
 Submit a Paper
Submit a Paper Propose a Special lssue
Propose a Special lssue Open Access
Open Access
ARTICLE

Investigating the Cultural Moderating Role in the Association between Exercise and Anxiety Symptoms
1 Department of Applied Social Sciences, The Hong Kong Polytechnic University, Kowloon, Hong Kong, China
2 Faculty of Humanities and Social Sciences, Macao Polytechnic University, Macao, China
* Corresponding Author: Albert Jiansong Zheng. Email:
International Journal of Mental Health Promotion 2026, 28(3), 9 https://doi.org/10.32604/ijmhp.2026.077733
Received 16 December 2025; Accepted 06 February 2026; Issue published 31 March 2026
 View Full Text
View Full Text Download PDF
Download PDFAbstract
Background: The anxiolytic benefits of exercise appear to vary across societies, yet limited research has examined how cultural norms shape this association. To address this gap, the present study investigates the moderating role of societal individualism–collectivism in the relation between exercise and anxiety symptoms. Methods: Using a sample of 123,298 individuals across 23 societies and two waves from the Global Flourishing Study, weighted multilevel models were employed to examine the lagged association between exercise at Wave 1 and anxiety symptoms at Wave 2, with and without adjustment for exercise at Wave 2. We further examined the cross-level moderating role of society-level individualism–collectivism in the individual-level association between Wave 1 exercise and Wave 2 anxiety symptoms. Results: The results indicate that exercise at Wave 1 is significantly associated with lower anxiety symptoms at Wave 2 in the basic lagged model. However, the association between Wave 1 exercise and Wave 2 anxiety symptoms attenuates after accounting for exercise at Wave 2, which shows a stronger association with anxiety symptoms at Wave 2 and a larger magnitude of association. Cross-level analyses further demonstrate that the lagged association between Wave 1 exercise and Wave 2 anxiety is more pronounced in collectivist societies and negligible in individualistic societies. Conclusions: These findings contribute theoretically to public mental health and cross-cultural research by elucidating the cultural moderation of the correlation between exercise and anxiety symptoms. From a practical perspective, culturally tailored approaches to encourage exercise for anxiety reduction are essential. In collectivist societies, group-based and community-oriented exercise may better support the long-term emotional benefits of sustained activity, whereas in individualistic societies, interventions may need to emphasize intrinsic motivation to enhance the mental health benefits of exercise.Keywords
Although randomized controlled trials have established the anxiolytic benefits of exercise [1,2,3], the extent to which these effects vary across different cultural contexts remains insufficiently understood. Individuals from different societies may report varying associations between exercise and anxiety symptoms, partly because the meaning and function of exercise differ across sociocultural environments [4]. For instance, in more collectivistic societies, such as East Asian regions, exercise is often viewed as a context for social interaction, and group-based activities may amplify anxiolytic effects through enhanced social connectedness [5]. In contrast, individuals in more individualistic societies, such as Ireland and the United States, tend to approach exercise primarily as a health-promotion behavior aimed at improving physical fitness or body image, which may shape its psychological benefits in different ways [6,7].
Exercise is a subset of physical activity characterized as structured, repetitive, and purposeful movement undertaken to improve health [1]. Given that individuals engage in exercise with explicit health-related intentions, these intentions are often shaped and regulated by cultural norms [4]. In this case, cultural frameworks may play a crucial role in shaping the anxiolytic effects of exercise. However, while sport sciences have traditionally emphasized the neurobiological outcomes of physical exercise, psychological research has focused more on its psychological mechanisms [8]. Despite these disciplinary advances, cross-cultural differences in the anxiolytic benefits of exercise remain insufficiently examined, particularly in studies involving multiple national comparisons. To address this gap, the present study draws on data from the large-scale and cross-societal Global Flourishing Study to examine how the association between exercise and anxiety symptoms may vary across cultural contexts [9].
Previous studies have shown that the health-related benefits of exercise vary by frequency, duration, intensity, and type, often revealing non-linear associations between exercise and health outcomes [10,11]. Nevertheless, meta-analytic evidence consistently supports the anxiolytic effects of exercise [3], indicating that individuals who engage in regular physical activity tend to report moderately lower levels of anxiety [12]. Building on this evidence, exercise can be conceptualized as a potential treatment for anxiety. In this study, we employ a binary indicator of whether respondents exercised in the past week to operationalize exercise as an intervention-like exposure.
Both recent exercise and prior exercise are possibly associated with anxiety symptoms, although their patterns of association appear to differ [13]. Recent exercise is more closely linked to immediate physiological responses, such as increased serotonin release and elevated brain-derived neurotrophic factor (BDNF), which are relevant to short-term emotional regulation [8]. While associations between anxiety symptoms and earlier or more sustained exercise tend to be weaker, they are more likely to reflect the social dimensions of exercise, including continued participation in socially embedded exercise, whose psychological correlates accumulate more gradually over time [14].
Cross-sectional evidence using the duration of exercise in the past week or month generally supports its association with reduced anxiety symptoms [15]. However, cross-sectional measures cannot capture the effects of long-term or habitual exercise [13]. To address these limitations, the present study uses the Global Flourishing Study, a two-wave, large-scale dataset, to examine the lagged association between sustained exercise behavior and later anxiety symptoms [9]. A two-wave design is sufficient for the main claim of this study as it allows recent and prior exercise to be temporally ordered and examined in relation to later anxiety symptoms while controlling for baseline anxiety [16]. However, while this design supports inferences about temporal associations, it cannot capture longer-term trajectories or establish causal effects [17].
This study makes several potential contributions. Theoretically, it advances research on exercise and anxiety symptoms by moving beyond unidirectional frameworks and demonstrating a lagged association between exercise and subsequent anxiety symptoms across societies. Methodologically, it leverages large-scale longitudinal and multilevel data to overcome limitations inherent in prior cross-sectional studies and to examine these associations across diverse cultural contexts. Practically, the findings offer implications for the development of culturally sensitive interventions and public mental health policies that promote physical activity as a means of alleviating anxiety symptoms, particularly in collectivistic societies.
The aims of this study are to examine (1) the association between initial exercise levels and later anxiety symptoms, and (2) the moderating role of societal individualism versus collectivism in this lagged association. This study contributes to the existing literature by examining the cross-level moderating role of societal individualism versus collectivism in the lagged association between exercise and anxiety symptoms. Specifically, the predictive role of baseline exercise on subsequent anxiety may vary across societies with differing levels of individualism versus collectivism. Because anxiety symptoms are also shaped by both demographic characteristics and broader societal conditions, we include individual-level age and gender [18,19], as well as the Human Development Index at the society-level as control variables [20]. The overall research framework is presented in Fig. 1.
