
 Submit a Paper
Submit a Paper Propose a Special lssue
Propose a Special lssue Open Access
Open Access
ARTICLE

Physical Activity or Organized Sport, Which Is Better for Depression? A Perspective on Attributable Healthcare Costs in Chinese Children and Adolescents
1 School of Physical Education, Shanghai University of Sport, Shanghai, China
2 College of Physical Education, Hunan University of Technology, Zhuzhou, China
3 Centre for Sport and Psycho-Social-Behavioral Research, Hunan University of Technology, Zhuzhou, China
* Corresponding Authors: Xiaojiao Sun. Email: ; Shuge Zhang. Email:
International Journal of Mental Health Promotion 2026, 28(3), 8 https://doi.org/10.32604/ijmhp.2026.073845
Received 26 September 2025; Accepted 08 January 2026; Issue published 31 March 2026
 View Full Text
View Full Text Download PDF
Download PDFAbstract
Background: Depression is a growing public health concern among Chinese children and adolescents, with substantial healthcare costs. Physical activity (PA) and organized sport are modifiable behaviours protective against depression. This study, therefore, estimated the healthcare costs of depression attributable to insufficient PA and organized sport participation. Methods: A cost-of-illness approach with population attributable fraction (PAF) was applied. Relative risks were derived from longitudinal evidence, prevalence estimates from national Chinese surveys, and depression case numbers from the Global Burden of Disease 2021. Direct healthcare costs were extrapolated from European Union estimates, adjusted to 2024 US dollars (USD), and Chinese expenditure. Sex-stratified analyses were conducted. Results: Estimated depression-related healthcare costs attributable to insufficient PA were approximately 81 million USD, compared with around 84 million USD attributable to insufficient organized sport participation. At the population level, the economic burden attributable to insufficient PA and organized sport was of a similar order of magnitude. Among boys, costs attributable to insufficient organized sport participation (approximately 57 million USD) exceeded those attributable to insufficient PA (around 39 million USD), whereas among girls, costs attributable to insufficient PA (approximately 42 million USD) were higher than those related to organized sport (around 27 million USD). These sex-specific patterns were consistent across sensitivity analyses examining uncertainty in key model parameters. Conclusions: Both insufficient PA and organized sport contribute substantially to depression-related healthcare costs, with sex-specific differences. Policies should prioritise promoting overall PA in girls and organized sport in boys to reduce depression burden and associated expenditures. The magnitude of these attributable costs indicates an economically meaningful burden that is potentially modifiable through behavioural interventions.Keywords
Depression is a leading contributor to the global burden of disease and disability, affecting an estimated 332 million people worldwide [1]. Among children and adolescents, depression is of particular concern due to its early onset, chronic course, and long-term consequences for education, social functioning, and health across the life span [2]. In China, the prevalence of depression among young people has been steadily increasing. Recent China-based meta-analytic evidence indicates that approximately 26.2% of children and adolescents exhibit depressive symptoms, with rates rising to 28.2% in high school students and exceeding 47% in certain western regions [3]. Given China’s large population base, the actual number of affected children is concerning, resulting in a pressing challenge for families, schools, and healthcare systems.
Specifically, the economic burden of depression is substantial, encompassing both direct medical expenditures and indirect costs related to lost productivity and long-term disability [4]. In high-income countries, per-case annual costs of depression are reported to exceed several thousand US dollars (USD), with healthcare costs accounting for a large proportion. Although data on depression-related expenditures in Chinese children and adolescents are still limited, evidence from adult populations suggests rapidly increasing costs, placing substantial pressure on healthcare systems [5]. It is, therefore, critical to identify modifiable risk factors for depression that can be targeted to reduce both health and economic burdens. One promising approach, commonly known to buffer against depression, is physical activity (PA) [6].
Indeed, research has well-documented insufficient PA as a risk factor for mental health problems such as depression [7,8]. On one hand, epidemiological studies consistently demonstrate that adolescents who fail to meet recommended PA guidelines face an elevated risk of depressive symptoms and disorders [9]. On the other hand, organized sport participation—representing structured, socially embedded, and often team-based forms of PA—has also been shown to provide unique psychosocial benefits, including lowering risk of depressive symptoms and disorders [10]. Despite these benefits, recent Chinese data show that only 16.6% of adolescents reported participating in organized sport over the past year, indicating that over 80% remain non-participating, and a large proportion still fail to meet recommended PA levels [11]. Insufficient PA and participation in organized sport, therefore, likely account for a prominent part of depression problems in Chinese children and adolescents.
Although organized sport is a subset of overall PA [12], it represents a socially structured mode of participation embedded within specific institutional and policy contexts. The distinction between general PA and organized sport is not intended to imply independent or separable causal constructs [13]. Rather, it reflects two policy-relevant forms of activity engagement that are subject to different intervention approaches, delivery systems, and implementation strategies. Accordingly, separate cost-attributable estimates are needed to inform alternative policy questions—such as whether to prioritise population-wide promotion of PA or targeted expansion of organized sport opportunities—rather than to suggest non-overlapping or additive causal pathways. This framing aligns the conceptual discussion with the population-attributable cost framework used in the analysis.
However, given the high prevalence of both insufficient PA and insufficient organized sport participation in Chinese children and adolescents, should policy or intervention efforts be given to prioritising promoting PA, organized sport, or equal for both? Conceptually, this question reflects a broader population health challenge, that is, how overlapping but policy-distinct forms of PA translate into differential population-level burden once exposure prevalence and behavioural context are taken into account. One approach to resolve such a key query is to estimate and compare the economic implications of depression (e.g., financial burden in the form of healthcare costs) that is attributable to insufficient PA and organized sport. That is, policy makers and stakeholders should consider prioritising a specific mental health promotion strategy for fighting against depression based on the magnitude of healthcare burden attributable to insufficient PA and organized sport participation. While existing cost-of-illness (COI) studies have largely focused on adults, we adopted the approach to target children and adolescents for attributable healthcare cost estimation in comparing insufficient PA and organized sport, aiming to inform cost-effective strategies for mental health promotion. Although previous studies in Europe, Australia, and North America have examined the health and economic impacts of different PA domains [14], evidence from China remains scarce. This provides contextually relevant insights to inform national PA and mental health promotion policies.
