
 Submit a Paper
Submit a Paper Propose a Special lssue
Propose a Special lssue Open Access
Open Access
ARTICLE

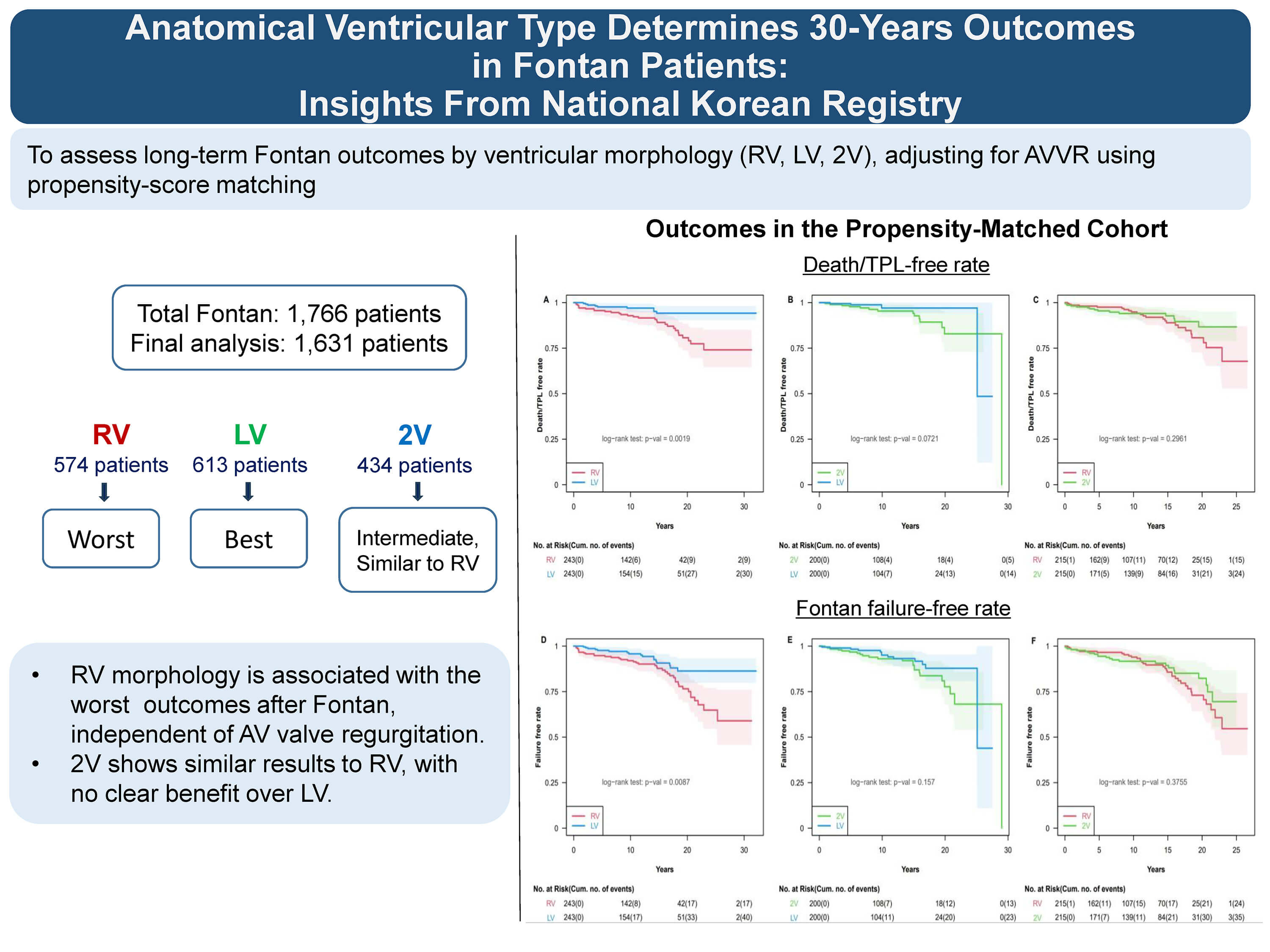
Anatomical Ventricular Type Determines 30-Year Outcomes in Fontan Patients: Insights from National Korean Registry
1 Department of Pediatrics, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Republic of Korea
2 Department of Pediatrics, Sejong General Hospital, Bucheon, Republic of Korea
3 Department of Pediatrics, College of Medicine, Seoul National University Children’s Hospital, Seoul, Republic of Korea
4 Department of Thoracic and Cardiovascular Surgery, Sejong General Hospital, Bucheon, Republic of Korea
5 Department of Thoracic and Cardiovascular Surgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Republic of Korea
6 Department of Pediatrics, Pusan National University Children’s Hospital, Pusan National University School of Medicine, Yangsan, Republic of Korea
7 Department of Pediatrics, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Republic of Korea
8 Department of Pediatrics, Seoul St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Republic of Korea
9 Department of Pediatrics, College of Medicine, Seoul National University Bundang Hospital, Sungnam, Republic of Korea
10 Department of Pediatric Cardiology, Gachon University Gil Medical Center, Incheon, Republic of Korea
11 Department of Pediatrics, Severance Cardiovascular Hospital, Yonsei University College of Medicine, Seoul, Republic of Korea
12 Department of Pediatrics, Kyungbook National University School of Medicine, Daegu, Republic of Korea
13 Department of Pediatrics, Dong-A University Hospital, Pusan, Republic of Korea
14 Department of Statistics and Actuarial Science, Soongsil University, Seoul, Republic of Korea
* Corresponding Author: Soo-Jin Kim. Email:
(This article belongs to the Special Issue: Registries in Congenital Heart Disease)
Structural and Congenital Heart Disease 2026, 21(2), 2 https://doi.org/10.32604/schd.2026.077034
Received 01 December 2025; Accepted 08 June 2026; Issue published 11 June 2026
 View Full Text
View Full Text Download PDF
Download PDFAbstract
Background: Systemic right ventricular morphology is associated with poor Fontan outcomes, but its independent effect remains uncertain due to confounding by atrioventricular valve regurgitation (AVVR). The prognostic role of two adequately sized ventricles is also unclear. This study aimed to evaluate the independent impact of ventricular morphology on long-term Fontan outcomes after adjustment for AVVR, using a large national registry. Methods: A total of 1631 Fontan survivors were analyzed. Death or heart transplantation and Fontan failure were primarily evaluated using inverse probability of treatment weighting. Fontan failure was defined as death, heart transplantation, Fontan takedown or conversion, protein-losing enteropathy, plastic bronchitis, or New York Heart Association class III/IV. Results: The cohort included 35.8% systemic right ventricular morphology, 38.6% systemic left ventricular morphology, and 25.6% two adequately sized ventricular morphology. Systemic right ventricular morphology was associated with a higher risk of death or heart transplantation compared with systemic left ventricular morphology (HR, 1.699; 95% CI, 1.130–2.554; p = 0.011). A similar pattern was observed for Fontan failure (HR, 1.487; 95% CI, 1.084–2.038; p = 0.014). In comparison, two adequately sized ventricular morphology did not demonstrate a clear advantage over systemic left ventricular morphology for death or heart transplantation (HR, 1.582; 95% CI, 0.977–2.563; p = 0.062) or Fontan failure (HR, 1.207; 95% CI, 0.815–1.788; p = 0.347), and showed no significant difference compared with systemic right ventricular morphology. Conclusion: Systemic right ventricle morphology was associated with the poorest long-term outcomes after adjustment for AVVR. Despite having two adequately sized ventricles, this morphology group showed no advantage over systemic left ventricular morphology and did not differ significantly from systemic right ventricular morphology.Graphic Abstract
