
 Submit a Paper
Submit a Paper Propose a Special lssue
Propose a Special lssue Open Access
Open Access
ARTICLE
Is Meeting 24-Hour Movement Guidelines Associated with Emotion Regulation among Children and Adolescents?
1 Department of Sports Science, College of Education, Zhejiang University, Hangzhou, 310058, China
2 Lab for Digital Sports and Health, College of Education, Zhejiang University, Hangzhou, 310058, China
* Corresponding Author: Liang Hu. Email:
(This article belongs to the Special Issue: Healthy Lifestyle Behaviours and Mental Health in Children and Adolescents)
International Journal of Mental Health Promotion 2025, 27(6), 771-785. https://doi.org/10.32604/ijmhp.2025.064984
Received 28 February 2025; Accepted 13 May 2025; Issue published 30 June 2025
 View Full Text
View Full Text Download PDF
Download PDFAbstract
Background: The Canadian 24-h movement guidelines (24-HMG) emphasize the holistic consideration of physical activity (PA), sedentary behavior, and sleep in shaping health outcomes. This study aimed to examine the associations between meeting 24-HMG and emotion regulation-related indicators among children and adolescents. Methods: A total of 534 Chinese children and adolescents aged 12.94 ± 1.10 years (49.81% males) participated in this study and completed self-report measures assessing 24-h movement behaviors, emotion regulation strategies, emotion regulation flexibility, and regulatory emotional self-efficacy. Results: Only 7.12% of the participants adhered to two or all three guidelines. The number of guidelines met was positively associated with the use of emotion regulation strategies, emotion regulation flexibility, and regulatory emotional self-efficacy. Compared with meeting none of the guidelines, participants who met one or more guidelines reported significantly better performance in these outcomes. Conclusion: Meeting 24-HMG was associated with superior emotion regulation in children and adolescents. The importance of engaging in regular PA, limiting recreational screen time, and getting enough sleep should be highlighted for fostering emotion regulation in this demographic.Keywords
Children and adolescents’ mental health has long been a focus of social concern. During this developmental stage—marked by continual physical and psychological transitions, and compounded by increasing pressures and conflicts—the prevalence of mental health issues continues to rise. Evidence suggests a significant decline in the emotional well-being among children and adolescents since the early 21st century [1], coinciding with a notable rise in depression, non-suicidal self-injury, and even suicide [2–4]. In navigating these challenges, timely and effective emotion regulation emerges as a pivotal factor. Enhancing positive emotions and mitigating negative emotions through emotion regulation are paramount for the psychological well-being and long-term development of children and adolescents.
Emotion regulation is the process through which individuals exert influence over which emotions they have, when they have them, and how they experience and express these emotions [5]. This process primarily involves the selection and use of emotion regulation strategies. Among these strategies, cognitive reappraisal and expressive suppression are the most common and valuable [6]. Cognitive reappraisal involves changing one’s interpretations or appraisals of affective stimuli, which is a form of antecedent-focused emotion regulation; expressive suppression is characterized by inhibiting emotion-expressive behavior while emotionally aroused, which is a form of response-focused emotion regulation [6]. Empirical studies have demonstrated that cognitive reappraisal is positively associated with the reduction of negative emotional experiences, and the enhancement of positive emotions and overall well-being [7,8]. Expressive suppression can regulate negative emotions as well, but its impact may be relatively weaker compared with cognitive reappraisal [6].
The effectiveness of emotion regulation is contingent not only upon the use of emotion regulation strategies, but also upon the context; it depends on the alignment of strategies with the situational demands [9]. Such emphasis on adaptability is reflected in the concept of emotion regulation flexibility, which refers to one’s ability to flexibly deploy emotion regulation strategies in response to changing situations [10]. It encompasses reappraisal flexibility, where individuals flexibly change their interpretation and evaluation of emotional stimuli from multiple perspectives (such as holistic perspective, long-term perspective), and expressive flexibility, which reflects the flexibility of individuals to adjust their emotional expression [11]. Prior research has indicated that individuals with high emotion regulation flexibility are better able to manage negative affect and cope with stress [12,13].
Another important indicator of emotion regulation is regulatory emotional self-efficacy, which generally includes self-efficacy in expressing positive emotions, regulating despondency/distress emotions, and regulating anger/irritation emotions [14]. Individual differences in effectively managing daily emotional experiences stem not only from variations in regulation skills but also from differing beliefs about one’s ability to regulate emotions [14]. These beliefs can influence the effectiveness of emotion regulation [15] and, at the same time, influence the individual’s emotional performance. Studies have shown that regulatory emotional self-efficacy contributes to facilitating positive emotional experiences, lowering levels of depression, and fostering positive expectations for the future [16,17].
Overall, the use of emotion regulation strategies, greater emotion regulation flexibility, and higher regulatory emotional self-efficacy are all conducive to emotional and psychological well-being [7,12,16]. Nonetheless, there is a scarcity of research exploring factors that could positively influence these emotion regulation-related indicators, especially among children and adolescents. This knowledge gap hinders endeavors aimed at enhancing their abilities to effectively regulate emotions. Consequently, investigations into the modifiable determinants of emotion regulation-related indicators among children and adolescents are urgently required.
Several studies have shown associations between daily movement behaviors and emotion regulation indicators. For instance, evidence suggests that physical activity (PA) is positively associated with cognitive reappraisal and negatively associated with expressive suppression [18]. Sleep deprivation is negatively associated with regulatory emotional self-efficacy [19] and may also impair cognitive reappraisal ability [20]. These movement behaviors likely exert influence on emotion regulation through biological, psychological, and social pathways. From a biological perspective, PA can promote neural plasticity in the prefrontal cortex, which is an area critical for executive functions and emotional regulation [21]. Similarly, sleep is beneficial for the perception of emotional stimuli and the processing of automatic responses by increasing neurological activity [22]. From psychological and cognitive perspectives, PA can enhance self-efficacy, which in turn boosts confidence in emotion regulation [23], while screen-based sedentary behavior may impair cognitive flexibility [24], hindering the use of adaptive strategies such as cognitive reappraisal. From a social perspective, engaging in team sports or family PA can provide social support and strengthen interpersonal connections, offering additional emotion regulatory benefits [25]. Taken together, these multidimensional pathways highlight the critical roles of maintaining healthy movement behaviors for effective emotion regulation.
Traditionally, these movement behaviors were studied separately. However, researchers now recognize the interdependence of daily movement behaviors and advocate that their influence on health outcomes should be considered concurrently. This shift led to the Canadian 24-h movement guidelines (24-HMG) for children and adolescents, which recommend at least 60 min of moderate to vigorous PA (MVPA) per day, no more than 2 h of recreational screen time (RST) per day, and 9–11 h of sleep for children aged 5–13 years or 8–10 h for adolescents aged 14–17 years to maintain well-being [26]. Since then, numerous studies have indicated that following 24-HMG offers significant benefits for children and adolescents, such as better body composition, decreased depression and anxiety, and greater global cognition [27–29].
Clearly, improving adherence to 24-HMG has the potential to gain physical, mental, and cognitive health benefits. However, to the best of our knowledge, there are no published studies investigating the relationships between meeting 24-HMG and emotion regulation-related indicators in children and adolescents. Expanding our knowledge in this direction is important to enhance individuals’ capacities to effectively manage daily emotions, thereby fostering emotional well-being. Therefore, this study aimed to examine the associations between meeting 24-HMG and emotion regulation indicators (i.e., the use of emotion regulation strategies, emotion regulation flexibility, and regulatory emotional self-efficacy) among children and adolescents. We hypothesized that meeting 24-HMG would be positively associated with increased use of emotion regulation strategies, elevated levels of emotion regulation flexibility, and enhanced regulatory emotional self-efficacy.
