
 Submit a Paper
Submit a Paper Propose a Special lssue
Propose a Special lssue Open Access
Open Access
ARTICLE

The Impact of Depression and Anxiety on Negative Ideation Among Standardized Residency Trainees: The Moderating Role of Individual Resilience Dimensions
1 Department of Nursing, Jiangsu Cancer Hospital & Jiangsu Institute of Cancer Research & The Affiliated Cancer Hospital of Nanjing Medical University, Nanjing, 210000, China
2 Department of Anesthesiology, Jiangsu Cancer Hospital & Jiangsu Institute of Cancer Research & The Affiliated Cancer Hospital of Nanjing Medical University, Nanjing, 210000, China
3 Department of Anesthesiology, Perioperative and Pain Medicine, Nanjing First Hospital, Nanjing Medical University, Nanjing, 210006, China
* Corresponding Authors: Lihai Chen. Email: ; Minhao Zhang. Email:
# These authors contributed equally to this work
International Journal of Mental Health Promotion 2026, 28(2), 11 https://doi.org/10.32604/ijmhp.2025.071717
Received 11 August 2025; Accepted 09 December 2025; Issue published 27 February 2026
 View Full Text
View Full Text Download PDF
Download PDFAbstract
Objectives: Although standardized residency trainees are at high risk for depression, anxiety, and suicidal ideation, the psychological pathways connecting depression and anxiety to suicidal ideation, especially the moderating role of resilience, remain elusive. This study aimed to examine the associations between depression, anxiety, and suicidal ideation among physicians undergoing standardized residency training, and to investigate the moderating roles of different dimensions of individual resilience, namely tenacity, strength, and optimism. Methods: A convenience sampling method was adopted to recruit 133 resident physicians. Validated instruments assessing individual resilience, depressive symptoms, anxiety levels, and suicidal ideation were administered. Spearman correlation analysis was used to evaluate the relationships among the variables. Hierarchical regression analysis was conducted to assess the moderating roles of tenacity, strength, and optimism in the associations between depression, anxiety, and suicidal ideation. Results: Depressive symptoms and anxiety levels were both positively associated with suicidal ideation (p < 0.001). All three resilience dimensions were negatively correlated with suicidal ideation (tenacity: r = −0.504, strength: r = −0.477, optimism: r = −0.440, all p < 0.001). Tenacity, strength, and optimism significantly moderated the associations between depression and suicidal ideation (all p < 0.05). When resilience levels in these dimensions were high, the associations between depression and suicidal ideation were weaker. Strength and optimism also moderated the associations between anxiety and suicidal ideation (strength: p = 0.028, optimism: p = 0.028). When the resiliences (strength and optimism) were high, the associations between anxiety and suicidal ideation were weaker. Conclusion: Individual resilience, particularly in the dimensions of tenacity, strength, and optimism, may serve as protective correlates for physicians in training, being associated with weaker relationships between depression, anxiety, and suicidal ideation. These findings highlight the potential value of resilience-enhancing strategies in clinical training settings, although causal inferences cannot be drawn due to the cross-sectional design.Keywords
The mental health of physicians has increasingly been recognized as a critical concern in the field of global public health. The period of standardized residency training (SRT) represents a pivotal transitional stage from medical student to practicing physician. During this phase, trainees are frequently exposed to multiple sources of stress, including rigorous assessments, financial constraints, familial responsibilities, employment uncertainties, and strained doctor-patient relationships [1]. Under the cumulative burden of these pressures, resident physicians have been found to be particularly vulnerable to the development of psychological distress. Existing literature suggests that the prevalence of depression among residents undergoing standardized training ranges from approximately 7.7% to 93% [2,3,4,5], while anxiety has been reported in about 10% to 63.9% of this population, and the incidence of suicidal ideation was 8.7–13% [6,7]. The reported range of depression and anxiety prevalence varies significantly, which may be due to factors such as differences in study populations, research methods, diagnostic tools, and the timing of data collection across studies. Currently, depression and anxiety have been confirmed to be closely associated with a higher suicide risk among physicians [8,9,10,11]. However, existing studies mainly focus on the prevalence of depression, anxiety, and suicidal ideation, as well as their influencing factors, and limited attention to the underlying associations through which these emotional issues are linked with suicidal ideation. Particularly, research on psychological protective factors within the group of standardized residency trainees remains relatively scarce.
Resilience, also referred to as psychological resilience or mental toughness, is defined as the capacity of individuals to maintain or regain psychological and physiological equilibrium in the face of stress, adversity, or trauma [12]. Within the framework of the resilience buffering hypothesis, resilience functions as a moderating factor between psychological stress and negative outcomes—it does not eliminate stress but rather buffers its effects [13]. Studies conducted on student populations and other groups have found that resilience can play a moderating role between negative life events, stress, and suicidal ideation [14,15,16]. However, research has not sufficiently addressed whether specific resilience dimensions differentially buffer the harmful effects of depression and anxiety on suicidal ideation. Furthermore, evidence focusing on standardized residency trainees—who experience unique occupational stressors—is limited. Based on the above research, we hypothesize that higher levels of depressive and anxiety symptoms will be associated with higher levels of suicidal ideation among standardized residency trainees, and that resilience—particularly its key dimensions of tenacity, strength, and optimism—will weaken these associations (Fig. 1). In other words, we expect that trainees with higher resilience will show weaker links between psychological distress and suicidal ideation compared with those with lower resilience. Understanding these mechanisms may offer critical insights for developing targeted psychological interventions in medical training environments.
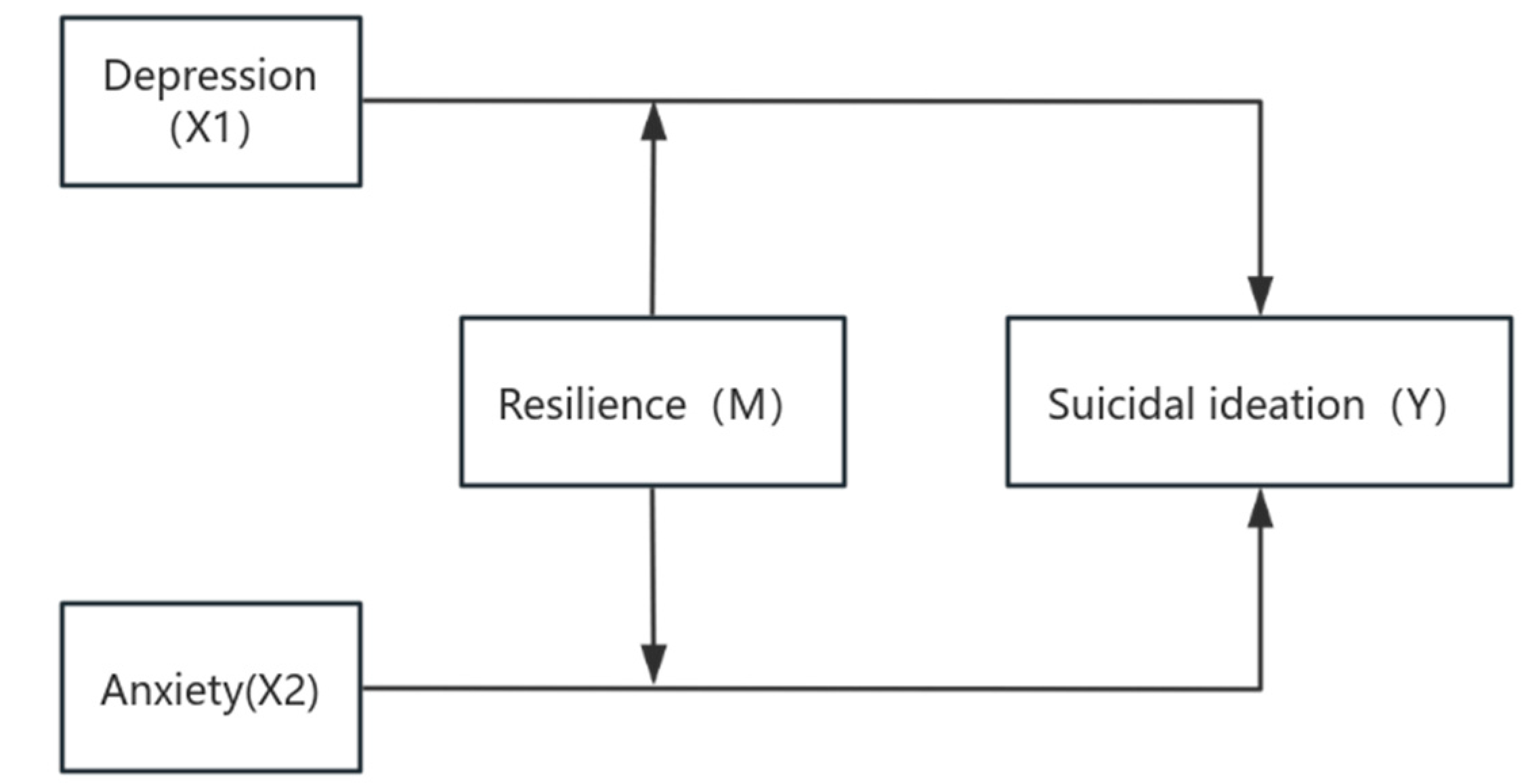
Figure 1: Research hypothesis model diagram. Note: X1 and X2 denote the independent variables; M denotes the moderator variable; Y denotes the dependent variable.
