies have been approved by the appropriate ethics committee and have been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments (study reviewed and approved by the Institutional Review Board and Ethics Committee of the Faculty of Psychology, authors’ university; IRB number: 202012100053).
Informed Consent: Informed consent was obtained from all individual participants included in the study.
Conflicts of Interest: The authors declare no conflicts of interest to report regarding the present study.
References
1. Zhai Z, Chen J, Li L. Future trends of China’s population and aging: 2015~2100. Popul Res. 2017;41(4):60–71. [Google Scholar]
2. Russell C. The aging experience. Abingdon, UK: Talylor Francis Group; 2024. [Google Scholar]
3. Kallmyer BA, Bass D, Baumgart M, Callahan CM, Dulaney S, Evertson LC, et al. Dementia care navigation: building toward a common definition, key principles, and outcomes. Alzheimers Dement Transl Res Clin Interv. 2023;9(3):e12408. doi:10.1002/trc2.12408. [Google Scholar] [PubMed] [CrossRef]
4. Huang X, Zhang M, Fang J, Zeng Q, Wang J, Li J. Classifying and characterizing the development of self-reported overall quality of life among the Chinese elderly: a twelve-year longitudinal study. BMC Public Health. 2022;22(1):1139. doi:10.1186/s12889-022-13314-6. [Google Scholar] [PubMed] [CrossRef]
5. Zafar J, Malik NI, Atta M, Makhdoom IF, Ullah I, Manzar MD. Loneliness may mediate the relationship between depression and the quality of life among elderly with mild cognitive impairment. Psychogeriatrics. 2021;21(5):805–12. doi:10.1111/psyg.12749. [Google Scholar] [PubMed] [CrossRef]
6. Ribeiro O, Teixeira L, Araújo L, Rodríguez-Blázquez C, Calderón-Larrañaga A, Forjaz MJ. Anxiety, depression and quality of life in older adults: trajectories of influence across age. Int J Environ Res Public Health. 2020;17(23):9039. doi:10.3390/ijerph17239039. [Google Scholar] [PubMed] [CrossRef]
7. Velaithan V, Tan MM, Yu TF, Liem A, Teh PL, Su TT. The association of self-perception of aging and quality of life in older adults: a systematic review. Gerontologist. 2024;64(4):gnad041. doi:10.1093/geront/gnad041. [Google Scholar] [PubMed] [CrossRef]
8. Adolfo CS, Albougami ASB, Roque MY, Aruta JJBR, Almazan JU. An integrative review of negative emotions of older adults in later life. Nurs Forum. 2022;57(6):1452–64. doi:10.1111/nuf.12785. [Google Scholar] [PubMed] [CrossRef]
9. Sturm VE, Datta S, Roy ARK, Sible IJ, Kosik EL, Veziris CR, et al. Big smile, small self: awe walks promote prosocial positive emotions in older adults. Emotion. 2022;22(5):1044–58. doi:10.1037/emo0000876. [Google Scholar] [PubMed] [CrossRef]
10. Zsoldos I, Hot P. Limited time horizons lead to the positivity effect in attention, but not to more positive emotions: an investigation of the socioemotional selectivity theory. Psychol Aging. 2024;39(1):46–58. doi:10.1037/pag0000781. [Google Scholar] [PubMed] [CrossRef]
11. Holmes SE, Esterlis I, Mazure CM, Lim YY, Ames D, Rainey-Smith S, et al. Trajectories of depressive and anxiety symptoms in older adults: a 6-year prospective cohort study. Int J Geriatr Psychiatry. 2018;33(2):405–13. doi:10.1002/gps.4761. [Google Scholar] [PubMed] [CrossRef]
12. Thapa DK, Visentin DC, Kornhaber R, Cleary M. Prevalence and factors associated with depression, anxiety, and stress symptoms among older adults: a cross-sectional population-based study. Nurs Health Sci. 2020;22(4):1139–52. doi:10.1111/nhs.12783. [Google Scholar] [PubMed] [CrossRef]
