
 Submit a Paper
Submit a Paper Propose a Special lssue
Propose a Special lssue Open Access
Open Access
CASE REPORT

Penile shaft reconstruction after cream self-injection: a case report
1 Department of Urology, Clinique Universitaire Saint-Luc., Bruxelles, 1200, Belgium
2 Department of Urology, CHU Helora (site Jolimont, Lobbes et Nivelles), Louvière, 7100, Belgium
3 Department of Plastic Surgery, CHU Helora (site Jolimont, Nivelles), Louvière, 7100, Belgium
4 Department of Urology, CHU Helora (site Jolimont, Nivelles), Louvière, 7100, Belgium
* Corresponding Author: Léa Bollen. Email:
Canadian Journal of Urology 2026, 33(1), 221-225. https://doi.org/10.32604/cju.2025.067192
Received 26 April 2025; Accepted 04 September 2025; Issue published 28 February 2026
 View Full Text
View Full Text Download PDF
Download PDFAbstract
Background: Penile augmentation through injectable substances is becoming increasingly common. A growing number of aesthetic clinics are developing penile enlargement procedures using various injectable materials. Although these procedures are now performed in more controlled and medically supervised environments, their long-term outcomes remain poorly understood. The promotion of such medical treatments contributes to an increasing interest among adult males in self-injection as a method to alleviate psychological distress associated with penile size concerns. At the same time, access to injectable substances through unofficial or unregulated sources has become increasingly easy. Tor our knowledge, we report the first documented case of self-injection with Garamycin® (gentamicin) cream, contributing to the literature on the often multidisciplinary management of penile enlargement injections, a field still lacking well-established guidelines. Case Description: This case report describes a young patient who self-injected Garamycin® into the penis for the purpose of enlargement. He presented to our urology department with worsening symptoms, including severe and poorly tolerated pain. His primary request was prompt relief of pain while preserving, as much as possible, the aesthetic appearance and functional integrity of his penis. This case required a multi-stage surgical approach to salvage the penis and preserve both its structural integrity and functional outcome. Conclusions: To our knowledge, this case report documents the first reported instance of Garamycin® injection performed for the purpose of penile enlargement. It provides insight into the clinical course of such penile cream injections, demonstrates that a two-stage scrotal flap can achieve both functional and aesthetic outcomes, and highlights the importance of comprehensive management particularly addressing the traumatic impact of penile deformity secondary to inflammation and/or infection, as well as the body dysmorphic concerns often associated with these cases.Keywords
Self-injections to increase penile size are becoming increasingly common. The most frequently injected substances are silicone and paraffin,1 although a wide variety of materials may be used, particularly when the procedure is performed outside of a medical institution. The majority of these cases require surgical intervention, ranging from simple circumcision to more complex flap-based reconstruction.2,3 In selected situations, however, conservative management may be appropriate an approach that is particularly suitable for young men4 although it is not always feasible. Multiple surgical procedures may be necessary to address complications or improve the final aesthetic outcome.5,6 To our knowledge, we report the first documented case of self-injection with Garamycin® cream and describe the surgical management performed to preserve both penile function and appearance.
This case report adds to the literature on surgical management options for penile self-injections. It describes the clinical course of a Garamycin® injection a substance promoted on certain non-medical websites for the purpose of penile enlargement. This report highlights the need to develop more standardized management protocols for such cases.
A 30-year-old patient with no known medical history presented in the emergency department with complaints of penile pain, progressive swelling, skin burns, and an inability to engage in sexual intercourse. The patient reported having self-injected Garamycin (an antibiotic commonly used in ophthalmology and otorhinolaryngology) twice into the subcutaneous tissue of the penis to enhance its size, approximately three months prior to presentation.
He obtained this cream by himself after reading online websites promoting its effectiveness for penile enlargement. The patient performed these injections in a context of significant psychological stress related to concerns about the size of his penis and his sexual performance. Initially, sexual intercourse remained possible, as no side effects were observed during the first three months following the injections. However, progressive swelling and pain subsequently developed.
Laboratory tests revealed normal biological parameters. On clinical examination, the penis was swollen and edematous, with areas of cyanotic and pale skin discoloration, significant and tender induration, and a lateral wound (Figure 1). The glans aspect was normal, supple, and painless.