Keywords
The Fontan operation, commonly performed in patients with functional single ventricle physiology, redirects systemic venous blood to the pulmonary arteries, bypassing the subpulmonary ventricle. Although these patients are often described as having single-ventricle physiology, most possess two anatomical ventricles, with one ventricle frequently being hypoplastic or incomplete and therefore unable to support the systemic circulation.
Over recent decades, the long-term outcomes have markedly improved due to advances in surgical techniques, perioperative care, and patient-specific management. As more patients survive into adulthood, understanding factors that influence long-term outcomes has become increasingly important.
Among several clinical and anatomical factors [1], ventricular morphology has emerged as a potential prognostic factor. Prior studies have suggested that systemic left ventricular morphology may be associated with more favorable outcomes compared to systemic right ventricular morphology [2,3,4,5]. However, the independent impact of ventricular morphology remains uncertain, in part due to its close association with other contributing factors, particularly atrioventricular valve regurgitation (AVVR).
AVVR is a common complication in Fontan patients, particularly in those with a common atrioventricular valve or systemic right ventricle. It has been identified as a major contributor to adverse long-term outcomes [4,6,7]. The incidence of atrioventricular valve failure in Fontan palliation showed marked disparity by valve morphology from 8% with a single mitral valve to 56% with a common atrioventricular valve [6]. As such, AVVR may serve as a confounding factor when evaluating the role of ventricular morphology.
Nonetheless, atrioventricular valve dysfunction alone may not fully explain the variations in long-term outcomes after the Fontan procedure. Understanding whether adverse outcomes are primarily caused by the ventricle’s intrinsic properties or by external factors such as atrioventricular valve dysfunction is crucial for optimizing patient management.
In addition, the prognostic significance of having two adequately sized ventricles also remains uncertain. Although the presence of two adequately sized ventricles may imply preserved ventricular mass or balanced loading conditions, recent evidence suggests that it does not necessarily offer a long-term survival benefit in Fontan patients, challenging the presumed advantage of two-ventricle anatomy [8].
Accordingly, this study aimed to compare long-term outcomes after the Fontan operation based on systemic ventricular morphology-systemic right ventricular morphology, systemic left ventricular morphology, and two adequately sized ventricles while adjusting for the potential confounding effect of AVVR.
The Korean Fontan Registry was established in 2022 and has collected data on demographic characteristics, cardiac anatomical variations, peri-Fontan operative data, current clinical status, functional outcomes, and complications of Fontan circulation for 1765 individuals from 10 pediatric cardiovascular centers across South Korea [9]. The registry includes patients who underwent the Fontan procedure between 1979 and 2019.
2.2 Patient Selection and Data Collection
Among 1765 patients who underwent the Fontan procedure in the Korean Fontan Registry, a total of 1631 patients were included in this study after excluding 71 patients with early mortality, 35 patients with insufficient clinical data, and 28 patients with undetermined ventricular morphology. Early mortality was defined as death occurring within the first 30 postoperative days or without discharge after Fontan surgery.