2.1 Participants and Procedure
This cross-sectional study was conducted in two schools (one primary school and one middle school) in Guangdong Province, China. To minimize selection bias, all classes in Grades 5 to 8 were invited to participate. The process of questionnaire collection was supervised by schoolteachers who had been trained in standardized questionnaire administration procedures (e.g., questionnaire explanation and test instruction). Participants were informed that their participation was voluntary, anonymous, and confidential, and they could quit the assessment whenever they wanted. Informed consent was obtained from both the participants and their guardians. The Medical Ethics Committee of the Department of Psychological and Behavioral Sciences at Zhejiang University approved this research (No. [2021]052). All participants in this study signed the informed consent form.
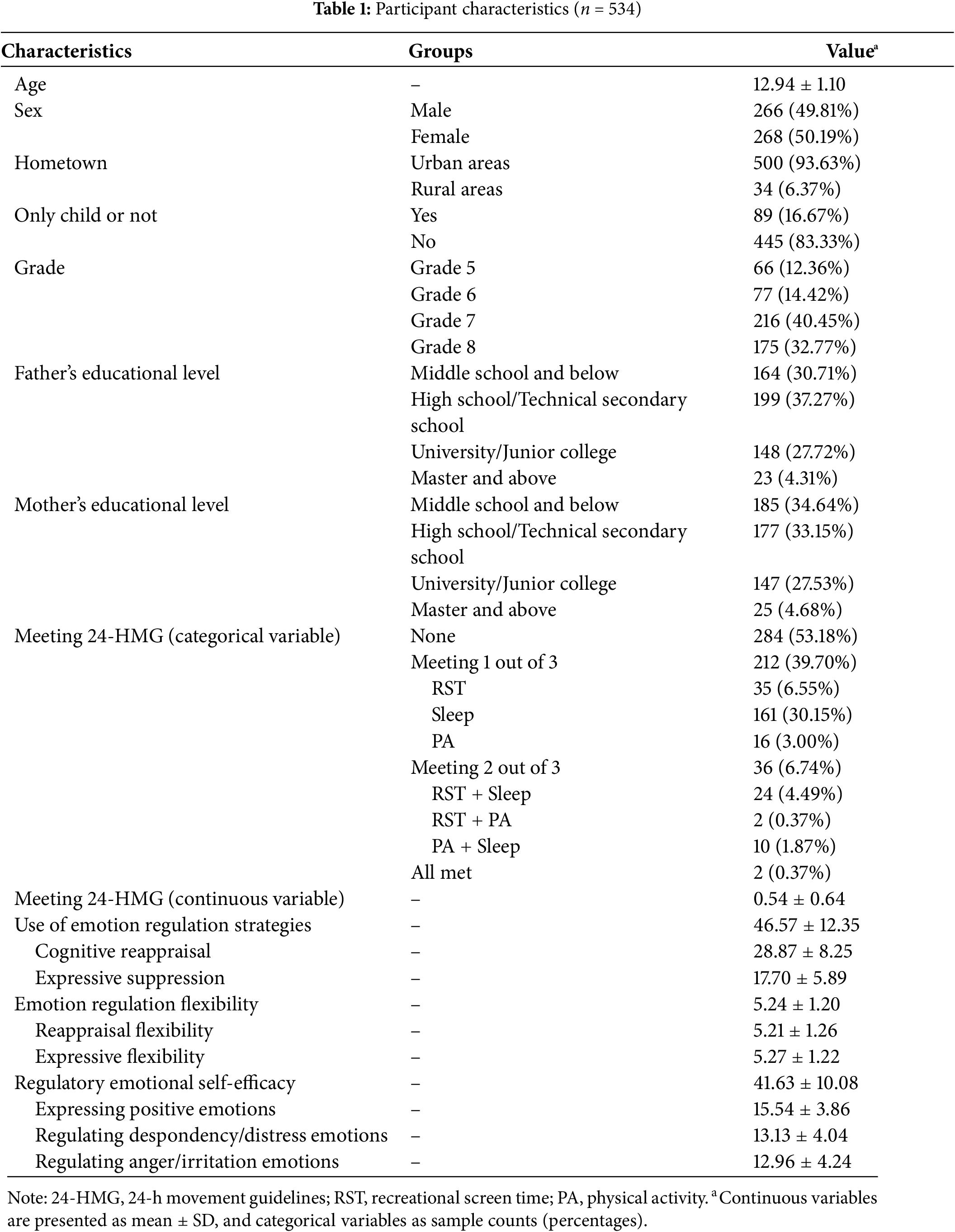
Initially, 580 students were recruited for the study. After excluding those who did not complete the questionnaires, a total of 534 students were included in the final statistical analysis. The demographic information of these participants is presented in Table 1.
2.2 Variables and Measurements
Meeting 24-HMG was handled in terms of continuous variable (the number of guidelines met, ranging from 0 to 3) and categorical variable (different combinations of guidelines met). The combinations included: (a) meeting 1 out of 3 guidelines (PA only, RST only, sleep only); (b) meeting 2 out of 3 guidelines (PA + RST, PA + sleep, or RST + sleep); (c) meeting all guidelines simultaneously.
The 3 components (PA, RST, and sleep) of 24-HMG were assessed using 3 single-item questions. PA was measured by the question, “How many days per week did you participate in MVPA for at least 60 min?”. In accordance with guidelines recommending a minimum of 60 min of MVPA per day, participants who reported engaging in MVPA for 7 days per week were coded as 1, while others were coded as 0. RST was assessed by the question, “How many days per week did you engage in screen-based entertainment (such as watching TV, playing games, or chatting online) for more than 2 h?”. Consistent with guidelines recommending no more than 2 h of RST per day, participants responding with “0 days per week” were coded as 1, while others were coded as 0. Sleep duration was assessed by asking participants about their wake-up and bedtime routines on weekdays and weekends over the past month. The average daily sleep duration was then computed. Based on the guidelines recommending 9–11 h of sleep for children and 8–10 h for adolescents, participants who met the recommended sleep duration were coded as 1, while those who did not were coded as 0.
2.2.2 Emotion Regulation-Related Indicators
Emotion regulation strategies were measured using the Emotional Regulation Questionnaire, which consists of 10 items, with 6 items measuring cognitive reappraisal and 4 items measuring expressive suppression [8]. Participants responded on a 7-point Likert scale ranging from 1 (completely disagree) to 7 (completely agree). Higher scores indicated a higher frequency of using cognitive reappraisal or expressive suppression strategies. The scores of the two subscales were summed to represent the overall use of emotion regulation strategies. The Chinese version has satisfactory reliability and validity [30]. In this study, Cronbach’s α for the total scale, cognitive reappraisal subscale, and expressive suppression subscale were 0.886, 0.898, and 0.799, respectively.
Emotion regulation flexibility was assessed using the Emotion Regulation Flexibility Scale, which comprises two subscales: the reappraisal flexibility subscale (5 items) and the expressive flexibility subscale (5 items) [11]. Participants rated each item on a 7-point Likert scale ranging from 1 (completely disagree) to 7 (completely agree). Higher scores indicated greater reappraisal flexibility or expressive flexibility. The scores of the two subscales were summed to represent the overall emotion regulation flexibility. The Chinese version of this scale has demonstrated satisfactory reliability and validity [11], including among adolescent populations [31]. In this study, Cronbach’s α for the total scale, reappraisal flexibility subscale, and expressive flexibility subscale were 0.922, 0.877, and 0.828, respectively.
Regulatory emotional self-efficacy, which encompasses three dimensions—self-efficacy in expressing positive emotions, self-efficacy in regulating despondency/distress emotions, and self-efficacy in regulating anger/irritation emotions—was assessed using the Regulatory Emotional Self-Efficacy Scale [14]. The scale consists of 12 items, with each dimension comprising 4 items. Participants responded on a 5-point Likert scale ranging from 1 (completely disagree) to 5 (completely agree). Higher scores indicated greater self-efficacy in emotion regulation. The Chinese version has satisfactory reliability and validity [32]. In this study, Cronbach’s α for the total scale and three subscales was 0.901, 0.877, 0.819, and 0.865, respectively.
