
 Submit a Paper
Submit a Paper Propose a Special lssue
Propose a Special lssue Open Access
Open Access
ARTICLE

Compliance with Three Movement Behaviors and Psychological Health among Adults with Diabetes
1 School of Liberal Arts, Shenzhen City Polytechnic, Shenzhen, China
2 Department of Kinesiology, Texas A&M University Texarkana, Texarkana, TX, USA
3 College of Wushu and Dance, Shenyang Sport University, Shenyang, China
4 Physical Education Unit, School of Humanities and Social Science, Chinese University of Hong Kong-Shenzhen, Shenzhen, China
5 Physical Activity and Health Promotion Laboratory, Chinese University of Hong Kong-Shenzhen, Shenzhen, China
* Corresponding Author: Yanjie Zhang. Email:
International Journal of Mental Health Promotion 2026, 28(2), 5 https://doi.org/10.32604/ijmhp.2026.072912
Received 06 September 2025; Accepted 20 January 2026; Issue published 27 February 2026
 View Full Text
View Full Text Download PDF
Download PDFAbstract
Objectives: 24-h movement behaviors (24-HMB), encompassing physical activity, sedentary behavior, and sleep duration, are increasingly regarded as interrelated and important factors for mental health. However, evidence on the comprehensive association of these behaviors with mental health in adults with diabetes in developing countries remains scarce. This study examined the association between 24-HMB guidelines and psychological health among adults with diabetes in developing countries. Methods: Data were retrieved from the World Health Organization’s study on Global Aging and Adult Health Survey dataset. Adults (N = 1905) diagnosed with diabetes from five low-and middle-income countries were included. The exposure of interest was adherence to 24-HMB guidelines, depression, cognition, and quality of life (QoL). Multiple logistic and multiple linear regression analyses were used to examine the association between meeting 24-HMB guidelines and depression, cognition, and QoL, respectively. Results: This cross-sectional study revealed that 28.61% complied with all three 24-HMB guidelines. Diabetic patients who met more numbers of 24-HMB guidelines had lower depression risk (OR = 0.74, 95% CI: 0.61 to 0.91, p = 0.004), greater cognition (β = 0.42, 95% CI: 0.25 to 0.60, p < 0.001), and QoL (β = 1.30, 95% CI: 1.04 to 1.55, p < 0.001) with the non-compliant population. For specific combinations, meeting all three guidelines were significantly associated with lower odds of depression, improved cognitive function, and enhanced QoL (all p < 0.001). Conclusion: These findings support that meeting 24-HMB guidelines in a single or combined movement behaviors was significantly related to reduced risk of depression, enhanced cognitive function, and improved QoL among individuals with diabetes.Keywords
Supplementary Material
Supplementary Material FileDiabetes is a rapidly increasing chronic disease worldwide, exerting significant influence on premature mortality, disability rates, and healthcare expenditures [1,2]. According to estimates provided by the International Diabetes Federation (IDF) [3], the number of people with diabetes aged 20 to 79 years worldwide reached 537 million in 2021, and approximately 75% of these individuals lived in low- and middle-income countries (LMICs) [4]. The projected figures indicate that the global population of this demographic is expected to increase to 643 million by 2030 and further rise to 783 million by 2045 [3]. The prevalence of diabetes in LMICs has continued to rise, presenting a severe challenge to public health systems. Diabetes can lead to various physical complications, including an increased risk of cardiovascular disease, neurological dysfunction, and kidney damage, which further exacerbate the medical burden [5,6]. Moreover, diabetes is also accompanied by psychological health issues, for example, depression, cognitive impairment, and poor quality of life (QoL) [7,8]. When diabetes combines with mental health conditions, its management becomes significantly more complex. Specifically, comorbid depressive disorder may hinder the treatment outcome of diabetes by reducing medication adherence [9]. Furthermore, the common cognitive decline among diabetic patients weakens their ability to self-manage the disease [10,11]. From a pathological mechanism perspective, diabetes-induced insulin resistance can interfere with the insulin signaling pathway in the brain, thereby exacerbating cognitive dysfunction [12]. These factors are interrelated, forming a complex bidirectional influence mechanism. As a result, there is an urgent need to establish effective health lifestyle models to promote the psychological health outcomes of diabetic patients.