The study participants were stratified according to their ventricular morphology into three groups: systemic right ventricular morphology (n = 584), systemic left ventricular morphology (n = 630), and patients with two adequately sized ventricles morphology (2V group, n = 417). The 2V group consisted of patients with two ventricles of near-comparable size without significant hypoplasia, in whom both ventricles were preserved and expected to contribute to systemic circulation after Fontan completion, despite not being suitable for true biventricular repair. Classification was based on primary cardiac diagnosis and a ventricular morphology variable recorded in the Korean Fontan Registry database, with the variable reflecting institutional echocardiographic and surgical assessment.
Data on demographic characteristics, cardiac anatomical variations, peri-Fontan operative details, current clinical status, and complications of Fontan circulation were collected from the Korean Fontan Registry database.
Survival outcomes included death or heart transplantation and Fontan failure. Late Fontan failure was defined as late mortality, heart transplantation, late takedown, protein-losing enteropathy, plastic bronchitis, or New York Heart Association Functional Class III or IV at follow-up or Fontan conversion.
Baseline patient characteristics were summarized as means with standard deviations or medians with interquartile range for continuous variables and frequencies with percentages for categorical variables. Missing baseline covariate data were handled using multiple imputation by chained equations to minimize loss of statistical power and potential selection bias associated with complete-case analysis. For each landmark- and outcome-specific analytic dataset, 20 imputed datasets were generated with 10 iterations.
To adjust for baseline confounding among the three ventricular morphology groups (systemic right ventricle, systemic left ventricle, 2V), inverse probability of treatment weighting (IPTW) was applied.
The primary propensity score model included the following covariates: performance of systemic-to-pulmonary shunt operation at stage I, performance of pulmonary artery banding operation at stage I, mean pulmonary artery pressure on pre-Fontan catheterization, grade of atrioventricular valve regurgitation at the time of Fontan operation, age at Fontan operation, type of Fontan surgery, Fontan era. Because the registry spans more than four decades, Fontan era was categorized into two periods (<2000 and ≥2000) to account for potential temporal changes in surgical techniques and perioperative management. Atrioventricular valve morphology was not included in the model due to its strong structural dependence on ventricular morphology, which precluded independent adjustment.
Weights were stabilized and trimmed at the 99th percentile to reduce the influence of extreme weights. Covariate balance across the three groups was assessed using maximum pairwise absolute standardized mean difference (SMD), with SMD < 0.10 considered acceptable balance.
Because early post-Fontan attrition may vary over time, landmark analyses were performed at prespecified time points of 0, 3, 6, and 12 months. For each landmark, patients who remained event-free beyond the landmark were included, and follow-up time was redefined from that landmark forward. Survival curves were presented up to 20 years to improve reliability estimates associated with small numbers at risk. Weighted Cox proportional hazards models were used to estimate hazard ratios (HRs) and 95% confidence intervals (CIs) for long-term mortality and Fontan failure. For analyses based on multiply imputed datasets, estimates were combined across imputations on the log-hazard scale using Rubin’s rules.
A prespecified sensitivity analysis was performed using a multiple imputation–based multivariable Cox model adjusted for the same seven core covariates as the primary model.
All statistical analyses were performed using R software (R Foundation for Statistical Computing, Vienna, Austria), primarily with the mice, WeightIt, cobalt, survey, and survival packages. All tests were two-sided, and p < 0.05 was considered statistically significant.
This study was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the Sejong General Hospital Institutional Review Board (Approval No. 2022-12-007), and the requirement for informed consent was waived due to the retrospective nature of the study design.
Table 1 displays the baseline characteristics of the study cohort before weighting. The cohort included 1631 patients who underwent the Fontan procedure, with a mean age at surgery of 4.3 ± 4.2 years and an average follow-up period of 12.6 ± 8.4 years. The types of Fontan operations performed were atriopulmonary in 127 patients (7.8%), lateral tunnel in 276 patients (17.0%), and extracardiac conduit in 1219 patients (75.2%). According to ventricular morphology, patients were classified into the systemic right ventricle (n = 584), systemic left ventricle (n = 630), and 2V (n = 417) groups. The distribution of underlying cardiac diagnoses across the three groups is summarized in Supplementary Table S1 and further described in the following section.
Before weighting, baseline characteristics differed substantially among the groups, particularly with respect to operative era, hemodynamic profile, and associated complex anatomic features, including isomerism and atrioventricular valve morphology (Table 1). To reduce these imbalances while preserving the full study population, IPTW after multiple imputation (MI-IPTW) was applied using the seven prespecified core clinical covariates. After MI-IPTW, all variables included in the primary propensity score model achieved acceptable balance, with maximum pairwise absolute standardized mean differences below 0.10 (Table 1 and Fig. S1). Residual imbalance remained in several non-propensity score variables, particularly those reflecting complex anatomic subgroups such as isomerism and atrioventricular valve morphology.
The distribution of underlying anatomical diagnoses varied substantially across ventricular morphology groups (Supplementary Table S1).
Patients with systemic right ventricular morphology were predominantly composed of diagnoses such as hypoplastic left heart syndrome, double outlet right ventricle, and mitral atresia, whereas systemic left ventricular morphology included a high proportion of tricuspid atresia and double inlet left ventricle.
The two-ventricle group demonstrated a heterogeneous anatomical composition, predominantly including atrioventricular septal defect, double outlet right ventricle, and congenitally corrected transposition. Due to the small size of several anatomical subgroups, further stratified analysis combining ventricular morphology and segmental anatomy was not feasible.