A convenience sampling method was adopted to recruit 133 standardized residency trainees who received standardized training at Nanjing First Hospital between January 1 and December 31, 2024, among them, 59 (44.36%) were male and 74 (55.64%) were female. The participants’ ages ranged from 23 to 42 years, with a median of 23 years. Participation was entirely voluntary, and informed consent was obtained from all respondents prior to data collection. All procedures performed in this study involving human participants were in accordance with the Declaration of Helsinki. Ethical approval for this study was granted by the Ethics Committee of Nanjing First Hospital (Ethical Approval No.: KY20250728-KS-02).
2.2.1 General Information Questionnaire
Basic demographic and training-related information was collected, including gender, age, training year, educational background, status as an only child, whether the participant was enrolled in a socialized training program, registered residence, parental educational levels, and monthly per capita household income.
2.2.2 Connor-Davidson Resilience Scale (CD-RISC)—Chinese Version
The Connor-Davidson Resilience Scale (CD-RISC)—Chinese Version was used to assess resilience [17]. The Chinese version retains all 25 items of the original scale and consists of three dimensions: tenacity, strength and optimism. The scale comprises 25 items rated on a 5-point Likert scale ranging from 0 (“not at all true”) to 4 (“true nearly all the time”). The subscale scores range as follows: tenacity (0–52), strength (0–32), and optimism (0–16), with a total possible score of 0–100. Higher scores indicate greater psychological resilience. In this study, the CD-RISC demonstrated high internal consistency with a Cronbach’s α coefficient of 0.892. Sample item: I can handle unhappiness.
2.2.3 Center for Epidemiologic Studies Depression Scale (CES-D)—Chinese Version
The Center for Epidemiologic Studies Depression Scale (CES-D)—Chinese Version [18] was employed to evaluate depressive symptoms. The scale consists of 20 items, rated on a 4-point scale from 0 (“rarely or none of the time”) to 3 (“most or all of the time”). Four of the items are reverse-scored. Total scores are calculated by summing the adjusted scores, with higher scores indicating more severe depressive symptoms. In the current study, the CES-D exhibited excellent reliability (Cronbach’s α = 0.948). Sample item: I feel down and unhappy.
2.2.4 Chinese Version of the Self-Rating Anxiety Scale (SAS)
The Chinese version of the Self-Rating Anxiety Scale (SAS) [19] was used to assess anxiety levels. This 20-item instrument uses a 4-point response format: 1 (“a little of the time”), 2 (“some of the time”), 3 (“a good part of the time”), and 4 (“most or all of the time”). Standard scores were calculated by multiplying the raw scores by 1.25 and converting them to integers. A standard score of 50 is considered the cut-off for anxiety: 50–59 (mild), 60–69 (moderate), and ≥70 (severe). The Cronbach’s α for this scale in the present study was 0.915. Sample item: I get upset or scared easily.
2.2.5 Beck Scale for Suicide Ideation—Chinese Version (BSI-CV)
Suicidal ideation was measured using the Chinese version of the Beck Scale for Suicide Ideation (BSI-CV) [20]. The scale contains 5 items, each rated on a 3-point scale (1 to 3), with higher scores indicating greater suicidal intent. The internal consistency of the scale was strong, with a Cronbach’s α coefficient of 0.904 in this study. Sample item: How strongly do you want to try suicide?
To ensure data integrity and reliability, all questionnaire items were set as mandatory and collected anonymously. After each questionnaire was completed, the research assistants immediately reviewed it for completeness and logical consistency, focusing on identifying any missing responses, duplicate selections, or clearly contradictory answers. If any issues were detected, the respondents were promptly contacted to provide clarification or corrections. Only questionnaires verified as accurate and complete were collected and subsequently coded and archived. A dual-entry system was used by two independent researchers to enter and verify the data. A total of 133 questionnaires were distributed and collected, all of which were deemed valid, resulting in a 100% valid response rate.
All statistical analyses were performed using SPSS version 26.0 (IBM Corp., Armonk, NY, USA). The Harman single-factor test was used to examine common method bias, with all items from the CD-RISC, CES-D, SAS, and BSI-CV scales in the 133 questionnaires being treated as variables for factor analysis. Since the continuous variables failed to meet normality assumptions as assessed by the Kolmogorov-Smirnov test, they were expressed as medians and interquartile ranges (IQR; P25, P75). Group comparisons were conducted using the Mann-Whitney U test (for two groups) or the Kruskal-Wallis H test (for multiple groups). Spearman’s rank correlation was employed to examine the associations among study variables. Hierarchical regression analysis was conducted to assess the moderating effects of resilience dimensions on the relationships between depression, anxiety, and suicidal ideation. Analytical Steps for Tenacity and Strength: Model 1 (Baseline): Suicidal ideation was regressed on depression/anxiety to examine their direct effect. Model 2 (Main Effects): The moderator (Tenacity or Strength, respectively) was added to Model 1 to assess its main effect on suicidal ideation after controlling for depression/anxiety. Model 3 (Moderation): The interaction term between depression/anxiety and the corresponding moderator (depression/anxiety × Tenacity or depression/anxiety × Strength) was incorporated into Model 2 to test for the moderating effect. Analytical Steps for Optimism: Model 1 (Covariate Model): Monthly household income per capita was entered first as a covariate into the regression equation.
Model 2 (Baseline Model): Depression/Anxiety was then added to Model 1 to examine its direct effect on suicidal ideation after controlling for income. Model 3 (Main Effects Model): The moderator, Optimism, was incorporated into Model 2 to assess its main effect on suicidal ideation, above and beyond the effects of income and depression/anxiety. Model 4 (Moderation Model): Finally, the interaction term between depression/anxiety and Optimism was added to Model 3 to test for the moderating effect. A p-value of less than 0.05 was considered statistically significant.