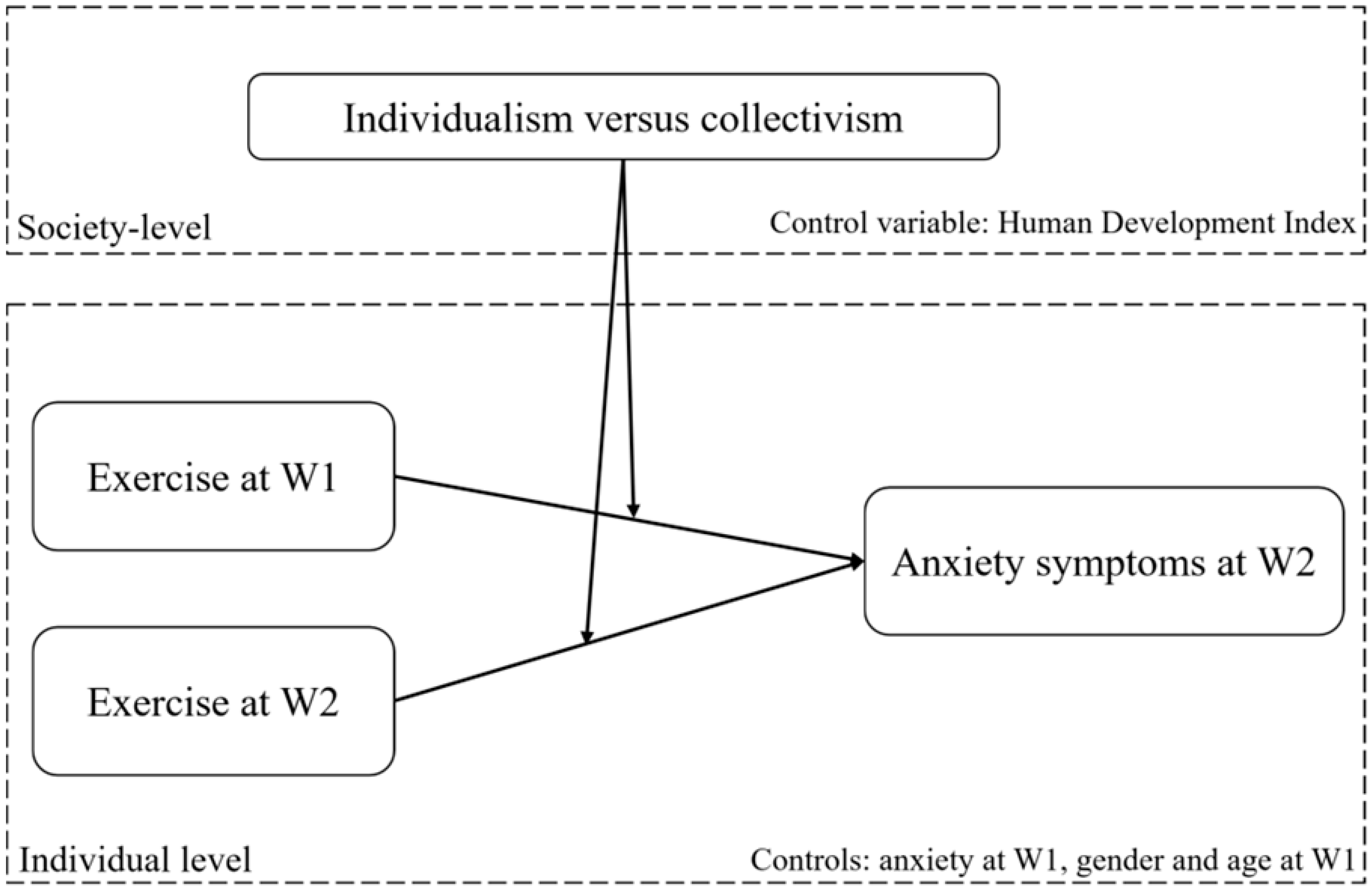
Figure 1: Research framework. Notes. W1 = Wave 1, W2 = Wave 2.
2 Literature Review and Hypotheses
There is substantial evidence for the anxiolytic effects of exercise, and randomized controlled trials (RCTs) have consistently demonstrated that exercise reduces anxiety symptoms [1]. However, most RCTs evaluate short-term outcomes and rely on designs that do not capture long-term behavioral patterns [13]. Consequently, relatively little research has examined whether habitual or prior exercise behavior is associated with subsequent anxiety symptoms over extended periods. In this context, it is necessary to investigate the lagged association between earlier exercise engagement and later anxiety symptoms.
Neurobiological evidence shows that regular aerobic exercise can increase serotonin levels, which in turn helps regulate mood and reduce anxiety [21]. In addition, exercise-induced neuroplastic changes, such as enhanced BDNF, have been shown to improve neural functioning and alleviate anxiety symptoms [22,23]. However, increases in serotonin and BDNF tend to occur rapidly following exercise and may be relatively short-lived [8]. These neurobiological mechanisms may account for the short-term anxiolytic effects of exercise, but they may be insufficient to explain the potential long-term impact of exercise on anxiety symptoms [24].
Psychological mechanisms may offer a plausible explanation for the longer-term associations between exercise and reduced anxiety symptoms [25]. Specifically, engaging in physical activity can distract individuals from negative thoughts and worries, decrease rumination, and alleviate stress [26]. Exercise may also enhance feelings of mastery and self-efficacy, promote relaxation through endorphin and related neurochemical release, and facilitate social interaction [8]. Collectively, these mechanisms may contribute to sustained reductions in anxiety symptoms associated with regular exercise over time [5,27].
Based on these considerations, we proposed the following hypothesis:
Hypothesis 1: Baseline exercise is associated with reduced subsequent anxiety symptoms.
Across different societies, the anxiolytic effects of exercise may vary. This variability may help explain why meta-analyses of RCTs on exercise and anxiety typically report only moderate effect sizes [1]. Given the social dimension of physical activity, collectivist societies, where group-based exercise is more culturally normative, may derive additional benefits through enhanced social support, greater social engagement, and reduced feelings of isolation [14]. These social resources are particularly relevant for mitigating anxiety symptoms [28,29].
In collectivist societies, supportive environments for group-based activities are strongly encouraged, which can enhance participants’ confidence, foster a sense of belonging, and reduce feelings of facing challenges alone [30]. Encouragement, shared laughter, and collective participation in team sports or fitness classes can improve mood, decrease stress, and strengthen interpersonal connections [31]. In this context, individuals experiencing anxiety-related motivational deficits may be more likely to overcome initial inertia and engage in exercise when social norms emphasize collective participation [32].
In individualistic societies, although team-based activities can still yield positive emotional effects, prevailing cultural norms that prioritize personal autonomy may attenuate the emotional benefits from group-based activities [33]. In this vein, the social and emotional benefits of group-based exercise may be comparatively weaker in such contexts [34]. In addition, in more individualistic cultures, exercise goals are often internalized as abstract ideals of self-improvement, which may be weakened by potential heightened self-criticism [35]. Given this cultural contrast, we proposed the following hypothesis:
Hypothesis 2: Societal individualism versus collectivism moderates the association between exercise and anxiety symptoms. Specifically, in more collectivist societies, baseline exercise is associated with a greater reduction in subsequent anxiety symptoms.
The description of the methods below has been adapted from VanderWeele, Johnson [9]. Further methodological details are available elsewhere [36,37,38,39,40].
3.1 Data Sources, Population, and Sampling
This study drew on data from the Global Flourishing Study (GFS), a large-scale longitudinal survey that recruited more than 200,000 participants at Wave 1 across over 20 geographically and culturally diverse societies. A complete list of participating societies is provided in Table 1. The sampling strategy emphasized broad global coverage and diversity in geography, culture, and religion, while also considering the feasibility of data collection based on existing infrastructure. All data were collected by Gallup, Inc. Gallup’s Institutional Review Board ensured all informed consent language used in the GFS met the ethical and legal requirements for human subjects research of this nature (https://www.cos.io/gfs-faqs).