Statistical analyses were performed using SPSS 26.0 (IBM Corp., Armonk, NY, USA). Descriptive statistics were calculated for all variables. Correlations between variables were assessed using Pearson correlations. Multiple linear regression was used to estimate the associations between 24-HMG and emotion regulation-related indices. Model diagnostics, including Q-Q plots (normality), fitted value residual plots (linearity and homoscedasticity), and variance inflation factors (multicollinearity), confirmed that all linear regression assumptions were met. The number of guidelines met (continuous variable) and different guideline combinations (categorical variables) were included as independent variables in the model. Gender, age, hometown, grade, whether or not to be an only child, father’s education level, and mother’s education level were included as covariates. For all statistical tests, the significance level was set at p < 0.05.
This study revealed that 6.55% (n = 35), 30.15% (n = 161), and 3.00% (n = 16) of participants met only the RST guideline, only the sleep guideline, or only the PA guideline, respectively. Additionally, 6.74% (n = 36) met 2 out of 3 guidelines, including RST + sleep (n = 24, 4.49%), RST + PA (n = 2, 0.37%), and PA + sleep (n = 10, 1.87%). Only two participants met all three components of the 24-HMG. Unfortunately, a majority of participants, constituting 53.18% (n = 284), did not meet any of the three guidelines (Table 1).
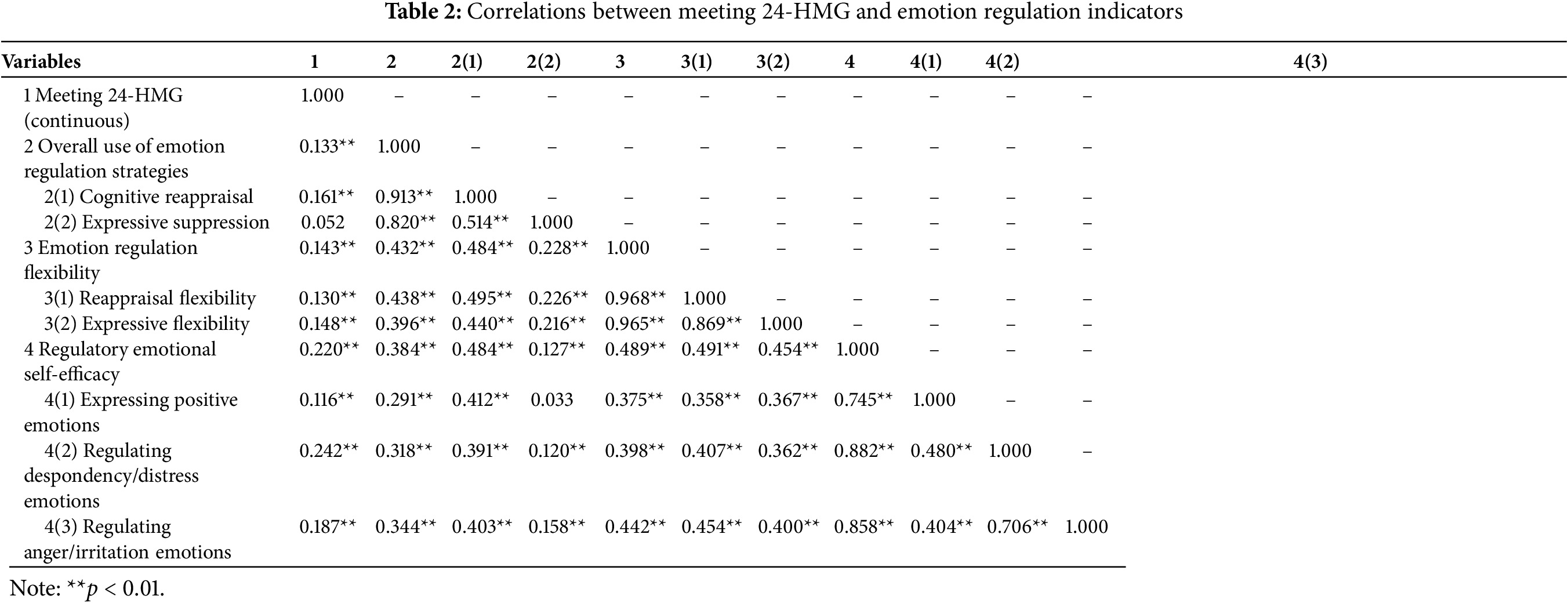
The correlations between meeting 24-HMG and emotion regulation-related indicators are presented in Table 2. We can see that meeting 24-HMG showed positive correlations with cognitive reappraisal, emotion regulation flexibility and its sub-dimensions, as well as regulatory emotional self-efficacy and its sub-dimensions (all p < 0.01). However, there was no significant correlation between meeting 24-HMG and expressive suppression (p > 0.05).
3.3 Associations between Meeting 24-HMG and Emotion Regulation Indicators
3.3.1 Associations with Emotion Regulation Strategies
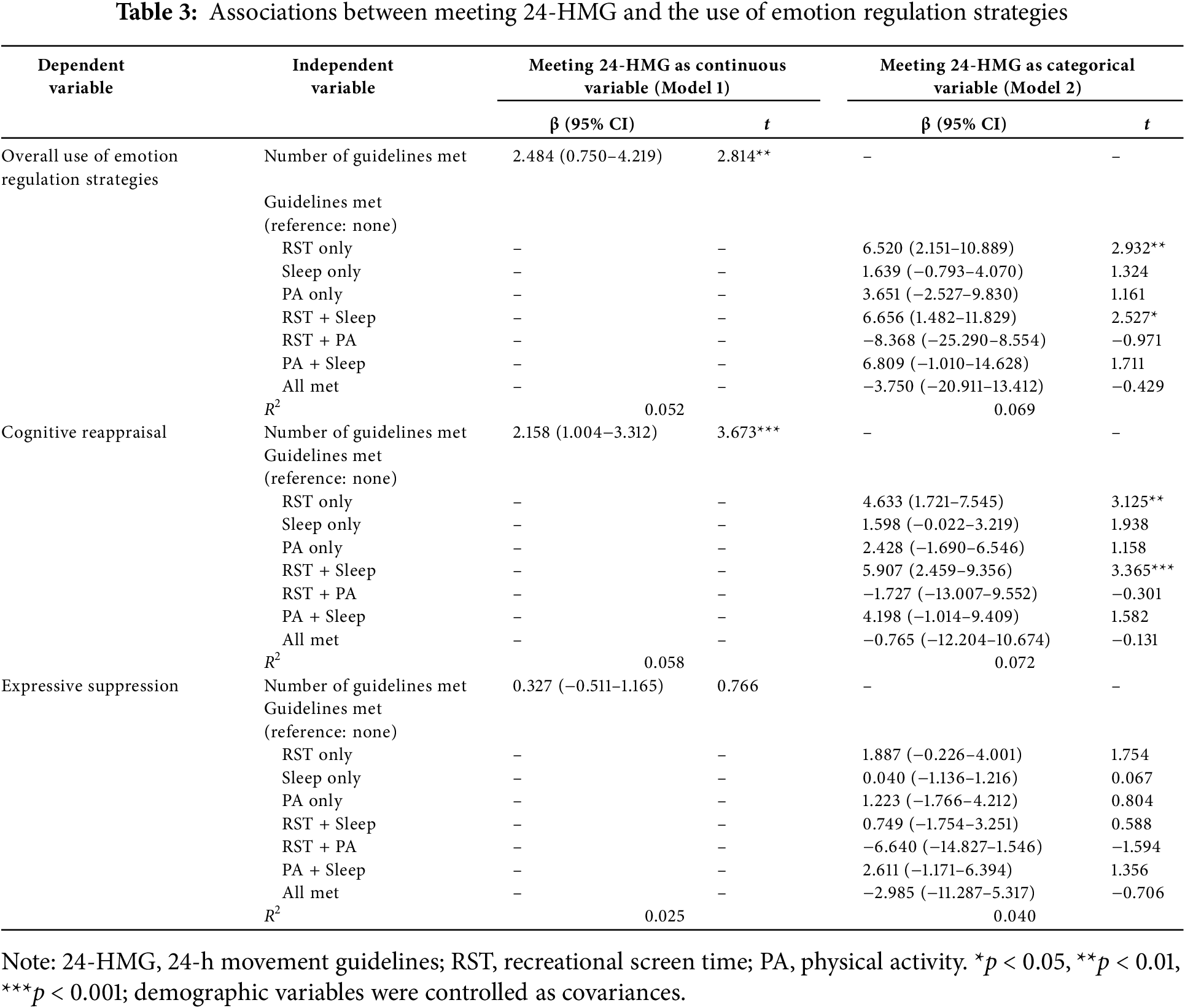
Table 3 shows the associations between meeting 24-HMG and the use of emotion regulation strategies. As a continuous variable, the number of 24-HMG met was positively associated with the use of cognitive reappraisal (β = 2.158, 95% CI: 1.004–3.312, p < 0.001), and overall emotion regulation strategies (β = 2.484, 95% CI: 0.750–4.219, p < 0.01). Children and adolescents who met only the RST guideline or met RST with sleep guidelines used more cognitive reappraisal (β = 4.633, 95% CI: 1.721–7.545, p < 0.01; β = 5.907, 95% CI: 2.459–9.356, p < 0.001) and overall emotion regulation strategies (β = 6.520, 95% CI: 2.151–10.889, p < 0.01; β = 6.656, 95% CI: 1.482–11.829, p < 0.05) than those who met none of the 24-HMG. However, there were no significant associations between either the number of 24-HMG met or meeting any subsets of the guidelines and the use of expressive suppression (all p > 0.05).
