
 Submit a Paper
Submit a Paper Propose a Special lssue
Propose a Special lssue Open Access
Open Access
ARTICLE

Shifting the Paradigm: A Fresh Look at Physical Activity Frequency and Its Impact on Mental Health, Life Satisfaction, and Self-Rated Health in Adolescents
1 Country School of Recreation and Community Sport, Capital University of Physical Education and Sports, Beijing, 100191, China
2 Institute of Physical Education and Training, Capital University of Physical Education and Sports, Beijing, 100191, China
* Corresponding Author: Xiaotian Li. Email:
(This article belongs to the Special Issue: Mental Health and Social Development)
International Journal of Mental Health Promotion 2024, 26(2), 83-92. https://doi.org/10.32604/ijmhp.2023.042014
Received 15 May 2023; Accepted 22 August 2023; Issue published 08 March 2024
 View Full Text
View Full Text Download PDF
Download PDFAbstract
As adolescent mental health problems are becoming a more serious issue globally, this paper explores the relationship of physical activity in adolescents and its frequency on mental health as well as examines the mediating effects of life satisfaction and self-rated health in order to provide a reference for the promotion of mental health in adolescents. A sample of 3578 Chinese high school students completed questionnaires assessing their mental health, physical activity frequency, life satisfaction, and self-rated health. The mean SCL-90 value for adolescents was found to be 1.629%, and 24.73% of adolescents had varying degrees of mental health issue. Increased physical activity frequency is positively associated with improved mental health (p < 0.001). Additionally, life satisfaction and self-rated health were found to play significant mediating roles in the relationship between physical activity frequency and mental health. Specifically, low-frequency physical activity had the most pronounced mediating effect on mental health through life satisfaction, while high-frequency physical activity exerted the most significant mediating effect on mental health through self-rated health. These findings underscore the importance of promoting physical activity among adolescents and highlight the distinct pathways through which physical activity frequency can influence mental health outcomes. Further research is needed to explore these relationships in diverse populations and settings, as well as to develop targeted intervention.Keywords
It has been estimated that approximately 10%–20% of adolescents globally experience mental health issues, a number that continues to rise [1]. Evidence suggests that a significant portion of adult mental health challenges originate during adolescence or persist from adolescent mental disorders [2]. As such, fostering positive mental health is crucial for the comprehensive development of adolescents, given that there can be no health without mental health [3]. Although the significance of promoting and preventing adolescent mental health issues has been widely acknowledged, adolescents are undergoing a unique period in their mental health development. Rapid physiological and psychological changes render this age group vulnerable to mental health challenges, which is why research on adolescent mental health remains a pressing concern for society.
The relationship between physical activity and its impact on physical health has been well-established within the academic community. Consequently, researchers have extended the examination of the positive effects of physical activity to encompass various psychological domains. Empirical evidence has highlighted the beneficial impact of physical activity on mental health, encompassing improvements in self-perception, social skills, and cognitive functioning, as well as a reduction in anxiety symptoms [4]. Furthermore, moderate and positive effects of physical activity on generalized anxiety disorder, phobias, panic attacks, and stress-related disorders have been observed [5]. As investigations have progressively deconstructed the components of physical activity, Ai et al. and Stubbs et al. have determined that both intensive and frequent physical activity positively contribute to enhancing mental health in adolescents [6,7]. However, evidence links excessive exercise to increased anxiety and heightened risk of adverse psychological consequences [8]. Consequently, the effects of physical activity frequency on mental health remain a topic of debate, with only a limited number of researchers having examined this issue within the context of mental health problems among Chinese adolescents.
Physical activity has been demonstrated to bolster mental health but also to correlate with life satisfaction [9]. In relation to life satisfaction, it is characterized as an individual’s subjective appraisal of their overall quality of life, constituting a cognitive variable [10]. Life satisfaction plays a pivotal role in evaluating mental health, and the development of concomitant psychobehavioral complications may be impeded by fostering life satisfaction in adolescents [11,12]. According to Feng et al. [13], a greater frequency of physical activity exhibits a stronger correlation with increased life satisfaction. As a result, there is a mediating effect of life satisfaction in physical activity and adolescent mental health.
On the other hand, physical activity has been linked to elevated self-rated health [14]. Concerning self-rated health—which functions as a uniquely valuable metric in individual health assessments—individuals engage in screening, appraising, and integrating information pertinent to both physical and psychological domains [15]. Subjective self-rated health, grounded in one’s perception of their own body, is influenced by sub-optimal physical conditions, resulting in adverse emotions and concerns regarding future physical health, which may subsequently impact mental health. Vingilis et al. has posited that adolescents’ self-rated health relies not only on physical health status but also psychological factors, with psychological distress correlating to lower self-rated health [16]. A notable association has been identified between physical activity frequency and self-rated health in adolescents, with enhancements in self-rated health coinciding with increased physical activity frequency [17]. Hence, self-rated health plays a mediating role in physical activity and young people’s mental health.
In summary, the underlying mechanisms and the role of physical activity frequency remain underexplored. At the same time, there was a lack of research exploring life satisfaction and self-rated health as mediators. The contribution of this study lies in its examination of the relationship between physical activity, mental health, life satisfaction, and self-rated health. By examining both low-, medium-, and high-frequency physical activity, this research provides a more nuanced understanding of the relationship between physical activity and adolescents’ mental health. Furthermore, the mediating roles of life satisfaction and self-rated health are investigated, offering valuable insights into the psychological and physiological mechanisms through which physical activity may improve mental health. These findings have significant implications for the development of targeted interventions and policies aimed at promoting mental health among adolescents by leveraging physical activity and its associated benefits. At the same time, this study uses a large sample of Chinese high school students, which enables the findings to be more generalizable and provides an essential perspective on mental health in this population. Focusing on the Chinese context contributes to the growing body of literature examining mental health in non-Western settings, enriching our understanding of the global dimensions of adolescent mental health. The following hypotheses are proposed in light of the above, with the associated research pathways shown in Fig. 1.
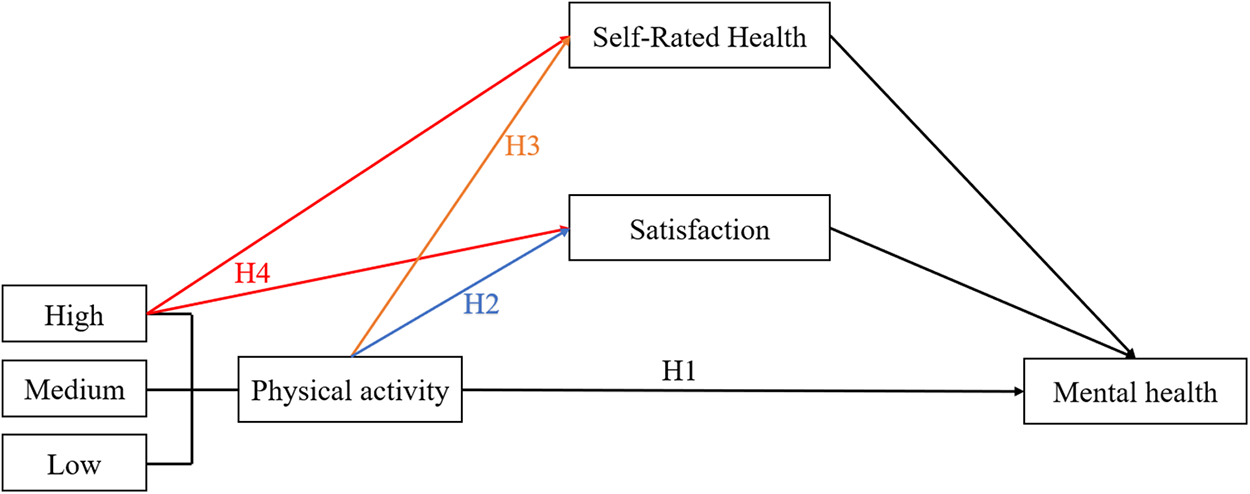
Figure 1: Research pathways.