FIGURE 1. Clinical presentation
Ultrasound and MRI (Figure 2) demonstrated a diffuse thickening and infiltration of the subcutaneous tissues of the penile shaft, extending up to 1.5 cm in depth, associated with increased vascularity consistent with cellulitis.1 There was no evidence of abscess formation. The corpora cavernosa and spongiosa were unaffected. Doppler imaging demonstrated reduced vascularization of the dorsal venous plexus, likely secondary to external compression from the injected substance.
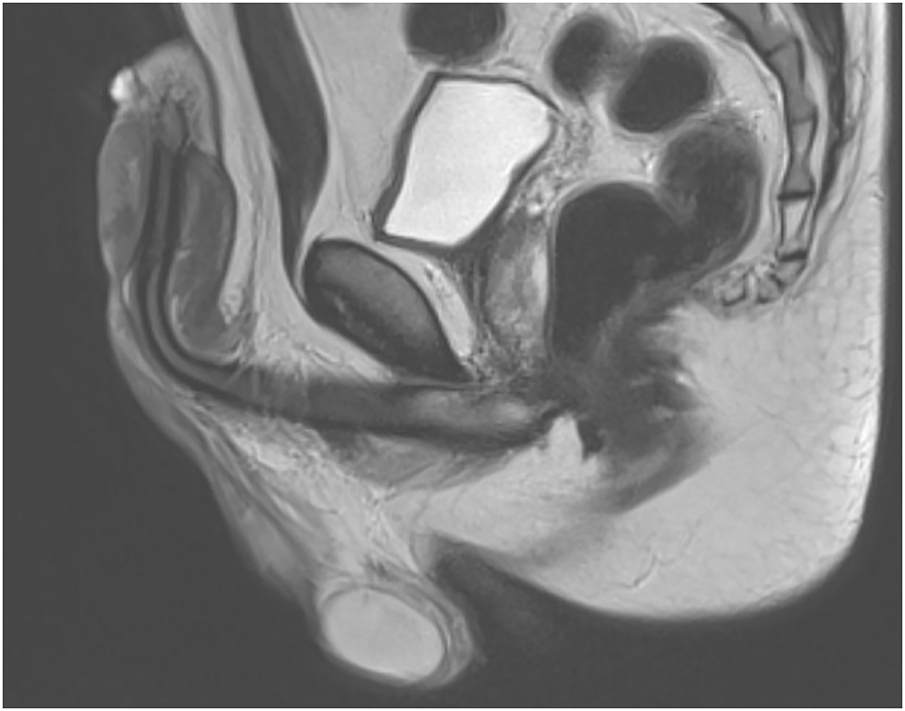
FIGURE 2. Penile MRI
During the workup, the patient’s pain rapidly required medical support and surgery was decided due to the risk of local infection and gangrene.
The patient underwent a penile degloving procedure, with preservation of the intact mucosa located just distal to the coronal sulcus. An elliptical circumferential incision was performed at the base of the shaft, in an area where the skin appeared clinically unaffected, to allow for the excision of all devitalized tissue and to expose the underlying corpora cavernosa (CC) and corpus spongiosum (CS).
Additionally, an incision was performed in the indurated area on the dorsal side of the penis to remove all necrotic and sclerotic tissue, exposing the CC, CS, and neurovascular bundle.7 The extent and depth of the involvement necessitated a deep excision in close proximity to the neurovascular structures, while preserving their integrity (Figure 3).

FIGURE 3. Penile degloving
At the end the penis was buried within the scrotal skin to maintain the coverage and to allow natural micturition.3 The urethra was completely preserved. A drain was left in place for 24 h (Figure 4).