Table 1: Baseline demographic and clinical characteristics according to the ventricle morphology in the study population.
| Total (n = 1631) | Ventricle Morphology | p-Value | Maximum Absolute SMD | ||||
|---|---|---|---|---|---|---|---|
| Systemic RV (n = 584) | Systemic LV (n = 630) | 2V (n = 417) | Before IPTW | After IPTW | |||
| Male (n = 1631) | 958 (58.7) | 348 (59.6) | 377 (59.8) | 233 (55.9) | 0.387 | 0.078 | 0.078 |
| Age at Fontan, yrs (n = 1625) | 4.3 (±4.2) | 4.1 (±3.8) | 4.1 (±3.9) | 4.8 (±4.9) | 0.008 | 0.194 | 0.012 |
| Fontan era | <0.01 | 0.349 | 0.052 | ||||
| <2000 | 507 (31.2) | 207 (35.5) | 209 (33.3) | 91 (21.9) | |||
| ≥2000 | 1118 (68.8) | 376 (64.5) | 418 (66.7) | 324 (78.1) | |||
| Right isomerism (n = 1590) | 278 (17.5) | 154 (27.0) | 32 (5.2) | 92 (22.8) | <0.001 | 0.612 | 0.441 |
| Left isomerism (n = 1590) | 75 (4.7) | 41 (7.2) | 5 (0.8) | 29 (7.2) | <0.001 | 0.324 | 0.270 |
| AV valve morphology (n = 1582) | |||||||
| Single TV | 280 (17.7) | 271 (48.6) | 0 (0) | 7 (1.7) | <0.001 | 1.255 | 1.243 |
| Two AVV | 525 (33.2) | 112 (20.1) | 151 (24.5) | 262 (64.4) | <0.001 | 0.998 | 0.960 |
| Single MV | 436 (27.6) | 0 (0) | 427 (69.2) | 11 (2.7) | <0.001 | 1.974 | 1.824 |
| Common AVV | 338 (21.4) | 172 (30.8) | 39 (6.3) | 127 (31.2) | <0.001 | 0.686 | 0.569 |
| Pulmonary venous return anomaly (n = 1598) | 134 (8.4) | 65 (11.3) | 21 (3.4) | 48 (11.8) | <0.001 | 0.301 | 0.040 |
| Bilateral SVC (n = 1618) | 407 (25.2) | 193 (33.4) | 88 (14.1) | 126 (30.4) | <0.001 | 0.496 | 0.428 |
| Azygos continuation (n = 1618) | 62 (3.8) | 36 (6.3) | 4 (0.6) | 22 (5.3) | <0.001 | 0.295 | 0.277 |
| Pre-BCS operation (n = 1631) | |||||||
| None | 717 (43.96) | 318 (54.5) | 232 (36.8) | 167 (40.5) | <0.001 | 0.431 | 0.005 |
| SP shunt | 570 (34.95) | 147 (25.2) | 250 (39.7) | 173 (41.5) | <0.001 | 0.378 | 0.004 |
| PAB | 342 (20.97) | 113 (19.4) | 137 (21.8) | 74 (17.8) | 0.2626 | 0.119 | 0.013 |
| BCS (n = 1631) | 1481 (90.8) | 516 (88.4) | 578 (91.7) | 387 (92.8) | 0.033 | 0.099 | 0.124 |
| Pre-Fontan evaluation | |||||||
| SVEDP, mmHg (n = 1241) | 8.13 (±3.64) | 8.16 (±3.66) | 8.14 (±3.84) | 8.09 (±3.31) | 0.960 | 0.031 | 0.010 |
| Mean PAP, mmHg (n = 1275) | 11.47 (±3.72) | 11.76 (±3.77) | 11.41 (±3.67) | 11.18 (±3.70) | 0.081 | 0.143 | 0.016 |
| PVR (n = 1058) | 1.73 (±1.15) | 1.71 (±1.17) | 1.73 (±1.17) | 1.76 (±1.08) | 0.843 | 0.027 | 0.079 |
| Dysfunction > moderate (n = 1262) | 37 (2.93) | 18 (3.91) | 10 (2.15) | 9 (2.8) | <0.001 | 0.153 | 0.177 |
| AVVR > moderate (n = 1299) | 124 (9.55) | 56 (11.9) | 18 (37) | 50 (14.8) | <0.001 | 0.433 | 0.331 |
| Fontan type (n = 1631) | |||||||
| ECC | 1219 (74.7) | 424 (72.6) | 449 (71.3) | 346 (83.0) | <0.001 | 0.322 | 0.055 |
| LT | 276 (16.9) | 111 (19.0) | 113 (17.9) | 52 | 0.014 | 0.228 | 0.017 |
| APC | 127 (7.8) | 47 (8.0) | 65 (10.3) | 15 (3.6) | <0.001 | 0.264 | 0.086 |
| Fenestration (n = 1571) | 629 (40.04) | 220 (38.6) | 249 (41.6) | 160 (39.8) | 0.7993 | 0.045 | 0.087 |
| CPB time, min (n = 1374) | 127.7 (±55.1) | 135.5 (±55.1) | 116.7 (±53.1) | 132.7 (±55.5) | <0.001 | 0.372 | 0.375 |
| ACC time, min (n = 803) | 45.3 (±31.6) | 45.9 (±31.4) | 41.2 (±28.5) | 49.6 (±34.9) | 0.010 | 0.243 | 0.225 |
| AVV repair/replacement (n = 1631) | 141 (8.6) | 61 (10.4) | 26 (4.1) | 54 (12.9) | <0.001 | 0.342 | 0.226 |
3.3 Long-Term Outcomes According to Ventricular Morphology
A total of 161 late deaths or heart transplantations occurred, including 80 in the systemic right ventricle group, 40 in the 2V group, and 41 in the systemic left ventricle group. The median follow-up duration was 13.2 years (range, 1 month–37.4 years).