Hypothesis1(H1): The frequency of physical activity is correlated with mental health.
Hypothesis2(H2): Satisfaction plays a mediating role in physical activity and the mental health of young people.
Hypothesis3(H3): Self-rated health plays a mediating role in physical activity and the mental health of young people.
Hypothesis4(H4): Life satisfaction and self-rated health mediated the most in high-frequency physical activity and mental health.
The data used in this paper were from the sample survey data of the “Adolescent Health Theme Database” of the Chinese National Population Health Science Data Centre, obtained to investigate the health status and health-related behaviours of middle and high school students [18]. This is the first publicly available free database on the health and health-related behaviours of Chinese adolescents. For the data used in this paper, high school students were considered as the study population and the relevant data were processed by looking at specific information on all relevant variables; removing outliers for age, physical activity, total SCL-90 score, and control variables; and excluding samples with incomplete answers and missing values, resulting in a valid sample with a size of 3578.
Variables and operational definitions
Mental Health. The dependent variable in this paper is mental health, which is a continuous variable. This variable was derived from the Symptom Check-List-90 of the Chinese version (SCL-90) in the database [19]. The Cronbach coefficient alpha of this scale ranged from 0.78 to 0.90, and there was a high degree of correlation between the nine original sub-scales, with correlation coefficients ranging from 0.39 to 0.79 [20]. Each item was rated on a five-point Likert scale from 1 (not at all) to 5 (very severe). The SCL-90 scale results were processed by adding the individual scores of each of the 90 items in order to obtain the total score, then dividing the total score by 90 to obtain the total mean score (i.e., total mean score = total score/90). The total mean score indicates the reporter’s self-perception as a value between 1 and 5, representing the overall level of mental health with higher values indicating lower levels of mental health among adolescents [19,21].
Frequency of Physical Activity. The independent variable in this paper is the frequency of physical activity, which is a categorical variable. The relevant database question was “Do you participate in physical activity regularly?”, with the answers: “Never” = 1 (never), “Rarely” = 2 (rarely), “Often” = 3 (often), “Always” = 4 (always).
Life Satisfaction and Self-Rated Health. The mediating variables were life satisfaction and self-rated health, dichotomous variables. The relevant question for the former was “Are you satisfied with your life?” and the value assigned to life satisfaction was 1 = unsatisfied or 2 = satisfied. The relevant question for the latter was “Are you satisfied with your health?” and the value assigned to self-rated health was 1 = unsatisfied or 2 = satisfied. Questions about frequency of physical activity, life satisfaction, and self-rated health were taken from the Child and Adolescent Quality of Life Scale. The scale has good reliability with a Cronbach coefficient of 0.885, content validity of 0.63 (p < 0.01), and construct validity of 0.890 (p = 0.00) [22].
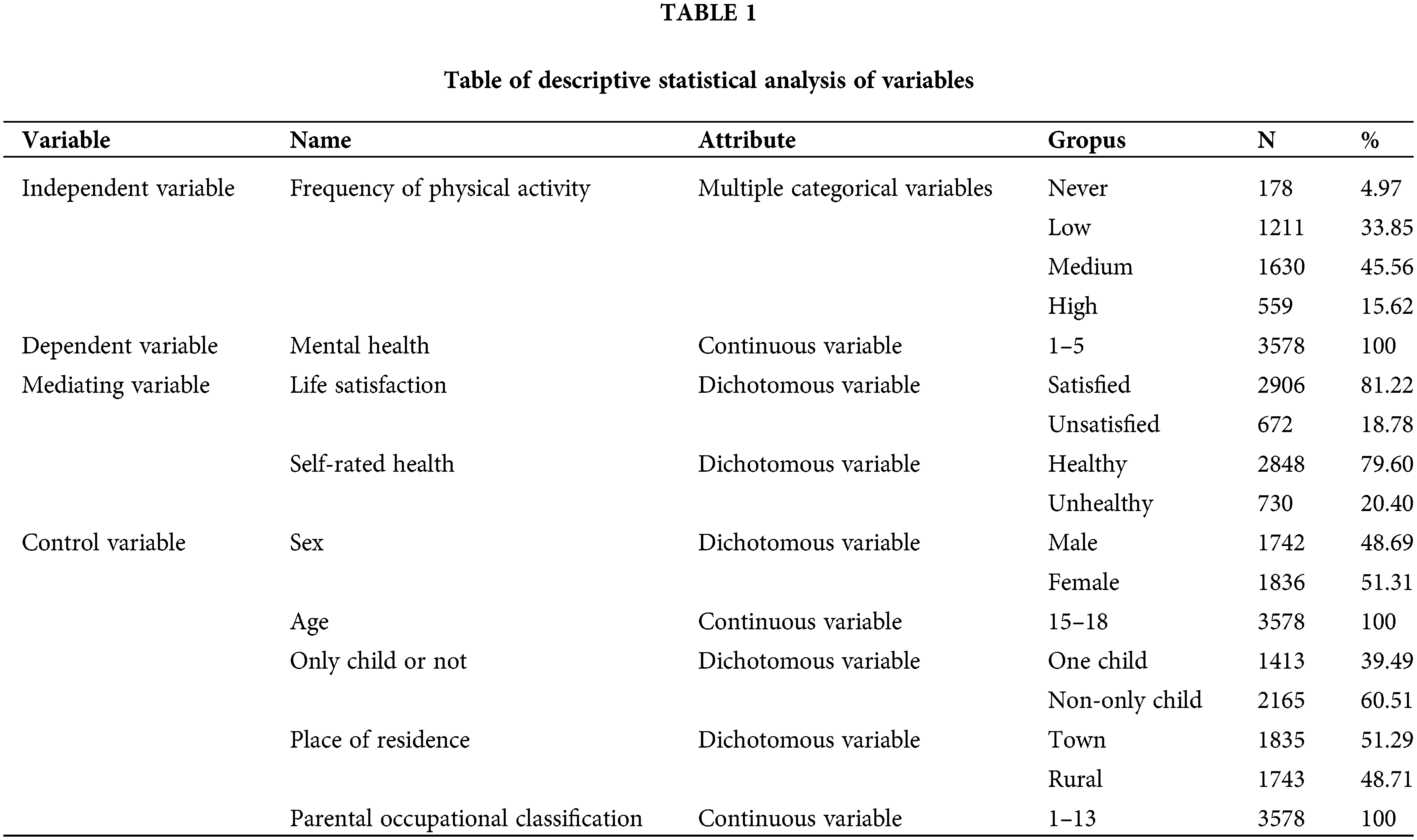
Furthermore, the following were chosen as control variables: Sex, age, whether the child was an only child, place of residence, and parental occupational classification (see Table 1).