As three important behavioral dimensions of a healthy lifestyle, physical activity, sedentary behavior, and sleep duration are increasingly attracting the attention of scholars [13,14,15]. These three behaviors occupy the major part of the 24 h in a day. A large amount of evidence supports the positive effect of high levels of physical activity on alleviating symptoms of depression and anxiety [16,17]. Prolonged sedentary behavior has been independently associated with severe depression and anxiety [16,17]. Additionally, daily sleep durations shorter than 7 h or longer than 8 h are linked to an increased risk of depression and anxiety [18]. Historically, most research has only focused on the impact of a specific movement behavior on health outcomes, while neglecting the interrelationships among different movement behaviors and their joint effects.
With the continuous improvement of public health policies, numerous government agencies and professional organizations have established “24-HMB guidelines” targeted at different population groups. These guidelines recommend three core recommendations for adults: (1) achieving ≥150 min of moderate to vigorous physical activities per week; (2) limiting ≤8 h of sedentary time each day; (3) obtaining 7 to 9 h of sleep per night for those aged 18–64 years, or 7 to 8 h of sleep per night for those aged 65+ years [19]. Fundamentally, physical activity, sedentary behavior, and sleep duration collectively constitute the core components of each person’s 24-h daily behavior. These behaviors exhibit distinct compositional relationships, wherein a reduction in time allocated to one behavior necessarily implies an increase in time spent in at least one of the others. Currently, the release of the 24-HMB guidelines for adults has sparked academic interest in exploring the relationships between these guidelines and adult health outcomes. A cross-sectional study found that European adults who followed the 24-HMB guidelines had better blood pressure control [20]. Another recent study showed that following the 24-HMB guidelines was positively correlated with better physical and mental health among Chinese elderly people [21].
Although a growing body of research has examined the prevalence and benefits of adhering to 24-HMB guidelines in adults, there remains limited exploration of how this integrated approach applies to health outcomes in population living with chronic conditions, such as diabetes. Evidence suggests that individuals with diabetes often display insufficient physical activity and sleep duration, and elevated sedentary behavior [22,23]. These factors may exacerbate adverse clinical consequences, including depression, anxiety, overweight or obesity, disease-related complications, and impaired QoL. However, existing studies have largely focused on analysing individual movement behaviors in isolation rather than holistically, with limited research evaluating the synergistic benefits of adhering to 24-HMB guidelines in diabetes management [24,25,26]. To our knowledge, only four studies to date have investigated meeting 24-HMB guidelines and their beneficial impacts on diabetic patients. For example, Swindell et al. conducted a cross-sectional study by collecting 1462 adults from eight European countries with pre-diabetes. This study employed compositional isotemporal substitution modeling to evaluate how reallocating time across 24-HMB correlated with cardiometabolic risk markers [27]. Key findings revealed that substituting moderate to vigorous physical activity with any other movement behaviors within the 24-h cycle consistently worsened cardiometabolic risk profiles. In a large-scale prospective cohort study, García-Hermoso et al. [28] analyzed longitudinal data of 12,370 healthy adolescents aged 12–18 years from the National Longitudinal Study of Adolescent to Adult Health to investigate the preventive potential of meeting 24-HMB guidelines. Their findings found that adolescents adhering to all three 24-HMB guidelines exhibited a lower likelihood of developing type 2 diabetes mellitus in adulthood compared to non-adherent peers [28]. In parallel, Willems and colleagues utilized data from 1549 adults with diabetes from the Hoorn Diabetes Care System to determine the associations between 24-HMB guidelines adherence and cardiometabolic health. Their work highlighted the significance of adherence to 24-HMB in body mass index (BMI), waist circumference, high-density lipoprotein (HDL) cholesterol, and triglycerides [15]. A recent systematic review study reported that no studies have comprehensively explored how adherence to 24-HMB guidelines intersects with both glycemic control and psychosocial outcomes in adolescents living with diabetes [22].