Accordingly, this study aimed to estimate depression-related healthcare costs attributable to insufficient PA and organized sport in the Chinese adolescent population by integrating international risk evidence with China-specific data on exposure prevalence, population structure, and healthcare costs. The following hypotheses were examined using the most recent available data (see Methods Section 2):
Hypothesis 1: Participating in insufficient organized sport is associated with a lower depression-related healthcare cost compared with insufficient PA.
Hypothesis 2: Sex differences may exist in the depression-related healthcare cost associated with insufficient PA and organized sport participation.
Hypothesis 3: The depression-related healthcare burden attributable to insufficient PA may be greater among girls, whereas the burden attributable to insufficient organized sport may be greater among boys.
2.1 General Methodological Approach
To estimate the healthcare costs of depression attributable to insufficient PA and non-participation in organized sport, a COI approach was applied [15]. The COI framework is a well-established method in health economics that quantifies the total economic burden of a disease or health condition on individuals, healthcare systems, and society [15,16]. In this study, COI estimation was based on the population attributable fraction (PAF) method, which calculates the proportion of disease cases (and corresponding costs) that can be attributed to a given risk factor. The PAFs were calculated separately for each exposure, without assuming independence or attempting to partition total disease burden across overlapping behaviours. Four types of data were required to examine our hypotheses, including: (i) relative risks (RRs) for depression associated with insufficient PA and non-participation in organized sport among children and adolescents; (ii) the prevalence of insufficient PA and in organized sport participation among Chinese children and adolescents; (iii) the healthcare cost per case of depression in Chinese children and adolescents; and (iv) the number of diagnosed depression cases in this population. More details of data sources are provided in Section 2.3 Data Sources.
Healthcare costs of depression attributable to insufficient PA were estimated using a five-step PAF approach. First, we searched the literature for adjusted RRs of depression associated with insufficient PA and non-participation in organized sport. Although adjusted RRs were not directly available in Chinese adolescents and children, hazard ratios (HRs) from the international birth cohort study were identified as suitable for conversion into RRs [17], as this study provided both RRs for insufficient PA and organized sport participation in children and adolescents. Accordingly, the target estimate of this study is the population-attributable healthcare cost of adolescent depression under current exposure of insufficient PA and organized sport participation in China, conditional on best available evidence for RRs, rather than a fully China-specific estimation. Following methodological recommendations [18,19,20], HRs were transformed into RRs by combining them with the cumulative incidence of depression observed up to age 18 years in the cohort. This ensured that the effect estimates, originally expressed on an instantaneous rate scale, were translated into cumulative risk measures appropriate for PAF calculation. Second, Levin’s formula [21] was applied to estimate the proportion of depression cases attributable to each exposure (i.e., insufficient PA vs. insufficient organized sport participation): PAF = [P × (RR − 1)]/[1 + P × (RR − 1)], where P represents the prevalence of insufficient PA or organized sport participation among Chinese children and adolescents, and RR denotes the relative risk for depression with insufficient PA or organized sport participation [17]. Third, the number of depression cases attributable to insufficient PA and organized sport participation was calculated by multiplying the PAF by the total number of depression cases in Chinese children and adolescents, stratified by sex and age group, where data allowed. Fourth, attributable healthcare costs were derived by multiplying the number of attributable cases by the average direct healthcare cost per case of depression. Cost estimates were restricted to healthcare cost (e.g., outpatient visits, inpatient care, medications). Finally, sex-stratified analyses were performed to examine potential differences in attributable costs between boys and girls. This step provided additional insights into whether insufficient PA and organized sport participation carry different economic implications across sex subgroups.
Such a PAF approach to cost estimation of depression attributable to insufficient PA and organized sport, in the present research, should be interpreted as direct healthcare cost exclusive to other possible indirect economic costs of depression (e.g., productivity loss). Although indirect costs, such as productivity losses, are often considered when using the PAF approach to estimate the economic burden of diseases, they are primarily relevant for studies focusing on adult populations, given that paid labour participation is minimal among children and adolescents [22]. For our target population (i.e., Chinese children and adolescents), estimation of indirect costs such as work- or productivity-related costs of depression is irrelevant, because this population is less than 18 years old, still attending schools, and is unlikely to generate significant work-related productivity. Therefore, indirect cost was not taken into account in the data analysis of the current research.
Due to the absence of China-specific unit healthcare cost data for depression among children and adolescents, European cost estimates were adapted to the Chinese context using a transparent, multi-step cost conversion and scaling procedure. First, the reported Europea-based healthcare cost of depression was adjusted to the reference year using the consumer price index provided by the World Bank. Second, the inflation-adjusted cost was converted to USD using annual average exchange rates provided by the World Bank [23]. Third, the converted cost was scaled to the Chinese context using the ratio of per-capita current health expenditure between China and the European Union. Per-capita health expenditure data were obtained from the World Health Organization and reflect current health expenditure expressed in USD [24]. This scaling approach was applied as a contextual adjustment to account for systematic differences in healthcare spending across health systems, rather than to imply causal inference in service utilization.
The China-contextualized unit healthcare cost was calculated as follows: China-contextualized cost (USD, 2024) = European Union cost (EURO, 2012) × (Consumer Price Index 2024/Consumer Price Index 2012) × annual exchange rate (EURO → USD, 2024) × (Per-capita current health expenditure in China/Per-capita current health expenditure in the European Union).
Sensitivity analyses were conducted to assess the robustness of the attributable healthcare cost estimates to uncertainty in key model parameters. Rather than combining multiple sources of uncertainty simultaneously, parameter-specific sensitivity analyses were performed to allow transparent attribution of variability to individual components of the model. Specifically, three sets of sensitivity analyses were conducted and presented separately. First, uncertainty in PAFs was examined by varying each PAF by ±5% around the base-case estimate [25]. Second, uncertainty in the imported RRs was assessed using alternative scenarios based on the reported confidence intervals of the original cohort study; when the lower confidence bound was below 1.0, it was truncated at 1.0 to avoid implausible negative PAFs. Third, uncertainty in healthcare costs was evaluated through cost-scaling sensitivity analyses by varying the health-expenditure ratio used to derive China-contextualised unit costs, with lower- and upper-bound scenarios defined as 75% and 125% of the base-case unit cost, respectively. Results from these sensitivity analyses are presented separately for PAFs, RRs, and healthcare costs to facilitate interpretation and to highlight the relative influence of each parameter on the attributable cost estimates.