Death/transplantation-free survival was significantly lower in the systemic right ventricle group than in the systemic left ventricle group (HR, 1.699; 95% CI, 1.130–2.554; p = 0.011).
In the landmark analyses, systemic right ventricle group remained associated with a higher risk of mortality at early time points, with adjusted hazard ratios of 1.731 (95% CI, 1.138–2.633; p = 0.010) at 3 months and 1.683 (95% CI, 1.102–2.571; p = 0.016) at 6 months. This association was attenuated at 12 months but remained in the same direction, although it did not reach statistical significance (HR, 1.526; 95% CI, 0.989–2.352; p = 0.056) (Table 2, Fig. 1).
In contrast, the 2V group did not differ significantly from the systemic left ventricle group at any time point; although hazard ratios were consistently above 1, none reached statistical significance. Direct comparisons between right ventricle and 2V were also not statistically significant across all analyses.
Table 2: IPTW analysis for long-term outcome.
| Systemic RV vs. LV | 2V vs. systemic LV | Systemic RV vs. 2V | ||||
|---|---|---|---|---|---|---|
| Landmark | HR (95% CI) | p Valve | HR (95% CI) | p Valve | HR (95% CI) | p Valve |
| Death/Heart transplantation | ||||||
| Overall | 1.699 (1.130–2.554) | 0.011 | 1.582 (0.977–2.563) | 0.062 | 1.074 (0.704–1.638) | 0.742 |
| 3 months | 1.731 (1.138–2.633) | 0.010 | 1.507 (0.913–2.489) | 0.109 | 1.148 (0.739–1.784) | 0.539 |
| 6 months | 1.683 (1.102–2.571) | 0.016 | 1.533 (0.925–2.542) | 0.097 | 1.097 (0.703–1.712) | 0.682 |
| 12 months | 1.526 (0.989–2.352) | 0.056 | 1.517 (0.908–2.534) | 0.112 | 1.006 (0.635–1.592) | 0.98 |
| Fontan failure | ||||||
| Overall | 1.487 (1.084–2.038) | 0.014 | 1.207 (0.815–1.788) | 0.347 | 1.231 (0.869–1.744) | 0.241 |
| 3 months | 1.499 (1.073–2.096) | 0.018 | 1.172 (0.789–1.741) | 0.433 | 1.280 (0.887–1.846) | 0.188 |
| 6 months | 1.454 (1.046–2.022) | 0.026 | 1.167 (0.778–1.751) | 0.454 | 1.246 (0.858–1.808) | 0.247 |
| 12 months | 1.356 (0.956–1.924) | 0.088 | 1.150 (0.761–1.739) | 0.506 | 1.179 (0.794–1.751) | 0.415 |

Figure 1: Landmark-weighted Kaplan–Meier curves for death/heart transplantation-free survival according to ventricular morphology. Weighted Kaplan–Meier curves are shown for the 0-month (A), 3-month (B), 6-month (C), and 12-month (D) landmark cohorts. The primary inferential results were based on MI-IPTW landmark Cox proportional hazards models. Numbers at risk and cumulative events are shown below each panel. Abbreviations: LV, systemic left ventricle; RV, systemic right ventricle; 2V, two adequately sized ventricles.
Fontan failure occurred in 221 patients during follow-up: 101 in the systemic right ventricle group, 65 in the systemic left ventricle group, and 55 in the 2V group. A similar pattern was observed for Fontan failure. Fontan failure-free survival was also poorer in the systemic right ventricle group compared with the systemic left ventricle group (HR, 1.487; 95% CI, 1.084–2.038; p = 0.014). In the landmark analysis, the systemic right ventricle group remained associated with a higher risk of Fontan failure at early time points, with hazard ratios of 1.499 (95% CI, 1.073–2.096; p = 0.018) at 3 months and 1.454 (95% CI, 1.046–2.022; p = 0.026) at 6 months. This association was attenuated after 12 months but remained in the same direction, although it did not reach statistical significance (HR, 1.356; 95% CI, 0.956–1.924; p = 0.088) (Table 2, Fig. 2).
The 2V group did not differ significantly from the systemic left ventricle group at any time point. Direct comparisons between the systemic right ventricle and 2V groups were also not statistically significant across all analyses.

Figure 2: Landmark-weighted Kaplan–Meier curves for Fontan failure-free survival according to ventricular morphology. Weighted Kaplan–Meier curves are shown for the 0-month (A), 3-month (B), 6-month (C), and 12-month (D) landmark cohorts. The primary inferential results were based on MI-IPTW landmark Cox proportional hazards models. Numbers at risk and cumulative events are shown below each panel. Abbreviations: LV, systemic left ventricle; RV, systemic right ventricle; 2V, two adequately sized ventricles.