(1) A general linear regression model was used to study the relationship of physical activity on the level of mental health in adolescents. The regression model is as follows:
where
(2) The Karlson–Holm–Breen (KHB) model was used to determine whether life satisfaction and self-rated health were significant, and the model also allowed for analysis of the relationship between life satisfaction, self-rated health and mental health levels and the contribution of the indirect effects of the two mediating variables.
The KHB mediation model is a method for estimating mediating effects in regression models. The method estimates the mediating effect by decomposing the total effect into a direct effect and an indirect effect [23]. The following equations are used in the KHB method:
where
Current state of adolescent mental health
The results indicated that the mean value of mental health for adolescents was 1.629. The level of mental health refers to the fact that, in general, the scores of the total symptom index ranged from 1.5 to 2.5, indicating the existence of mild symptoms and a low frequency of symptoms among Chinese adolescents. There were 885 adolescents with a mean SCL-90 total score greater than or equal to 2, meaning that about 24.73% of adolescents had varying degrees of mental health problems.
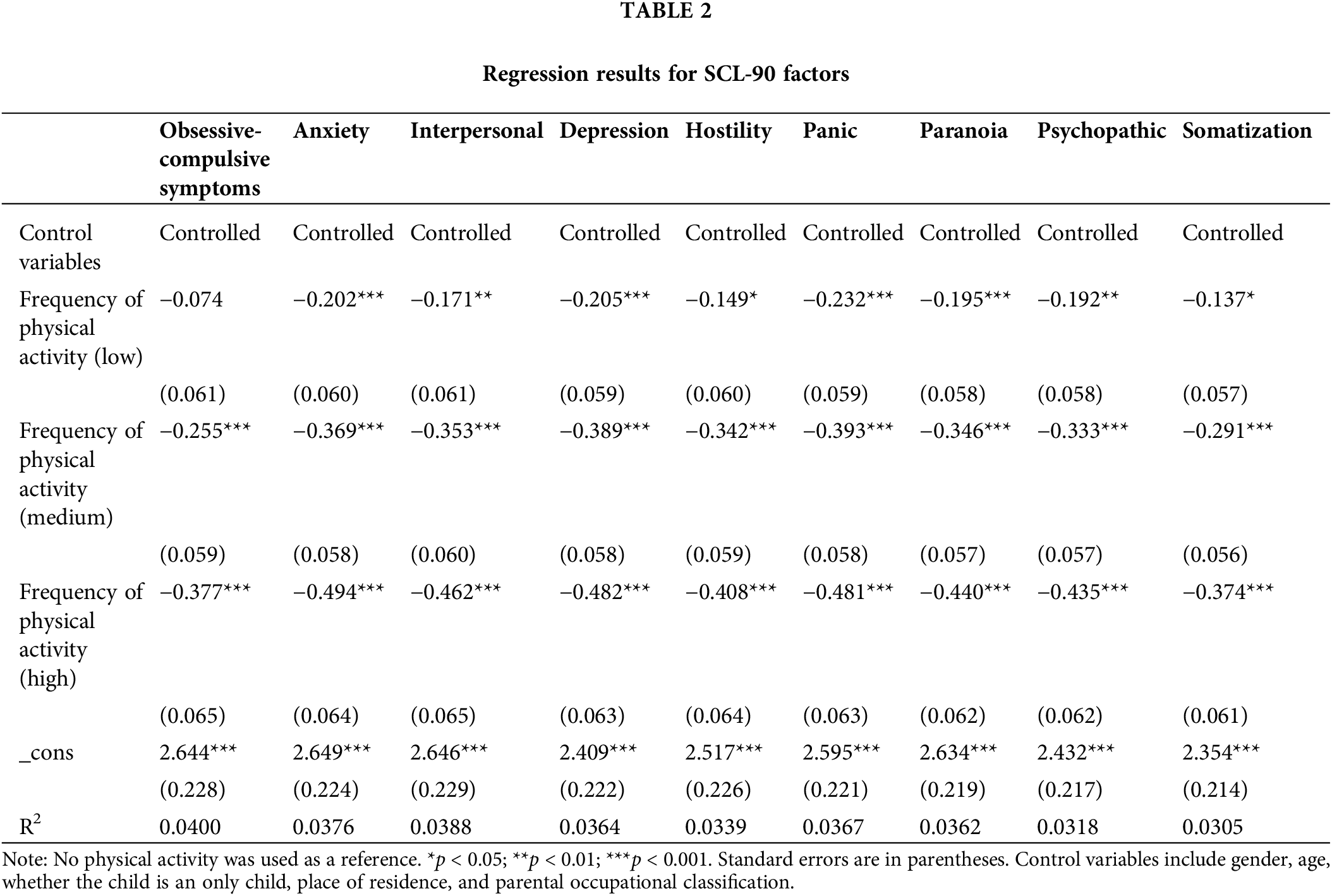
To examine the extent to which different frequencies of physical activity affected each factor of the SCL-90 scale, a general linear regression analysis was conducted between the nine elements and frequency of physical activity after controlling for all variables (Table 2). In these nine models, low-frequency physical activity was not correlated with obsessive–compulsive symptoms, partially correlated with somatization (p < 0.05), and correlated more significantly with interpersonal interactions and psychoticism (p < 0.01). Compared to low-frequency physical activity, medium- and high-frequency physical activity were significantly negatively correlated with each factor (p < 0.001). The more significant the relationship on each element as physical activity frequency increased. Of the nine models, high-frequency physical activity was most significantly correlated with anxiety, and low and medium-frequency physical activity was most significantly correlated with distress.
To analyze the relationship of between physical activity and mental health, a general linear regression was conducted with mental health as the dependent variable, incorporating the control and independent variables (frequency of physical activity) and mediating variables in turn (see Table 3).