To address concerns regarding the transportability of RRs derived from Swedish cohorts to Chinese population, we also conducted a transportability-focused sensitivity analysis by systematically attenuating and amplifying effect sizes on the logarithmic scale. Specifically, alternative RRs were generated using the transformation RRs = exp (k × ln RR), where k represents scaling factors of 0.50, 0.75, and 1.25. This approach preserves the assumed direction of association (RR ≥ 1) for all scenarios when the base-case RR exceeds unity, thereby avoiding implausible risk-reducing estimates and negative PAFs. The scaling factors were selected to reflect plausible effect heterogeneity across populations with substantially different cultural, healthcare, and PA contexts, rather than statistical uncertainty within the source cohorts. Revised RRs from each scenario were subsequently used to re-estimate PAFs and corresponding economic costs, allowing us to assess the robustness of the findings under conservative and alternative transportability assumptions.
RRs: HRs for insufficient PA and organized sport participation were obtained from the Swedish birth cohort study and converted into RRs using the cumulative incidence of depression up to age 18 years [17]. These estimates were selected because longitudinal Chinese cohort data were unavailable, and the Swedish cohort provides high-quality evidence on adolescent PA, organized sport, and depression risk. Similar approaches have been successfully used in cost estimation studies in relation to depression and other mental health problems [4,26,27].
Prevalence of exposures: Prevalence of insufficient PA and organized sport participation among Chinese children and adolescents was derived from nationally representative surveys conducted in China [28,29]. These surveys included stratification by sex and age group, allowing sex-specific PAF calculations.
Cost per case with depression: The average healthcare cost per case with depression was derived from the European Union published data by Olesen et al. [30], with the cost value of €1782. Then, this estimate was adjusted for inflation and converted into 2024 USD for better cross-country comparison of findings with existing and future studies.
Number of cases with depression: The number of diagnosed depression cases was derived from the Global Burden of Disease Study 2021. We used data on the number of cases with major depressive disorders among Chinese children and adolescents aged 10–19 years old.
All analyses were conducted using a PAF-based approach. PAFs were calculated using Levin’s formula based on exposure prevalence and RRs. Sex-specific PAFs were estimated using sex-stratified prevalence data. The number of depression cases attributable to insufficient PA and organized sport was obtained by applying the corresponding PAFs to the total number of diagnosed cases. Attributable healthcare costs were calculated by multiplying attributable case numbers by the average direct healthcare cost per case. Sensitivity analyses were performed by varying PAFs, RRs and healthcare cost. Results are reported in 2024 USD. Analyses were conducted using Microsoft Excel 2016 Version.
For RRs calculation, insufficient PA at age 11 years was consistently associated with an elevated risk of depression by age 18 years. When analysed by sex, a 21% higher risk (RR = 1.21, 95%CI: 1.00–1.48) was observed in females, whereas males showed a 40% higher risk (RR = 1.40, 95%CI: 0.94–2.10) compared with those who were sufficiently physically active. Similarly, insufficient organized sport participation at age 11 years was also associated with an elevated risk of depression by age 18 years. After converting HRs to RRs, insufficient organized sport participation was responsible for an estimated 12% higher cumulative risk of depression among females (RR = 1.12, 95%CI: 0.99–1.26) and a 53% higher risk among males (RR = 1.53, 95%CI: 1.19–1.94) compared with those who participated sufficiently in organized sports.
Based on the most recent prevalence of insufficient PA reported in Guo et al. [29] and organized sport participation reported in Liu et al. [28] in Chinese children and adolescents. Among females, the prevalence of insufficient PA was 66.0%, while among females, the prevalence was 77.0%. The prevalence of insufficient organized sport participation of males and females was 81.7% and 83.5%, respectively. The PAFs for depression with insufficient PA and organized sport participation by sex were displayed in Table 1 and Table 2, respectively.
According to the GBD Study 2021, the most recent number of cases with depression in Chinese children and adolescents by sex was 377,559 (males) and 604,686 (females), respectively. Based on the study by Olesen et al. [30] the average cost per case with depression was €1782 for depression in 2012. It was first converted into current values in 2024 and then converted into USD in 2024, after taking inflation based on the CPI (1.70) and currency exchange rate (0.92), and ratio (0.28/0.05 = 5.6) between the mean of EU member countries (0.28) and China (0.05) in terms of health spending USD per capita (in 2022) into consideration. The cost transfer from the European Union to China was calculated as follows: cost per case (China, 2024 USD) = €1782 × 1.70 (inflation adjustment) × 0.92 (EURO–USD exchange rate) × (0.28/0.05) (ratio of per-capita health expenditure), yielding approximately USD 497 per case. Accordingly, the average cost per case with depression in Chinese children and adolescents was 497 USD.
Table 1: Information summary on calculating the cost of depression attributable to insufficient physical activity in Chinese children and adolescents by sex.
| Parameter | Males | Females |
|---|---|---|
| Insufficient physical activity prevalence ratea | 66.0% | 77.0% |
| Relative risksb | 1.40 | 1.21 |
| Population attributable fraction | 20.9% | 13.9% |
| Number of cases with depressionc | 377,559 | 604,686 |
| Cost per case with depressiond | 497 | 497 |
| Total cost | 187,646,962 | 300,528,957 |
| Attributable cost | 39,192,087 | 41,812,688 |
Table 2: Information summary on calculating the cost of depression attributable to insufficient sport participation in Chinese children and adolescents by sex.
| Parameter | Males | Females |
|---|---|---|
| Insufficient organized sport participation prevalence ratea | 81.7% | 83.5% |
| Relative risks (RRs)b | 1.53 | 1.12 |
| Population attributable fraction | 30.2% | 9.1% |
| Number of cases with depressionc | 377,559 | 604,686 |
| Cost per case with depressiond (USD) | 497 | 497 |
| Total cost | 187,646,962 | 300,528,957 |
| Attributable cost (2024 USD) | 56,700,938 | 27,370,479 |
Fig. 1 presents the estimated costs of depression attributable to insufficient PA. In 2024 USD, sex-specific attributable costs were approximately 42 million for females and 39 million for males, yielding a total estimated cost of around 81 million USD. For comparison, Fig. 2 presents sex-specific depression costs attributable to insufficient organized sport participation. Estimated costs were approximately 27 million for females and 57 million for males, with a total cost of about 84 million USD.