3.4 Sensitivity Analysis Using Multivariable Cox Models
The sensitivity analysis yielded results broadly consistent with the IPTW-based analysis. In the multiple imputation–based multivariable Cox analysis adjusted for the same covariates, the systemic right ventricle versus systemic left ventricle contrast remained significantly associated with both mortality and Fontan failure across all landmarks, including at 12 months (Supplementary Table S2). These findings support the robustness of the primary results.
In pediatric patients undergoing Fontan surgery with a functional single ventricle, ventricular morphology varies and includes a systemic right ventricle, a systemic left ventricle, or two adequately sized ventricles. Persistent concern remains about whether ventricular morphology, particularly a systemic right ventricle with its distinct myocardial architecture and contraction pattern, might influence long-term outcomes following Fontan surgery.
Our study examined the impact of ventricular morphology on long-term outcomes following Fontan surgery, comparing patients with a systemic right ventricle, a systemic left ventricle, and two adequately sized ventricles. To mitigate confounding and baseline imbalance, we applied inverse probability of treatment weighting after multiple imputation within a unified landmark analysis framework.
Results showed that death/transplantation-free survival rates and Fontan failure-free rates were worse with the systemic right ventricle compared to the systemic left ventricle. This association was most pronounced during early and intermediate periods and attenuated beyond 12 months, while maintaining a consistent direction across analytical approaches. Moreover, the 2V group did not demonstrate superior outcomes compared to either the systemic left or the systemic right ventricle groups.
Patients with a systemic right ventricle showed the poorest long-term outcome after the Fontan procedure. Previous studies have suggested that ventricular morphology influences long-term outcomes. A recent meta-analysis examining 27 studies focused on the impact of ventricular morphology in Fontan palliation [10] and reported that a systemic right ventricle was associated with worse long-term survival. Our findings are consistent with these observations. Even after adjustment for potential factors that could influence long-term outcomes, a systemic right ventricle was consistently associated with poorer outcomes.
Vulnerability in the myocardial architecture of a systemic right ventricle in patients who underwent the Fontan procedure has been highlighted by several studies on myocardial architecture and ventricular strain. One study on ventricular strain in patients who underwent the Fontan procedure observed that global radial strain and circumferential strain were lower in dominant right ventricle patients compared to dominant left ventricle patients both before and after Fontan surgery [11]. Another study reported that patients who underwent the Fontan procedure with a dominant right ventricle have higher myocardial wall stress, a higher rate of ventricular dilatation, and lower circumferential myocardial shortening compared to those with a dominant left ventricle, with these factors associated with death or heart transplantation [12].
Importantly, our findings extend prior observations by showing that the impact of systemic right ventricular morphology is not constant over time, with a greater effect in the early and intermediate periods and attenuation during later follow-up.
Notably, and unexpectedly, 2V morphology did not confer a prognostic advantage compared with either systemic left or systemic right ventricle. The lack of significant differences between the systemic right ventricle group and the 2V group suggests that outcomes may be influenced by factors beyond ventricular morphology alone. One possible explanation is the influence of atrioventricular valve morphology. In our cohort, a single mitral valve—the most favorable systemic atrioventricular valve morphology—was observed almost exclusively in the systemic left ventricle group, whereas it was absent in the systemic right ventricle group and rare in the 2V group. In contrast, patients with a systemic right ventricle more frequently had a tricuspid valve or a common atrioventricular valve, while those with two adequately sized ventricles most commonly had two atrioventricular valves. These differences in systemic atrioventricular valve morphology distribution may partially explain why the 2V group did not demonstrate superior outcomes compared with the systemic right ventricle group. However, more detailed subclassification combining ventricular morphology and atrioventricular anatomy was not feasible, as it would have resulted in numerous subgroups, each with insufficient sample sizes for meaningful analysis. In particular, atrioventricular valve morphology was unevenly distributed across ventricular morphology groups, further limiting the feasibility of combined subgroup analyses. Therefore, the possibility of residual confounding cannot be excluded.
This observation is supported by prior studies. In patients with congenitally corrected transposition, systemic tricuspid valve failure occurred in approximately one-third of patients, and systemic tricuspid valve failure emerged as the sole factor associated with decreased survival [13]. This finding may similarly apply to patients with single ventricle physiology. In addition, a multicenter study in children with a single ventricle and unbalanced atrioventricular septal defect showed similar results [14]. A quarter of patients required atrioventricular valve surgery, and the study revealed that severe atrioventricular valve regurgitation was associated with poor long-term outcomes. At least in comparisons between the systemic right ventricle and the 2V groups, factors such as atrioventricular valve morphology may have a greater influence on outcomes than ventricular morphology itself.
Another contributing factor may be ventricular dyssynchrony. Cardiac magnetic resonance imaging studies of patients with Fontan circulation revealed higher dyssynchrony metrics in those with systemic right ventricle or mixed morphology compared to those with systemic left ventricle morphology [15]. Elevated dyssynchrony indices are associated with an increased risk of death or the need for heart transplantation [15,16]. An echocardiographic study reported that a classic pattern dyssynchrony is observed in a substantial number of adolescent and adult patients with Fontan circulation. Patients with two sizable ventricular components exhibit broad QRS duration and classic pattern of dyssynchrony [17]. These findings suggest that the mechanical dyssynchrony observed in two adequately sized ventricles may be related to their unfavorable long-term outcomes in our study despite the presence of two functional ventricles.