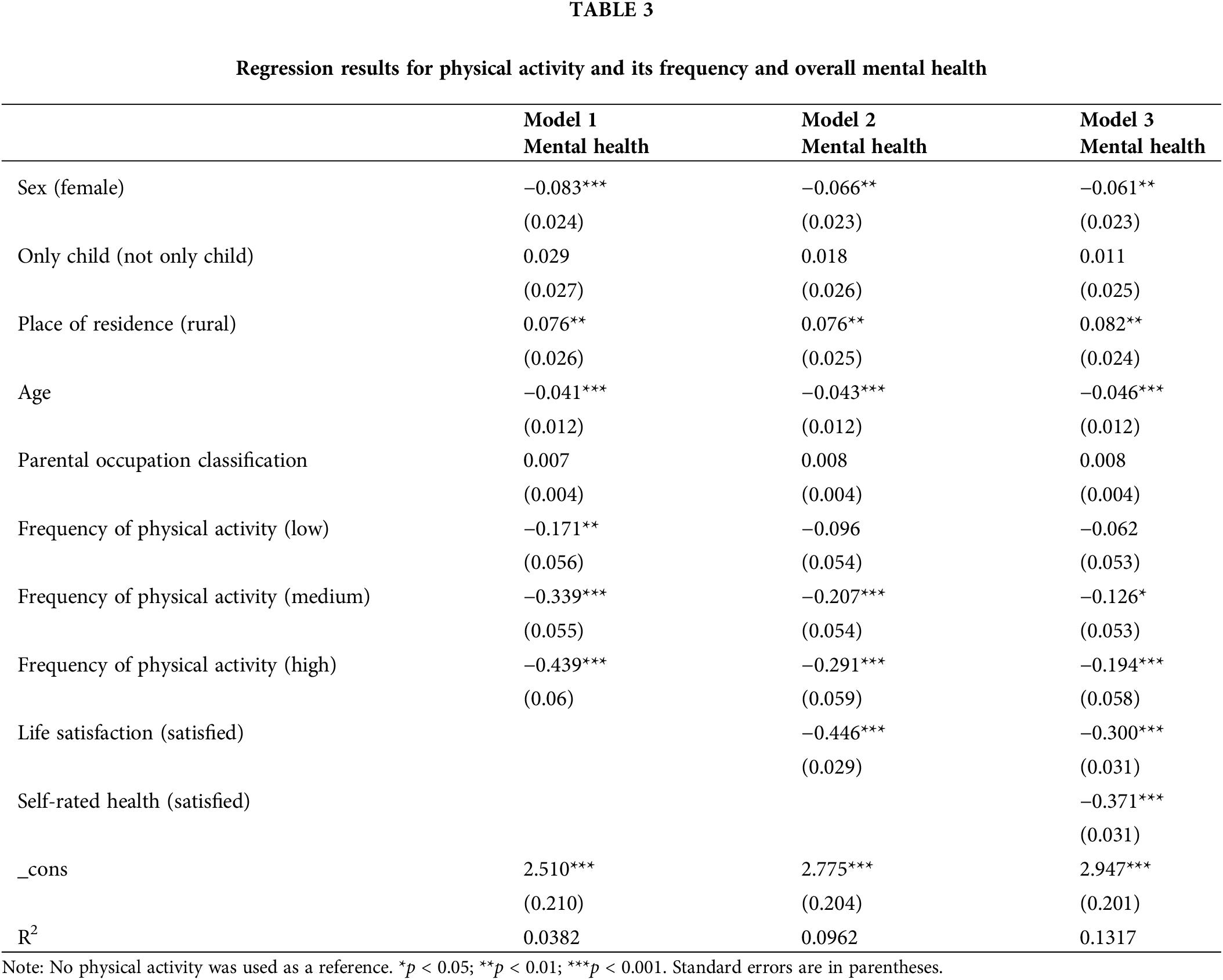
First, the relationship of between physical activity and the level of mental health of adolescents was analyzed. Model 1 in Table 3 considers, with the inclusion of control variables, the effect of physical activity on mental health. The results indicate that the significance of the effect of physical activity on the level of mental health increases gradually as the frequency of physical activity increases (taking never participating in physical activity as the reference group); that is, as the frequency of physical activity increased, the level of mental health increased. The frequency of physical activity increased from low- to medium- and medium- to high-frequency by 0.168 and 0.1 units, respectively, and Hypothesis 1 was verified. The regression results for the control variables demonstrated that age, sex, and place of residence had significant effects on adolescent mental health. Both sex and age had a significant negative association with mental health (p < 0.001), with girls having 0.083 units higher mental health than boys (95% CI: −0.13, −0.04). Adolescent mental health increased by 0.041 units (95% CI: −0.07, −0.018) with increasing age. Rural adolescents had higher mental health, relative to urban adolescents (p < 0.05).
The mediating variables of life satisfaction and self-rated health were added into models 2 and 3. The correlation of physical activity on mental health gradually decreased, and the correlation of low-frequency physical activity on the level of mental health was no longer significant, while medium- and high-frequency physical activity still had significant correlations on the level of mental health. In addition, with the addition of the two mediating variables to model 3 at the same time, there were significant negative correlations (p < 0.001) between life satisfaction and self-rated health with mental health, with coefficients of −0.300 and −0.371, respectively. The regression coefficients of the mediating variables life satisfaction and self-rated health were both significantly negative, and the coefficient of self-rated health was smaller than that of life satisfaction, indicating that life satisfaction and self-rated health had significant contributions to the mental health level, where the contribution of self-rated health on mental health was greater than that of life satisfaction on mental health. From model 1 to model 3, the regression coefficients of low-, medium-, and high-frequency physical activity on mental health decreased from −0.171, −0.339, and −0.439 to −0.062, −0.126, and −0.194, respectively, indicating that the two mediating variables play a mediating role in the effect of physical activity on mental health. Therefore, on the basis of the general linear regression model, the KHB mediation model was utilized for the analysis of mediating effects [24].
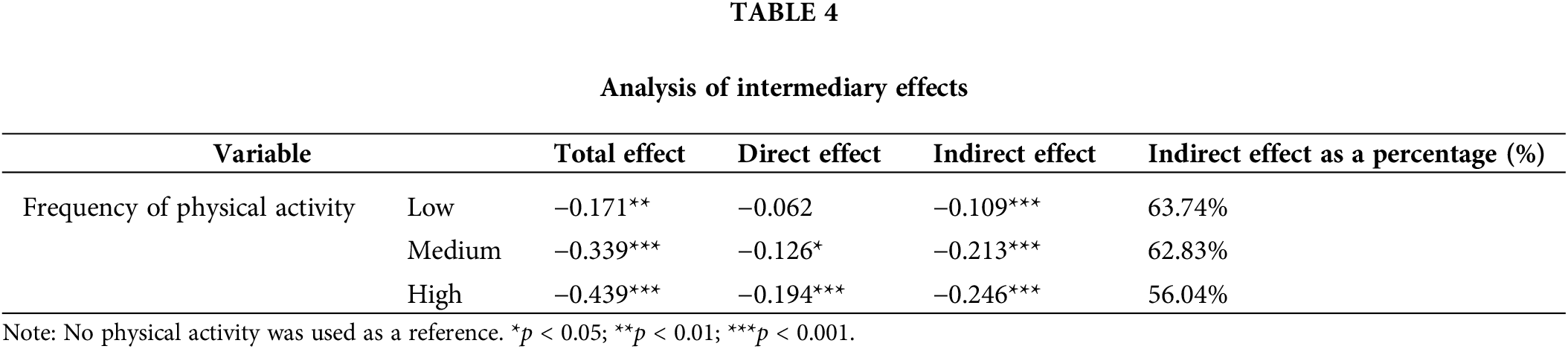
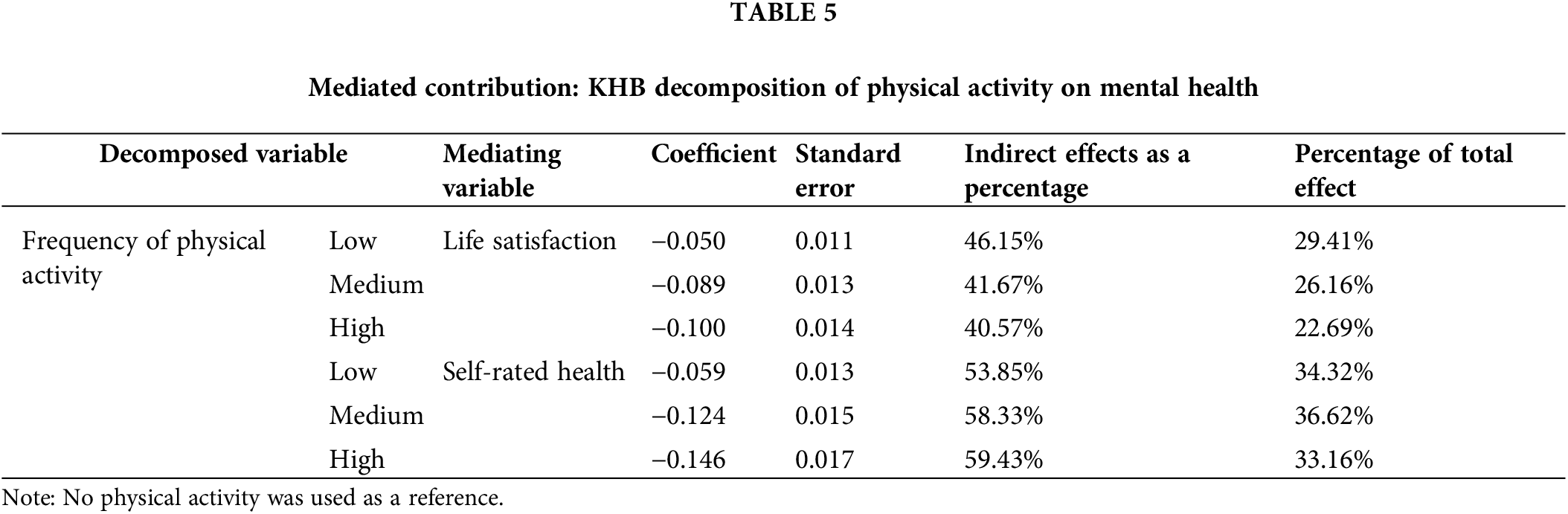
The results of the mediated effects model indicated that the total effect of low-, medium-, and high-frequency physical activity on mental health was −0.171 (p < 0.01), −0.339 (p < 0.001), and −0.439 (p < 0.001), respectively, with mediated effects of −0.109, −0.213, and −0.246 (p < 0.001), respectively (see Table 4). In terms of direct effects, physical activity had a significant direct effect on mental health (p < 0.01). In terms of indirect effects, the indirect effects were negative, indicating partial mediating effects (p < 0.001) for both mediating variables (i.e., life satisfaction and self-rated health). Therefore, physical activity had an indirect positive effect on mental health through increasing life satisfaction and self-rated health and, so, Hypotheses 2 and 3 were verified. Further decomposition of the contributions of life satisfaction and self-rated health revealed that low-, medium-, and high-frequency physical activity acted on mental health through life satisfaction, with mediating effects of 46.15%, 41.67%, and 40.57%, respectively (see Table 5). Low-, medium-, and high-frequency physical activity also acted on mental health through self-rated health, with mediating effects of 53.85%, 58.33%, and 59.43%, respectively. The largest mediating effect for low-frequency physical activity on psychological well-being was through life satisfaction, while the largest mediating effect for high-frequency physical activity on psychological well-being was through self-rated health; therefore, Hypothesis 4 was rejected.
The direct effect of physical activity
In the regression model of the SCL-90 factors, high-frequency physical activity was most significantly correlated with low anxiety, while low and medium-frequency physical activity was most significantly correlated with reduced distress. Adolescents within this age group in China may experience psychological problems due to the excessive burden of college entrance exams, insufficient parental care, stringent discipline, and their own maladaptive habits [25]. Engaging in physical activity is beneficial for adolescents in reducing symptoms such as obsessive-compulsive symptoms and anxiety, fostering a healthy personality, and promoting emotional stability [26]. This substantiates the role of physical activity as an intervention for psychological problems.