While empirical evidence supports the integrative benefits of adhering to 24-HMB guidelines for physiological and psychological health outcomes in general populations, their translational potential remains underexplored in chronic disease management, particularly among individuals with diabetes living in LMICs. By emphasizing the importance of integrated physical activity, reduced sedentary behavior, and adequate sleep duration, this research addresses a critical gap in contextualizing 24-HMB strategies for diabetes care in resource-constrained settings. Specifically, our study aimed to investigate how adherence to 24-HMB guidelines associates with psychological health outcomes (depression, cognition, and QoL) among adults with diabetes in LMICs.
Public data from the World Health Organization (WHO) study on Global Ageing and Adult Health Survey (SAGE) (through https://apps.who.int/healthinfo/systems/surveydata/index.php/catalog/?page=1&ps=15) were used for the present study. This health survey was conducted in China, Ghana, India, the Russian Federation, and South Africa from 2007 to 2010. To some extent, these countries represent diverse geographical locations and varying levels of socioeconomic and demographic transition, and were considered as developing countries depending on the World Bank classification [29]. A multistage clustered sampling design was employed to collect nationally representative samples aged 18+ years and above in all countries. The stratification is based on the size of the first-level sampling units (e.g., regions) and the type of location (e.g., cities/rural areas) [14]. Researcher collected data through face-to-face structured interviews in participants’ homes. The interviews were conducted by professionally trained researchers using standardized questionnaires. In the interview, a combination of computer-assisted personal interviewing (CAPI) and paper-and-pencil methods was employed. To ensure comparability across countries, standardized translation procedures were implemented. The survey response rates were as follows: China (93%), Ghana (81%), India (68%), Russia (83%), and South Africa (75%). The SAGE study was approved by the Ethics Review Committee of the WHO and local research ethics review committees.
In this secondary data analysis, participants were included based on the following criteria: (1) age ≥ 18 years; (2) self-reported diagnosed diabetes or taking insulin or other blood sugar lowering medications; (3) complete data on movement behavior, depression, cognition, and QoL. As results, 1905 participants were included in the analysis.
2.2 Measures of 24-h Movement Behaviors
Physical activity was assessed by a series of questions according to the Global Physical Activity Questionnaire (GPAQ, version 2). This questionnaire was developed by the WHO and its consistency has been assessed based on the measurement method using accelerometers [30]. The questions included frequency (number of days a week) and duration (amount of time a day) of moderate and vigorous physical activity in three dimensions: work, transport, and recreational activities during the past week [31]. The amount of physical activity was calculated by converting them into metabolic equivalent (MET) and measuring them in terms of minutes per week (MET-min/week). According to the recommendation of the WHO, 0 to 600 MET-min/week is categorized as insufficient physical activity. It was categorized as moderate level of physical activity when the rang is between 601 and 3000 MET-min/week; and more than 3000 MET-min/week is considered high level of physical activity [14]. The moderate and vigorous physical activity was determined to meet the recommended level of physical activity [14]. Sedentary behavior was measured using the GPAQ. Participants were asked to answer one question: “How much time do you usually spend sitting or reclining on a typical day? such as sitting at a desk, sitting with friends, travelling in car, bus, train, reading, playing cards or watching television.” [32]. Participants were classified within the “recommended sedentary behavior” group if they spent sitting time less than 8 h/day [31]. For sleep duration, participants responded the question “how many hours they slept on each of the preceding two nights” during the face-to-face interview. In line with previous sleep studies, the average duration values obtained from two consecutive nights were employed to calculate a comprehensive measure of sleep length [33,34]. The sleep duration of 7 to 9 h (for adults aged 18 to 64) and 7 to 8 h (for adults aged 65 and above) were considered to meet the requirements of the relevant guidelines, respectively. According to the Canadian 24-HMB guidelines [19], participants were categorized as 0 = meeting none of guidelines, 1 = meeting one of guidelines (physical activity guideline only, sedentary behavior guideline only, or sleep duration guideline only), 2 = meet two of guidelines (physical activity + sedentary behavior guidelines, sedentary behavior + sleep duration guidelines, or physical activity + sleep duration guidelines), and 3 = meeting all three guidelines (physical activity + sedentary behavior + sleep duration guidelines).