Our findings suggest that the prognostic role of ventricular morphology in Fontan circulation is more nuanced than previously recognized. The impact of systemic right ventricular morphology is time-dependent, and the presence of two adequately sized ventricles does not necessarily confer a prognostic advantage. Factors beyond ventricular morphology, including atrioventricular valve characteristics and ventricular synchrony, may influence long-term outcomes.
This study has limitations inherent to its retrospective design and reliance on registry data. Ventricular morphology classification was based on a registry-recorded variable reflecting institutional echocardiographic and surgical assessments, which may have introduced some inter-center variability. Additionally, it utilized data from multiple centers, potentially introducing variability in surgical techniques, perioperative care, and follow-up protocols, which may have influenced the long-term outcomes. The effects of ventricular morphology could not be clearly distinguished from those of atrioventricular valve morphology. This limitation reflects both small subgroup sizes and the inherent distribution of valve types across ventricular morphology groups. Consequently, detailed subgroup analyses combining these anatomical features were not feasible, potentially leading to residual confounding related to anatomical heterogeneity.
Systemic right ventricular morphology was associated with the poorest long-term outcomes following Fontan completion. The impact of systemic right ventricular morphology appeared to be time-dependent. Although the two ventricles had adequately sized chambers, they did not demonstrate a clear prognostic advantage compared with other ventricular morphologies. These findings highlight the need for careful long-term surveillance, especially in patients with a systemic right ventricle and in those with two adequately sized ventricles.
Acknowledgement:
Funding Statement: The authors declare financial support for the research, authorship, and/or publication of this article. This research was supported and funded by the SNUH Lee Kunhee Child Cancer & Rare Disease Project, Republic of Korea (grant number: 23C-030-00400).
Author Contributions: Jae Suk Baek: conceptualization; data curation; formal analysis; Investigation; methodology; project administration; visualization; writing—original draft. Soo-Jin Kim: conceptualization; data curation; formal analysis; funding acquisition; investigation; methodology; project administration; supervision; visualization; validation; writing—review & editing. Sang-Yun Lee: data curation; investigation. Chang-Ha Lee: data curation; investigation. Chun Soo Park: data curation; investigation. Eun Seok Choi: data curation; investigation. Hoon Ko: data curation; investigation. Hyo Soon An: data curation; investigation. I. Seok Kang: data curation; investigation. Ja Kyoung Yoon: data curation; investigation. Jae-Young Lee: data curation; investigation. Jinyoung Song: data curation; investigation. Joo Won Lee: data curation; investigation. June Huh: data curation; investigation. Kyung-Jin Ahn: data curation; investigation. Se-Yong Jung: data curation; investigation. Seul Gi Cha: data curation; investigation. Yeo-Hyang Kim: data curation; investigation. Young-Seok Lee: data curation; investigation. Sang-Hoon Cho: formal analysis. All authors reviewed and approved the final version of the manuscript.
Availability of Data and Materials: The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval: This study was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the Sejong General Hospital Institutional Review Board (Approval No. 2022-12-007), and the requirement for informed consent was waived due to the retrospective nature of the study design. Neither the study participants nor the public were involved in the design, conduct, reporting or dissemination plans of this study. All ethical standards were met in writing and submitting this article.
Conflicts of Interest: The authors declare no conflicts of interest.
Supplementary Materials: The supplementary material is available online at https://www.techscience.com/doi/10.32604/schd.2026.077034/s1.
Abbreviations
| AVVR | Atrioventricular valve regurgitation. |
| IPTW | inverse probability of treatment weighting |
| 2V | two adequately sized ventricles |
Appendix A Key Members of the Korean Fontan Registry Committee
| Key Members | Affiliations |
| Jeong Jin Yu, Tae-Jin Yun | Asan Medical Center, Seoul, Korea |
| Hyoung Doo Lee, Hyungtae Kim | Pusan National University Children’s Hospital |
| Chang Hyu Choi | Gachon University Gil Medical Center |
| Myung Chul Hyun, Joon Yong Cho | Kyungpook National University Hospital |
| Tae-Gook Jun, Ji-Hyuk Yang | Samsung Medical Center |
| Yong-Jin Kim, Jeong-Il Noh, Seong-Ho Kim | Sejong General Hospital |
| Woong-Han Kim, Eun-Jung Bae, Gi-Beom Kim | Seoul National University Children’s Hospital |
| Young Hwan Park, Han Ki Park, Jae Young Choi | Severance Cardiovascular Hospital |