Harman’s single-factor test uses exploratory factor analysis (EFA) to determine whether there is significant common method bias in the data. When the variance explained by the first factor is less than 40%, it is generally considered that there is no serious common method bias and the measurement results are relatively reliable. However, if the variance explained exceeds 40%, it indicates that a single factor accounts for too much explanatory power, suggesting the possible presence of substantial common method bias that needs to be further controlled or corrected. Harman’s single-factor test revealed 12 factors with eigenvalues greater than 1. The first factor explained 36.52% of variance, far below the 40% threshold, indicating no significant common method bias in the data.
3.2 Depression, Anxiety, Suicidal Ideation, and Resilience Scores Across Demographic Subgroups
The median (IQR) scores among all participants were as follows: Depression: 25.0 (20.0, 31.0). Anxiety: 41.0 (36.0, 47.0). Suicidal ideation: 4.0 (4.0, 5.0). For resilience dimensions: Tenacity: 27.0 (22.0, 33.0), Strength: 18.0 (16.0, 23.0), Optimism: 9.0 (8.0, 10.0).
When scores for depression, anxiety, suicidal ideation, and resilience (tenacity and strength) were compared across different demographic groups, no statistically significant differences were observed (p > 0.05). However, a significant difference was found in resilience (optimism) scores across groups with different monthly household income per capita (p = 0.020). To control for potential confounding, household income was included as a covariate in the subsequent hierarchical regression analysis (Table 1).
Table 1: Depression, anxiety, and suicidal ideation scores by demographic characteristics.
| Variable | n | Depression Score | Anxiety Score | Suicidal Ideation Score | ||||
|---|---|---|---|---|---|---|---|---|
| Tenacity | Strength | Optimism | Total | |||||
| Gender | Male | 59 | 23.0 (20.0, 28.0) | 42.0 (37.0, 48.0) | 26.0 (20.0, 31.0) | 18.0 (15.0, 22.0) | 9.0 (7.0, 10.0) | 4.0 (4.0, 5.0) |
| Female | 74 | 25.0 (19.8, 31.3) | 40.0 (34.0, 46.0) | 29.0 (25.0, 36.8) | 20.0 (16.0, 24.0) | 9.0 (8.0, 11.0) | 4.0 (4.0, 5.0) | |
| p-value | / | 0.310 | 0.183 | 0.085 | 0.066 | 0.129 | 0.638 | |
| Age (years) | ≤24 | 25 | 24.0 (19.0, 26.0) | 40.00 (35.0, 45.0) | 27.00 (25.0, 31.0) | 17.0 (16.0, 22.0) | 9.0 (8.0, 10.0) | 53.00 (50.0, 62.0) |
| 25 | 35 | 25.0 (21.5, 35.0) | 41.00 (36.5, 51.0) | 26.00 (17.0, 33.5) | 18.0 (14.0, 22.5) | 8.0 (6.0, 10.0) | 50.0 (38.5, 65.0) | |
| 26 | 33 | 25.0 (20.0, 31.0) | 41.00 (36.0, 48.0) | 26.0 (20.0, 29.0) | 18.0 (14.0, 21.0) | 9.0 (7.0, 10.0) | 53.0 (43.0, 59.0) | |
| ≥27 | 40 | 23.5 (18.0, 29.3) | 40.50 (34.8, 45.5) | 29.0 (25.0, 36.3) | 20.0 (16.0, 24.0) | 9.0 (8.0, 11.0) | 59.0 (49.8, 72.0) | |
| p-value | / | 0.199 | 0.565 | 0.247 | 0.276 | 0.263 | 0.267 | |
| Participation in Socialized Residency Training | No | 88 | 24.0 (19.3, 31.0) | 40.0 (36.0, 47.5) | 26.0 (21.3, 33.5) | 18.0 (15.3, 23.0) | 9.0 (8.0, 10.0) | 4.0 (4.0, 5.0) |
| Yes | 45 | 25.0 (21.5, 31.5) | 41.0 (34.0, 47.5) | 29.0 (22.5, 33.5) | 19.0 (16.0, 23.0) | 9.0 (7.0, 10.5) | 4.0 (4.0, 6.0) | |
| p-value | / | 0.512 | 0.813 | 0.887 | ||||
| Year of Training | First Year | 55 | 28.0 (24.0, 36.0) | 19.0 (16.0, 24.0) | 28.0 (24.0, 36.0) | 19.0 (16.0, 24.0) | 9.0 (8.0, 10.0) | 9.0 (8.0, 10.0) |
| Second Year | 51 | 27.0 (20.0, 31.0) | 18.0 (15.0, 22.0) | 27.0 (20.0, 31.0) | 18.0 (15.0, 22.0) | 8.0 (6.0, 10.0) | 8.0 (6.0, 10.0) | |
| Third Year | 27 | 26.0 (23.0, 33.0) | 20.0 (16.0, 23.0) | 26.0 (23.0, 33.0) | 20.0 (16.0, 23.0) | 9.0 (8.0, 11.0) | 9.0 (8.0, 11.0) | |
| p-value | / | 0.410 | 0.364 | 0.410 | 0.364 | 0.390 | 0.390 | |
| Place of Household Registration | Urban | 61 | 25.0 (18.0, 31.0) | 41.0 (34.0, 47.5) | 28.0 (22.0, 37.0) | 19.0 (15.5, 24.0) | 9.0 (7.5, 11.0) | 4.0 (4.0, 5.0) |
| Rural | 68 | 24.5 (21.0, 31.8) | 42.0 (36.3, 47.5) | 26.0 (20.0, 30.0) | 18.0 (16.0, 21.8) | 9.0 (7.0, 10.0) | 4.0 (4.0, 5.0) | |
| Unknown | 4 | 19.0 (17.3, 20.0) | 39.5 (36.0, 54.3) | 28.0 (26.0, 34.5) | 18.5 (16.0, 22.5) | 8.0 (8.0, 10.3) | 4.0 (4.0, 4.0) | |
| p-value | / | 0.110 | 0.693 | 0.409 | 0.359 | 0.417 | 0.384 | |
| Only Child Status | No | 87 | 25.0 (21.0, 31.0) | 40.0 (35.0, 48.0) | 28.0 (22.0, 32.0) | 18.0 (16.0, 22.0) | 9.0 (7.0, 10.0) | 4.0 (4.0, 5.0) |
| Yes | 46 | 23.0 (18.0, 31.0) | 41.0 (36.5, 46.8) | 26.0 (21.8, 37.3) | 19.0 (16.0, 24.0) | 9.0 (8.0, 11.0) | 4.0 (4.0, 5.0) | |
| p-value | / | 0.150 | 0.446 | 0.879 | 0.269 | 0.318 | 0.300 | |
| Father’s Education Level | High school or below | 104 | 25.0 (20.3, 30.5) | 41.0 (36.0, 46.0) | 28.0 (22.0, 33.8) | 19.0 (16.0, 23.0) | 9.0 (7.0, 10.0) | 4.0 (4.0, 5.0) |
| College or university | 24 | 22.5 (15.0, 31.8) | 40.5 (35.0, 48.0) | 26.0 (19.5, 34.8) | 17.0 (15.3, 23.8) | 8.5 (8.0, 10.0) | 4.0 (4.0, 5.8) | |
| Other | 5 | 30.0 (18.5, 45.5) | 53.0 (39.0, 69.5) | 26.0 (20.0, 41.0) | 18.0 (15.5, 26.0) | 10.0 (8.5, 13.5) | 4.0 (4.0, 4.0) | |
| p-value | / | 0.461 | 0.186 | 0.766 | 0.915 | 0.321 | 0.303 | |
| Mother’s Education Level | High school or below | 105 | 24.0 (20.0, 29.5) | 40.0 (35.5, 45.0) | 28.0 (22.0, 34.5) | 19.0 (16.0, 23.0) | 9.0 (7.0, 10.5) | 4.0 (4.0, 5.0) |