These patterns were consistent with Hypothesis 3, indicating a higher attributable healthcare burden from insufficient PA among females and from insufficient organized sport participation among males. The observed sex-specific differences were also aligned with Hypothesis 2. However, Hypothesis 1 was not directly tested by the COI estimates, as total attributable costs reflect the joint influence of effect size and exposure prevalence rather than the comparative protective efficacy of organized sport versus overall PA.
To account for uncertainty in key model inputs, sensitivity analyses were conducted separately for PAFs, RRs, and healthcare costs. Across plausible parameter ranges, total costs attributable to insufficient PA varied from approximately 57 to 105 million USD, while estimates for insufficient organized sport participation ranged from around 60 to 108 million USD.
When uncertainty in RRs was examined, attributable costs exhibited wider variation, ranging from near zero to approximately 160 million USD for insufficient PA and from around 25 to 135 million USD for insufficient organized sport participation, reflecting assumptions regarding cross-population effect heterogeneity.
Transportability-based analyses further indicated that total attributable cost estimates were sensitive to scaling assumptions. Under conservative (k = 0.50), intermediate (k = 0.75), and scaled (k = 1.25) scenarios, estimated costs for insufficient PA ranged from approximately 41 to 100 million USD, while corresponding estimates for insufficient organized sport participation ranged from around 45 to 102 million USD.
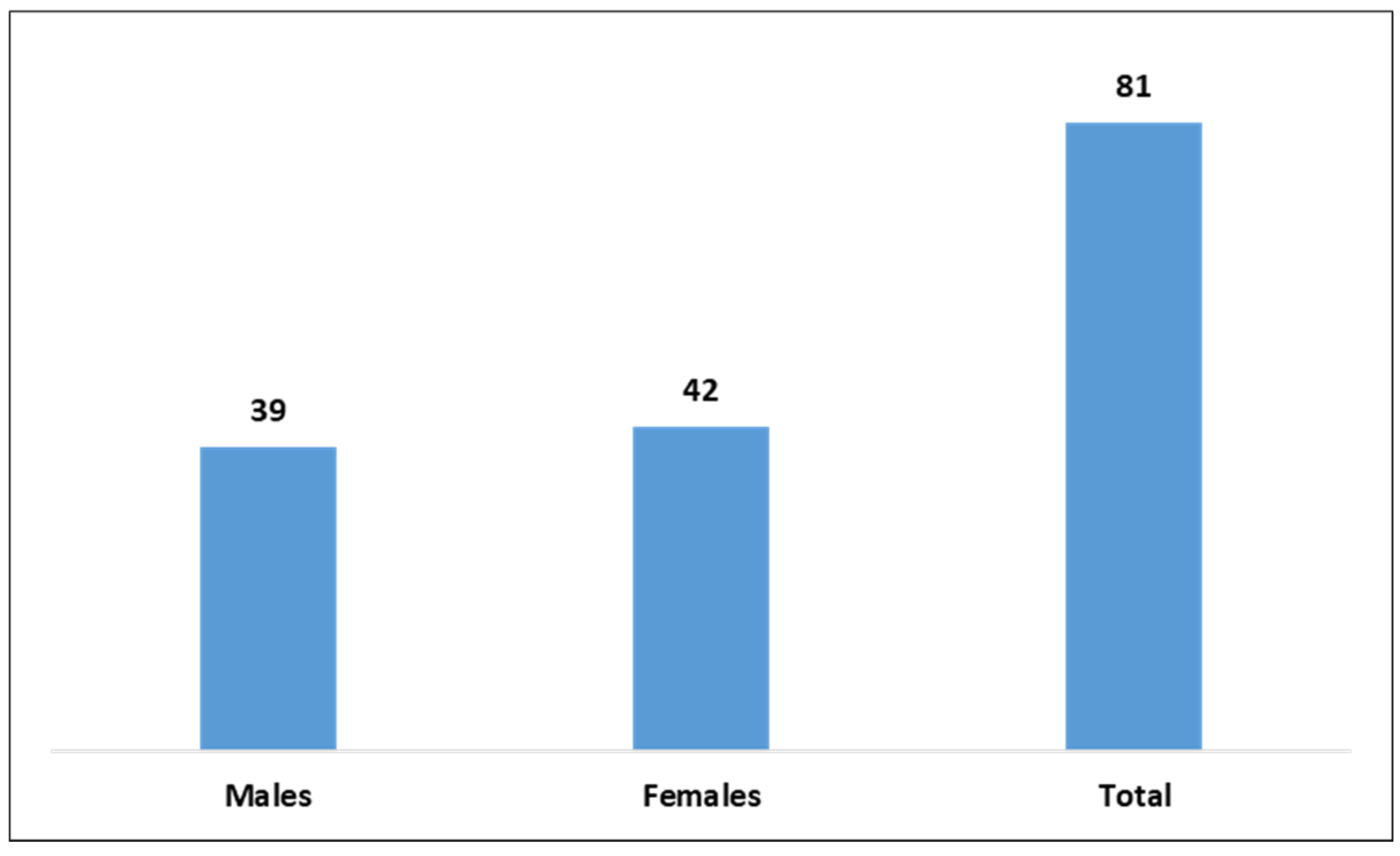
Figure 1: Cost (million, 2024 USD) of depression attributable to insufficient physical activity in Chinese children and adolescents by sex.