3.3.2 Associations with Emotion Regulation Flexibility
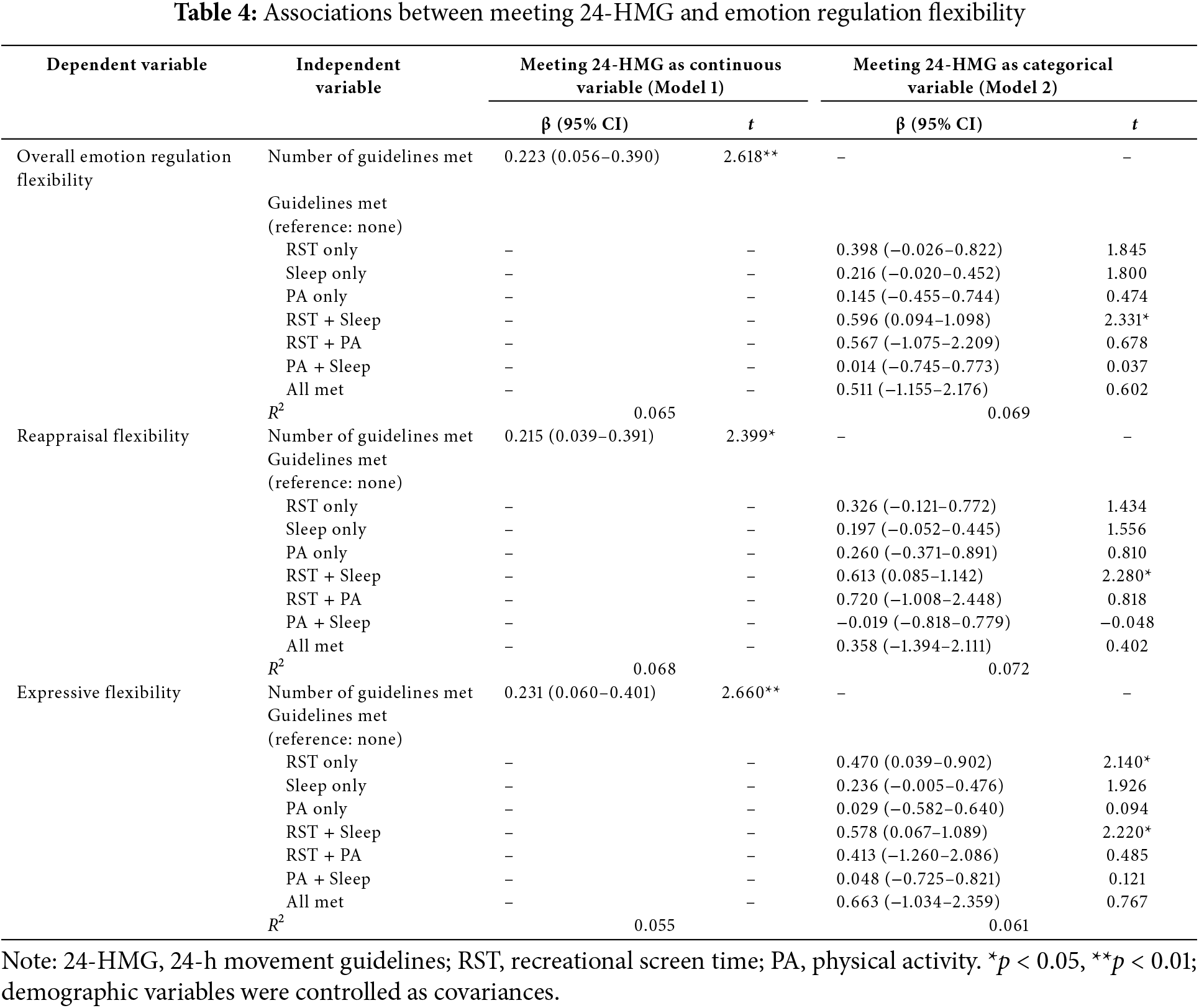
Table 4 shows the associations between meeting 24-HMG and emotion regulation flexibility. As a continuous variable, the number of 24-HMG met was positively associated with reappraisal flexibility (β = 0.215, 95% CI: 0.039–0.391, p < 0.05), expressive flexibility (β = 0.231, 95% CI: 0.060–0.401, p < 0.01), and overall emotion regulation flexibility (β = 0.223, 95% CI: 0.056–0.390, p < 0.01). Compared with meeting none of the 24-HMG, children and adolescents who met RST with sleep guidelines showed significantly higher reappraisal flexibility (β = 0.613, 95% CI: 0.085–1.142, p < 0.05), expressive flexibility (β = 0.578, 95% CI: 0.067–1.089, p < 0.05), and overall emotion regulation flexibility (β = 0.596, 95% CI: 0.094–1.098, p < 0.05). Participants who met RST guideline alone also showed higher expressive flexibility than those who did not meet any of 24-HMG (β = 0.470, 95% CI: 0.039–0.902, p < 0.05).