It was determined that medium- and high-frequency physical activity were more significantly associated with mental health compared to low-frequency physical activity on mental health. This suggests that physical activity can promote mental health, and escalating the frequency of physical activity can effectively bolster adolescent mental health. Hamer also discovered that varying frequencies of physical activity resulted in distinct degrees of disparities in the mental health of students, demonstrating that mental health improved as the frequency of physical activity increased [27]. Moreover, in another study, the more weekly physical activities that adolescents participated in, the more pronounced the enhancement of their mental health [28]. Physical activity can ameliorate mental health and reduce depression, anxiety, and other negative emotions through physiological, psychological, and inflammatory mechanisms. As physical activity frequency increases, the body continually produces analgesic and euphoric endorphins, which improve adverse moods and modulate the central nervous system. Alternatively, physical activity may disperse negative emotions, augment self-esteem and self-worth, decrease chronic inflammation, and positively influence emotional states, thereby affecting mental health [29]. Consequently, the results of this study reaffirm the existing literature, indicating that adolescent mental health can be improved by augmenting the frequency of physical activity.
Mediating role of life satisfaction and self-rated health
The results of this study demonstrated that adolescent physical activity exerts a positive influence on psychological well-being, with life satisfaction and self-rated health playing significant mediating roles between physical activity and psychological well-being.
An et al. concluded that physical activity among adolescents has a favorable impact on life satisfaction, which is in line with the findings of this study [30]. Some scholars have contended that physical activity not only mitigates psychological symptoms, but also enhances individual well-being and sustains elevated levels of life satisfaction [31]. Others have argued that physical activity bolsters individual life satisfaction by decelerating or restoring one’s physiological functions, enabling the attainment of information and the accomplishment of set goals [32].
The influence of life satisfaction on mental health has been substantiated. Life satisfaction should be regarded as a crucial aspect of positive mental health, as it has exhibited a moderate correlation with other mental health indicators within various populations [33]. Consequently, life satisfaction impacts adolescent mental health. Specifically, life satisfaction is also associated with psychiatric disorders, such as major depression, anxiety disorders, and suicidal tendencies, all of which profoundly affect mental health [34].
Moreover, studies investigating the effects of physical activity on self-rated health have corroborated that higher frequencies of physical activity correspond to improved self-rated health status. It has been observed that a high frequency of physical activity in adolescents is positively associated with self-rated ‘good health’ status, which concurs with the findings of this study [35,36]. An increased frequency of physical activity contributes to enhancing the perceived physical health level in adolescents, thus fostering positive self-rated health status [37].
Self-rated health is significantly correlated with mental disorders and the exacerbation of psychological symptoms [38,39]. Individuals with poor self-rated health tend to experience considerably more psychological distress [40]. Lower self-rated health exerts a negative impact on mental health and may be associated with emotions that emerge during illness. Research has indicated that pain constitutes a negative body-centered emotion, with more significant pain correlating with emotional stress [41,42]. Therefore, the discomfort and pain resulting from physical illness can lead to both a negative evaluation of one’s physical health and corresponding emotions, which can engender a certain degree of stress, subsequently making the connection with mental health.
Comparison of mediating effects
This study discovered that low-frequency physical activity had the most substantial mediating effect on the mental health through life satisfaction. In contrast, the most significant mediating effect of high-frequency physical activity on mental health was through self-rated health. Furthermore, the mediating effects of self-rated health were consistently more significant than those of life satisfaction.