| Cheul Lee | The Catholic University of Korea Seoul St. Mary’s Hospital |
References
1. Alsaied T, Bokma JP, Engel ME, Kuijpers JM, Hanke SP, Zuhlke L, et al. Factors associated with long-term mortality after Fontan procedures: A systematic review. Heart. 2017;103(2):104–10. doi:10.1136/heartjnl-2016-310108. [Google Scholar] [CrossRef]
2. Moon J, Shen L, Likosky DS, Sood V, Hobbs RD, Sassalos P, et al. Relationship of ventricular morphology and atrioventricular valve function to long-term outcomes following Fontan procedures. J Am Coll Cardiol. 2020;76(4):419–31. doi:10.1016/j.jacc.2020.05.059. [Google Scholar] [CrossRef]
3. King G, Buratto E, Cordina R, Iyengar A, Grigg L, Kelly A, et al. Atrioventricular septal defect in Fontan circulation: Right ventricular dominance, not valve surgery, adversely affects survival. J Thorac Cardiovasc Surg. 2023;165(2):424–33. doi:10.1016/j.jtcvs.2022.04.011. [Google Scholar] [CrossRef]
4. d’Udekem Y, Xu MY, Galati JC, Lu S, Iyengar AJ, Konstantinov IE, et al. Predictors of survival after single-ventricle palliation: The impact of right ventricular dominance. J Am Coll Cardiol. 2012;59(13):1178–85. doi:10.1016/j.jacc.2011.11.049. [Google Scholar] [CrossRef]
5. Alsoufi B, Gillespie S, Kim D, Shashidharan S, Kanter K, Maher K, et al. The impact of dominant ventricle morphology on palliation outcomes of single ventricle anomalies. Ann Thorac Surg. 2016;102(2):593–601. doi:10.1016/j.athoracsur.2016.04.054. [Google Scholar] [CrossRef]
6. King G, Ayer J, Celermajer D, Zentner D, Justo R, Disney P, et al. Atrioventricular valve failure in Fontan palliation. J Am Coll Cardiol. 2019;73(7):810–22. doi:10.1016/j.jacc.2018.12.025. [Google Scholar] [CrossRef]
7. Anderson PA, Sleeper LA, Mahony L, Colan SD, Atz AM, Breitbart RE, et al. Contemporary outcomes after the Fontan procedure: A Pediatric Heart Network multicenter study. J Am Coll Cardiol. 2008;52(2):85–98. doi:10.1016/j.jacc.2008.01.074. [Google Scholar] [CrossRef]
8. Rossi E, Frigo AC, Reffo E, Cabrelle G, Castaldi B, Di Salvo G, et al. The presence of an additional ventricular chamber does not change the outcome of Fontan circulation: A comparative study. Eur J Cardiothorac Surg. 2021;60(5):1074–81. doi:10.1093/ejcts/ezab194. [Google Scholar] [CrossRef]
9. Lee SY, Kim SJ, Lee CH, Park CS, Choi ES, Ko H, et al. The long-term outcomes and risk factors of complications after Fontan surgery: From the Korean Fontan Registry (KFR). Korean Circ J. 2024;54(10):653–68. doi:10.4070/kcj.2023.0211. [Google Scholar] [CrossRef]
10. Ponzoni M, Azzolina D, Vedovelli L, Gregori D, Di Salvo G, D’Udekem Y, et al. Ventricular morphology of single-ventricle hearts has a significant impact on outcomes after Fontan palliation: A meta-analysis. Eur J Cardiothorac Surg. 2022;62(6):ezac535. doi:10.1093/ejcts/ezac535. [Google Scholar] [CrossRef]
11. Shiraga K, Ozcelik N, Harris MA, Whitehead KK, Biko DM, Partington SL, et al. Imposition of Fontan physiology: Effects on strain and global measures of ventricular function. J Thorac Cardiovasc Surg. 2021;162(6):1813–22.e3. doi:10.1016/j.jtcvs.2021.02.034. [Google Scholar] [CrossRef]
12. Ghelani SJ, Colan SD, Azcue N, Keenan EM, Harrild DM, Powell AJ, et al. Impact of ventricular morphology on fiber stress and strain in Fontan patients. Circ Cardiovasc Imaging. 2018;11(7):e006738. doi:10.1161/CIRCIMAGING.117.006738. [Google Scholar] [CrossRef]
13. Huhta JC, Danielson GK, Ritter DG, Ilstrup DM. Survival in atrioventricular discordance. Pediatr Cardiol. 1985;6(2):57–60. doi:10.1007/BF02282738. [Google Scholar] [CrossRef]
14. Arrigoni SC, IJsselhof R, Postmus D, Vonk JM, Francois K, Bove T, et al. Long-term outcomes of atrioventricular septal defect and single ventricle: A multicenter study. J Thorac Cardiovasc Surg. 2022;163(3):1166–75. doi:10.1016/j.jtcvs.2021.05.015. [Google Scholar] [CrossRef]
15. Gearhart A, Bassi S, Rathod RH, Beroukhim RS, Lipsitz S, Gold MP, et al. Ventricular dyssynchrony late after the Fontan operation is associated with decreased survival. J Cardiovasc Magn Reson. 2023;25(1):66. doi:10.1186/s12968-023-00984-3. [Google Scholar] [CrossRef]
16. Ishizaki U, Nagao M, Shiina Y, Inai K, Mori H, Takahashi T, et al. Global strain and dyssynchrony of the single ventricle predict adverse cardiac events after the Fontan procedure: Analysis using feature-tracking cine magnetic resonance imaging. J Cardiol. 2019;73(2):163–70. doi:10.1016/j.jjcc.2018.07.005. [Google Scholar] [CrossRef]
17. Rosner A, Khalapyan T, Dalen H, McElhinney DB, Friedberg MK, Lui GK. Classic-pattern dyssynchrony in adolescents and adults with a Fontan circulation. J Am Soc Echocardiogr. 2018;31(2):211–9. doi:10.1016/j.echo.2017.10.018. [Google Scholar] [CrossRef]
Cite This Article
 Copyright © 2026 The Author(s). Published by Tech Science Press.
Copyright © 2026 The Author(s). Published by Tech Science Press.This work is licensed under a Creative Commons Attribution 4.0 International License , which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
 Downloads
Downloads
 Citation Tools
Citation Tools