| College or university | 24 | 25.0 (19.3, 32.8) | 41.0 (35.3, 52.3) | 25.50 (17.3, 29.8) | 18.0 (14.3, 20.0) | 8.0 (7.3, 10.0) | 4.0 (4.0, 6.8) | |
| Other | 4 | 28.0 (19.0, 52.8) | 48.0 (35.5, 73.3) | 28.0 (21.5, 46.5) | 19.0 (17.3, 29.0) | 10.5 (9.3, 14.8) | 4.0 (4.0, 4.0) | |
| p-value | / | 0.682 | 0.444 | 0.228 | 0.496 | 0.182 | 0.295 | |
| Monthly Household Income (RMB) | 0–10,000 | 99 | 25.0 (20.0, 31.0) | 41.0 (36.0, 46.0) | 26.0 (22.0, 31.0) | 18.0 (15.0, 22.0) | 8.0 (7.0, 10.0) | 4.0 (4.0, 5.0) |
| 10,000–20,000 | 10 | 22.0 (11.0, 31.3) | 38.5 (32.5, 45.5) | 29.0 (25.0, 37.5) | 20.0 (15.8, 24.3) | 10.0 (7.8, 11.3) | 4.0 (4.0, 5.0) | |
| >20,000 | 6 | 24.5 (19.5, 40.3) | 40.0 (33.3, 55.5) | 34.5 (18.8, 39.5) | 22.0 (17.3, 26.8) | 10.0 (7.0, 12.0) | 4.0 (4.0, 9.5) | |
| Unknown | 18 | 22.5 (17.8, 31.0) | 41.5 (38.0, 53.0) | 28.0 (23.3, 39.5) | 20.0 (16.8, 24.5) | 10.5 (8.0, 12.3) | 4.0 (4.0, 4.0) | |
| p-value | / | 0.523 | 0.59 | 0.246 | 0.055 | 0.020 | 0.186 | |
3.3 Correlation Analysis among Depression, Anxiety, Suicidal Ideation, and Resilience Dimensions
Significant positive correlations were observed between both depression and anxiety with suicidal ideation (r = 0.466 and r = 0.395, respectively; all p < 0.001. Conversely, all three resilience dimensions, including tenacity, strength, and optimism, were found to be negatively correlated with suicidal ideation (r = −0.504, −0.477, and −0.440, respectively; all p < 0.001) (see Table 2).
Table 2: Spearman correlation coefficients among key variables.
| Variable | Depression Score | Anxiety Score | Resilience Score | Suicidal Ideation Score | ||||
|---|---|---|---|---|---|---|---|---|
| Tenacity | Strength | Optimism | ||||||
| Depression Score | r | 1.000 | 0.629 | −0.416 | −0.409 | −0.288 | 0.466 | |
| p | <0.001 | <0.001 | <0.001 | 0.001 | <0.001 | |||
| Anxiety Score | r | 0.629 | 1.000 | −0.402 | −0.363 | −0.263 | 0.395 | |
| p | <0.001 | <0.001 | <0.001 | 0.002 | <0.001 | |||
| Resilience Score | Tenacity | r | −0.416 | −0.402 | 1.000 | 0.899 | 0.720 | −0.504 |
| p | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | |||
| Strength | r | −0.409 | −0.363 | 0.899 | 1.000 | 0.774 | −0.477 | |
| p | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | |||
| Optimism | r | −0.288 | −0.263 | 0.72 | 0.774 | 1.000 | −0.440 | |
| p | 0.001 | 0.002 | <0.001 | <0.001 | <0.001 | |||
| Suicidal Ideation Score | r | 0.466 | 0.395 | −0.504 | −0.477 | −0.440 | 1.000 | |
| p | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | |||
3.4 Moderating Role of Resilience Dimensions in the Relationship between Depression and Suicidal Ideation among Standardized Residency Trainees
When tenacity and strength were entered as moderators:
In Model 1, depression was significantly and independently associated with suicidal ideation (β = 0.394, t = 4.905, p < 0.001). In Model 3, after including interaction terms, the explained variance increased to 35.40% and 32.70%, respectively, with additional ΔR2 values of 3.10% and 3.40%. Significant negative moderating effects were found for both dimensions (β = –0.196, t = –2.497, p = 0.014; β = –0.204, t = –2.570, p = 0.011) (Table 3 and Table 4).
When optimism was examined as a moderator, and household income was controlled:
Depression remained a significant and independently associated with suicidal ideation (β = 0.394, t = 4.976, p < 0.001). In Model 3, after including the interaction term, the variance explained reached 30.70%, with a ΔR2 of 0.035. A significant negative moderating effect of optimism was observed (β = –0.211, t = –2.596, p = 0.011) (Table 5).
The simple slope analysis demonstrated that when different dimensions of resilience were at a low level (Mean − 1 SD [standard deviation]), the slopes were noticeably steeper, indicating that the effect of depression on suicidal ideation was stronger. In contrast, when different dimensions of resilience were at a high level (Mean + 1 SD), the slopes were noticeably flatter, suggesting that the effect of depression on suicidal ideation was weaker (Fig. 2).
Table 3: Moderating effect of tenacity on the depression-suicidal ideation relationship.
| Variable | Model 1 | Model 2 | Model 3 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| β | t | p | β | t | p | β | t | p | |
| Depression | 0.394 | 4.905 | <0.001 | 0.279 | 3.730 | <0.001 | 0.354 | 4.463 | <0.001 |
| Resilience (Tenacity) | −0.426 | −5.683 | <0.001 | −0.358 | −4.573 | <0.001 | |||
| Depression * Resilience (Tenacity) | −0.196 | −2.497 | 0.014 | ||||||
| R2 | 0.155 | 0.323 | 0.354 | ||||||
| F Value | 24.054 | 31.046 | 23.609 | ||||||
| ΔR2 | 0.155 | 0.168 | 0.031 | ||||||
Table 4: Moderating effect of strength on the depression-suicidal ideation relationship.
| Variable | Model 1 | Model 2 | Model 3 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| β | t | p | β | t | p | β | t | p | |
| Depression | 0.394 | 4.905 | <0.001 | 0.283 | 3.672 | <0.001 | 0.368 | 4.467 | <0.001 |
| Resilience (Strength) | −0.387 | −5.029 | <0.001 | −0.342 | −4.42 | <0.001 | |||
| Depression * Resilience (Strength) | −0.204 | −2.57 | 0.011 | ||||||
| R2 | 0.155 | 0.293 | 0.327 | ||||||
| F Value | 24.054 | 26.904 | 20.91 | ||||||
| ΔR2 | 0.155 | 0.138 | 0.034 | ||||||
Table 5: Moderating effect of optimism on the depression–suicidal ideation relationship.