Wave 1 data were primarily collected in 2023, with some societies beginning in 2022, and collection dates varied by location [38,39]. Four additional waves are planned annually from 2024 to 2027, with data from Waves 1 and 2 currently available for public access (https://www.cos.io/gfs-wave-data). This study was preregistered on the Open Science Framework (https://osf.io/m7t49). Wave 2 of the GFS was conducted approximately one year after Wave 1. Appendix 1 of the methodology report (https://osf.io/k2s7u) reports the specific data collection periods for each participating society.
When matching the longitudinal data from Wave 1 and Wave 2, respondents who did not participate in both waves were excluded, yielding a retained sample of 128,868 individuals. After additionally removing cases with missing data on exercise at both waves, anxiety symptoms at both waves, gender, and baseline age, the final individual-level sample comprised 123,298 respondents. Societal-level data on individualism–collectivism and the Human Development Index were available for all 23 societies. Accordingly, the final dataset consisted of 123,298 individuals nested within 23 societies for the multilevel modeling analysis.
Anxiety symptoms were measured using the Generalized Anxiety Disorder 2-item (GAD-2) scale from the GFS [9]. The GAD-2 demonstrates good diagnostic accuracy for detecting anxiety disorders across multiple languages and diverse populations, with performance comparable to that of the Generalized Anxiety Disorder 7-item [41]. The measure includes two items: FEEL_ANXIOUS (Been Bothered in Last Two Weeks By: Feeling Nervous, Anxious or on Edge) and CONTROL_WORRY (Been Bothered in Last Two Weeks By: Not Being Able to Stop or Control Worrying). Response options for both items were: 1 = Nearly every day, 2 = More than half the days, 3 = Several days, and 4 = Not at all. Both items were rated on a 4-point scale and were reverse-scored. Mean scores were calculated to represent individuals’ anxiety symptom levels, with higher scores indicating greater anxiety symptoms. The Cronbach’s alpha coefficients for this scale were 0.801 at Wave 1 and 0.791 at Wave 2, indicating good internal consistency [42].
Exercise was assessed using the GFS item DAYS_EXERCISE, which measured the number of days (0–7) a respondent engaged in exercise during the past week. The item asked: “On how many days did you exercise or engage in vigorous physical activities for 30 min or more in the past week?” We transformed the exercise variable into a dichotomous measure (1 = reported exercising at least 1 day; 0 = reported exercising 0 days) to distinguish between physically inactive and active individuals, an approach commonly used in public health research to simplify interpretation and model associations with health outcomes such as anxiety symptoms [43]. This binary classification facilitates clearer inference regarding the presence versus absence of exercise behavior in large cross-societal samples.
Demographic variables were obtained from the GFS. Age was treated as a continuous variable. Gender was coded as a binary variable (0 = female, 1 = male). Since participants who identified with other gender identities constituted a small number of cases (N = 406) and to ensure adequate statistical power for the main analysis, these cases were omitted from the present study.
Individualism versus collectivism was assessed using Hofstede’s cultural dimension theoretical framework [33]. This index is scaled from 0 to 100. Higher scores indicate a greater societal orientation toward Individualism, while lower scores represent a stronger tendency toward Collectivism.
The Human Development Index (HDI) was obtained from the Human Development Report 2023/2024 [44]. We used HDI scores from 2022. The HDI is a composite indicator that summarizes a society’s average achievement across three dimensions including life expectancy, education, and per capita income. HDI scores range from 0 to 1, with higher values signifying greater levels of human development.
Multilevel Modeling (MLM) was employed to examine the association between exercise and anxiety symptoms, and to test the cross-level moderating role of society-level individualism versus collectivism. Data cleaning and validity checks were conducted using Stata 17 MP (StataCorp LLC, College Station, TX, United States). Subsequent descriptive analysis, data visualization, and the multilevel modeling were performed using R (version 4.3.2) with the packages ggplot2 and lme4.
The null model with anxiety symptoms at Wave 2 as dependent variable was estimated to calculate the intraclass correlation coefficient (ICC). The ICC quantifies the proportion of total variance in anxiety symptoms that is attributable to between-society differences. Following Cohen [45], an ICC value exceeding 0.059 was used as the criterion to confirm the appropriateness of Multilevel Modeling.
All individual-level continuous variables were group-mean centered, while all society-level variables were grand-mean centered. Two main models with random slopes and intercepts were then specified. In particular, one model considered only exercise at Wave 1 and the another consider exercise at Wave 1 and 2. We also included individual-level covariates (e.g., age at Wave 1, gender). We controlled for society-level variation in Wave 1 and Wave 2 exercise, Wave 1 anxiety, and Wave 1 age and gender.
Three full models additionally incorporated cross-level interaction terms with individualism–collectivism. The first full model included exercise at Wave 1 and its interaction with individualism–collectivism. The second model included exercise at Wave 2, and the third incorporated exercise at Wave 2 along with its interaction with individualism–collectivism. All three models further adjusted for societal-level covariates, including individualism–collectivism and the HDI. Society-level variations in all individual-level variables were controlled for. When significant cross-level interactions emerged, simple slope analyses were conducted to examine the nature of the moderation [46].
Table 1 presents descriptive statistics grouped by societies. Columns 2 and 3 report the proportion of respondents who exercised in the previous week at Wave 1 and Wave 2, respectively. Columns 4 to 7 display the mean and standard deviation of anxiety symptoms at Wave 1 and Wave 2. Column 8 provides the proportion of males in each society. Columns 9 and 10 show the mean and standard deviation of participants’ age at Wave 1. Columns 11 and 12 present the values of society-level variables, including individualism–collectivism and the HDI. Column 13 reports the sample size for each society.
To ensure that the factor structure derived from the overall sample was appropriately represented within each society, we conducted a Procrustes rotation [47] and calculated Tucker’s phi congruence coefficients [48] to assess factorial agreement across societies. The results showed high congruence. Specifically, the Tucker’s phi values for anxiety symptoms between Wave 1 and Wave 2 were 1.000 in all societies. Tucker’s phi values exceeded the recommended threshold of 0.950, indicating a very good congruence across societies [49].
We estimated the null model using anxiety symptoms at Wave 2 as the dependent variable. The result showed that the intraclass correlation coefficient for the null model was 0.075, exceeding the threshold of 0.059 [45]. This level of between-society variance justified the use of multilevel modeling to examine cross-societal differences in residents’ anxiety symptoms at Wave 2.
Table 2 presents the results of the main models. The coefficient of exercise at Wave 1 on anxiety symptoms at Wave 2 was significant (β = −0.041, p < 0.01). However, after including exercise at Wave 2 in the model, the effect of Wave 1 exercise was no longer significant, whereas exercise at Wave 2 remained a significant negative predictor of anxiety symptoms (β = −0.066, p < 0.001).
The temporal stability of anxiety symptoms was evident, as Wave 1 symptoms consistently and positively predicted Wave 2 symptoms. All individual-level control variables also demonstrated significant associations with anxiety symptoms. For instance, males reported lower levels of anxiety symptoms than females, and age was significantly and positively associated with anxiety symptoms.
