
 Submit a Paper
Submit a Paper Propose a Special lssue
Propose a Special lssue Open Access
Open Access
ARTICLE
Congenital Coronary Artery Fistula in Children: A Review of 28 Cases with Clinical and Imaging Outcomes
1 Division of Pediatric Cardiology, Department of Pediatrics, Faculty of Medicine, Siriraj Hospital, Mahidol University, Bangkok, Thailand
2 Department of Surgery, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand
* Corresponding Author: Chodchanok Vijarnsorn. Email:
Congenital Heart Disease 2022, 17(4), 463-478. https://doi.org/10.32604/chd.2022.021545
Received 20 February 2022; Accepted 05 June 2022; Issue published 04 July 2022
 View Full Text
View Full Text Download PDF
Download PDFAbstract
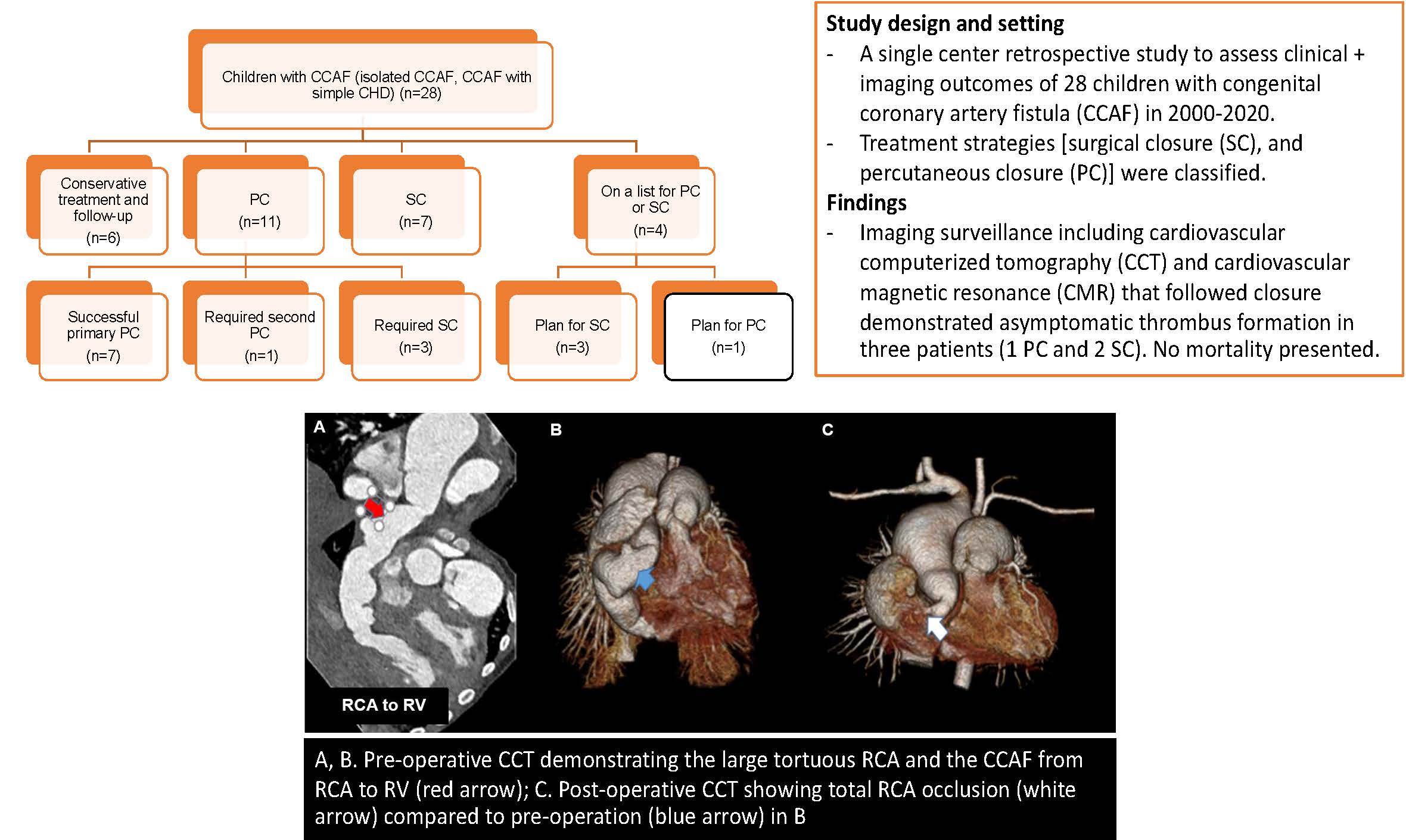
Background: Congenital coronary artery fistula (CCAF) is a rare anomaly. Treatment strategies tend to close the defect with a symptomatic and significant shunt, primarily based on expert consensus and case series. Results for long-term follow-up in children are limited Methods: We conducted a retrospective study to assess clinical and imaging outcomes of children with CCAF at Siriraj Hospital, Thailand during 2000–2020. Patients with single ventricle were excluded. Treatment strategies [surgical closure (SC), and percutaneous closure (PC)] were classified and the clinical outcomes at the follow-up in 2021, including coronary thrombosis, myocardial ischemia, and the results of cardiovascular imaging were reviewed. Results: Twenty-eight children with CCAF were included in the study. The median age at diagnosis was 2.5 years (2 days–18 years). Presenting symptoms were audible murmur (82%) and heart failure (35%). Most of fistulae arose from the right coronary artery (12/28) and exited at the right atrium (11/28). In recent visits (0.5–14 years follow-up), six patients with asymptomatic small CCAF were managed by watchful follow-up without complications. PC was primarily treated in 11 children: 7 underwent successful procedures; 1 had a residual shunt and required re-intervention; 1 had ischemic symptoms immediately after the procedure with left coronary occlusion that required device removal plus SC and 2 were technically