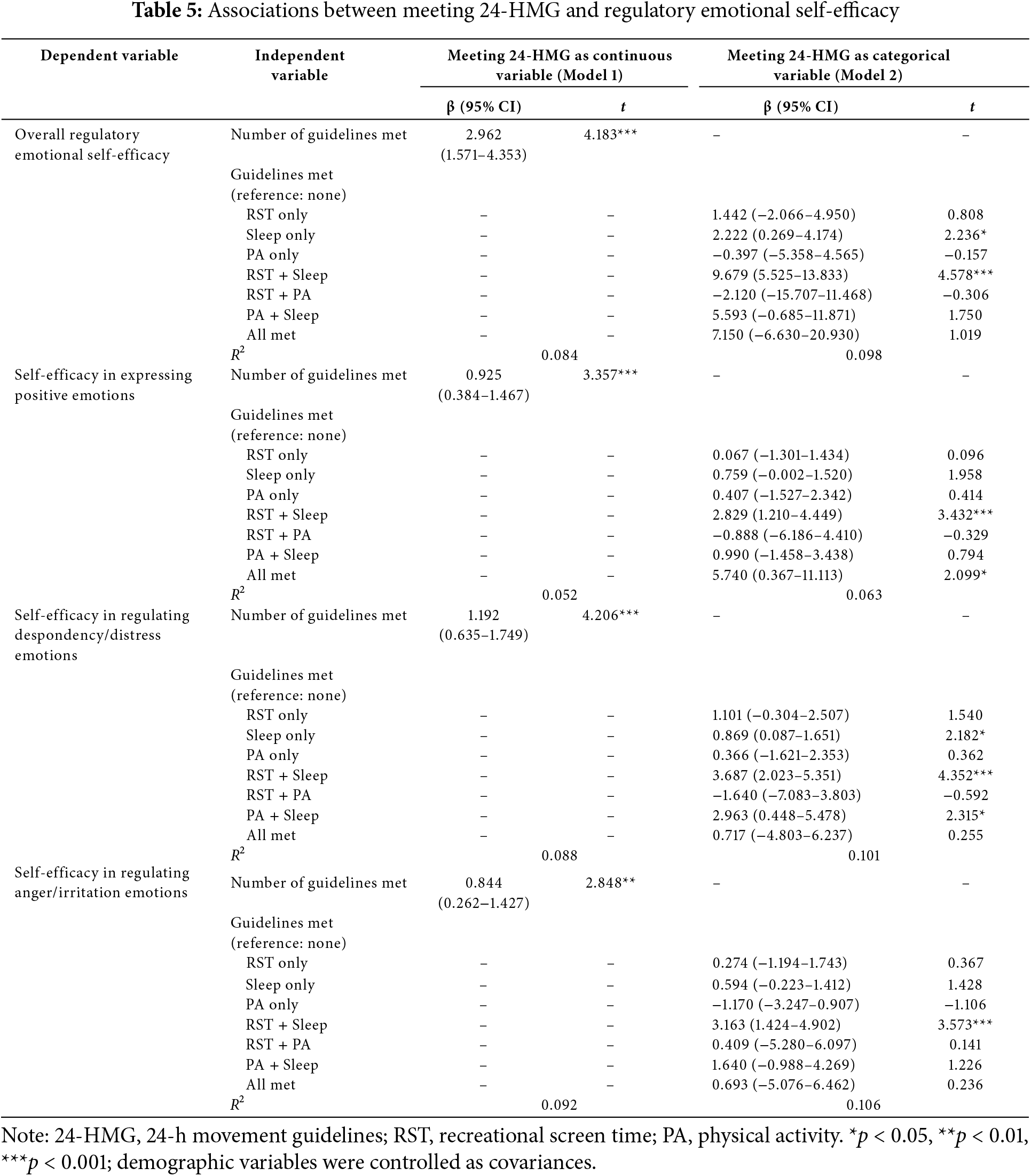
3.3.3 Associations with Regulatory Emotional Self-Efficacy
Table 5 shows the associations between meeting 24-HMG and regulatory emotional self-efficacy. As a continuous variable, the number of 24-HMG met was positively associated with self-efficacy in expressing positive emotions (β = 0.925, 95% CI: 0.384–1.467, p < 0.001), regulating despondency/distress emotions (β = 1.192, 95% CI: 0.635–1.749, p < 0.001), regulating anger/irritation emotions (β = 0.844, 95% CI: 0.262–1.427, p < 0.01), and overall regulatory emotional self-efficacy (β = 2.962, 95% CI: 1.571–4.353, p < 0.001). Participants who met sleep guideline alone (β = 2.222, 95% CI: 0.269–4.174, p < 0.05) or RST with sleep guidelines (β = 9.679, 95% CI: 5.525–13.833, p < 0.001) showed higher overall regulatory emotional self-efficacy than those who met none. In terms of self-efficacy in regulating different emotions, participants who met RST with sleep guidelines (β = 2.829, 95% CI: 1.210–4.449, p < 0.001) or met all the three guidelines (β = 5.740, 95% CI: 0.367–11.113, p < 0.05) showed higher self-efficacy in expressing positive emotions than those who met none. Participants who met sleep guideline alone (β = 0.869, 95% CI: 0.087–1.651, p < 0.05), RST with sleep guidelines (β = 3.687, 95% CI: 2.023–5.351, p < 0.001), or PA with sleep guidelines (β = 2.963, 95% CI: 0.448–5.478, p < 0.05) showed higher self-efficacy in regulating despondency/distress emotions than those who met none. Participants who met RST with sleep guidelines (β = 3.163, 95% CI: 1.424–4.902, p < 0.001) showed higher self-efficacy in regulating anger/irritation emotions than those who met none.
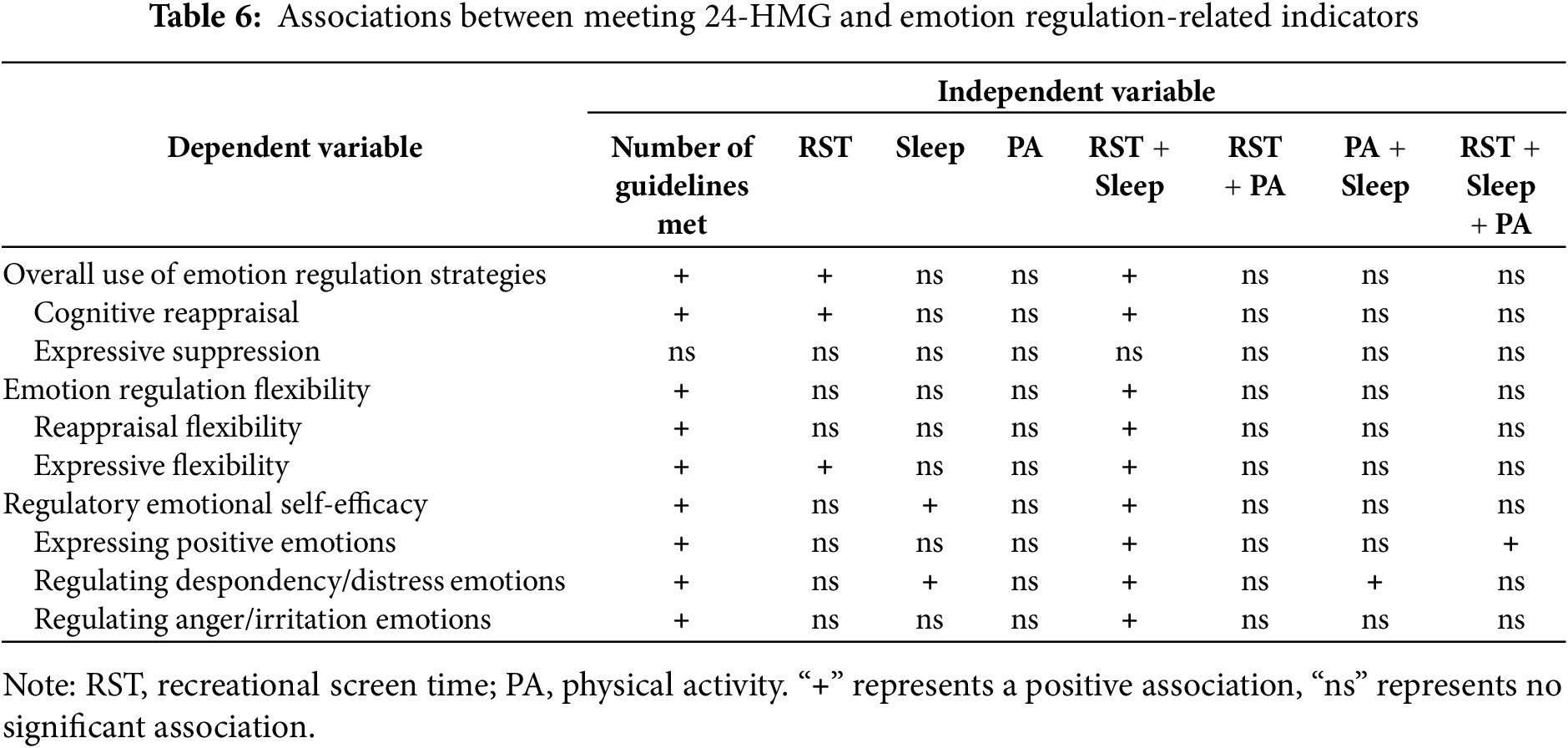
The current study examined the relationships between meeting 24-HMG and emotion regulation-related indicators (i.e., the use of emotion regulation strategies, emotion regulation flexibility, and regulatory emotional self-efficacy) among Chinese children and adolescents. We observed that only a very limited number of children and adolescents met all three 24-HMG. Significant positive associations were found between the number of guidelines met or meeting specific guidelines and some of the examined outcomes (Table 6 for an overview). Our study contributes to the existing literature on the 24-hour movement behaviors framework by deepening our understanding of the role of daily movement behaviors in emotion regulation among children and adolescents. Simultaneously, it responds to the appeal for research that aims to promote emotion regulation in this specific population.