| Variable | Model 1 | Model 2 | Model 3 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| β | t | p | β | t | p | β | t | p | |
| Monthly Household Income | −0.167 | −2.111 | 0.037 | −0.073 | −0.945 | 0.346 | −0.045 | −0.598 | 0.551 |
| Depression | 0.394 | 4.976 | <0.001 | 0.325 | 4.297 | <0.001 | 0.406 | 5.053 | <0.001 |
| Resilience (Optimism) | −0.35 | −4.456 | <0.001 | −0.297 | −3.726 | <0.001 | |||
| Depression * Resilience (Optimism) | −0.211 | −2.596 | 0.011 | ||||||
| R2 | 0.183 | 0.276 | 0.307 | ||||||
| F Value | 14.574 | 17.745 | 15.585 | ||||||
| ΔR2 | 0.183 | 0.109 | 0.035 | ||||||
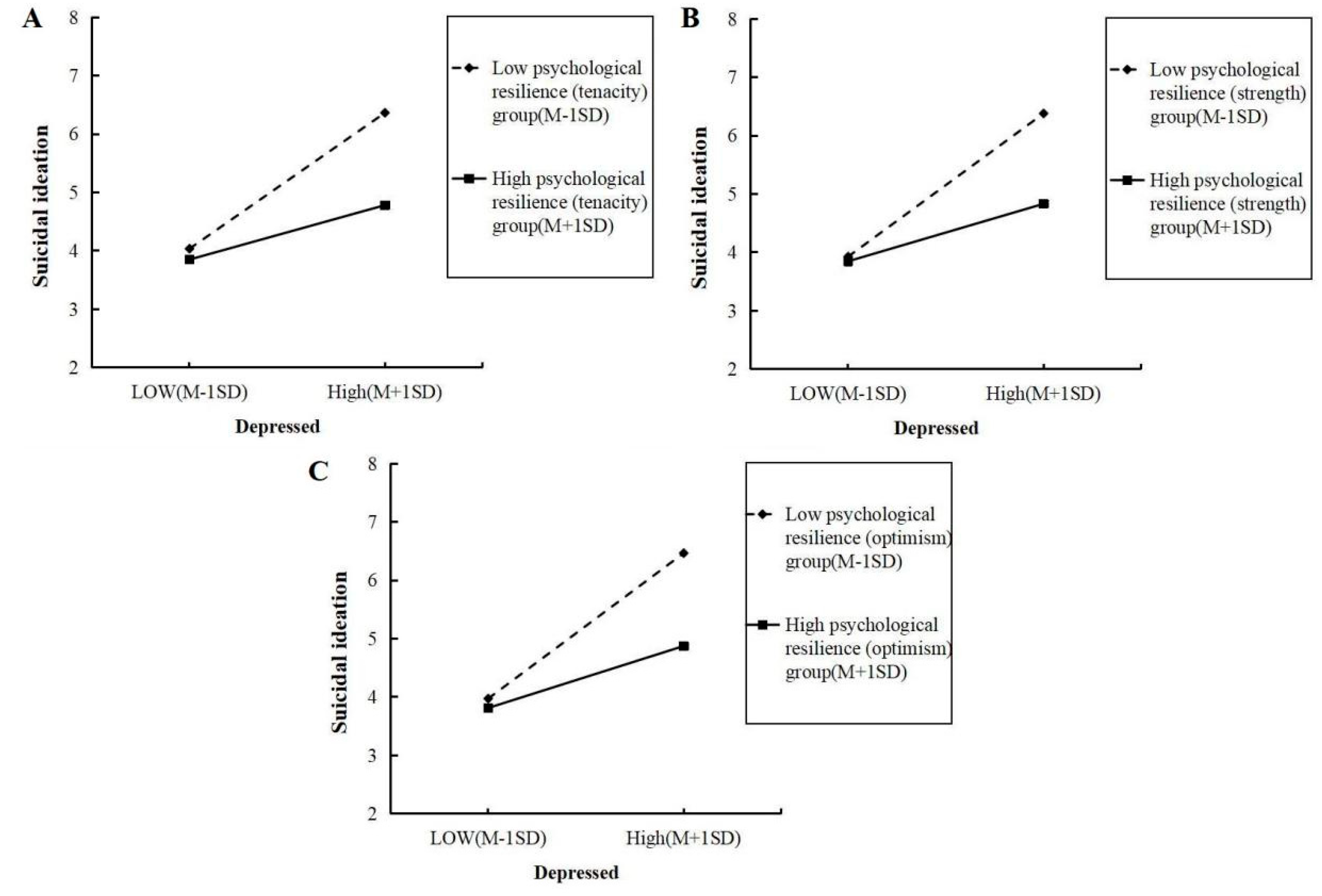
Figure 2: Simple slope plot of the moderating effects of tenacity, strength, and optimism on the relationship between depression and suicidal ideation.
3.5 Moderating Roles of Different Dimensions of Resilience in the Association between Anxiety and Suicidal Ideation among Standardized Residency Trainees
When tenacity and strength were entered as moderators:
In Model 1, anxiety was significantly and independently associated with suicidal ideation (β = 0.318, t = 3.844, p < 0.001). In Model 3, after including the interaction terms of anxiety with resilience (tenacity and strength), the model explained 30.50% and 18.355% of the variance in suicidal ideation, respectively. The change in explained variance (ΔR2) was 0.0210 and 0.0270, respectively. The interaction between anxiety and tenacity was not statistically significant (β = –0.162, t = –1.982, p = 0.050), indicating that tenacity was not a significant moderator of the association between anxiety and suicidal ideation. In contrast, the interaction between anxiety and strength was significant (β = –0.178, t = –2.219, p = 0.028), indicating a negative moderating association (Table 6 and Table 7).
When optimism was examined as a moderator, and household income was controlled:
In Model 1, anxiety remained significantly and independently associated with suicidal ideation (β = 0.346, t = 4.23, p < 0.001). After adding the interaction term between anxiety and optimism in Model 3, the model explained 29.3% of the variance in suicidal ideation, with an increase of ΔR2 = 2.70%. Optimism significantly moderated the association between anxiety and suicidal ideation in a negative direction (β = –0.188, t = –2.226, p = 0.028) (Table 8).
The simple slope analysis (Fig. 3) showed that when resilience (strength and optimism) was at a low level (Mean − 1 SD), the slopes were steeper, indicating a stronger positive association between anxiety and suicidal ideation. Conversely, when resilience (strength and optimism) was at a high level (Mean + 1 SD), the slopes were flatter, indicating a weaker association between anxiety and suicidal ideation.
Table 6: Moderating role of tenacity in the association between anxiety and suicidal ideation among residency physicians.
| Variable | Model 1 | Model 2 | Model 3 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| β | t | p | β | t | p | β | t | p | |
| Anxiety | 0.318 | 3.844 | <0.001 | 0.224 | 2.991 | 0.003 | 0.286 | 3.556 | 0.001 |
| Resilience (Tenacity) | −0.455 | −6.071 | <0.001 | −0.4 | −5.048 | <0.001 | |||
| Anxiety * Resilience (Tenacity) | −0.162 | −1.982 | 0.050 | ||||||
| R2 | 0.094 | 0.289 | 0.305 | ||||||
| F Value | 14.774 | 27.834 | 20.284 | ||||||
| ΔR2 | 0.101 | 0.198 | 0.021 | ||||||
Table 7: Moderating role of strength in the association between anxiety and suicidal ideation among residency physicians.
| Variable | Model 1 | Model 2 | Model 3 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| β | t | p | β | t | p | β | t | p | |
| Anxiety | 0.318 | 3.844 | <0.001 | 0.235 | 3.078 | 0.003 | 0.299 | 3.713 | <0.001 |
| Resilience (Strength) | −0.422 | −5.529 | <0.001 | −0.377 | −4.836 | <0.001 | |||
| Anxiety * Resilience (Strength) | −0.178 | −2.219 | 0.028 | ||||||
| R2 | 0.094 | 0.261 | 0.283 | ||||||
| F Value | 14.774 | 24.337 | 18.355 | ||||||
| ΔR2 | 0.101 | 0.171 | 0.027 | ||||||
Table 8: Moderating role of optimism in the association between anxiety and suicidal ideation among residency physicians.