Depression was assessed using a series of symptomatic questions derived from the World Mental Health Survey version of the Composite International Diagnostic Interview (CIDI) [35]. The CIDI focuses on the presence, duration and frequency of core depressive symptoms, which enables the assessment and classification of depression to be standardized. These questions have consistent norms with the main diagnostic criteria and collect relevant information on participants’ recent and past experiences of depressive symptoms. Participants were asked to respond to a total of 18 items, indicating whether each depressive symptom had been present at any time during the past 12 months. The responses were recorded in a dichotomous format (yes = 1 or no = 0). Based on the algorithm outlined by Arokiasamy et al. [36], the assessment consisted of two sets of variables: Set A and Set B. Set A comprised items related to core symptoms, including depressed mood, anhedonia, reduced energy, and the duration of these symptoms. Set B consisted of additional depressive symptoms such as changes in appetite, psychomotor slowing, sleep disturbances, difficulties in concentration, and suicidal ideation. Detailed descriptions of the questions can be found in the Supplementary Materials (Supplementary file). Participants were classified as having experienced a major depressive episode in the past 12 months if they scored ≥2 from Set A and ≥4 from Set B, respectively [37]. The test of reliability for depression was high quality (Cronbach’s α = 0.97).
There were five cognitive performance tests, including immediate and delayed verbal recall, forward and backward digit span, and verbal fluency to test cognitive function [33]. The overall cognitive function score was derived from a composite of these five areas. For the immediate verbal recall test, participants were verbally told a list of 10 words by interviewers and were then instructed to recall as many words as possible within one minute. This task was repeated three times. The delayed recall ability was assessed by recollecting the word list. The digit span tasks involved repeating sequences of numbers, with progressively longer series being presented. The forward digit span score was determined by the length of the longest sequence correctly repeated without error. Similarly, the backward digit span test required participants to repeat new sequences of numbers in reverse order, with increasing difficulty. For the verbal fluency assessment, individuals were instructed to answer as many animals as possible within 60 s. The final score for language fluency was calculated by subtracting the number of incorrect answers from that of correct responses. An overall cognitive score was calculated using standardized z-scores, which were averaged across all five tests. Higher scores reflected better cognitive function [33]. The test of reliability for cognition was of high quality (Cronbach’s α = 0.83).
QoL was assessed using the 8-item WHO-QoL instrument. It involved measuring satisfaction across various aspects of life, including health, finances, interpersonal relationships, functional health, self-perception, and overall life satisfaction. Participants responded to each item on a 5-point Likert scale, ranging from 1 (not at all) to 5 (completely). The overall QoL score was calculated by summing the scores of the eight items, with higher scores indicating better QoL [38]. The test of reliability for QoL was good quality (Cronbach’s α = 0.71).
The control variables were identified according to the previous studies [14,39]. It included age, sex, education levels (no formal education, elementary school, high school, and college or above), marital status, chronic diseases, smoking status, drinking status, BMI, and residential area.
All statistical analyses in this cross-sectional study were conducted with STATA 18.0 (STATA Corporation, College Station, TX, USA). The sample characteristics were reported through descriptive statistical methods. The multivariable logistic regression model was fitted to examine the associations between meeting 24-HMB guidelines and depression, cognition, and QoL after controlling for all the control variables mentioned above (e.g., age, sex, and marital status). In the multivariable logistic regression models, meeting 24-HMB guidelines was categorized as a continuous variable (0, 1, 2, 3) and a categorical variable (none, physical activity, sedentary behavior, sleep duration, physical activity + sedentary behavior, physical activity + sleep duration, sedentary behavior + sleep duration, physical activity + sedentary behavior + sleep duration). The results of multivariable logistic regression models were presented with odds ratio (OR) and 95% confidence interval (CI). Statistical significance was set at p < 0.05.
The present study included 1905 diabetes adults with a mean age of 63.31 ± 10.30 years. The proportion of females was 57.59% (n = 1097). The majority of participants (45.09%) had 1–6 years of education, while 13.75% had no formal education. The sample included 69.24% (n = 1319) of married individuals and 76.59% of those living in urban areas. The detailed characteristics of the study sample are presented in Table 1.