Table 2 also reports estimates from the three full models. The interaction between exercise at Wave 1 and individualism–collectivism was significant, indicating a significant moderating effect of individualism–collectivism (β ranged from 0.105 to 0.108, p < 0.05 in the full models). In contrast, the interaction between exercise at Wave 2 and individualism–collectivism did not significantly predict anxiety symptoms at Wave 2 (β = 0.009, p > 0.05 in the full model 3).
To further examine the significant cross-level moderating effect, a simple slope analysis was conducted (Fig. 2). Individualism–collectivism was operationalized using the upper and lower quartiles to represent individualism and collectivism, respectively. Exercise in the previous week was treated as the independent variable, and anxiety symptoms at Wave 2 were used as the dependent variable in the analysis.
The simple slope analysis showed that in more collectivistic societies, the association between individuals’ baseline exercise and follow-up anxiety symptoms was more negative. This indicates that individuals who exercised earlier tended to report lower anxiety symptoms in societies with more collectivism. In contrast, in more individualistic societies, the association between baseline exercise and follow-up anxiety symptoms was weak or negligible, suggesting that residents in individualistic societies exhibited a limited linkage between exercise and anxiety symptoms.
Table 1: Descriptive statistics.
| Societies | Exercise at W1 | Exercise at W2 | Anxiety Symptoms at W1 | Anxiety Symptoms at W2 | Gender | Age at W1 | IND-COL | HDI | N | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | |||||||
| Argentina | 0.552 | 0.607 | 2.129 | 0.966 | 2.063 | 0.982 | 0.494 | 42.8 | 16.3 | 51.0 | 0.849 | 2833 |
| Australia | 0.767 | 0.765 | 1.854 | 0.852 | 1.880 | 0.883 | 0.491 | 50.0 | 17.6 | 73.0 | 0.946 | 2526 |
| Brazil | 0.587 | 0.583 | 2.346 | 1.043 | 2.272 | 1.008 | 0.479 | 42.7 | 16.2 | 36.0 | 0.760 | 4147 |
| Egypt | 0.207 | 0.175 | 2.327 | 0.971 | 2.313 | 0.976 | 0.515 | 36.9 | 14.1 | 13.0 | 0.728 | 2994 |
| Germany | 0.716 | 0.724 | 1.700 | 0.770 | 1.739 | 0.762 | 0.487 | 49.5 | 17.1 | 79.0 | 0.950 | 5403 |
| India | 0.592 | 0.590 | 1.963 | 0.940 | 2.081 | 0.976 | 0.535 | 37.9 | 14.4 | 24.0 | 0.644 | 4661 |
| Indonesia | 0.791 | 0.782 | 1.571 | 0.773 | 1.673 | 0.845 | 0.499 | 38.1 | 13.9 | 5.0 | 0.713 | 2583 |
| Israel | 0.519 | 0.539 | 1.554 | 0.745 | 1.551 | 0.751 | 0.489 | 44.1 | 18.2 | 56.0 | 0.915 | 2342 |
| Japan | 0.552 | 0.544 | 1.646 | 0.792 | 1.686 | 0.809 | 0.472 | 52.1 | 17.0 | 62.0 | 0.920 | 13,385 |
| Kenya | 0.659 | 0.684 | 2.073 | 0.889 | 2.068 | 0.891 | 0.489 | 35.3 | 14.6 | 5.0 | 0.601 | 7588 |
| Mexico | 0.631 | 0.647 | 1.896 | 0.870 | 1.920 | 0.903 | 0.476 | 40.9 | 15.9 | 34.0 | 0.781 | 2182 |
| Nigeria | 0.762 | 0.849 | 2.046 | 0.894 | 2.142 | 0.880 | 0.513 | 34.6 | 13.3 | 0.0 | 0.548 | 2963 |
| Philippines | 0.857 | 0.860 | 2.297 | 0.956 | 2.245 | 0.964 | 0.480 | 38.8 | 15.3 | 17.0 | 0.710 | 2650 |
| Poland | 0.452 | 0.445 | 1.477 | 0.628 | 1.470 | 0.604 | 0.475 | 46.4 | 16.4 | 47.0 | 0.881 | 6091 |
| South Africa | 0.651 | 0.643 | 1.914 | 0.847 | 2.153 | 0.895 | 0.484 | 38.5 | 15.0 | 23.0 | 0.717 | 950 |
| Spain | 0.723 | 0.718 | 2.007 | 0.886 | 2.080 | 0.890 | 0.500 | 46.6 | 15.5 | 67.0 | 0.911 | 2858 |
| Tanzania | 0.746 | 0.756 | 1.851 | 0.944 | 1.865 | 0.933 | 0.488 | 35.8 | 14.8 | 25.0 | 0.532 | 5349 |
| Türkiye | 0.631 | 0.566 | 2.153 | 1.049 | 2.155 | 1.017 | 0.503 | 41.9 | 15.9 | 46.0 | 0.855 | 485 |
| United Kingdom | 0.691 | 0.701 | 1.862 | 0.925 | 1.878 | 0.932 | 0.483 | 49.8 | 17.2 | 76.0 | 0.940 | 3509 |
| United States | 0.744 | 0.719 | 1.752 | 0.852 | 1.753 | 0.846 | 0.477 | 52.1 | 16.4 | 60.0 | 0.927 | 31,369 |
| Sweden | 0.768 | 0.752 | 1.609 | 0.789 | 1.642 | 0.806 | 0.496 | 49.3 | 18.3 | 87.0 | 0.952 | 11,203 |
| Hong Kong SAR | 0.624 | 0.613 | 1.865 | 0.768 | 1.831 | 0.724 | 0.442 | 48.0 | 14.9 | 50.0 | 0.956 | 696 |
| Chinese Mainland | 0.830 | 0.856 | 1.715 | 0.736 | 1.693 | 0.671 | 0.506 | 44.8 | 15.4 | 43.0 | 0.788 | 4531 |
Table 2: Estimations of multilevel models with anxiety symptoms at Wave 2 as the dependent variable.