4.1 24-HMG Adherence among Children and Adolescents
In this study, only a minority of children and adolescents (7.12%) successfully adhered to two or all three 24-HMG. Unfortunately, more than half of the participants failed to adhere to any of the guidelines. These findings are similar to previous research. Liang et al. found that only 1.7% of adolescents met all three guidelines, with the majority of adolescents struggling to follow the evidence-based lifestyle recommendations outlined in the 24-HMG [33]. Huang et al. also made a note that the prevalence of compliance with 24-HMG in China is much lower than the global level, which may be partially attributable to high academic burdens [34]. Chinese children and adolescents dedicate a substantial amount of time to accomplish academic tasks, which has squeezed their available time for other activities like PA and sleep [33]. It is critical to address the challenge of poor adherence to the 24-HMG among Chinese children and adolescents as part of future health promotion initiatives. A key strategy is to raise the stakeholders’ (parents, teachers, educational policy makers) awareness of health benefits associated with meeting these guidelines, which is not limited to the physical domain, but also extends to mental and cognitive aspects [27–29]. Our study further provides evidence on the association between meeting 24-HMG and emotion regulation, with a view to enhancing awareness of following these healthy lifestyle guidelines among children and adolescents.
4.2 Meeting 24-HMG and Emotion Regulation Strategies
The use of emotion regulation strategies is a crucial aspect of emotion regulation. We found that the number of meeting 24-HMG was positively associated with cognitive reappraisal and the total use of emotion regulation strategies. Such findings are supported by previous studies [18,35]. Aparicio et al. suggested that healthy lifestyles, such as reduced sedentary behavior, adequate sleep, and improved PA, may have benefits for emotion regulation and the development of adaptive emotion regulation strategies [36], which further supports our findings. It is well-documented that both sufficient PA and sleep enhance prefrontal functions [21,37], which are essential for emotion regulation. Besides, less screen-based sedentary behavior may benefit cognitive flexibility [24], allowing for greater use of emotion regulation strategies amidst fluctuating emotional states.
As a categorical variable, different combinations of 24-HMG, including meeting only RST, or meeting RST and sleep recommendations, were linked to better performance in cognitive reappraisal and overall use of emotion regulation strategies. However, we did not observe the association between meeting 24-HMG and expressive suppression. Similarly, Parsons et al. also reported no statistically significant associations between sleep duration and expressive suppression [38]. It appears that meeting 24-HMG will better facilitate children and adolescents in altering their appraisals of emotional stimuli when faced with emotionally arousing events, rather than suppressing emotional expression.
4.3 Meeting 24-HMG and Emotion Regulation Flexibility
Emotion regulation flexibility reflects the ability to implement emotion regulation strategies that are synchronized with contextual demands [10]. We found that the number of meeting 24-HMG was positively associated with reappraisal flexibility, expressive flexibility, and overall emotion regulation flexibility. Furthermore, as a categorical variable, meeting only RST, or meeting RST and sleep recommendations, was related to better performance in these outcomes. Although studies regarding the associations between daily movement behaviors and emotion regulation flexibility are limited, a study reported that greater PA predicts flexible reduction of negative emotions as the context shifted from peer-rejection to peer-acceptance, that is, greater emotion regulation flexibility [39]. Besides, Rezaie et al. discovered that more sleep problems are associated with worse emotion dysregulation (e.g., struggling to manage impulsive behaviors, refusal to accept negative emotions), and more PA is associated with less emotion dysregulation [37], which further supports our research.
To our knowledge, this is one of the few studies investigating determinants of emotion regulation flexibility among children and adolescents. We demonstrated the positive associations between healthy lifestyles (i.e., limited RST, adequate sleep duration, and PA) and emotion regulation flexibility. Such associations are plausible given that emotion regulation flexibility depends on underlying cognitive control processes (e.g., inhibition, updating, shifting) [40], and that meeting 24-HMG was beneficially linked to these cognitive processes [29,41]. Considering our findings, it is recommended that children and adolescents adhere to 24-HMG, particularly RST and sleep guidelines, as this is conducive to heightened emotion regulation flexibility.
4.4 Meeting 24-HMG and Regulatory Emotional Self-Efficacy
The number of meeting 24-HMG was positively associated with self-efficacy in expressing positive emotions, regulating despondency/distress emotions, regulating anger/irritation emotions, as well as overall regulatory emotional self-efficacy. These findings are consistent with the observations from other studies. For example, Wu et al. identified the positive association of PA with regulatory emotional self-efficacy [42]. Furthermore, Yang et al. found that sleep disturbance was negatively related to regulatory emotional self-efficacy and its three dimensions [19]. Based on these findings, it seems reasonable to speculate that meeting 24-HMG may be an important step in promoting regulatory emotional self-efficacy in children and adolescents, although future longitudinal research is needed to empirically support this assumption.
As a categorical variable, meeting different combinations of 24-HMG exhibits distinct associations with self-efficacy in emotion regulation across various emotional domains. For expressing positive emotions, meeting RST and sleep recommendations, or meeting all three guidelines was related to higher self-efficacy; for regulating despondency and distress emotions, meeting only sleep, meeting RST and sleep, or meeting PA and sleep recommendations was related to higher self-efficacy; for regulating anger and irritation emotions, meeting RST and sleep was related to higher self-efficacy. We validated the positive relationship between daily lifestyles and self-efficacy in regulating various emotions, providing insights for enhancing emotional management competence of children and adolescents.
4.5 Implications and Limitations
Our study has several important implications. As one of the few investigations examining the determinants of emotion regulation indicators in children and adolescents, this research provides empirical evidence supporting a positive association between meeting 24-HMG and enhanced emotion regulation outcomes, suggesting that all health-related behaviors (PA, sedentariness, sleep) throughout the day matter for emotion regulation. From a practical standpoint, these results offer valuable insights for enhancing children’s and adolescents’ emotion regulation from the perspective of daily behavior management. Effective measures should be taken to ensure adequate PA, sufficient sleep, and reduced RST each day. Specifically, health education programs for teachers and parents can be developed to emphasize the importance of meeting 24-HMG and offer practical tips for helping children and adolescents balance study, PA, sedentary activities, and sleep throughout the day. Additionally, psychosocial strategies such as goal-setting, self-regulation techniques, and peer or familial support can be designed and delivered to target groups. Furthermore, collaborative communications between school and family members should be strengthened to ensure activities of students can be monitored and guided both in and out-school.