Table 1: Sample characteristics in diabetes patients (N = 1905).
| Variables | n | Mean ± Standard Deviation/% |
|---|---|---|
| Age | 63.31 ± 10.30 | |
| Sex | ||
| Male | 808 | 42.41 |
| Female | 1097 | 57.59 |
| Body mass index (BMI) | 1905 | 27.34 ± 5.10 |
| Education (years) | ||
| 0 | 262 | 13.75 |
| 1–6 | 859 | 45.09 |
| 7–12 | 505 | 26.51 |
| >12 | 279 | 14.65 |
| Marital status | ||
| Married | 1319 | 69.24 |
| Unmarried | 586 | 30.76 |
| Residential areas | ||
| Rural | 446 | 23.41 |
| Urban | 1459 | 76.59 |
| Alcohol consumption | ||
| Yes | 796 | 41.78 |
| No | 1109 | 58.22 |
| Smoking | ||
| Never | 1337 | 70.18 |
| Current | 209 | 10.97 |
| Past | 359 | 18.85 |
| Number of chronic diseases | ||
| 1–2 | 1097 | 57.59 |
| ≥3 | 808 | 42.41 |
| Meeting 24-h movement guidelines | ||
| None | 93 | 4.88 |
| Sedentary behavior only | 349 | 18.32 |
| Sleep duration only | 63 | 3.31 |
| Physical activity only | 64 | 3.36 |
| Physical activity + sedentary behavior | 434 | 22.78 |
| Physical activity + sleep duration | 50 | 2.62 |
| Sedentary behavior + sleep duration | 307 | 16.12 |
| All three | 545 | 28.61 |
Regarding adherence to the 24-HMB guidelines, the proportion of adults who met all three guideline recommendations was 28.61%. The proportions of adults meeting the individual guidelines for physical activity, sedentary behavior, and sleep duration were 3.31%, 18.32%, and 3.36%, respectively. The proportions of adults who met the guidelines for physical activity and sedentary behavior, physical activity and sleep duration, and sedentary behavior and sleep duration were 22.78%, 2.62%, and 16.12%, respectively. The proportion of adults who did not meet any of the recommended guidelines was 4.88% (Fig. 1).