The impacts of varying physical activity frequency on life satisfaction are divergent. Adolescents with increased physical activity frequency and higher participation in active sports experience lower levels of depressive symptoms and higher life satisfaction [43,44]; however, in line with this study’s findings, high-intensity physical activity frequency was not associated with life satisfaction, while low- and moderate-intensity physical activity frequency improved life satisfaction [45]. Similarly, the study of Schmiedeberg did not reveal any increase in life satisfaction with heightened exercise frequency [46].
Differences in life satisfaction levels across physical activity frequencies could be attributed to the relationship between life satisfaction and academics in adolescents [47]. Engagement in academic activities indirectly affects the life satisfaction of students, with positive academic attitudes and involvement effectively promoting their life satisfaction [48]. The lives of Chinese high school students are dominated by studying in a concentrated learning atmosphere. The competitive environment and high expectations can increase pressure on adolescents, affecting their perceived quality of life [49]. Consequently, higher physical activity frequency may detract from time dedicated to studying, socializing, and resting, thus impacting academic performance, interpersonal interactions, and rest quality, subsequently reducing life satisfaction.
Health perception levels in adolescents are influenced by their physical activity engagement. Embodied cognitive theory [50] posits that cognitive processes are deeply rooted in the body–world interaction, and the body’s state directly affects cognitive functions, with physical behavior influencing mental activity and cognitive perception. Increased physical activity frequency leads to positive health perception changes in individuals and promotes better self-rated health outcomes through good exercise behavior. Thus, the level of self-rated health increases with the frequency of physical activity.
Comparing the two mediating variables across physical activity frequencies, the mediating effect of self-rated health was notably higher than that of life satisfaction. Self-rated health pertains to a single health indicator focused on one’s health status and is more individual-centric. The health perceptions of adolescents depend on their physical health status, with health, disability, higher BMI, stress, sleep quality, and poor health behaviors associated with lower self-rated health [16,51]. Consequently, higher physical activity frequency, as positive health behavior, will be directly associated with higher self-rated health. Simultaneously, increased physical activity participation by adolescents decreases the likelihood of engaging in health-risk behaviors and enhances health behaviors, thus improving self-rated health [52]. Physical activity frequency, duration, and intensity are directly related to physiology [53], and physical health will positively contribute to favorable self-rated health evaluations [54]. Therefore, physical activity can be made to drive mental health through self-assessment of health.
Conversely, life satisfaction is a subjective assessment of the overall quality of life [55]. Factors such as the environment, social desirability effects, personality, interpersonal relationships, community, and life events all influence the life satisfaction of adolescents [55,56]. Although physical activity frequency is closely related to life satisfaction, its effect on life satisfaction is relatively small compared to other influencing factors and can be affected by different life aspects. For instance, physical activity frequency is influenced by intrinsic motivation in buffering the adverse effects of stress on life satisfaction in adolescents [57]. As a result, the relationship of physical activity frequency and life satisfaction may be confounded by other factors.
Higher physical activity frequencies—as optimistic, healthy behaviors—were more significantly associated with self-rated health. In contrast, less correlation between the frequency of physical activity and life satisfaction, as life satisfaction is more profoundly and complexly affected by other individuals or the external environment. Therefore, the mediating effect of self-rated health was found to be higher than that of life satisfaction.
This study offers valuable insights into the effects of physical activity frequency on adolescents’ mental health, as well as the mediating roles of life satisfaction and self-rated health. The main findings were as follows: (1) Physical activity was significantly correlated with mental health in adolescents, mental health levels increase with frequency of physical activity, and (2) Life satisfaction and self-rated health played significant mediating roles in the relationship between physical activity frequency and mental health. Specifically, low-frequency physical activity has the most pronounced mediating effect on mental health through life satisfaction, while high-frequency physical activity exerts the most significant mediating effect on mental health through.
Despite the valuable contributions of this study, there are some limitations to consider. First, the use of the SCL-90 scale, which reflects mental health status over one week, may not fully capture the long-term effects of physical activity frequency on mental health. Future research could employ longitudinal designs to better understand the causal relationships between physical activity frequency, life satisfaction, self-rated health, and mental health over time.
Second, the sample consists of Chinese high school students, which limits the generalizability of the findings to other cultural contexts and age groups. Future studies could examine the relationships of interest in diverse populations, considering factors such as cultural differences, socio-economic status, and age.
Third, the present study only focuses on the mediating roles of life satisfaction and self-rated health. There may be other potential mediators, such as social connectedness, academic performance, and sleep quality, which could be explored in future research to provide a more comprehensive understanding of the relationship between physical activity frequency and mental health.
Lastly, the study relies on self-reported measures, which may be subject to reporting biases. Future research could incorporate objective assessments of physical activity and mental health, as well as qualitative data, to gain a richer understanding of the phenomena under investigation.
Acknowledgement: The authors thank research participants for their participation in this study.
Funding Statement: The authors received no specific funding for this study.
Author Contributions: The authors confirm contribution to the paper as follows: study conception and design: W.L., X.L.; data collection: Y.G., G.L.; analysis and interpretation of results: W.L., R.H., M.Z.; draft manuscript preparation: W.L., Y.G. All authors reviewed the results and approved the final version of the manuscript.
Availability of Data and Materials: 10.12213/11.a0031.202107.209.v1.0.
Ethics Approval: Not applicable.
Conflicts of Interest: The authors declare that they have no conflicts of interest to report regarding the present study.