| Main Model 1 | Main Model 2 | Full Model 1 | Full Model 2 | Full Model 3 | ||
|---|---|---|---|---|---|---|
| Individual-level coefficient | Exercise at W1 | −0.041** | −0.016 | −0.042** | −0.017 | −0.017 |
| (0.013) | (0.012) | (0.014) | (0.012) | (0.012) | ||
| Exercise at W2 | −0.066*** | −0.066*** | −0.070* | |||
| (0.014) | (0.014) | (0.028) | ||||
| Anxiety symptoms at W1 | 0.431*** | 0.430*** | 0.431*** | 0.430*** | 0.430*** | |
| (0.032) | (0.032) | (0.032) | (0.032) | (0.032) | ||
| Gender | −0.070*** | −0.069*** | −0.070*** | −0.069*** | −0.069*** | |
| (0.004) | (0.004) | (0.004) | (0.004) | (0.004) | ||
| Age at W1 | 0.004*** | 0.004*** | 0.004*** | 0.004*** | 0.004*** | |
| (0.0001) | (0.0001) | (0.0001) | (0.0001) | (0.0001) | ||
| Society-level coefficient | IND-COL | 0.035 | 0.065 | 0.065 | ||
| (0.152) | (0.152) | (0.152) | ||||
| HDI | −0.066 | −0.137 | −0.137 | |||
| (0.260) | (0.271) | (0.271) | ||||
| Cross-level interaction item coefficient | Exercise at W1 × IND-COL | 0.108* | 0.106* | 0.105* | ||
| (0.049) | (0.046) | (0.046) | ||||
| Exercise at W2 × IND-COL | 0.009 | |||||
| (0.055) | ||||||
| Akaike’s information criterion | 305,889.9 | 305,676.5 | 305,901.6 | 305,688.2 | 305,694.1 | |
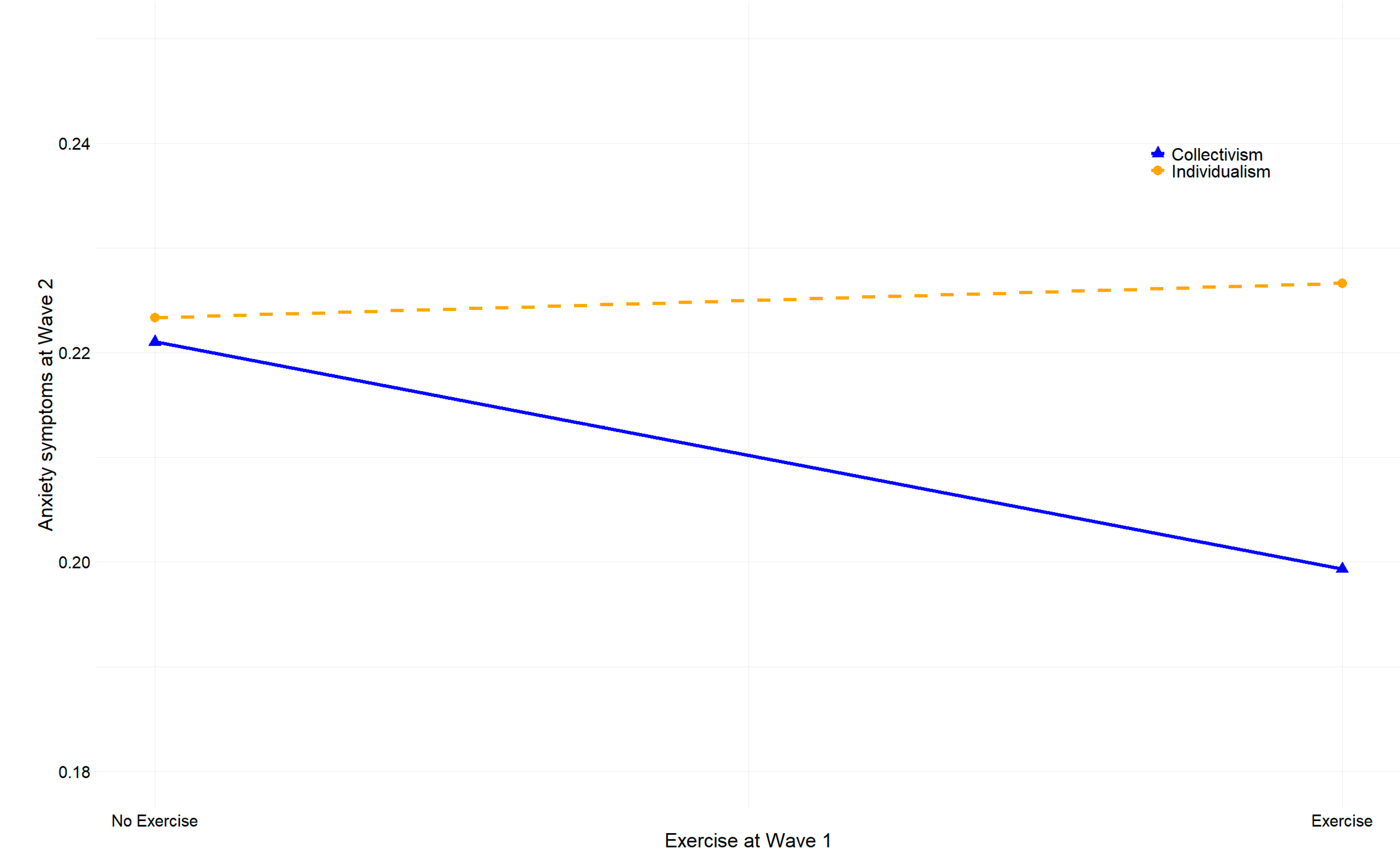
Figure 2: Result of the simple slope test.
The findings reveal a lagged association between exercise and subsequent anxiety symptoms, supporting Hypothesis 1. This result aligns with a substantial body of research showing that regular physical activity is linked to lower anxiety and can help reduce anxiety-related conditions [3,5,15]. Prior studies have demonstrated that exercise alleviates anxiety through physiological pathways such as neurochemical changes [50], as well as through psychosocial mechanisms including enhanced social connectedness and more effective stress coping [31]. By drawing on a longitudinal and cross-societal dataset, the present study extends this literature and shows that the anxiolytic benefits of exercise can be observed across diverse societal contexts.
When exercise at Wave 2 was included in the model, the predictive role of exercise at Wave 1 in subsequent anxiety symptoms attenuated, whereas Wave 2 exercise showed a stronger association with reduced anxiety symptoms. This pattern suggests that the short-term influence of exercise on anxiety may be more pronounced than its longer-term effect [13]. A plausible explanation is that the immediate physiological responses elicited by physical activity, such as increased serotonin release and higher levels of BDNF, generate rapid and effective anxiolytic benefits [22]. These biological mechanisms may contribute more directly to emotional relief than the social benefits of exercise, which tend to accumulate gradually [51].
The observed temporal stability of anxiety symptoms is consistent with prior research [16]. In addition, lower reported anxiety among males may reflect gender differences in emotional expression and socialization, whereby men are less likely to acknowledge or report anxiety symptoms [52]. In contrast, females may experience greater exposure to psychosocial stressors and demonstrate higher emotional sensitivity [53]. The observed positive association between age and anxiety symptoms may be related to increasing functional limitations in later adulthood [54].
The cross-cultural models consistently indicated that the anxiety-reducing effect of earlier exercise was more pronounced in collectivist societies. Hypothesis 2 was supported. Individuals who exercised at baseline reported lower anxiety symptoms at follow-up in these cultural contexts. In contrast, the association between baseline exercise and later anxiety symptoms was negligible in more individualistic societies. Collectivist cultures emphasize shared activities, group cohesion, and mutual support, which may enhance the psychosocial benefits of exercise [14]. By comparison, individualistic cultures prioritize autonomy, which may limit the extent to which the social aspects of exercise translate into emotional relief [34,55].
The moderating role of individualism versus collectivism in the association between Wave 2 exercise and Wave 2 anxiety symptoms was not significant. This suggests that the short-term biological benefits of exercise operate independently of cultural value orientations [13]. The short-term effect appears stronger than the longer-term influence [56]. This is not shaped by cultural individualism or collectivism, which further supports the proposition that proximal effects of exercise are primarily driven by neuroscientific mechanisms [23]. In contrast, longer-term influences are more likely to reflect psychosocial pathways, as social processes are more sensitive to cultural norms [53]. Given this, individual-level independent and interdependent self-construals may also serve as important moderators [57].