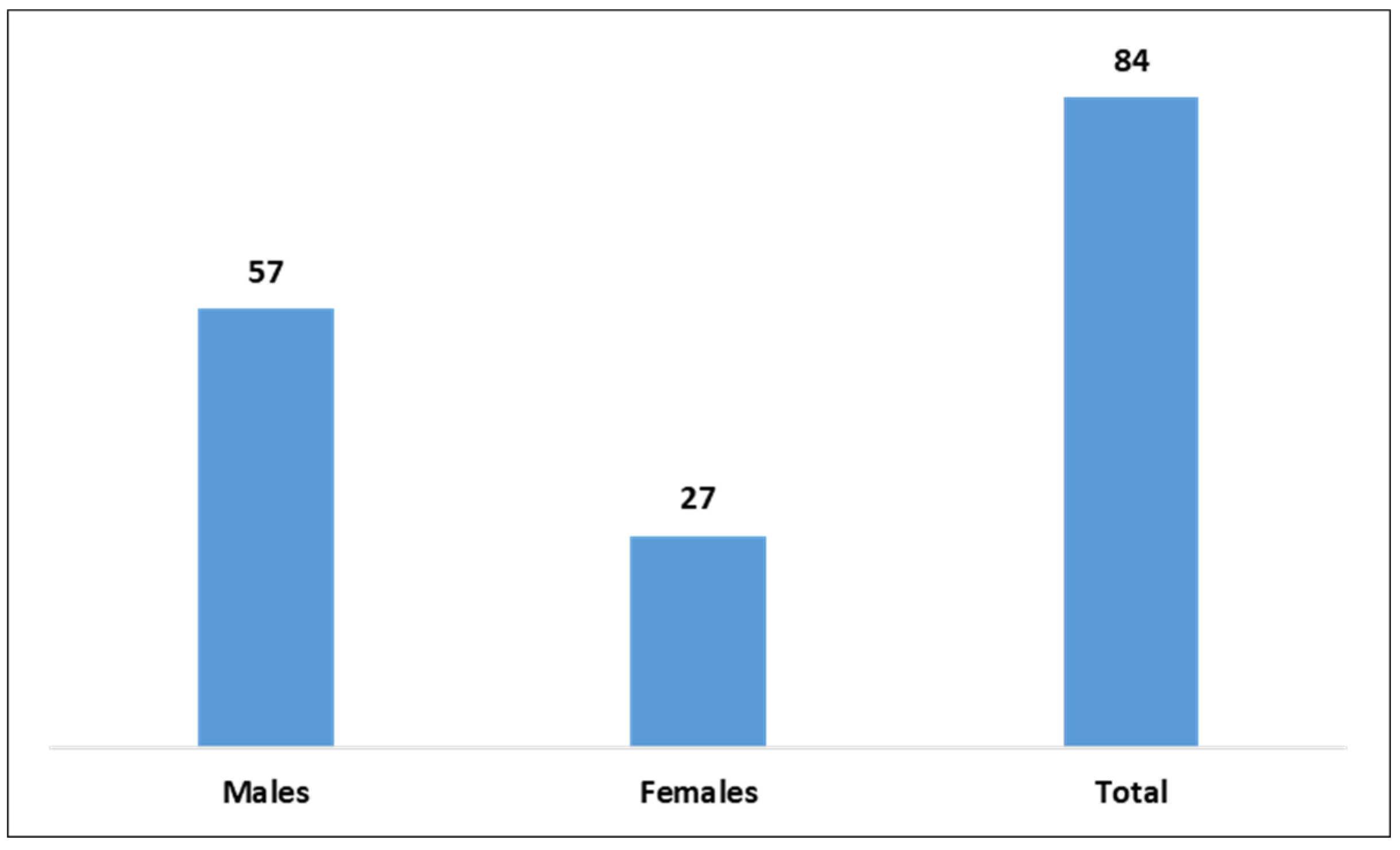
Figure 2: Cost (million, 2024 USD) of depression attributable to insufficient organized sport participation in Chinese children and adolescents by sex.
Sensitivity analyses are reported separately for PAFs, RRs, and healthcare costs, allowing the impact of uncertainty in each parameter to be examined independently. For the varying PAFs, sensitivity analysis indicated that the costs for insufficient PA may have been as low as 56.60 million (males: 29.81 million; females: 26.79 million) and as high as 105.41 million (males: 48.57 million; females: 56.84 million), and the costs of insufficient organized sport participation may have been as low as 59.66 million (males: 47.32 million; females: 12.34 million) and as high as 108.48 million (males: 66.08; females: 42.40 million).
For the varying RRs, sensitivity analysis indicated that the costs for insufficient PA may have been as low as 0 million (males: 0 million; females: 0 million) and as high as 160 million (males: 78.93 million; females: 81.07 million), and the costs of insufficient organized sport participation may have been as low as 25.21 million (males: 25.21 million; females: 0 million) and as high as 135.12 million (males: 81.51 million; females: 53.61 million).
For the varying cost per case, sensitivity analysis indicated that the costs for insufficient PA may have been as low as 60.75 million (males: 29.39 million; females: 41.81 million) and as high as 101.26 million (males: 48.99 million; females: 52.27 million), and the costs of insufficient organized sport participation may have been as low as 63.05 million (males: 42.53 million; females: 27.37 million) and as high as 105.09 million (males: 70.88 million; females: 34.21 million).
Transportability-based analyses showed that attributable cost estimates were sensitive to assumptions regarding cross-population effect heterogeneity. For insufficient PA, total attributable costs ranged from 41.40 to 99.75 million under conservative (k = 0.50) and scaled (k = 1.25) scenarios, with an estimate of 61.25 million (k = 0.75). Corresponding estimates for insufficient organized sport participation ranged from 45.10 (k = 0.5) to 101.72 million (k = 1.25), compared with an estimate of 65.46 million (k = 0.75).
This study quantified the depression-related economic cost attributable to two modifiable movement behaviours (i.e., insufficient PA and non-participation in organized sport) in Chinese children and adolescents. The economic costs of depression attributable to insufficient PA and organized sport participation were large. Relatively, the cost attributable to insufficient organized sport participation was higher than that attributable to insufficient PA. However, for sex-related comparisons, different patterns were identified, of which the cost attributable to insufficient organized sport participation was higher than insufficient PA in boys, while in girls, there was a totally opposite pattern. Despite unavoidable data imperfections, our sex-stratified cost estimates took a critical step toward a fuller accounting of the mental-health economic burden linked to insufficient PA among Chinese children and adolescents. This evidence can offer actionable messages for policy prioritisation, funding allocation, and program commissioning across education and health sectors.