However, some limitations should be considered when interpreting the findings. First, due to the cross-sectional nature of the research, causal relationships between variables cannot be established. Subsequent research should employ longitudinal designs or randomized controlled trials to establish directionality and causality. Second, all measures relied on self-reported questionnaires, introducing the possibility of respondent biases and social desirability. Future studies are encouraged to use more objective and comprehensive measures. Third, the reliance on a single Chinese sample may limit the generalizability of the findings. Future studies should incorporate populations from diverse cultural contexts to assess the cross-cultural applicability of the findings.
Meeting 24-HMG was associated with increased use of emotion regulation strategies, higher emotion regulation flexibility, and enhanced regulatory emotional self-efficacy among children and adolescents. To promote better emotion regulation in children and adolescents, efforts should be united to help them adhere to at least one movement guideline (such as the RST guideline) and then progressively adopt all movement guidelines.
Acknowledgement: We thank all the school teachers who helped to collect the questionnaires, and all the students who participated in the survey.
Funding Statement: This research was supported by Zhejiang Provincial Social Science Funding (22NDJC050YB).
Author Contributions: Conceptualization, Shanshan Xu and Liang Hu; methodology, Shanshan Xu and Liang Hu; investigation, Shanshan Xu; data curation, Shanshan Xu and Liang Hu; writing—original draft, Shanshan Xu; writing—review & editing, Liang Hu and Shanshan Xu; project administration, Liang Hu; funding acquisition, Liang Hu. All authors reviewed the results and approved the final version of the manuscript.
Availability of Data and Materials: The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval: The Medical Ethics Committee of the Department of Psychological and Behavioral Sciences at Zhejiang University approved this research (No. [2021]052). All participants in this study signed the informed consent form.
Conflicts of Interest: The authors declare no conflicts of interest to report regarding the present study.
References
1. De Looze ME, Cosma AP, Vollebergh WAM, Duinhof EL, de Roos SA, van Dorsselaer S, et al. Trends over time in adolescent emotional wellbeing in The Netherlands, 2005–2017: links with perceived schoolwork pressure, parent-adolescent communication and bullying victimization. J Youth Adolesc. 2020;49(10):2124–35. doi:10.1007/s10964-020-01280-4. [Google Scholar] [PubMed] [CrossRef]
2. Shorey S, Ng ED, Wong CHJ. Global prevalence of depression and elevated depressive symptoms among adolescents: a systematic review and meta-analysis. Br J Clin Psychol. 2022;61(2):287–305. doi:10.1111/bjc.12333. [Google Scholar] [PubMed] [CrossRef]
3. Liu RT, Walsh RFL, Sheehan AE, Cheek SM, Sanzari CM. Prevalence and correlates of suicide and nonsuicidal self-injury in children: a systematic review and meta-analysis. JAMA Psych. 2022;79(7):718–26. doi:10.1001/jamapsychiatry.2022.1256. [Google Scholar] [PubMed] [CrossRef]
4. Chang Q, Shi Y, Yao S, Ban X, Cai Z. Prevalence of suicidal ideation, suicide plans, and suicide attempts among children and adolescents under 18 years of age in mainland China: a systematic review and meta-analysis. Trauma Violence Abuse. 2024;25(3):2090–102. doi:10.1177/15248380231205828. [Google Scholar] [PubMed] [CrossRef]
5. Gross JJ. The emerging field of emotion regulation: an integrative review. Rev Gen Psychol. 1998;2(3):271–99. doi:10.1037/1089-2680.2.3.271. [Google Scholar] [CrossRef]
6. Gross JJ. Antecedent-and response-focused emotion regulation: divergent consequences for experience, expression, and physiology. J Pers Soc Psychol. 1998;74(1):224–37. doi:10.1037/0022-3514.74.1.224. [Google Scholar] [PubMed] [CrossRef]
7. Ray RD, Wilhelm FH, Gross JJ. All in mind’s eye? Anger rumination and reappraisal. J Pers Soc Psychol. 2008;94(1):133–45. doi:10.1037/0022-3514.94.1.133. [Google Scholar] [PubMed] [CrossRef]
8. Gross JJ, John OP. Individual differences in two emotion regulation processes: implications for affect, relationships, and well-being. J Pers Soc Psychol. 2003;85(2):348–62. doi:10.1037/0022-3514.85.2.348. [Google Scholar] [PubMed] [CrossRef]
9. Aldao A. The future of emotion regulation research: capturing context. Perspect Psychol Sci. 2013;8(2):155–72. doi:10.1177/1745691612459518. [Google Scholar] [PubMed] [CrossRef]
10. Aldao A, Sheppes G, Gross JJ. Emotion regulation flexibility. Cogn Ther Res. 2015;39(3):263–78. doi:10.1007/s10608-014-9662-4. [Google Scholar] [CrossRef]
11. Huang M, Tang G, Yi X, Sun S. Zhongyong thinking mode facilitates social adaptation: mediating effect of emotion regulation flexibility. Chin Soc Psychol Rev. 2014;8:88–112. (In Chinese). [Google Scholar]
12. Specker P, Sheppes G, Nickerson A. Does emotion regulation flexibility work? Investigating the effectiveness of regulatory selection flexibility in managing negative affect. Soc Psychol Pers Sci. 2024;15(5):561–9. doi:10.1177/19485506231189002. [Google Scholar] [CrossRef]
13. Galatzer-Levy IR, Burton CL, Bonanno GA. Coping flexibility, potentially traumatic life events, and resilience: a prospective study of college student adjustment. J Soc Clin Psychol. 2012;31(6):542–67. doi:10.1521/jscp.2012.31.6.542. [Google Scholar] [CrossRef]
14. Caprara GV, Giunta LD, Eisenberg N, Gerbino M, Pastorelli C, Tramontano C. Assessing regulatory emotional self-efficacy in three countries. Psychol Assess. 2008;20(3):227–37. doi:10.1037/1040-3590.20.3.227. [Google Scholar] [PubMed] [CrossRef]
15. Jiang Y, Zhang L, Mao Z. Physical exercise and mental health: the effect of emotion regulation self-efficacy and emotion regulation strategy. Stud Psychol Behav. 2018;16(4):570–6. (In Chinese). doi:10.3969/j.issn.1672-0628.2018.04.020. [Google Scholar] [CrossRef]
16. Caprara GV, Steca P, Gerbino M, Paciello M, Vecchio GM. Looking for adolescents’ well-being: self-efficacy beliefs as determinants of positive thinking and happiness. Epidemiol Psichiatr Soc. 2006;15(1):30–43. doi:10.1017/S1121189X00002013. [Google Scholar] [PubMed] [CrossRef]
17. Zhang Q, Zhang Q, Ran G, Liang Y. Childhood abuse and depression in emerging adults: the mediating role of regulatory emotional self-efficacy and the moderating role of subjective social status. J Adult Dev. 2024;31(3):206–16. doi:10.1007/s10804-023-09463-6. [Google Scholar] [CrossRef]
18. Wu J, Zhu L, Dong X, Sun Z, Cai K, Shi Y, et al. Relationship between physical activity and emotional regulation strategies in early adulthood: mediating effects of cortical thickness. Brain Sci. 2022;12(9):1210. doi:10.3390/brainsci12091210. [Google Scholar] [PubMed] [CrossRef]