References
1. World Health Organization. Adolescent mental health. Available from: https://wwwwhoint/news-room/fact-sheets/detail/adolescent-mental-health. [Accessed 2008]. [Google Scholar]
2. Kim-Cohen J, Caspi A, Moffitt TE, Harrington H, Milne BJ, Poulton R. Prior juvenile diagnoses in adults with mental disorder: developmental follow-back of a prospective-longitudinal cohort. Arch Gen Psychiatry. 2003;60(7):709–17. doi:10.1001/archpsyc.60.7.709. [Google Scholar] [PubMed] [CrossRef]
3. Prince M, Patel V, Saxena S, Maj M, Maselko J, Phillips MR, et al. No health without mental health. The Lancet. 2007;370(9590):859–77. doi:10.1016/S0140-6736(07)61238-0. [Google Scholar] [PubMed] [CrossRef]
4. Taylor CB, Sallis JF, Needle R. The relation of physical activity and exercise to mental health. Public Health Rep. 1985;100:195. doi:10.2307/20056436. [Google Scholar] [CrossRef]
5. O’Connor PJ, Raglin JS, Martinsen EW. Physical activity, anxiety and anxiety disorders. Int J Sport Psychol. 2000;31:136–55. [Google Scholar]
6. Ai X, Yang J, Lin Z, Wan X. Mental health and the role of physical activity during the COVID-19 pandemic. Front Psychol. 2021;12:759987. doi:10.3389/fpsyg.2021.759987. [Google Scholar] [PubMed] [CrossRef]
7. Stubbs B, Koyanagi A, Hallgren M, Firth J, Richards J, Schuch F, et al. Physical activity and anxiety: a perspective from the World Health Survey. J Affect Disord. 2017;208:545–52. doi:10.1016/j.jad.2016.10.028. [Google Scholar] [PubMed] [CrossRef]
8. Syed NK, Alqahtani SS, Meraya AM, Elnaem MH, Albarraq AA, Syed MH, et al. Psychological impact of COVID-19 restrictions among individuals at risk of exercise addiction and their socio-demographic correlates: a Saudi Arabian survey study. Curr Psychol. 2022;1–16. doi:10.1007/s12144-022-02892-8. [Google Scholar] [PubMed] [CrossRef]
9. Valois RF, Zullig KJ, Huebner ES, Drane JW. Physical activity behaviors and perceived life satisfaction among public high school adolescents. J School Health. 2004;74(2):59–65. doi:10.1111/j.1746-1561.2004.tb04201.x. [Google Scholar] [PubMed] [CrossRef]
10. Diener E, Inglehart R, Tay L. Theory and validity of life satisfaction scales. Soc Indic Res. 2013;112(3):497–527. doi:10.1007/s11205-012-0076-y. [Google Scholar] [CrossRef]
11. Kjell O, Daukantaitė D, Hefferon K, Sikström S. The harmony in life scale complements the satisfaction with life scale: expanding the conceptualization of the cognitive component of subjective well-being. Soc Indic Res. 2016;126(2):893–919. doi:10.1007/s11205-015-0903-z. [Google Scholar] [CrossRef]
12. Pavot W, Diener E. The satisfaction with life scale and the emerging construct of life satisfaction. J Posit Psychol. 2008;3(2):137–52. doi:10.1080/17439760701756946. [Google Scholar] [CrossRef]
13. Feng B, Xu K, Zhou P. Association between vigorous physical activity and life satisfaction in adolescents. Front Public Health. 2022;10:944620. doi:10.3389/fpubh.2022.944620. [Google Scholar] [PubMed] [CrossRef]
14. Zhang T, Lu G, Wu XY. Associations between physical activity, sedentary behaviour and self-rated health among the general population of children and adolescents: a systematic review and meta-analysis. BMC Public Health. 2020;20(1):1–16. doi:10.1186/s12889-020-09447-1. [Google Scholar] [PubMed] [CrossRef]
15. Jylhä M. What is self-rated health and why does it predict mortality? Towards a unified conceptual model. Soc Sci Med. 2009;69(3):307–16. doi:10.1016/j.socscimed.2009.05.013. [Google Scholar] [PubMed] [CrossRef]
16. Vingilis ER, Wade TJ, Seeley JS. Predictors of adolescent self-rated health: analysis of the National Population Health Survey. Can J Public Health. 2002;93(3):193–7. doi:10.1007/BF03404999. [Google Scholar] [PubMed] [CrossRef]
17. Wang M, Deng L, Feng Y, Lou Y, Liu J, Huang Y. Mediating effects of adolescent physical activity, self-rated health and family income. Front Public Health. 2022;940141. doi:10.3389/fpubh.2022.940141. [Google Scholar] [PubMed] [CrossRef]
18. Shandong University. Adolescent health subject database. National Population Health Science Data Center Data Warehousing PHDA. 2021. doi:10.12213/11.a0031.202107.209.v1.0. [Google Scholar] [CrossRef]
19. Wang Z. Symptom self-rating scale (SCL-90). Shanghai Arch Psychiatry. 1984;2:68–70. [Google Scholar]
20. Feng Z, Zhang D. Study on the validity of the symptom check-list-90 of Chinese version. J Third Mil Med Univ. 2001;(4):481–83. [Google Scholar]
21. Tian F, Li H, Tian S, Yang J, Shao J, Tian C. Psychological symptoms of ordinary Chinese citizens based on SCL-90 during the level I emergency response to COVID-19. Psychiat Res. 2020;288:112992. doi:10.1016/j.psychres.2020.112992. [Google Scholar] [PubMed] [CrossRef]
22. Dong X, Ding M, Chen W, Liu Z, Yi X. Relationship between smoking, physical activity, screen time, and quality of life among adolescents. Int J Env Res Pub He. 2020;17:8043. doi:10.3390/ijerph17218043. [Google Scholar] [PubMed] [CrossRef]
23. Kohler U, Karlson KB, Holm A. Comparing coefficients of nested nonlinear probability models. Stata J. 2011;11(3):420–38. doi:10.1177/1536867X1101100306. [Google Scholar] [CrossRef]
24. Breen R, Bernt Karlson K, Holm A. A note on a reformulation of the KHB method. Sociol Method Res. 2021;50(2):901–12. doi:10.1177/0049124118789717. [Google Scholar] [CrossRef]
25. Wu KD, Clark LA, Watson D. Relations between obsessive-compulsive disorder and personality: beyond Axis I–Axis II comorbidity. J Anxiety Disord. 2006;20(6):695–717. doi:10.1016/j.janxdis.2005.11.001. [Google Scholar] [PubMed] [CrossRef]
26. Abrantes AM, Farris SG, Brown RA, Greenberg BD, Strong DR, McLaughlin NC, et al. Acute effects of aerobic exercise on negative affect and obsessions and compulsions in individuals with obsessive-compulsive disorder. J Affect Disorders. 2019;245(1):991–7. doi:10.1016/j.jad.2018.11.074. [Google Scholar] [PubMed] [CrossRef]
27. Hamer M, Stamatakis E, Steptoe A. Dose-response relationship between physical activity and mental health: the Scottish Health Survey. Brit J Sport Med. 2009;43(14):1111–4. doi:10.1136/bjsm.2008.046243. [Google Scholar] [PubMed] [CrossRef]
28. Grasdalsmoen M, Eriksen HR, Lønning KJ, Sivertsen B. Physical exercise, mental health problems, and suicide attempts in university students. BMC Psychiatry. 2020;20(1):1–11. doi:10.1186/s12888-020-02583-3. [Google Scholar] [PubMed] [CrossRef]
29. Mikkelsen K, Stojanovska L, Polenakovic M, Bosevski M, Apostolopoulos V. Exercise and mental health. Maturitas. 2017;106(4):48–56. doi:10.1016/j.maturitas.2017.09.003. [Google Scholar] [PubMed] [CrossRef]
30. An HY, Chen W, Wang CW, Yang HF, Huang WT, Fan SY. The relationships between physical activity and life satisfaction and happiness among young, middle-aged, and older adults. Int J Env Res Pub He. 2020;17:4817. doi:10.3390/ijerph17134817. [Google Scholar] [PubMed] [CrossRef]