13. Andreas S, Schulz H, Volkert J, Dehoust M, Sehner S, Suling A, et al. Prevalence of mental disorders in elderly people: the European MentDis_ICF65+ study. Br J Psychiat. 2017;210(2):125–31. doi:10.1192/bjp.bp.115.180463. [Google Scholar] [PubMed] [CrossRef]
14. Cai H, Jin Y, Liu R, Zhang Q, Su Z, Ungvari GS, et al. Global prevalence of depression in older adults: a systematic review and meta-analysis of epidemiological surveys. Asian J Psychiatr. 2023;80(8):103417. doi:10.1016/j.ajp.2022.103417. [Google Scholar] [PubMed] [CrossRef]
15. Deckx L, van den Akker M, Buntinx F, van Driel M. A systematic literature review on the association between loneliness and coping strategies. Psychol Health Med. 2018;23(8):899–916. doi:10.1080/13548506.2018.1446096. [Google Scholar] [PubMed] [CrossRef]
16. Sivertsen H, Bjørkløf GH, Engedal K, Selbæk G, Helvik AS. Depression and quality of life in older persons: a review. Dement Geriatr Cogn Disord. 2015;40(5–6):311–39. doi:10.1159/000437299. [Google Scholar] [PubMed] [CrossRef]
17. de Sousa RD, Rodrigues AM, Gregório MJ, Branco JDC, Gouveia MJ, Canhão H, et al. Anxiety and depression in the Portuguese older adults: prevalence and associated factors. Front Med. 2017;4:196. doi:10.3389/fmed.2017.00196. [Google Scholar] [PubMed] [CrossRef]
18. Muhammad T, Meher T. Association of late-life depression with cognitive impairment: evidence from a cross-sectional study among older adults in India. BMC Geriatr. 2021;21(1):364. doi:10.1186/s12877-021-02314-7. [Google Scholar] [PubMed] [CrossRef]
19. Yang C, Wang L, Zhang J, Wang W, Pi Z, Li X. The influences of affect labeling based on daily events on older adults’ subjective life quality. J Psychol Sci. 2022;45(2):331–8. [Google Scholar]
20. Heckhausen J, Schulz R. A life-span theory of control. Psychol Rev. 1995;102(2):284–304. doi:10.1037/0033-295X.102.2.284. [Google Scholar] [PubMed] [CrossRef]
21. Chipperfield JG, Perry RP. Primary- and secondary-control strategies in later life: predicting hospital outcomes in men and women. Health Psychol. 2006;25(2):226–36. doi:10.1037/0278-6133.25.2.226. [Google Scholar] [PubMed] [CrossRef]
22. Hall NC, Chipperfield JG, Heckhausen J, Perry RP. Control striving in older adults with serious health problems: a 9-year longitudinal study of survival, health, and well-being. Psychol Aging. 2010;25(2):432–45. doi:10.1037/a0019278. [Google Scholar] [PubMed] [CrossRef]
23. Bone JK, Bu F, Fluharty ME, Paul E, Sonke JK, Fancourt D. Engagement in leisure activities and depression in older adults in the United States: longitudinal evidence from the health and retirement study. Soc Sci Med. 2022;294(12):114703. doi:10.1016/j.socscimed.2022.114703. [Google Scholar] [PubMed] [CrossRef]
24. Galiana L, Tomás JM, Fernández I, Oliver A. Predicting well-being among the elderly: the role of coping strategies. Front Psychol. 2020;11:616. doi:10.3389/fpsyg.2020.00616. [Google Scholar] [PubMed] [CrossRef]
25. Gamrowska A, Steuden S. Coping with the events of daily life and quality of life of the socially active elderly. Health Psychol Rep. 2014;2(2):123–31. doi:10.5114/hpr.2014.43919. [Google Scholar] [CrossRef]
26. Holding A, Moore A, Verner-Filion J, Kachanoff F, Koestner R. Choosing to lose it: the role of autonomous motivation in goal disengagement. Motiv Emot. 2022;46(6):769–89. doi:10.1007/s11031-022-09952-3. [Google Scholar] [CrossRef]