Although some epidemiological parameters were derived from non-Chinese cohorts, this study estimates depression-related healthcare costs attributable to insufficient PA and organized sport within the Chinese adolescent population by integrating international risk evidence with China-specific data on exposure prevalence, population structure, and healthcare costs. The findings should therefore be interpreted within this contextualized estimation framework. Moreover, PA and organized sport participation are inherently overlapping and nested behaviours. Accordingly, the separate population-attributable cost estimates presented in this study should not be interpreted as independent or additive components of total depression-related healthcare costs. Rather, each estimate represents a policy-relevant counterfactual scenario addressing a distinct intervention focus. As such, the estimates are not intended to be summed or compared as mutually exclusive causal contributions. The resulting estimates should therefore be interpreted as policy-oriented, context-specific attributable costs, rather than as evidence of independent causal effects of two mechanically linked exposures (i.e., organized sport and overall PA). Conceptually, this framing advances a population-level prevention perspective by illustrating how overlapping but policy-distinct forms of PA can generate different economic burden profiles, depending on exposure prevalence and behavioural context.
Our results indicated that a substantial proportion of depression-related healthcare costs was attributable to insufficient PA or non-participation in organized sport. Building on this result, the relative attributable cost is determined by three factors, including the population exposure prevalence, the baseline level of depression-related healthcare expenditure, and the strength of the association between depression and PA [13]. Given the high prevalences observed (two-thirds for insufficient PA prevalence rate and >80% for non-participation sport prevalence rate), it is likely that the cost attributable to insufficient PA or organized sport participation would be high, even modest RRs translate into PAFs. Based on these findings, addressing the prevalence of insufficient PA and organized sport participation in Chinese children and adolescents would be an economical approach to reduce the economic burden of depression.
This study found that the costs of depression attributable to insufficient PA and organized sport participation were comparable. In our data, for insufficient PA and organized sport participation, their resultant PAFs fall in the same range, which yielded similar total attributable costs. Nevertheless, this comparability does not imply interchangeability when considering which is important in saving more money caused by depression [32]. This is because the two exposures reflect different domains, which insufficient PA captured all activity domains (e.g., transport, leisure), whereas organized sport participation added structured, socially embedded participation [13]. Given that these two behaviours are related, we reported specific total costs separately and recommend targeted strategies. Beyond the results related to cost attributable to insufficient PA and organized sport participation, it is needed to consider the effectiveness of interventions based on overall PA or interventions based on organized sport participation in the different settings [33]. Despite this, our findings are still useful to inform the public that depression-related interventions based on PA or organized sport participation could have economic benefits.
However, sex-stratified results further revealed different cost-related patterns. Specifically, for girls, a higher prevalence of insufficient PA yielded a higher attributable cost, whereas among boys, the cost linked to organized-sport non-participation was comparatively greater. Two possible explanations for why the depression cost attributable to non-participation in organized sport should be mentioned. One explanation is based on the utilised epidemiological statistics for economic cost estimation [4]. Among boys, the prevalence of non-participation in organized sport was markedly higher than that of insufficient overall PA, which amplified the corresponding PAF. When combined with an RR indicating a consistent elevation in depression risk for non-participants in sport activity, this resulted in a comparatively greater proportion of depression cases attributable to the exposure, and thus higher costs, being attributable to insufficient organized sport participation. Second, from a psychosocial perspective, organized sport relates more than energy expenditure [34]. It provides structured habits, social connectedness, role identity, and adult mentorship, all of which are protective for mood regulation and resilience. Absence of such participation take off both physiological and psychosocial benefits, which can yield an effect size comparable to, or even greater than, failing to achieve sufficient PA [34,35]. In addition, boys who do not engage in organized sport often display co-occurring risk patterns, including higher sedentary time, irregular sleep, and lower self-efficacy. These factors compound vulnerability to depression and increase service utilization, further inflating economic impact. While sufficient PA mainly reflects energy expenditure, organized sport integrates structured schedules, teamwork, goal setting, and mentorship, which together foster self-discipline, social bonds, and a sense of belonging [12]. These elements address not only the biological mechanisms of activity but also the psychological and social determinants of mental health [36]. As a result, organized sport may provide more consistent and durable protection against depression in boys. Taken together, the higher exposure prevalence, and the broader psychosocial aspects associated with organized sport provide for why the depression cost attributable to organized-sport non-participation exceeds that attributable to insufficient PA in boys.
When comparing insufficient PA and organized sport participation, distinct cost-related patterns emerged across sex groups. Across sexes, insufficient PA imposed higher costs among girls, while insufficient sport participation was more costly among boys, reflecting differences in prevalence and psychosocial benefits. The sex-stratified analysis further confirmed that adolescent boys were particularly vulnerable to sport non-participation, whereas adolescent girls were more affected by insufficient PA. These findings suggest that sex- and age-tailored strategies—promoting overall PA for girls and organized sport for boys—may achieve the greatest economic benefits.
While the methodological framework is informed by prior COI studies, the present analysis contributes new contextual evidence by adapting the approach to the Chinese population and healthcare system. The integration of some China-based data provides a more policy-relevant estimate of the potential economic benefits of promoting different types of PA within China’s public health action plans.
4.1 Public Health Implications
The present findings suggest that promoting PA may be economically relevant for adolescent depression prevention in China, while the empirical uncertainty of the estimates warrants cautious interpretation. At a macro-policy level, the results underscore the importance of strengthening population-wide PA promotion as part of broader mental health and prevention strategies. Based on this perspective, organized sport may be considered as one potential, but not exclusive, means of supporting PA participation. Consideration of organized sport should be embedded within broader PA promotion efforts and informed by contextual evaluation of feasibility, equity, and acceptability. Given the limited China-specific evidence on sociocultural moderators, observed sex-stratified patterns should be treated as exploratory signals, and any differentiated approaches should be tested and validated in local contexts before informing policy or practice. Overall, the study highlights the need for context-sensitive approaches to PA promotion, alongside further investment in China-specific surveillance and longitudinal research, to better inform future mental health–oriented PA policies.
This study has several limitations. First, PA-related and mental health measures were self-reported, which may underestimate the true attributable cost. Second, due to data limitations, RRs and some certain cost parameters were derived from non-Chinese populations. Although consistent with international COI approach, this limits contextual validity and requires cautious interpretation. Accordingly, the findings should be viewed as scenario-dependent estimates rather than precise causal effects, highlighting the need for China-specific longitudinal RRs and cost data. Third, this study estimated direct healthcare costs only and excluded indirect costs, such as parental productivity loss and school disruption, due to the absence of age-specific Chinese data. As indirect costs often constitute a substantial share of the total economic cost, the reported estimates likely represent conservative lower-bound estimates of the overall societal burden.