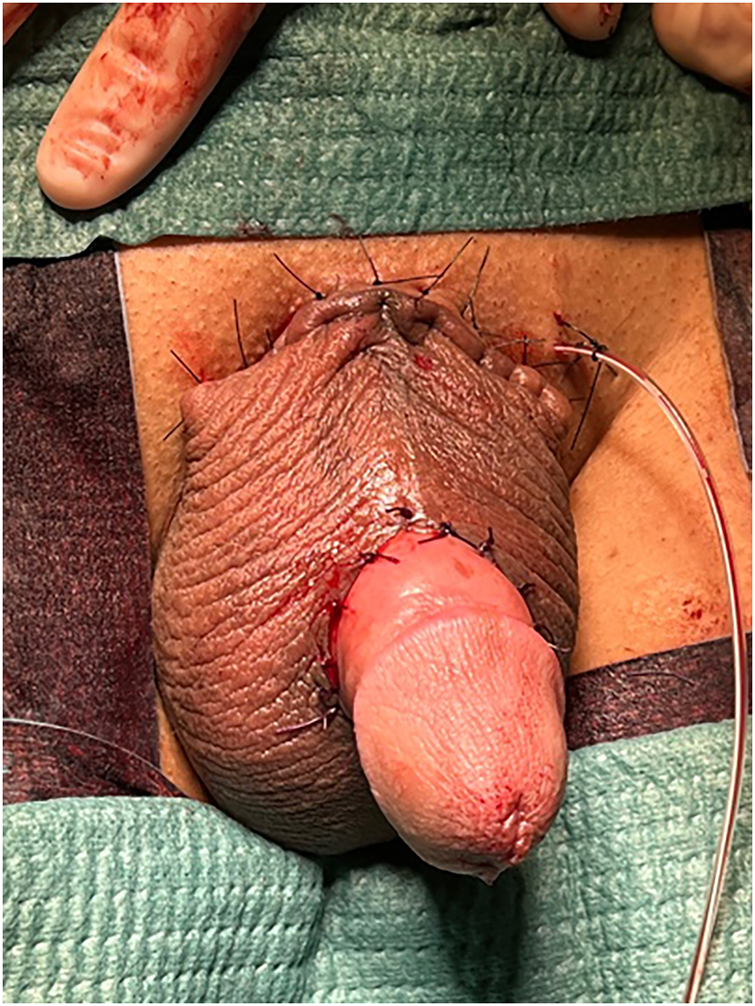
FIGURE 4. Scrotal burying of the penis
Histopathological analysis confirmed the presence of an inflammatory reaction characterized by macrophage infiltration and multinucleated giant cells, along with areas of fat necrosis in the subcutaneous penile tissue.8
Forty-five days after the first surgery, a ventral incision was performed in the inferior aspect of the penis to reconstruct the penile sheath. This procedure involved creating incisions along the underside of the penis while ensuring sufficient tissue was preserved to support the distal portions of the scrotal flap along the lower midline. It’s a native skin coverage9 (Figure 5). The second surgical intervention was carried out in an outpatient setting.

FIGURE 5. Scrotal flap
One year after the initial surgery and following a revision procedure performed three months postoperatively to address excess skin at the base of the penis (Figure 6). The patient has retained full sensitivity and functionality of the penis, with the scrotal flap enabling effective erection and sexual intercourse.

FIGURE 6. Final surgical outcome
This case highlights three key aspects of penile self-injection.
First, a wide array of injectable substances is available outside regulated medical frameworks, allowing patients to perform self-injections under non-sterile and unsafe conditions. The most frequently reported agents include silicone and paraffin.1 Case reports in the literature often describe a delayed onset of local or systemic complications following injection.5,6
Second, the absence of standardized guidelines for surgical management presents a therapeutic challenge.2 Since the treatment of our patient, a systematic review has summarized commonly injected agents, associated risks, and management strategies.4 It advocates a conservative approach, particularly in younger patients, favoring serial debridement and, when needed, vacuum-assisted closure (VAC) therapy. In our case, the extent of tissue necrosis necessitated wide excision, precluding conservative management. A two-stage scrotal flap was chosen over a single-stage reconstruction to obtain a longer, more viable flap and promote optimal healing. The final aesthetic and functional outcomes were satisfactory. Residual pilosity on the flap may be managed with laser hair removal if necessary. Conservative approaches are the first way to go, and surgical planning must be tailored to the extent of tissue damage, preservation of neurovascular structures, and the anticipated functional and cosmetic outcomes.
The psychological dimension is critical.4 Patients frequently present with penile dysmorphophobia, an inaccurate perception of inadequate penile size. Whether performed in medical or non-medical settings, such procedures rarely lead to sustained improvement in body image. These behaviors often reflect deeper psychological distress.10 For this reason, psychological evaluation and support should be systematically offered to patients presenting with self-injection related complications. Even when surgical outcomes are functionally and aesthetically acceptable, psychological sequelae may persist.