19. Yang G, Li C, Zhu X, Yan J, Liu J. Prevalence of and risk factors associated with sleep disturbances among HPCD exposed to COVID-19 in China. Sleep Med. 2021;80(1):16–22. doi:10.1016/j.sleep.2020.12.034. [Google Scholar] [PubMed] [CrossRef]
20. Li Z, Qin Y, Cai W, Deng S, Mao X, Zhang J, et al. Sleep deprivation impairs human cognitive reappraisal ability: a randomized controlled trial. Nat Sci Sleep. 2023;15:729–36. doi:10.2147/NSS.S414962. [Google Scholar] [PubMed] [CrossRef]
21. Giles GE, Cantelon JA, Eddy MD, Brunye TT, Urry HL, Mahoney CR, et al. Habitual exercise is associated with cognitive control and cognitive reappraisal success. Exp Brain Res. 2017;235(12):3785–97. doi:10.1007/s00221-017-5098-x. [Google Scholar] [PubMed] [CrossRef]
22. Lollies F, Schnatschmidt M, Bihlmeier I, Genuneit J, In-Albnon T, Holtmann M, et al. Associations of sleep and emotion regulation processes in childhood and adolescence—a systematic review, report of methodological challenges and future directions. Sleep Sci. 2022;15(4):490–514. doi:10.5935/1984-0063.20220082. [Google Scholar] [PubMed] [CrossRef]
23. Mu F, Liu J, Lou H, Zhu W, Wang Z, Li B, et al. How breaking a sweat affects mood: the mediating role of self-efficacy between physical exercise and emotion regulation ability. PLoS One. 2024;19(6):e0303694. doi:10.1371/journal.pone.0303694. [Google Scholar] [PubMed] [CrossRef]
24. Cui J, Li L, Dong C. The associations between specific-type sedentary behaviors and cognitive flexibility in adolescents. Front Hum Neurosci. 2022;16:910624. doi:10.3389/fnhum.2022.910624. [Google Scholar] [PubMed] [CrossRef]
25. Sobol M, Wozny M, Czubak-Paluch K. Emotion regulation and social support as related to depressive symptoms: a study of healthy and hospitalized adolescents. Personal Individ Differ. 2021;174(2):110665. doi:10.1016/j.paid.2021.110665. [Google Scholar] [CrossRef]
26. Tremblay MS, Carson V, Chaput JP, Gorber SC, Dinh T, Duggan M, et al. Canadian 24-hour movement guidelines for children and youth: an integration of physical activity, sedentary behaviour, and sleep. Appl Physiol Nutr Metab. 2016;41(6):S311–27. doi:10.1139/apnm-2016-0151. [Google Scholar] [PubMed] [CrossRef]
27. Haegele JA, Zhu X, Healy S, Patterson F. The 24-hour movement guidelines and body composition among youth receiving special education services in the United States. J Phys Act Health. 2021;18(7):838–43. doi:10.1123/jpah.2019-0665. [Google Scholar] [PubMed] [CrossRef]
28. Lu S, Cheval B, Yu Q, Hossain MM, Chen S, Taylor A, et al. Associations of 24-hour movement behavior with depressive symptoms and anxiety in children: cross-sectional findings from a Chinese sample. Healthcare. 2021;9(11):1532. doi:10.3390/healthcare9111532. [Google Scholar] [PubMed] [CrossRef]
29. Walsh JJ, Barnes JD, Cameron JD, Goldfield GS, Chaput JP, Gunnell KE, et al. Associations between 24 h movement behaviours and global cognition in US children: a cross-sectional observational study. Lancet Child Adol Health. 2018;2(11):783–91. doi:10.1016/S2352-4642(18)30278-5. [Google Scholar] [PubMed] [CrossRef]
30. Jiang Y, Bai X, Shen L. The development of emotion regulation strategy on primary and secondary school students. J Psychol Sci. 2008;31(6):1308–12. (In Chinese). doi:10.16719/j.cnki.1671-6981.2008.06.014. [Google Scholar] [CrossRef]
31. Yao Y, Yan Z, Xu D, Xuan Y. The relationship between emotion regulation ability and anxiety in adolescents: independent and collaborative mediating roles of adaptive and nonadaptive emotion regulation strategies. Curr Psychol. 2024;43(42):33059–76. doi:10.1007/s12144-024-06818-4. [Google Scholar] [CrossRef]
32. Ye B, Li L, Wang P, Wang RN, Liu MF, Wang XQ, et al. Social anxiety and subjective well-being among Chinese college students: a moderated mediation model. Pers Individ Differ. 2021;175(1):110680. doi:10.1016/j.paid.2021.110680. [Google Scholar] [CrossRef]
33. Liang K, Chen S, Chi X. Differential associations between meeting 24-hour movement guidelines with mental wellbeing and mental illness among Chinese adolescents. J Adolescent Health. 2023;72(5):658–66. doi:10.1016/j.jadohealth.2022.11.231. [Google Scholar] [PubMed] [CrossRef]
34. Huang S, Huang Y, Gu Y, Chen H, Lv RX, Wu SY, et al. Adherence to 24-hour movement guidelines in relation to the risk of overweight and obesity among children and adolescents. J Adolescent Health. 2023;73(5):887–95. doi:10.1016/j.jadohealth.2023.06.009. [Google Scholar] [PubMed] [CrossRef]
35. Palmer C, Oosterhoff B, Bower J, Kaplow J, Alfano C. Associations among adolescent sleep problems, emotion regulation, and affective disorders: findings from a nationally representative sample. J Psychiatr Res. 2017;96(15):1–8. doi:10.1016/j.jpsychires.2017.09.015. [Google Scholar] [PubMed] [CrossRef]
36. Aparicio E, Canals J, Arija V, De Henauw S, Michels N. The role of emotion regulation in childhood obesity: implications for prevention and treatment. Nutr Res Rev. 2016;29(1):17–29. doi:10.1017/S0954422415000153. [Google Scholar] [PubMed] [CrossRef]
37. Rezaie L, Norouzi E, Bratty AJ, Khazaie H. Better sleep quality and higher physical activity levels predict lower emotion dysregulation among persons with major depression disorder. BMC Psychol. 2023;11(1):171. doi:10.1186/s40359-023-01213-3. [Google Scholar] [PubMed] [CrossRef]
38. Parsons CE, Schofield B, Batziou SE, Ward C, Young KS. Sleep quality is associated with emotion experience and adaptive regulation of positive emotion: an experience sampling study. J Sleep Res. 2021;31(4):e13533. doi:10.1111/jsr.13533. [Google Scholar] [PubMed] [CrossRef]
39. Shields MC, Matt LM, Coifman KG. Physical activity and negative emotion during peer-rejection: evidence for emotion context sensitivity. J Health Psychol. 2016;21(12):2851–62. doi:10.1177/1359105315587139. [Google Scholar] [PubMed] [CrossRef]
40. Pruessner L, Barnow S, Holt DV, Joormann J, Schulze K. A cognitive control framework for understanding emotion regulation flexibility. Emotion. 2020;20(1):21–9. doi:10.1037/emo0000658. [Google Scholar] [PubMed] [CrossRef]
41. Zeng X, Cai L, Yang W, Tan W, Huang W, Chen Y. Association between the 24-hour movement guidelines and executive function among Chinese children. BMC Public Health. 2022;22(1):1017. doi:10.1186/s12889-022-13420-5. [Google Scholar] [PubMed] [CrossRef]
42. Wu R, Jing L, Liu Y, Wang H, Yang J. Effects of physical activity on regulatory emotional self-efficacy, resilience, and emotional intelligence of nurses during the COVID-19 pandemic. Front Psychol. 2022;13:1059786. doi:10.3389/fpsyg.2022.1059786. [Google Scholar] [PubMed] [CrossRef]
Cite This Article
 Copyright © 2025 The Author(s). Published by Tech Science Press.
Copyright © 2025 The Author(s). Published by Tech Science Press.This work is licensed under a Creative Commons Attribution 4.0 International License , which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
 Downloads
Downloads
 Citation Tools
Citation Tools