27. Heckhausen J, Wrosch C, Schulz R. Agency and motivation in adulthood and old age. Annu Rev Psychol. 2019;70(1):191–217. doi:10.1146/annurev-psych-010418-103043. [Google Scholar] [PubMed] [CrossRef]
28. Schilling OK, Wahl HW, Boerner K, Horowitz A, Reinhardt JP, Cimarolli VR, et al. Developmental regulation with progressive vision loss: use of control strategies and affective well-being. Dev Psychol. 2016;52(4):679–94. doi:10.1037/dev0000099. [Google Scholar] [PubMed] [CrossRef]
29. Jobin J, Wrosch C. Goal disengagement capacities and severity of disease across older adulthood: the sample case of the common cold. Int J Behav Dev. 2016;40(2):137–44. doi:10.1177/0165025415597549. [Google Scholar] [CrossRef]
30. Ji LJ, Imtiaz F, Su Y, Zhang Z, Bowie AC, Chang B. Culture, aging, self-continuity, and life satisfaction. J Happiness Stud. 2022;23(8):3843–64. doi:10.1007/s10902-022-00568-5. [Google Scholar] [PubMed] [CrossRef]
31. Bakalar N. Happiness may come with age, study says. New York, NY, USA: The New York Times; 2010. [Google Scholar]
32. Livingstone KM, Isaacowitz DM. Age and emotion regulation in daily life: frequency, strategies, tactics, and effectiveness. Emotion. 2021;21(1):39–51. doi:10.1037/emo0000672. [Google Scholar] [PubMed] [CrossRef]
33. Livingstone KM, Isaacowitz DM. The roles of age and attention in general emotion regulation, reappraisal, and expressive suppression. Psychol Aging. 2018;33(3):373–83. doi:10.1037/pag0000240. [Google Scholar] [PubMed] [CrossRef]
34. Bar-Tur L. Fostering well-being in the elderly: translating theories on positive aging to practical approaches. Front Med. 2021;8:517226. doi:10.3389/fmed.2021.517226. [Google Scholar] [PubMed] [CrossRef]
35. Irving J, Davis S, Collier A. Aging with purpose: systematic search and review of literature pertaining to older adults and purpose. Int J Aging Hum Dev. 2017;85(4):403–37. doi:10.1177/0091415017702908. [Google Scholar] [PubMed] [CrossRef]
36. Fakhri M, Abdan M, Ramezanpour M, Dehkordi AH, Sarikhani D. Systematic review and meta-analysis on quality of life in diabetic patients in Iran. Int J Prev Med. 2021;12(1):41. doi:10.4103/ijpvm.IJPVM_327_19. [Google Scholar] [PubMed] [CrossRef]
37. Tonapa SI, Mulyadi M, Yusuf A, Lee BO. Longitudinal association among illness perceptions, coping, and quality of life after extremity injury. Orthop Nurs. 2023;42(2):83–91. doi:10.1097/NOR.0000000000000927. [Google Scholar] [PubMed] [CrossRef]
38. Isaacowitz DM. What do we know about aging and emotion regulation? Perspect Psychol Sci. 2022;17(6):1541–55. doi:10.1177/17456916211059819. [Google Scholar] [PubMed] [CrossRef]
39. McHorney CA, Ware JEJr, Raczek AE. The MOS 36-item short-form health survey (SF-36ii. psychometric and clinical tests of validity in measuring physical and mental health constructs. Med Care. 1993;31(3):247–63. doi:10.1097/00005650-199303000-00006. [Google Scholar] [PubMed] [CrossRef]
40. Li L, Wang HM, Shen Y. Development and psychometric tests of a Chinese version of the SF-36 health survey scales. Chin J Prev Med. 2002;36(2):109–13. [Google Scholar]
41. Lovibond PF, Lovibond SH. The structure of negative emotional states: comparison of the depression anxiety stress scales (DASS) with the beck depression and anxiety inventories. Behav Res Ther. 1995;33(3):335–43. doi:10.1016/0005-7967(94)00075-U. [Google Scholar] [PubMed] [CrossRef]