Substantial depression-related healthcare costs were attributable to insufficient PA and organized sport among Chinese children and adolescents. Sex-stratified analyses revealed distinct and contrasting cost patterns between boys and girls, indicating sex-specific differences in the economic cost associated with these behaviours. Reducing the prevalence of insufficient PA and organized sport participation may represent a cost-relevant strategy for mitigating depression-related healthcare costs. Accordingly, interventions promoting overall PA and access to organized sport participation should be prioritised, with sex-specific considerations in intervention design. In particular, policies should address structural and financial access barriers that may limit girls’ and socioeconomically disadvantaged groups’ participation in organized sport, to ensure equitable benefits of sport-based interventions. Future research using population-based Chinese data is needed to refine cost estimates and to evaluate the long-term economic impacts of targeted intervention strategies.
Acknowledgement:
Funding Statement: The authors received no specific funding.
Author Contributions: The authors confirm contribution to the paper as follows: Conceptualization, Xiaojiao Sun and Shuge Zhang; methodology, Xiaojiao Sun; formal analysis, Xiaojiao Sun; investigation, Xiaojiao Sun; writing—original draft preparation, Xiaojiao Sun; writing—review and editing, Xiaojiao Sun and Shuge Zhang; supervision, Shuge Zhang. All authors reviewed and approved the final version of the manuscript.
Availability of Data and Materials: Data were derived from published research detailed in Section 2.3 (Data Sources) prior to combining for data analysis. The data that support the findings of this study are available from the lead author (Xiaojiao Sun) upon reasonable request.
Ethics Approval: Not applicable.
Conflicts of Interest: The authors declare no conflicts of interest.
Abbreviations
| PA | Physical activity |
| PAF | Population attributable fraction |
| COI | Cost-of-illness |
| RRs | Relative risks |
References
1. Depressive disorder (depression) [Internet]. [cited 2025 Sep 1]. Available from: https://www.who.int/news-room/fact-sheets/detail/depression. [Google Scholar]
2. Thapar A , Collishaw S , Pine DS , Thapar AK . Depression in adolescence. Lancet. 2012; 379( 9820): 1056– 67. doi:10.1016/S0140-6736(11)60871-4. [Google Scholar] [CrossRef]
3. Zhou J , Liu Y , Ma J , Feng Z , Hu J , Hu J , et al. Prevalence of depressive symptoms among children and adolescents in China: A systematic review and meta-analysis. Child Adolesc Psychiatry Ment Health. 2024; 18( 1): 150. doi:10.1186/s13034-024-00841-w. [Google Scholar] [CrossRef]
4. Chisholm D , Sweeny K , Sheehan P , Rasmussen B , Smit F , Cuijpers P , et al. Scaling-up treatment of depression and anxiety: A global return on investment analysis. Lancet Psychiatry. 2016; 3( 5): 415– 24. doi:10.1016/S2215-0366(16)30024-4. [Google Scholar] [CrossRef]
5. Hu TW , He Y , Zhang M , Chen N . Economic costs of depression in China. Soc Psychiatry Psychiatr Epidemiol. 2007; 42( 2): 110– 6. doi:10.1007/s00127-006-0151-2. [Google Scholar] [CrossRef]
6. Schuch FB , Vancampfort D , Firth J , Rosenbaum S , Ward PB , Silva ES , et al. Physical activity and incident depression: A meta-analysis of prospective cohort studies. Am J Psychiatry. 2018; 175( 7): 631– 48. doi:10.1176/appi.ajp.2018.17111194. [Google Scholar] [CrossRef]
7. Hou J , Deng Q , Sha L , Zhu J , Xiang R , Zhao X , et al. Physical activity and risk of depression in adolescents: A systematic review and meta-analysis of prospective observational studies. J Affect Disord. 2025; 371: 279– 88. doi:10.1016/j.jad.2024.11.065. [Google Scholar] [CrossRef]
8. Pearce M , Garcia L , Abbas A , Strain T , Schuch FB , Golubic R , et al. Association between physical activity and risk of depression: A systematic review and meta-analysis. JAMA Psychiatry. 2022; 79( 6): 550– 9. doi:10.1001/jamapsychiatry.2022.0609. [Google Scholar] [CrossRef]
9. Zahl T , Steinsbekk S , Wichstrøm L . Physical activity, sedentary behavior, and symptoms of major depression in middle childhood. Pediatrics. 2017; 139( 2): e20161711. doi:10.1542/peds.2016-1711. [Google Scholar] [CrossRef]
10. Ramer JD , DuBois DL , Duncan RJ , Bustamante AS , Vandell DL , Marquez DX , et al. Childhood predictors of high school sport participation and effects of participation on young adult activity and mental health. Ann Med. 2025; 57( 1): 2447905. doi:10.1080/07853890.2024.2447905. [Google Scholar] [CrossRef]
11. Ren T , Yan J , Sun Q . Sociodemographic correlates of organized sports participation in a sample of middle school students in China. Front Public Health. 2021; 9: 730555. doi:10.3389/fpubh.2021.730555. [Google Scholar] [CrossRef]
12. Nelson HJ , Spurr S , Bally JMG . The benefits and barriers of sport for children from low-income settings: An integrative literature review. Sage Open. 2022; 12: 21582440221087272. doi:10.1177/21582440221087272. [Google Scholar] [CrossRef]
13. Westerbeek H , Eime R . The physical activity and sport participation framework-a policy model toward being physically active across the lifespan. Front Sports Act Living. 2021; 3: 608593. doi:10.3389/fspor.2021.608593. [Google Scholar] [CrossRef]
14. Ding D , Kolbe-Alexander T , Nguyen B , Katzmarzyk PT , Pratt M , Lawson KD . The economic burden of physical inactivity: A systematic review and critical appraisal. Br J Sports Med. 2017; 51( 19): 1392– 409. doi:10.1136/bjsports-2016-097385. [Google Scholar] [CrossRef]