This study provides several theoretical contributions to mental health research by deepening the understanding of how exercise relates to anxiety across diverse cultural contexts. Drawing on the GFS, it offers longitudinal evidence that clarifies the associations between exercise and subsequent anxiety symptoms and shows that more immediate exercise behavior has a stronger linkage with emotional outcomes than exercise performed over a longer interval [36]. The findings also enrich cross-cultural literature by identifying a cultural boundary condition in the exercise–anxiety relationship. The stronger association between prior exercise and subsequent anxiety symptoms in collectivist societies demonstrates that cultural orientations shape the psychosocial pathways through which exercise contributes to long-term emotional well-being, indicating that cultural values act as active components rather than background characteristics in mental health processes [15,58].
The findings of this study offer several practical implications for mental health promotion and exercise-based interventions across societies. The strong association between recent exercise and reduced anxiety symptoms suggests that encouraging regular and sustained physical activity may be an effective strategy for improving emotional well-being [3]. Public health agencies and community organizations may consider designing programs that facilitate more frequent participation in exercise, particularly those that generate immediate physiological benefits [13,59].
The cultural variation observed in this study further highlights the importance of tailoring interventions to societal value orientations. In more collectivist contexts, initiatives that promote group-based activities, shared routines, and community engagement may more effectively enhance the longer-term emotional benefits of sustained exercise [26]. In individualistic societies, public health efforts may need to strengthen the psychological conditions under which exercise becomes emotionally beneficial, such as fostering intrinsic motivation within activity programs [34]. These insights underscore the importance of culturally informed strategies in maximizing the mental health benefits of exercise at both individual and societal levels.
There are several limitations. First, the individual-level dataset from the two-wave GFS limits the ability to draw strong causal inferences. Although the longitudinal design improves upon cross-sectional studies, more robust causal analyses will be possible once additional waves of GFS data are collected. Second, the use of self-reported measures may introduce recall bias and social desirability bias. Future research could employ RCTs across multiple societies to reduce measurement bias and more fully account for the social context of exercise, such as differences between group-based and individual exercise [60]. Last, this study did not directly assess neuroscientific and psychosocial mechanisms. Instead, these mechanisms were inferred indirectly based on the significance or non-significance of coefficients across time. Further empirical evidence is required to strengthen and validate these mediation or moderated mediation inferences.
We identified a lagged association between baseline exercise and subsequent reductions in anxiety symptoms across societies. Cross-level analyses further showed that exercise was a stronger negative predictor of subsequent anxiety symptoms in more collectivist societies, whereas this association was negligible in more individualistic contexts.
Acknowledgement:
Funding Statement: The authors received no specific funding.
Author Contributions: The authors confirm contribution to the paper as follows: Conceptualization, Albert Jiansong Zheng and Junxian Shen; methodology, Albert Jiansong Zheng; software, Albert Jiansong Zheng; validation, Albert Jiansong Zheng and Junxian Shen; formal analysis, Albert Jiansong Zheng; investigation, Albert Jiansong Zheng; resources, Albert Jiansong Zheng and Junxian Shen; data curation, Albert Jiansong Zheng; writing—original draft preparation, Albert Jiansong Zheng; writing—review and editing, Albert Jiansong Zheng and Junxian Shen; visualization, Albert Jiansong Zheng; supervision, Junxian Shen; project administration, Albert Jiansong Zheng. All authors reviewed and approved the final version of the manuscript.
Availability of Data and Materials: The data that support the findings of this study are available in the Open Science Framework repository upon submission of pre-registration https://www.cos.io/gfs-access-data (accessed on 10 December 2025).
Ethics Approval: Not applicable. This study is based on secondary analysis of publicly available data. The dataset was collected and managed by the survey organizers in accordance with relevant ethical standards. As the research uses anonymized secondary data and does not involve direct interaction with human subjects, no additional ethical approval was required.
Conflicts of Interest: The authors declare no conflicts of interest.
Abbreviations
| BDNF | Brain-derived neurotrophic factor |
| CI | Confidence interval |
| GFS | Global Flourishing Study |
| GAD-2 | Generalized Anxiety Disorder 2-item |
| MLM | Multilevel Modeling |
| ICC | Intraclass correlation coefficient |
| HDI | Human Development Index |
| RCTs | Randomized controlled trials |
| SAR | Special Administrative Region |
| SD | Standard deviation |
| IND-COL | Individualism versus collectivism |
| W1 | Wave 1 |
| W2 | Wave 2 |
References
1. Ramos-Sanchez CP , Schuch FB , Seedat S , Louw QA , Stubbs B , Rosenbaum S , et al. The anxiolytic effects of exercise for people with anxiety and related disorders: An update of the available meta-analytic evidence. Psychiatry Res. 2021; 302: 114046. doi:10.1016/j.psychres.2021.114046. [Google Scholar] [CrossRef]
2. Jayakody K , Gunadasa S , Hosker C . Exercise for anxiety disorders: Systematic review. Br J Sports Med. 2014; 48( 3): 187– 96. doi:10.1136/bjsports-2012-091287. [Google Scholar] [CrossRef]
3. Budde H , Dolz N , Mueller-Alcazar A , Schacht F , Velasques B , Ribeiro P , et al. A 10 years update of effects of exercise on depression disorders-in otherwise healthy adults: A systematic review of meta-analyses and neurobiological mechanisms. PLoS One. 2025; 20( 5): e0317610. doi:10.1371/journal.pone.0317610. [Google Scholar] [CrossRef]
4. Li J , Wilczyńska DM , Lipowska M , Łada-Maśko AB , Radtke BM , Sajewicz-Radtke U , et al. Beyond borders: Investigating the impact of COVID-19 anxiety and eating attitudes on psychological well-being and physical activity objectives in Poland and China. Nutrients. 2024; 17( 1): 41. doi:10.3390/nu17010041. [Google Scholar] [CrossRef]
5. Lin Y , Gao W . The effects of physical exercise on anxiety symptoms of college students: A meta-analysis. Front Psychol. 2023; 14: 1136900. doi:10.3389/fpsyg.2023.1136900. [Google Scholar] [CrossRef]