Further documentation of such cases is essential. Efforts should be directed toward developing standardized, multidisciplinary management protocols combining surgical and psychological care to optimize long-term outcomes in this vulnerable population.
Acknowledgement
The authors would like to thank the Urology Department of Jolimont Hospital for their valuable support in the preparation of this case report, with special thanks to Gilles Dosin. Special thanks to Estelle Lapraille for her assistance with language and editorial revisions.
Funding Statement
The authors received no specific funding for this study.
Author Contributions
The authors confirm contribution to the paper as follows: Data collection: Stéphane Rysselinck, Jean-Philippe Salmin; Study conception, case analysis, and manuscript preparation: Léa Bollen; Continuous support and contribution throughout all stages of the case report: Gilles Dosin. All authors reviewed the results and approved the final version of the manuscript.
Availability of Data and Materials
Data sharing is not applicable to this article as this is a case report, and no datasets were generated or analyzed during the study.
Ethics Approval
This study was conducted with the informed consent of the patient. As this is a case report, it was exempted from full ethical review after being approved by ethics committee of the author’s affiliated institution (Comité d’Ethique Hôpitaux de Jolimont–Lobbes–Nivelles–Tubize).
Conflicts of Interest
The authors declare no conflicts of interest to report regarding the present study.
References
1. Pang KH, Randhawa K, Tang S et al. Complications and outcomes following injection of foreign material into the male external genitalia for augmentation: a single-centre experience and systematic review. Int J Impot Res 2024;36(5):498–508. doi:10.1038/s41443-023-00675-8. [Google Scholar] [PubMed] [CrossRef]
2. Yao H, Zheng D, Xie M et al. A modified bilateral scrotal flap for penile skin defect repair. J Vis Exp 2022;189. doi:10.3791/64017. [Google Scholar] [PubMed] [CrossRef]
3. Svensøy JN, Travers V, Osther PJS. Complications of penile self-injections: investigation of 680 patients with complications following penile self-injections with mineral oil. World J Urol 2018;36(1):135–143. doi:10.1007/s00345-017-2110-9. [Google Scholar] [PubMed] [CrossRef]
4. Penske WL, Leslie DC, Latini JM, Lerner LB. Injectable penile enhancement procedures : a review of agents, risks, and complications. Urology 2024;189(suppl_1):126–134. doi:10.1016/j.urology.2024.05.013. [Google Scholar] [PubMed] [CrossRef]
5. De Siati M, Selvaggio O, Di Fino G et al. An unusual delayed complication of paraffin self-injection for penile girth augmentation. BMC Urol 2013;13(1):66. doi:10.1186/1471-2490-13-66. [Google Scholar] [PubMed] [CrossRef]
6. Son H, Pae W. Reconstruction using a scrotal flap with autologous augmentation for delayed infection caused by penile filler injection: a case report. Medicina 2023;59(11):1998. doi:10.3390/medicina59111998. [Google Scholar] [PubMed] [CrossRef]
7. Mendel L, Neuville P, Allepot K et al. Bilateral pedicled scrotal flaps as an alternative to skin graft in penile shaft defects repair. Urology 2023;176(suppl 4):206–212. doi:10.1016/j.urology.2023.03.025. [Google Scholar] [PubMed] [CrossRef]
8. Zimmermann US, Clerici TJ. The histological aspects of fillers complications. Semin Cutan Med Surg 2004 Dec;23(4):241–250. doi:10.1016/j.sder.2004.09.004. [Google Scholar] [PubMed] [CrossRef]
9. Fakin R, Zimmermann S, Jindarak S, Lindenblatt N, Giovanoli P, Suwajo P. Reconstruction of penile shaft defects following silicone injection by bipedicled anterior scrotal flap. J Urol 2017;197(4):1166–1170. [Google Scholar] [PubMed]
10. Chifano N, Cakir OO, Castiglione F et al. Multidisciplinary approach and management of patients who seek medical advice for penile size concerns: a narrative review. Int J Impot Res 2022;34(5):434–451. doi:10.1038/s41443-021-00444-5. [Google Scholar] [PubMed] [CrossRef]
Cite This Article
 Copyright © 2026 The Author(s). Published by Tech Science Press.
Copyright © 2026 The Author(s). Published by Tech Science Press.This work is licensed under a Creative Commons Attribution 4.0 International License , which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
 Downloads
Downloads
 Citation Tools
Citation Tools