31. Zhang Y, Ren M, Zou S. Effect of physical exercise on college students’ life satisfaction: mediating role of competence and relatedness needs. Front Psychol. 2022;930253. doi:10.3389/fpsyg.2022.930253. [Google Scholar] [PubMed] [CrossRef]
32. Jenaabadi H. Examining the relationship of self-knowledge with quality of work life and mental health of high school managers in Nimrouz. ADV Physiol Educ. 2015;5(3):211–24. doi:10.4236/ape.2015.53026. [Google Scholar] [CrossRef]
33. Bray I, Gunnell D. Suicide rates, life satisfaction and happiness as markers for population mental health. Soc Psych Psych Epid. 2006;41(5):333–7. doi:10.1007/s00127-006-0049-z. [Google Scholar] [PubMed] [CrossRef]
34. Fergusson DM, McLeod G, Horwood LJ, Swain NR, Chapple S, Poulton R. Life satisfaction and mental health problems (18 to 35 years). Psychol Med. 2015;45(11):2427–36. doi:10.1017/S0033291715000422. [Google Scholar] [PubMed] [CrossRef]
35. Granger E, Williams G, Di Nardo F, Harrison A, Verma A. The relationship between physical activity and self-rated health status in European adolescents: results of the EURO-URHIS 2 survey. Eur J Public Health. 2017;27(suppl_2):107–11. doi:10.1093/eurpub/ckw177. [Google Scholar] [PubMed] [CrossRef]
36. Pierannunzio D, Spinelli A, Berchialla P, Borraccino A, Charrier L, Dalmasso P, et al. Physical activity among Italian adolescents: association with life satisfaction, self-rated health and peer relationships. Int J Env Res Pub He. 2022;19:4799. doi:10.3390/ijerph19084799. [Google Scholar] [PubMed] [CrossRef]
37. Marques A, Mota J, Gaspar T, de Matos MG. Associations between self-reported fitness and self-rated health, life-satisfaction and health-related quality of life among adolescents. J Exerc Sci Fit. 2017;15(1):8–11. doi:10.1016/j.jesf.2017.03.001. [Google Scholar] [PubMed] [CrossRef]
38. Spitzer RL, Kroenke K, Linzer M, Hahn SR, Williams JB, Degruy FV, et al. Health-related quality of life in primary care patients with mental disorders: results from the PRIME-MD, 1000 Study. JAMA. 1995;274(19):1511–7. doi:10.1001/jama.1995.03530190025030. [Google Scholar] [CrossRef]
39. Mulsant BH, Ganguli M, Seaberg EC. The relationship between self-rated health and depressive symptoms in an epidemiological sample of community-dwelling older adults. J Am Geriatr Soc. 1997;45(8):954–8. doi:10.1111/j.1532-5415.1997.tb02966.x. [Google Scholar] [PubMed] [CrossRef]
40. Cano A, Scaturo DJ, Sprafkin RP, Lantinga LJ, Fiese BH, Brand F. Family support, self-rated health, and psychological distress. Prim Care Companion J Clin Psychiatry. 2003;5(3):111. doi:10.4088/PCC.v05n0302. [Google Scholar] [PubMed] [CrossRef]
41. Chapman CR, Gavrin J. Suffering and its relationship to pain. J Palliat Care. 1993;9(2):5–13. doi:10.1177/082585979300900202. [Google Scholar] [CrossRef]
42. Lumley MA, Cohen JL, Borszcz GS, Cano A, Radcliffe AM, Porter LS, et al. Pain and emotion: a biopsychosocial review of recent research. J Clin Psychol. 2011;67(9):942–68. doi:10.1002/jclp.20816. [Google Scholar] [PubMed] [CrossRef]
43. Dolan P, Kavetsos G, Vlaev I. The happiness workout. Soc Indic Res. 2014;119(3):1363–77. doi:10.1007/s11205-013-0543-0. [Google Scholar] [CrossRef]
44. Piko BF, Keresztes N. Physical activity, psychosocial health and life goals among youth. J Commun Health. 2006;31(2):136–45. doi:10.1007/s10900-005-9004-2. [Google Scholar] [PubMed] [CrossRef]
45. Panza GA, Taylor BA, Thompson PD, White CM, Pescatello LS. Physical activity intensity and subjective well-being in healthy adults. J Health Psychol. 2019;24(9):1257–67. doi:10.1177/1359105317691589. [Google Scholar] [PubMed] [CrossRef]
46. Schmiedeberg C, Schröder J. Leisure activities and life satisfaction: an analysis with German panel data. Appl Res Qual Life. 2017;12(1):137–51. doi:10.1007/s11482-016-9458-7. [Google Scholar] [CrossRef]
47. Leung CYW, McBrideChang C, Lai BPY. Relations among maternal parenting style, academic competence, and life satisfaction in Chinese early adolescents. J Early Adolesc. 2004;24(2):113–43. doi:10.1177/0272431603262678. [Google Scholar] [CrossRef]
48. Hakimzadeh R, Besharat MA, Khaleghinezhad SA, Ghorban Jahromi R. Peers’ perceived support, student engagement in academic activities and life satisfaction: a structural equation modeling approach. School Psychol Int. 2016;37(3):240–54. doi:10.1177/0143034316630020. [Google Scholar] [CrossRef]
49. Shek DT, Liu TT. Life satisfaction in junior secondary school students in Hong Kong: a 3-year longitudinal study. Soc Indic Res. 2014;117(3):777–94. doi:10.1007/s11205-013-0398-4. [Google Scholar] [CrossRef]
50. Wilson M. Six views of embodied cognition. Psychon B Rev. 2002;9(4):625–36. doi:10.3758/BF03196322. [Google Scholar] [PubMed] [CrossRef]
51. Lee J. Mediating effect of sleep satisfaction on the relationship between stress and self-rated health among Korean adolescents: a nationwide cross-sectional study. Child Youth Serv Rev. 2020;109(6):104717. doi:10.1016/j.childyouth.2019.104717. [Google Scholar] [CrossRef]
52. Delisle TT, Werch CE, Wong AH, Bian H, Weiler R. Relationship between frequency and intensity of physical activity and health behaviors of adolescents. J School Health. 2010;80(3):134–40. doi:10.1111/j.1746-1561.2009.00477.x. [Google Scholar] [PubMed] [CrossRef]
53. Pate RR, Pratt M, Blair SN, Haskell WL, Macera CA, Bouchard C, et al. Physical activity and public health: a recommendation from the centers for disease control and prevention and the American college of sports medicine. JAMA. 1995;273(5):402–7. doi:10.1001/jama.1995.03520290054029. [Google Scholar] [CrossRef]
54. Ocampo JM. Self-rated health: importance of use in elderly adults. Colomb Medica. 2010;41(3):275–89. doi:10.25100/cm.v41i3.715. [Google Scholar] [CrossRef]
55. Proctor CL, Linley PA, Maltby J. Youth life satisfaction: a review of the literature. J Happiness Stud. 2009;10(5):583–630. doi:10.1007/s10902-008-9110-9. [Google Scholar] [CrossRef]
56. Neto F. Satisfaction with life among adolescents from immigrant families in Portugal. J Youth Adolescence. 2001;30(1):53–67. doi:10.1023/A:1005272805052. [Google Scholar] [CrossRef]
57. Meyer S, Grob A, Gerber M. No fun, no gain: the stress-buffering effect of physical activity on life satisfaction depends on adolescents’ intrinsic motivatio. Psychol Sport Exerc. 2021;56(157):102004. doi:10.1016/j.psychsport.2021.102004. [Google Scholar] [CrossRef]
Cite This Article
 Copyright © 2024 The Author(s). Published by Tech Science Press.
Copyright © 2024 The Author(s). Published by Tech Science Press.This work is licensed under a Creative Commons Attribution 4.0 International License , which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
 Downloads
Downloads
 Citation Tools
Citation Tools