| Variable | Model 1 | Model 2 | Model 3 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| β | t | p | β | t | p | β | t | p | |
| Monthly Household Income | −0.211 | −2.583 | 0.011 | −0.104 | −1.307 | 0.193 | −0.084 | −1.058 | 0.292 |
| Anxiety | 0.346 | 4.23 | <0.001 | 0.281 | 3.626 | <0.001 | 0.35 | 4.249 | <0.001 |
| Resilience (Optimism) | −0.367 | −4.599 | <0.001 | −0.312 | −3.803 | <0.001 | |||
| Anxiety * Resilience (Optimism) | −0.188 | −2.226 | 0.028 | ||||||
| R2 | 0.145 | 0.266 | 0.293 | ||||||
| F Value | 11.044 | 15.555 | 13.263 | ||||||
| ΔR2 | 0.145 | 0.12 | 0.027 | ||||||
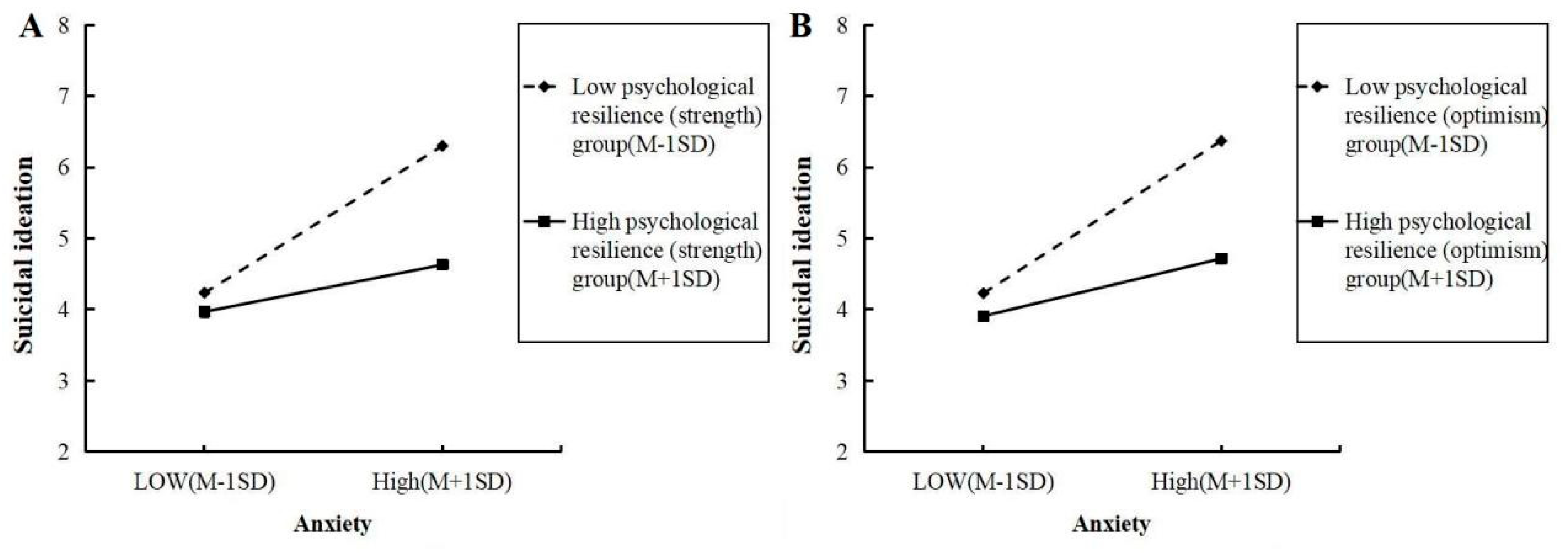
Figure 3: Simple slope plots for the moderating roles of strength and optimism in the anxiety–suicidal ideation relationship.
4.1 Main Findings and Their Implications
Multiple factors have been identified as influencing the occurrence of suicidal ideation in physicians, including demographic characteristics, psychological vulnerabilities, and social stressors. Among these, psychological factors, particularly depression and anxiety, have consistently been linked to elevated suicide risk in medical professionals [7,8]. In the present study, a questionnaire-based survey was conducted to explore how depressive and anxiety symptoms are associated with suicidal ideation among standardized residency trainees. The findings revealed significant associations between both depression and anxiety and suicidal ideation. As standardized residency trainees serve as a crucial reserve workforce in China’s healthcare system, a deeper understanding of the potential pathways linking depression and anxiety with suicidal ideation is of significant importance for improving healthcare quality and building a stronger medical workforce in China.
Individual resilience can be conceptualized along three dimensions: tenacity, strength, and optimism. Tenacity refers to an individual’s ability to remain calm, persistent, and in control in the face of adversity; strength involves the capacity to recover and grow from setbacks or traumatic experiences; optimism reflects a tendency to interpret experiences positively and to trust in both personal and external resources [21,22,23]. This study specifically examined how these three dimensions of resilience moderate the relationships between depression, anxiety, and suicidal ideation. All three dimensions were significantly associated with lower levels of suicidal ideation, particularly in attenuating the positive association between depressive symptoms and suicidal ideation. In other words, higher resilience scores were associated with lower reported levels of suicidal intent, regardless of depressive severity. These findings were consistent with our research hypothesis that psychological distress would be positively associated with suicidal ideation and that resilience—particularly strength and optimism—would buffer these associations. These results were consistent with our research hypothesis. In the present study, tenacity was not found to moderate the relationship between anxiety and suicidal ideation among standardized residency trainees, whereas strength and optimism were associated with weaker positive associations between anxiety and suicidal ideation. Individuals with higher strength and optimism tended to report lower levels of suicidal ideation, even when anxiety symptoms were elevated. Drawing on the buffering hypothesis of the psychological resilience framework [24,25] and the cognitive-behavioral theoretical framework [26,27], several possible interpretations of these associations are proposed.
First, Depression is typically characterized by motivational deficits [28,29]. Individuals with high tenacity may show greater capacity to maintain functioning under depressive states [30]. maintaining basic functioning and preventing total psychological collapse. Those with higher strength may interpret depressive experiences more adaptively, viewing them as opportunities for growth rather than signs of personal failure. Individuals with higher optimism may be more inclined to engage in problem-solving and help-seeking behaviors, which could be associated with lower levels of suicidal ideation [31]. Second, anxiety is characterized by a perceived lack of control and hypervigilance [32,33]. Tenacity, which emphasizes persistence and tolerance, may be less strongly associated with reduced anxiety-related distress. In contrast, individuals with high levels of strength and optimism may perceive anxiety-inducing situations as more manageable and tend to adopt more adaptive emotion-regulation strategies.
This study revealed a significant association between family monthly income per capita and the optimism dimension of resilience among trainees, suggesting that socioeconomic status may be associated with variations in this psychological characteristic. To account for this potential confounder, subsequent analyses controlled for family income. The results showed that even after controlling for income, both depressive and anxiety symptoms remained significantly associated with suicidal ideation. Moreover, optimism continued to exhibit a significant moderating association, indicating that its moderating role remained stable. This suggests that higher optimism may be associated with more positive cognition and a greater sense of hope despite financial pressure, which could relate to lower levels of suicidal ideation.
The differential moderating roles of resilience dimensions highlight the need to move beyond one-size-fits-all approaches. Future studies and training programs may consider developing tailored resilience-building strategies aligned with the specific emotional challenges faced by standardized residency trainees.