6. Herring MP , Rasmussen CL , McDowell CP , Gordon BR , Kenny RA , Laird E . Physical activity dose for generalized anxiety disorder & worry: Results from the Irish longitudinal study on ageing. Psychiatry Res. 2024; 332: 115723. doi:10.1016/j.psychres.2024.115723. [Google Scholar] [CrossRef]
7. Severin R , Arena R . A culture of health promotion in healthcare: can’t pour from an empty cup. Prog Cardiovasc Dis. 2025; 90: 45– 50. doi:10.1016/j.pcad.2025.02.007. [Google Scholar] [CrossRef]
8. Ewuzie Z , Ezeano C , Aderinto N . A review of exercise interventions for reducing anxiety symptoms: Insights and implications. Medicine. 2024; 103( 41): e40084. doi:10.1097/MD.0000000000040084. [Google Scholar] [CrossRef]
9. VanderWeele TJ , Johnson BR , Bialowolski PT , Bonhag R , Bradshaw M , Breedlove T , et al. The global flourishing study: Study profile and initial results on flourishing. Nat Ment Health. 2025; 3( 6): 636– 53. doi:10.1038/s44220-025-00423-5. [Google Scholar] [CrossRef]
10. Cerin E , Leslie E , Sugiyama T , Owen N . Associations of multiple physical activity domains with mental well-being. Ment Health Phys Act. 2009; 2( 2): 55– 64. doi:10.1016/j.mhpa.2009.09.004. [Google Scholar] [CrossRef]
11. Lopes MVV , Matias TS , da Costa BGG , Schuch FB , Chaput JP , Samara Silva K . The relationship between physical activity and depressive symptoms is domain-specific, age-dependent, and non-linear: An analysis of the Brazilian national health survey. J Psychiatr Res. 2023; 159: 205– 12. doi:10.1016/j.jpsychires.2023.01.041. [Google Scholar] [CrossRef]
12. Liu C , Liang X , Sit CHP . Physical activity and mental health in children and adolescents with neurodevelopmental disorders: A systematic review and meta-analysis. JAMA Pediatr. 2024; 178( 3): 247– 57. doi:10.1001/jamapediatrics.2023.6251. [Google Scholar] [CrossRef]
13. Herring MP , Jacob ML , Suveg C , O’Connor PJ . Effects of short-term exercise training on signs and symptoms of generalized anxiety disorder. Ment Health Phys Act. 2011; 4( 2): 71– 7. doi:10.1016/j.mhpa.2011.07.002. [Google Scholar] [CrossRef]
14. Golaszewski NM , LaCroix AZ , Hooker SP , Bartholomew JB . Group exercise membership is associated with forms of social support, exercise identity, and amount of physical activity. Int J Sport Exerc Psychol. 2022; 20( 2): 630– 43. doi:10.1080/1612197x.2021.1891121. [Google Scholar] [CrossRef]
15. Huo M , Yang Z . Exercise, depression, and anxiety in young people: A cross-sectional survey. Int J Ment Health Promot. 2023; 25( 4): 551– 62. doi:10.32604/ijmhp.2023.023406. [Google Scholar] [CrossRef]
16. Schlechter P , Hellmann JH , Morina N . The longitudinal relationship between well-being comparisons and anxiety symptoms in the context of uncontrollability of worries and external locus of control: A two-wave study. Anxiety Stress Coping. 2024; 37( 5): 602– 14. doi:10.1080/10615806.2024.2306530. [Google Scholar] [CrossRef]
17. Zheng H , Kyung Kim H , Joanna Sin SC , Theng YL . Exploring developmental trajectory of cyberchondria over time: A three-wave panel study. Telematics Inform. 2022; 75: 101892. doi:10.1016/j.tele.2022.101892. [Google Scholar] [CrossRef]
18. Barry MM . Addressing the determinants of positive mental health: Concepts, evidence and practice. Int J Ment Health Promot. 2009; 11( 3): 4– 17. doi:10.1080/14623730.2009.9721788. [Google Scholar] [CrossRef]
19. Wan H , Huang W , Zhang W , Hu C . Exploring adolescents’ social anxiety, physical activity, and core self-evaluation: A latent profile and mediation approach. Int J Ment Health Promot. 2025; 27( 10): 1611– 26. doi:10.32604/ijmhp.2025.070457. [Google Scholar] [CrossRef]
20. Zheng J , Zhang T , Wang X . Estimating mechanisms linking relative income to self-rated health by multilevel modeling: The moderating role of healthcare access and quality index. BMC Public Health. 2025; 25( 1): 1735. doi:10.1186/s12889-025-22783-4. [Google Scholar] [CrossRef]
21. Morgan JA , Corrigan F , Baune BT . Effects of physical exercise on central nervous system functions: A review of brain region specific adaptations. J Mol Psychiatry. 2015; 3( 1): 3. doi:10.1186/s40303-015-0010-8. [Google Scholar] [CrossRef]
22. Ferrer-Uris B , Ramos MA , Busquets A , Angulo-Barroso R . Can exercise shape your brain? A review of aerobic exercise effects on cognitive function and neuro-physiological underpinning mechanisms. AIMS Neurosci. 2022; 9( 2): 150– 74. doi:10.3934/Neuroscience.2022009. [Google Scholar] [CrossRef]
23. Lucibello KM , Parker J , Heisz JJ . Examining a training effect on the state anxiety response to an acute bout of exercise in low and high anxious individuals. J Affect Disord. 2019; 247: 29– 35. doi:10.1016/j.jad.2018.12.063. [Google Scholar] [CrossRef]
24. Stonerock GL , Hoffman BM , Smith PJ , Blumenthal JA . Exercise as treatment for anxiety: Systematic review and analysis. Ann Behav Med. 2015; 49( 4): 542– 56. doi:10.1007/s12160-014-9685-9. [Google Scholar] [CrossRef]
25. Herring MP , Meyer JD . Resistance exercise for anxiety and depression: Efficacy and plausible mechanisms. Trends Mol Med. 2024; 30( 3): 204– 6. doi:10.1016/j.molmed.2023.11.016. [Google Scholar] [CrossRef]
26. Gil-Beltrán E , Coo C , Meneghel I , Llorens S , Salanova M . How physical exercise with others and prioritizing positivity contribute to (work) wellbeing: A cross-sectional and diary multilevel study. Front Sports Act Living. 2024; 6: 1437974. doi:10.3389/fspor.2024.1437974. [Google Scholar] [CrossRef]
27. Wang L , Faridniya H , Yu H . A public health perspective on virtual reality interventions: Exploring the impact of VR extreme sports on stress, anxiety, and depression in men with social anxiety disorder. Front Public Health. 2025; 13: 1617483. doi:10.3389/fpubh.2025.1617483. [Google Scholar] [CrossRef]
28. Zheng J , Zhang T . The effects of the Internet on well-being among older adults ageing in place: the roles of subjective income and social trust. China Perspect. 2023; 134: 43– 56. doi:10.4000/chinaperspectives.15773. [Google Scholar] [CrossRef]
29. Zheng J , Zhang T . Patterns of trust and subjective well-being across societies: The role of long-term versus short-term orientation. BMC Psychol. 2025; 13( 1): 697. doi:10.1186/s40359-025-03048-6. [Google Scholar] [CrossRef]
30. Gu M , Wang Y , Shi Y , Yu J , Xu J , Jia Y , et al. Impact of a group-based intervention program on physical activity and health-related outcomes in worksite settings. BMC Public Health. 2020; 20( 1): 935. doi:10.1186/s12889-020-09036-2. [Google Scholar] [CrossRef]
31. Di Bartolomeo G , Papa S . The effects of physical activity on social interactions: The case of trust and trustworthiness. J Phys Econ. 2019; 20( 1): 50– 71. doi:10.1177/1527002517717299. [Google Scholar] [CrossRef]
32. Su Z , Zhang Z , Zhou Y . Impact of exercise atmosphere on adolescents’ exercise behavior: Chain mediating effect of exercise identity and exercise habit. Int J Ment Health Promot. 2024; 26( 7): 579– 88. doi:10.32604/ijmhp.2024.051842. [Google Scholar] [CrossRef]