unable to place the device, requiring SC. Four patients were waiting for interventions (1 PC and 3 SC). Cardiovascular imaging surveillance that followed closure demonstrated asymptomatic thrombus formation in three patients (1 PC and 2 SC). No mortality presented. Conclusion: CCAF with significant shunt is indicated to close either SC or PC. Ischemic events are rare but have been reported after closure. In addition, thrombus formation should be watched for post-intervention. Surveillance with cardiovascular imaging is recommended after defect closure (ideally 1–5 years post closure), or at interval follow-ups in patients with symptoms to evaluate possible recanalization, thrombus, or ischemia. Life-long clinical and echocardiographic follow-up is warranted. Watchful follow-up is acceptable for hemodynamically insignificant fistula without complication in the series.Graphic Abstract
Keywords
Congenital coronary artery fistula; pediatrics; surgical closure; transcatheter closure; thrombosis
Cite This Article
APA Style
Plearntummakun, P., Vijarnsorn, C., Durongpisitkul, K., Chanthong, P., Chungsomprasong, P. et al. (2022). Congenital Coronary Artery Fistula in Children: A Review of 28 Cases with Clinical and Imaging Outcomes. Congenital Heart Disease, 17(4), 463–478. https://doi.org/10.32604/chd.2022.021545
Vancouver Style
Plearntummakun P, Vijarnsorn C, Durongpisitkul K, Chanthong P, Chungsomprasong P, Kanjanauthai S, et al. Congenital Coronary Artery Fistula in Children: A Review of 28 Cases with Clinical and Imaging Outcomes. Congeni Heart Dis. 2022;17(4):463–478. https://doi.org/10.32604/chd.2022.021545
IEEE Style
P. Plearntummakun et al., “Congenital Coronary Artery Fistula in Children: A Review of 28 Cases with Clinical and Imaging Outcomes,” Congeni. Heart Dis., vol. 17, no. 4, pp. 463–478, 2022. https://doi.org/10.32604/chd.2022.021545
 Copyright © 2022 The Author(s). Published by Tech Science Press.
Copyright © 2022 The Author(s). Published by Tech Science Press.This work is licensed under a Creative Commons Attribution 4.0 International License , which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
 Downloads
Downloads
 Citation Tools
Citation Tools