4.2 Comparison with Previous Studies
While previous research has consistently documented the associative role of psychological resilience in mental health—such as its moderating role in the relationships between stress and anxiety [34] and between adversity and depression [35,36]—the present study extends this body of evidence in two important ways. First, we identified a similar moderating association linking anxiety and depression with suicidal ideation. Second, by moving beyond a unitary construct, this study provided a more nuanced understanding through the distinct moderating roles of the tenacity, strength, and optimism dimensions of resilience. This refined approach offers a more comprehensive depiction of how resilience is associated with emotional distress, thereby enriching the existing literature.
4.3 Study Strengths and Limitations
The strengths of this study lie in its pioneering examination of the moderating roles of resilience—across its distinct dimensions of tenacity, strength, and optimism—in the associations between depression, anxiety, and suicidal ideation among medical residents. We applied hierarchical regression analysis with simple slope tests to verify the significance and stability of these moderating associations, thereby enhancing the reliability and validity of our findings. The results provide preliminary theoretical insights that may inform the development of targeted psychological strategies for this population and contribute to a better understanding of the multidimensional associations between resilience and mental health.
However, this study has several limitations. First, the cross-sectional design precludes the determination of causal relationships among the variables. Second, the sample size was limited and primarily drawn from a specific regional cohort of standardized residency trainees, which may restrict the generalizability of the findings. Third, the reliance on self-reported measures introduces the potential for response biases, such as social desirability. Fourth, given resource and feasibility constraints (budget, personnel, and time), this study focuses on individual-level psychological characteristics. Environmental and contextual factors typically require multi-source or longitudinal measurement and larger samples, which exceed the resources available at this stage; accordingly, they were not included in the analyses.
Based on the aforementioned limitations, future research could be explored in the following directions: (1) Optimization of research design: Longitudinal cohort studies or diary sampling methods are recommended to clarify causal relationships and temporal dynamics between variables. (2) Expansion of sample scope: Multi-center, large-scale collaborative surveys should be conducted, covering standardized residency trainees from different regions, hospital tiers, and specialties to enhance the representativeness and generalizability of the findings. (3) Integration of multi-level variables: Beyond focusing on individual psychological traits, future studies should systematically investigate the independent and interactive effects of organizational environmental factors and socio-contextual factors within the pathway linking depression, anxiety, and suicidal ideation.
Resilience (including toughness, strength, and optimism) was found to be an important psychological correlate of better mental health among standardized residency trainees. In practical terms, healthcare institutions may consider promoting physicians’ coping skills and resilience through regular mental health assessments, resilience-oriented training, and emotional management programs. Additionally, healthcare management may place greater emphasis on optimizing the work environment, ensuring reasonable work–rest arrangements, and providing adequate psychological support to help alleviate mental stress. Future policy development may place greater emphasis on integrating mental health education and resilience training into standardized residency programs, thereby contributing to a more comprehensive psychological support system for the physician community.
Acknowledgement:
Funding Statement: This work was supported by Jiangsu Cancer Hospital Science and Technology Development Fund Project (NO. XHMS202404); Nanjing Medical Science and Technology Development Fund Project (GBX22289).
Author Contributions: Jie Zhang, Xiaoxu Zhi, Lihai Chen and Minhao Zhang were involved in the study design, data analysis, and manuscript drafting. Jiahui Chen and Paerhati Halisa participated in the data collection and manuscript revision. All authors reviewed the results and approved the final version of the manuscript.
Availability of Data and Materials: The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval: All procedures performed in this study involving human participants were in accordance with the Declaration of Helsinki. Ethical approval for this study was granted by the Ethics Committee of Nanjing First Hospital (Ethical Approval No.: KY20250728-KS-02).
Informed Consent: Informed consent was taken from all the participants.
Conflicts of Interest: The authors declare no conflicts of interest to report regarding the present study.
References
1. Li Z , Wu M , Zhang X , Yan K , Wang X , Xu H , et al. Interrelationships of stress, burnout, anxiety, depression, quality of life and suicidality among Chinese residents under standardized residency training: a network analysis. Ann Med. 2024; 56( 1): 2433030. doi:10.1080/07853890.2024.2433030. [Google Scholar] [CrossRef]
2. Mata DA , Ramos MA , Bansal N , Khan R , Guille C , Di Angelantonio E , et al. Prevalence of depression and depressive symptoms among resident physicians: a systematic review and meta-analysis. JAMA. 2015; 314( 22): 2373– 83. doi:10.1001/jama.2015.15845. [Google Scholar] [CrossRef]
3. Chen L , Zhao Z , Wang Z , Zhou Y , Zhou X , Pan H , et al. Prevalence and risk factors for depression among training physicians in China and the United States. Sci Rep. 2022; 12( 1): 8170. doi:10.1038/s41598-022-12066-y. [Google Scholar] [CrossRef]
4. de Mélo Silva Júnior ML , Valença MM , Rocha-Filho PAS . Individual and residency program factors related to depression, anxiety and burnout in physician residents—a Brazilian survey. BMC Psychiatry. 2022; 22( 1): 272. doi:10.1186/s12888-022-03916-0. [Google Scholar] [CrossRef]
5. Obeng Nkrumah S , Adu MK , Agyapong B , da Luz Dias R , Agyapong VIO . Prevalence and correlates of depression, anxiety, and burnout among physicians and postgraduate medical trainees: a scoping review of recent literature. Front Public Health. 2025; 13: 1537108. doi:10.3389/fpubh.2025.1537108. [Google Scholar] [CrossRef]
6. Wang J , Liu M , Bai J , Chen Y , Xia J , Liang B , et al. Prevalence of common mental disorders among medical students in China: a systematic review and meta-analysis. Front Public Health. 2023; 11: 1116616. doi:10.3389/fpubh.2023.1116616. [Google Scholar] [CrossRef]
7. Robbins-Welty G , Nakatani M , Song YK , Riordan P , Pieper C , Price M , et al. Psychiatry resident physicians experience personal and professional grief, burnout and depression: results from a national survey. Am J Hosp Palliat Care. 2025; 42( 3): 296– 9. doi:10.1177/10499091241256106. [Google Scholar] [CrossRef]
8. Keuch L , Pukas L , Rabkow N , Ehring E , Kindt T , Rehnisch C , et al. Beck’s depression inventory II suicidal ideation in medical students–prevalence and associated factors. Int J Med Stud. 2023; 11( 1): 38– 44. doi:10.5195/ijms.2023.1434. [Google Scholar] [CrossRef]