33. Hofstede G . Culture’s consequences: comparing values, behaviors, institutions, and organizations across nations. 2nd ed. London, UK: SAGE; 2001. [Google Scholar]
34. Rice JM , Gordon BR , Lindheimer JB , Lyons M , Herring MP . Associations between expected and observed psychological responses to acute resistance exercise in analogue generalized anxiety disorder. Sci Rep. 2025; 15( 1): 11378. doi:10.1038/s41598-025-96156-7. [Google Scholar] [CrossRef]
35. Wang H , Lou X . The correlation between self-compassion and life satisfaction varies across societal individualism-collectivism: A three-level meta-analysis. J Cross Cult Psychol. 2022; 53( 9): 1097– 116. doi:10.1177/00220221221109547. [Google Scholar] [CrossRef]
36. Lomas T , Bradshaw M , Case B , Cowden RG , Crabtree S , English C , et al. The development of the Global Flourishing Study questionnaire: Charting the evolution of a new 109-item inventory of human flourishing. BMC Glob Public Health. 2025; 3( 1): 30. doi:10.1186/s44263-025-00139-9. [Google Scholar] [CrossRef]
37. Crabtree S , English C , Johnson BR , Ritter Z , VanderWeele TJ . Global flourishing study: Questionnaire development report. Washington, DC, USA: Gallup Inc.; 2021. [Google Scholar]
38. Padgett RN , Cowden RG , Chattopadhyay M , Han Y , Honohan J , Ritter Z , et al. Survey sampling design in wave 1 of the Global Flourishing Study. Eur J Epidemiol. 2025; 40( 4): 391– 406. doi:10.1007/s10654-024-01167-9. [Google Scholar] [CrossRef]
39. Ritter Z , Srinivasan R , Han Y , Chattopadhyay M , Honohan J , Johnson B , et al. Global Flourishing Study Methodology. Washington, DC, USA: Gallup Inc.; 2024. [Google Scholar]
40. Johnson KA , Moon JW , VanderWeele TJ , Schnitker S , Johnson BR . Assessing religion and spirituality in a cross-cultural sample: Development of religion and spirituality items for the Global Flourishing Study. Religion Brain Behav. 2024; 14( 4): 345– 58. doi:10.1080/2153599X.2023.2217245. [Google Scholar] [CrossRef]
41. Aktürk Z , Hapfelmeier A , Fomenko A , Dümmler D , Eck S , Olm M , et al. Generalized Anxiety Disorder 7-item (GAD-7) and 2-item (GAD-2) scales for detecting anxiety disorders in adults. Cochrane Database Syst Rev. 2025; 3( 3): CD015455. doi:10.1002/14651858.CD015455. [Google Scholar] [CrossRef]
42. Taber KS . The use of cronbach’s alpha when developing and reporting research instruments in science education. Res Sci Educ. 2018; 48( 6): 1273– 96. doi:10.1007/s11165-016-9602-2. [Google Scholar] [CrossRef]
43. Cristi-Montero C . An integrative methodology for classifying physical activity level in apparently healthy populations for use in public health. Rev Panam Salud Publica. 2017; 41: e161. doi:10.26633/RPSP.2017.161. [Google Scholar] [CrossRef]
44. United Nations Development Programme . Human development report 2023-24 [Internet]. 2024 [cited 2026 Jan 1]. Available from: https://hdr.undp.org/content/human-development-report-2023-24. [Google Scholar]
45. Cohen J . Statistical power analysis for the behavioral sciences. Erlbaum, NJ, USA: Lawrence Erlbaum Associates; 1988. [Google Scholar]
46. Preacher KJ , Curran PJ , Bauer DJ . Computational tools for probing interactions in multiple linear regression, multilevel modeling, and latent curve analysis. J Educ Behav Stat. 2006; 31( 4): 437– 48. doi:10.3102/10769986031004437. [Google Scholar] [CrossRef]
47. van de Vijver FJR , Leung K . Methods and data analysis for cross-cultural research. Thousand Oaks, CA, USA: Sage Publications; 1997. [Google Scholar]
48. Tucker LR . A method for synthesis of factor analysis studies. Princeton, NJ, USA: Educational Testing Service; 1951. doi:10.21236/AD0047524. [Google Scholar] [CrossRef]
49. Lorenzo-Seva U , ten Berge JMF . Tucker’s congruence coefficient as a meaningful index of factor similarity. Methodology. 2006; 2( 2): 57– 64. doi:10.1027/1614-2241.2.2.57. [Google Scholar] [CrossRef]
50. Basso JC , Suzuki WA . The effects of acute exercise on mood, cognition, neurophysiology, and neurochemical pathways: A review. Brain Plast. 2017; 2( 2): 127– 52. doi:10.3233/BPL-160040. [Google Scholar] [CrossRef]
51. Cheng T , Douglas Affonso F , Yu J , Zhong Y , Ma Z , Hussain A , et al. Rapid antidepressant effect of single-bout exercise is mediated by adiponectin-induced APPL1 nucleus translocation in anterior cingulate cortex. Mol Psychiatry. 2025; 30( 12): 5760– 76. doi:10.1038/s41380-025-03317-1. [Google Scholar] [CrossRef]
52. Farhane-Medina NZ , Luque B , Tabernero C , Castillo-Mayén R . Factors associated with gender and sex differences in anxiety prevalence and comorbidity: A systematic review. Sci Prog. 2022; 105( 4): 00368504221135469. doi:10.1177/00368504221135469. [Google Scholar] [CrossRef]
53. Wang Q , Zhang J , Xiao M . Association between social media use, physical activity level, and depression and anxiety among college students: A cross-cultural comparative study. Sci Rep. 2025; 15( 1): 6596. doi:10.1038/s41598-025-88140-y. [Google Scholar] [CrossRef]
54. van Steen M , Zoet M , Hendriks GJ , Rhebergen D , Lugtenburg A , Lammers M , et al. Association between personality traits and functional limitations in older adults with affective disorders: A cross sectional study. Clin Gerontol. 2025; 48( 1): 149– 60. doi:10.1080/07317115.2023.2240317. [Google Scholar] [CrossRef]
55. Shen J , Zheng AJ . Future optimism and subjective well-being across societies: Reciprocal links and the role of cultural flexibility–monumentalism. Cross Cult Res. 2026: 10693971261421331. doi:10.1177/10693971261421331. [Google Scholar] [CrossRef]
56. Herring MP , O’Connor PJ , Dishman RK . The effect of exercise training on anxiety symptoms among patients: A systematic review. Arch Intern Med. 2010; 170( 4): 321– 31. doi:10.1001/archinternmed.2009.530. [Google Scholar] [CrossRef]
57. Tan TX , Liu Y , Li G , Yi Z . Independent and interdependent self-construal and anxiety in Chinese college students: A path analysis. J Coll Character. 2022; 23( 2): 127– 43. doi:10.1080/2194587X.2022.2053291. [Google Scholar] [CrossRef]
58. Zheng J , Shen J . Social comparisons for well-being: The role of power distance. Soc Indic Res. 2025; 178( 2): 905– 28. doi:10.1007/s11205-025-03531-y. [Google Scholar] [CrossRef]
59. Zheng J , Wang X , Xie S , Wang H , Shen J , Zhang T . The mediating role of trust in government in intergenerational transmission of fertility intentions. Front Public Health. 2024; 12: 1338122. doi:10.3389/fpubh.2024.1338122. [Google Scholar] [CrossRef]
60. Le Berre M , Forest L , Dumoulin C . Implementation of group-based exercise programs in physiotherapy: A rapid scoping review. Am J Phys Med Rehabil. 2024; 103( 8): 761– 8. doi:10.1097/PHM.0000000000002477. [Google Scholar] [CrossRef]
Cite This Article
 Copyright © 2026 The Author(s). Published by Tech Science Press.
Copyright © 2026 The Author(s). Published by Tech Science Press.This work is licensed under a Creative Commons Attribution 4.0 International License , which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
 Downloads
Downloads
 Citation Tools
Citation Tools