15. Ribeiro TD , Peralta M , Ribeiro T , Marques A . Individual, social and economic burden of depression and physical inactivity. In: Physical activity, physical fitness and depression. New York, NY, USA: Routledge; 2025. p. 23– 34. doi:10.4324/9781003478539-2. [Google Scholar] [CrossRef]
16. Doran CM , Kinchin I . A review of the economic impact of mental illness. Aust Health Rev. 2019; 43( 1): 43– 8. doi:10.1071/ah16115. [Google Scholar] [CrossRef]
17. Lundgren O , Tigerstrand H , Lebena A , Löf M , Ludvigsson J . Impact of physical activity on the incidence of psychiatric conditions during childhood: A longitudinal Swedish birth cohort study. Br J Sports Med. 2025; 59( 14): e108148. doi:10.1136/bjsports-2024-108148. [Google Scholar] [CrossRef]
18. Laaksonen MA , Härkänen T , Knekt P , Virtala E , Oja H . Estimation of population attributable fraction (PAF) for disease occurrence in a cohort study design. Stat Med. 2010; 29( 7–8): 860– 74. doi:10.1002/sim.3792. [Google Scholar] [CrossRef]
19. Laaksonen MA , Knekt P , Härkänen T , Virtala E , Oja H . Estimation of the population attributable fraction for mortality in a cohort study using a piecewise constant hazards model. Am J Epidemiol. 2010; 171( 7): 837– 47. doi:10.1093/aje/kwp457. [Google Scholar] [CrossRef]
20. Samuelsen SO , Eide GE . Attributable fractions with survival data. Stat Med. 2008; 27( 9): 1447– 67. doi:10.1002/sim.3022. [Google Scholar] [CrossRef]
21. Levin ML . The occurrence of lung cancer in man. Acta Unio Int Contra Cancrum. 1953; 9( 3): 531– 41. [Google Scholar]
22. Krol M , Brouwer W , Rutten F . Productivity costs in economic evaluations: Past, present, future. Pharmacoeconomics. 2013; 31( 7): 537– 49. doi:10.1007/s40273-013-0056-3. [Google Scholar] [CrossRef]
23. Inflation, consumer prices (annual %) [Internet]. [cited 2025 Sep 1]. Available from: https://data.worldbank.org/indicator/FP.CPI.TOTL.ZG. [Google Scholar]
24. Global health expenditure databases [Internet]. [cited 2025 Sep 1]. Available from: https://apps.who.int/nha/database/. [Google Scholar]
25. Mukadam N , Sommerlad A , Huntley J , Livingston G . Population attributable fractions for risk factors for dementia in low-income and middle-income countries: An analysis using cross-sectional survey data. Lancet Glob Health. 2019; 7( 5): e596– 603. doi:10.1016/S2214-109X(19)30074-9. [Google Scholar] [CrossRef]
26. Trautmann S , Rehm J , Wittchen HU . The economic costs of mental disorders: Do our societies react appropriately to the burden of mental disorders? EMBO Rep. 2016; 17( 9): 1245– 9. doi:10.15252/embr.201642951. [Google Scholar] [CrossRef]
27. GBD 2019 Diseases and Injuries Collaborators . Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the global burden of disease study 2019. Lancet. 2020; 396( 10258): 1204– 22. doi:10.1016/S0140-6736(20)30925-9. [Google Scholar] [CrossRef]
28. Liu Y , Ke Y , Liang Y , Zhu Z , Cao Z , Zhuang J , et al. Results from the China 2022 report card on physical activity for children and adolescents. J Exerc Sci Fit. 2023; 21( 1): 1– 5. doi:10.1016/j.jesf.2022.10.004. [Google Scholar] [CrossRef]
29. Guo M , Zhu Y , Wang X . Physical activity and recreational screen time among Chinese children and adolescents: A national cross-sectional study. Front Public Health. 2024; 12: 1376330. doi:10.3389/fpubh.2024.1376330. [Google Scholar] [CrossRef]
30. Olesen J , Gustavsson A , Svensson M , Wittchen HU , Jönsson B . The economic cost of brain disorders in Europe. Eur J Neurol. 2012; 19( 1): 155– 62. doi:10.1111/j.1468-1331.2011.03590.x. [Google Scholar] [CrossRef]
31. Global burden of disease study 2021 (GBD 2021) data resources [Internet]. [cited 2025 Sep 1]. Available from: https://ghdx.healthdata.org/gbd-2021. [Google Scholar]
32. Keane L , Hoare E , Richards J , Bauman A , Bellew W . Methods for quantifying the social and economic value of sport and active recreation: A critical review. Sport Soc. 2019; 22( 12): 2203– 23. doi:10.1080/17430437.2019.1567497. [Google Scholar] [CrossRef]
33. Miller K , Kaja S , Adler S . 109. healthcare providers’ perspectives on developing a physical activity intervention for trans and gender diverse adolescents. J Adolesc Health. 2025; 76( 3): S56– 7. doi:10.1016/j.jadohealth.2024.11.125. [Google Scholar] [CrossRef]
34. Eime RM , Young JA , Harvey JT , Charity MJ , Payne WR . A systematic review of the psychological and social benefits of participation in sport for children and adolescents: Informing development of a conceptual model of health through sport. Int J Behav Nutr Phys Act. 2013; 10: 98. doi:10.1186/1479-5868-10-98. [Google Scholar] [CrossRef]
35. Engeroff T , Füzéki E , Vogt L , Banzer W . Breaking up sedentary time, physical activity and lipoprotein metabolism. J Sci Med Sport. 2017; 20( 7): 678– 83. doi:10.1016/j.jsams.2016.11.018. [Google Scholar] [CrossRef]
36. Lubans D , Richards J , Hillman C , Faulkner G , Beauchamp M , Nilsson M , et al. Physical activity for cognitive and mental health in youth: A systematic review of mechanisms. Pediatrics. 2016; 138( 3): e20161642. doi:10.1542/peds.2016-1642. [Google Scholar] [CrossRef]
Cite This Article
 Copyright © 2026 The Author(s). Published by Tech Science Press.
Copyright © 2026 The Author(s). Published by Tech Science Press.This work is licensed under a Creative Commons Attribution 4.0 International License , which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
 Downloads
Downloads
 Citation Tools
Citation Tools