42. Gong X, Xie XY, Xu R, Luo YJ. Psychometric properties of the Chinese versions of DASS-21 in Chinese college students. Chin J Clin Psychol. 2010;18(4):443–6. [Google Scholar]
43. Heckhausen J, Wrosch C, Fleeson W. Developmental regulation before and after a developmental deadline: the sample case of biological clock for childbearing. Psychol Aging. 2001;16(3):400–13. doi:10.1037/0882-7974.16.3.400. [Google Scholar] [PubMed] [CrossRef]
44. LeBreton JM, Senter JL. Answers to 20 questions about interrater reliability and interrater agreement. Organ Res Meth. 2008;11(4):815–52. doi:10.1177/1094428106296642. [Google Scholar] [CrossRef]
45. Fateme A, Nemat SA, Abolfazl K. The development of a quality of life model based on metacognitive beliefs with the mediation role of perceived stress in the elderly. Aging Psychol. 2021;6(4):341–55. [Google Scholar]
46. McQuaid GA, Weiss CH, Said AJ, Pelphrey KA, Lee NR, Wallace GL. Increased perceived stress is negatively associated with activities of daily living and subjective quality of life in younger, middle, and older autistic adults. Autism Res. 2022;15(8):1535–49. doi:10.1002/aur.2779. [Google Scholar] [PubMed] [CrossRef]
47. Wrosch C, Scheier M. Adaptive self-regulation, subjective well-being, and physical health: the importance of goal adjustment capacities. Adv Motiv Sci. 2022;7(3):199–238. doi:10.1016/bs.adms.2019.07.001. [Google Scholar] [CrossRef]
48. Sun R, Sauter D. Sustained stress reduces the age advantages in emotional experience of older adults: commentary on carstensen et al (2020). Psychol Sci. 2021;32(12):2035–41. doi:10.1177/09567976211052476. [Google Scholar] [PubMed] [CrossRef]
49. Liebzeit D, Rutkowski R, Arbaje AI, Fields B, Werner NE. A scoping review of interventions for older adults transitioning from hospital to home. J Am Geriatr Soc. 2021;69(10):2950–62. doi:10.1111/jgs.17323. [Google Scholar] [PubMed] [CrossRef]
50. López-Ruiz VR, Huete-Alcocer N, Alfaro-Navarro JL, Nevado-Peña D. The relationship between happiness and quality of life: a model for Spanish society. PLoS One. 2021;16(11):e0259528. doi:10.1371/journal.pone.0259528. [Google Scholar] [PubMed] [CrossRef]
51. Hajian-Tilaki K, Heidari B, Hajian-Tilaki A. Are gender differences in health-related quality of life attributable to sociodemographic characteristics and chronic disease conditions in elderly people? Int J Prev Med. 2017;8(1):95. doi:10.4103/ijpvm.IJPVM_197_16. [Google Scholar] [PubMed] [CrossRef]
52. Yu T, Enkh-Amgalan N, Zorigt G, Hsu YJ, Chen HJ, Yang HY. Gender differences and burden of chronic conditions: impact on quality of life among the elderly in Taiwan. Aging Clin Exp Res. 2019;31(11):1625–33. doi:10.1007/s40520-018-1099-2. [Google Scholar] [PubMed] [CrossRef]
53. Chen PL, Tsai YL, Lin MH, Wang J. Gender differences in health promotion behaviors and quality of life among community-dwelling elderly. J Women Aging. 2018;30(3):259–74. doi:10.1080/08952841.2017.1301170. [Google Scholar] [PubMed] [CrossRef]
Cite This Article
 Copyright © 2025 The Author(s). Published by Tech Science Press.
Copyright © 2025 The Author(s). Published by Tech Science Press.This work is licensed under a Creative Commons Attribution 4.0 International License , which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
 Downloads
Downloads
 Citation Tools
Citation Tools