9. Rátiva Hernández NK , Carrero-Barragán TY , Ardila AF , Rodríguez-Salazar JD , Lozada-Martinez ID , Velez-Jaramillo E , et al. Factors associated with suicide in physicians: a silent stigma and public health problem that has not been studied in depth. Front Psychiatry. 2023; 14: 1222972. doi:10.3389/fpsyt.2023.1222972. [Google Scholar] [CrossRef]
10. Yang XL , Yang CY , Chen PY , Sun XY , Wang Y . The relationship between self-regulation orientation and depression, anxiety symptoms, and suicide risk in medical students. Chin J Sch Health. 2020; 41: 1354– 7. (In Chinese). [Google Scholar]
11. Menon NK , Shanafelt TD , Sinsky CA , Linzer M , Carlasare L , Brady KJS , et al. Association of physician burnout with suicidal ideation and medical errors. JAMA Netw Open. 2020; 3( 12): e2028780. doi:10.1001/jamanetworkopen.2020.28780. [Google Scholar] [CrossRef]
12. Tan Y , Wang J , Chen H , Yang M , Zhu N , Yuan Y . Exploring the cultivation of psychological resilience in medical students from the perspective of doctor-patient relationship. Med Teach. 2024; 46( 11): 1511– 5. doi:10.1080/0142159X.2023.2295793. [Google Scholar] [CrossRef]
13. Zhang P , Tu CP , Zhang LG , Wang P . The relationship between depression, anxiety and psychological resilience among science and engineering college students. J Beijing Univ Posts Telecommun. 2024; 26: 112– 20. (In Chinese). [Google Scholar]
14. Okechukwu FO , Ogba KTU , Nwufo JI , Ogba MO , Onyekachi BN , Nwanosike CI , et al. Academic stress and suicidal ideation: moderating roles of coping style and resilience. BMC Psychiatry. 2022; 22( 1): 546. doi:10.1186/s12888-022-04063-2. [Google Scholar] [CrossRef]
15. Kumar SA , Hein CL , DiLillo D , Pietrzak RH . Resilience to suicidal ideation among U.S. military veterans with posttraumatic stress: results from the national health and resilience in veterans study. Mil Behav Health. 2022; 10( 4): 328– 37. doi:10.1080/21635781.2021.2015019. [Google Scholar] [CrossRef]
16. Min JA , Lee CU , Chae JH . Resilience moderates the risk of depression and anxiety symptoms on suicidal ideation in patients with depression and/or anxiety disorders. Compr Psychiatry. 2015; 56: 103– 11. doi:10.1016/j.comppsych.2014.07.022. [Google Scholar] [CrossRef]
17. Wu L , Tan Y , Liu Y . Factor structure and psychometric evaluation of the Connor-Davidson resilience scale in a new employee population of China. BMC Psychiatry. 2017; 17( 1): 49. doi:10.1186/s12888-017-1219-0. [Google Scholar] [CrossRef]
18. Zhang J , Wu ZY , Fang G , Li J , Han BX , Chen ZY . Establishment of national urban norms for the depression scale of the epidemiological investigation center. Chin J Ment Health. 2010; 24: 139– 43. (In Chinese). [Google Scholar]
19. Zung WW . A rating instrument for anxiety disorders. Psychosomatics. 1971; 12( 6): 371– 9. doi:10.1016/S0033-3182(71)71479-0. [Google Scholar] [CrossRef]
20. Li XY , Fei LP , Zhang YL , Xu D , Tong YS , Yang FD , et al. Reliability and validity of the Chinese version of beck scate for suicide ideation (BSI-CV) among university students. Chin Ment Health J. 2011; 25( 11): 862– 6. (In Chinese). [Google Scholar]
21. Wang Y , Chen Y , Xu J , Chen H , Gao J . Association between resilience and frailty among Chinese older adults. Front Psychiatry. 2022; 13: 948958. doi:10.3389/fpsyt.2022.948958. [Google Scholar] [CrossRef]
22. Turan N , Canbulat Ş . The effectiveness of the training program on accepting and expressing emotions on the psychological resilience and depression levels of nurses: a two-year follow-up study. Arch Psychiatr Nurs. 2023; 44: 1– 7. doi:10.1016/j.apnu.2023.03.002. [Google Scholar] [CrossRef]
23. Turkey HMKÜ , İşgör İY , Yılmaz Y , Laçin BGD . The prediction of psychological resilience by fear of happiness and ruminative thoughts. Educ Q Rev. 2022; 5( 3): 195– 206. doi:10.31014/aior.1993.05.03.538. [Google Scholar] [CrossRef]
24. Cheng J , Zhao YY , Wang J , Sun YH . Academic burnout and depression of Chinese medical students in the pre-clinical years: the buffering hypothesis of resilience and social support. Psychol Health Med. 2020; 25( 9): 1094– 105. doi:10.1080/13548506.2019.1709651. [Google Scholar] [CrossRef]
25. Troy AS , Willroth EC , Shallcross AJ , Giuliani NR , Gross JJ , Mauss IB . Psychological resilience: an affect-regulation framework. Annu Rev Psychol. 2023; 74: 547– 76. doi:10.1146/annurev-psych-020122-041854. [Google Scholar] [CrossRef]
26. Salkovskis PM , Warwick HM . Morbid preoccupations, health anxiety and reassurance: a cognitive-behavioural approach to hypochondriasis. Behav Res Ther. 1986; 24( 5): 597– 602. doi:10.1016/0005-7967(86)90041-0. [Google Scholar] [CrossRef]
27. Diefenbach GJ , Lord KA , Stubbing J , Rudd MD , Levy HC , Worden B , et al. Brief cognitive behavioral therapy for suicidal inpatients: a randomized clinical trial. JAMA Psychiatry. 2024; 81( 12): 1177. doi:10.1001/jamapsychiatry.2024.2349. [Google Scholar] [CrossRef]
28. Xing TY , Wei C , Wen HY , Wang X . The relationship between anxiety and social interaction in college students. Insight·Si. 2025; 8: 60– 2. (In Chinese). doi:10.20122/j.cnki.2097-0536.2025.08.007. [Google Scholar] [CrossRef]
29. Fossati P , Ergis AM , Allilaire JF . Neuropsychologie des troubles des fonctions exécutives dans la dépression: une revue de la littérature [Executive functioning in unipolar depression: a review]. Encephale. 2002; 28: 97– 107. (In French). [Google Scholar]
30. Kutcher AM , Byon HD , Esquivel JH . Depression, anxiety, and resilience: the association of emotions with self-care in patients with heart failure. J Cardiovasc Nurs. 2024; 39( 3): E72– 9. doi:10.1097/JCN.0000000000001049. [Google Scholar] [CrossRef]
31. Pinto TM , Campos FM Jr , Laurence PG , de Oliveira Serpa AL , Macedo EC . Resilience, life satisfaction, and optimism as protective factors against depressive symptoms among adolescents during the COVID-19 pandemic. Psicologia Teoria E Prática. 2024; 26( 2): 1– 14. doi:10.5935/1980-6906/eptpcp15556.en. [Google Scholar] [CrossRef]
32. Chen M , Lyu DS , Wang Z , Hou Y . Effect of target characteristics on prospective memory in patients with depressive disorder. Sichuan Ment Health. 2025; 38( 1): 14– 21. (In Chinese). [Google Scholar]
33. Diamond GM , Lipsitz JD , Fajerman Z , Rozenblat O . Ongoing traumatic stress response (OTSR) in Sderot, Israel. Prof Psychol Res Pract. 2010; 41( 1): 19– 25. doi:10.1037/a0017098. [Google Scholar] [CrossRef]
34. Schmuck J , Hiebel N , Kriegsmann-Rabe M , Schneider J , Matthias JK , Erim Y , et al. Individual stress burden and mental health in health care workers during the COVID-19 pandemic: moderating and mediating effects of resilience. Int J Environ Res Public Health. 2022; 19( 11): 6545. doi:10.3390/ijerph19116545. [Google Scholar] [CrossRef]
35. Chang JJ , Ji Y , Li YH , Yuan MY , Su PY . Childhood trauma and depression in college students: mediating and moderating effects of psychological resilience. Asian J Psychiatr. 2021; 65: 102824. doi:10.1016/j.ajp.2021.102824. [Google Scholar] [CrossRef]
36. Luo S , Zhang Y , Wang P , Yang Z , Zheng J , Wang Z , et al. The moderating role of resilience in the association between workload and depressive symptoms among radiology residents in China: results from a nationwide cross-sectional study. Eur Radiol. 2024; 34( 1): 695– 704. doi:10.1007/s00330-023-10021-7. [Google Scholar] [CrossRef]
Cite This Article
 Copyright © 2026 The Author(s). Published by Tech Science Press.
Copyright © 2026 The Author(s). Published by Tech Science Press.This work is licensed under a Creative Commons Attribution 4.0 International License , which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
 Downloads
Downloads
 Citation Tools
Citation Tools