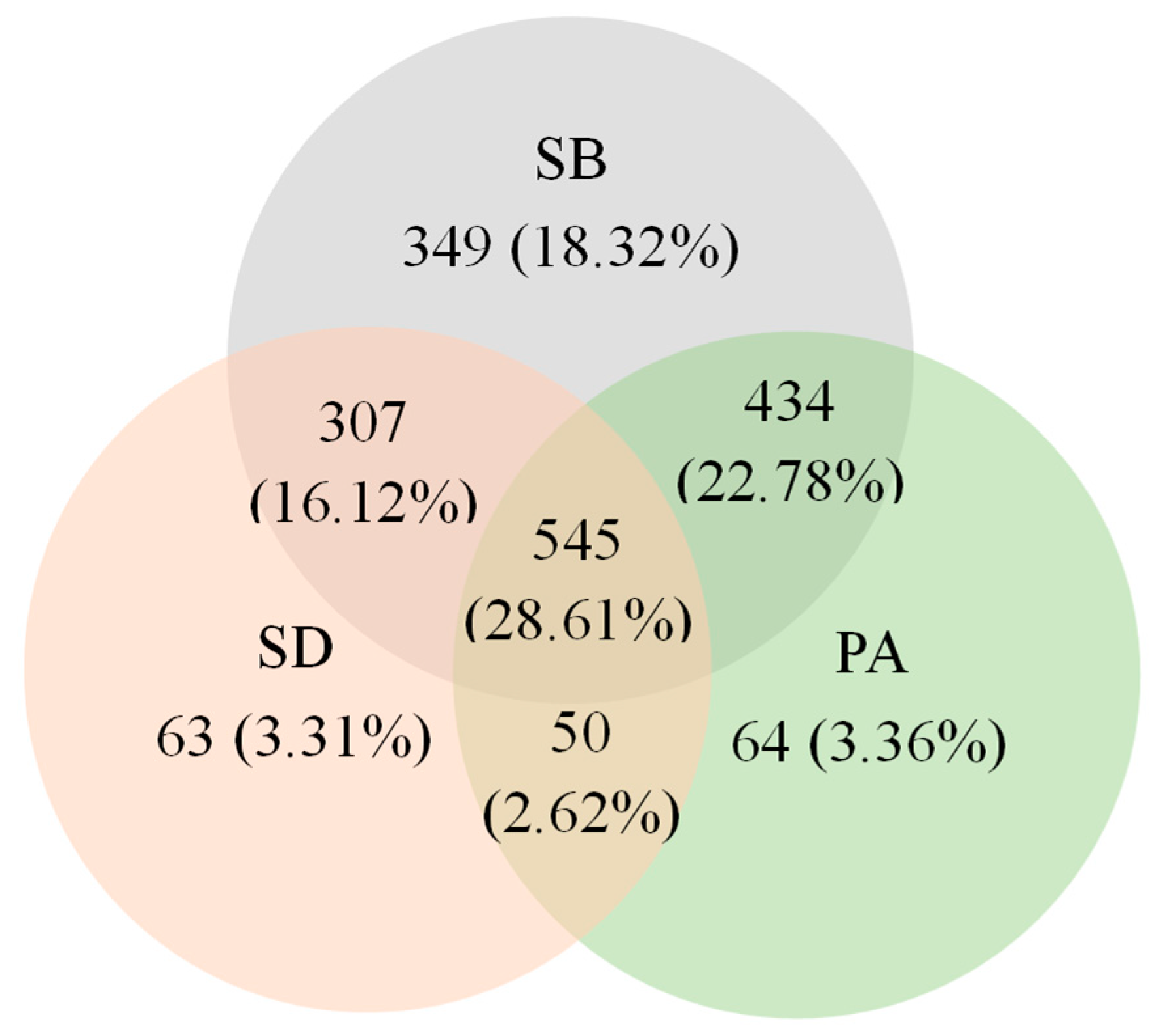
Figure 1: Venn diagram presenting proportions of adults with diabetes who met independent and integrated components of 24-h movement behavior guidelines. Abbreviations: SB, sedentary behavior; PA, physical activity; SD, sleep duration.
3.1 Association between Adherence to 24-HMB Guidelines and Depression
Table 2 presents the associations between meeting 24-HMB guidelines and depression among diabetes patients. Meeting the sleep guideline (OR = 0.16, 95% CI: 0.03 to 0.75, p = 0.02), sedentary behavior and sleep duration guidelines (OR = 0.34, 95% CI: 0.15 to 0.76, p < 0.001), all three guidelines (OR = 0.34, 95% CI: 0.16 to 0.70, p < 0.001) were significantly associated with lower odds of depression, respectively. For general combinations of guideline, meeting three guidelines (OR = 0.34, 95% CI: 0.16 to 0.70, p < 0.001) was significantly related to lower risk of depression. Moreover, each additional guideline met was associated with a reduced risk of depression (OR = 0.74, 95% CI: 0.61 to 0.91, p = 0.004), indicating that higher adherence to 24-HMB guidelines correlates with a lower likelihood of depression among diabetes patients.
Table 2: The association between meeting 24-HMB guidelines and depression.
| Meeting 24-HMB Guidelines | p | t | Odds Ratio | 95% CI | |
|---|---|---|---|---|---|
| Specific combinations | |||||
| None (Reference) | |||||
| SB | 0.23 | −1.20 | 0.64 | 0.31 | 1.32 |
| SD | 0.02 | −2.32 | 0.16 | 0.03 | 0.75 |
| PA | 0.50 | −0.68 | 0.71 | 0.27 | 1.89 |
| PA and SB | 0.20 | −1.30 | 0.63 | 0.31 | 1.27 |
| PA and SD | 0.19 | −1.31 | 0.45 | 0.13 | 1.50 |
| SB and SD | <0.001 | −2.62 | 0.34 | 0.15 | 0.76 |
| All three | <0.001 | −2.90 | 0.34 | 0.16 | 0.70 |
| General combinations | |||||
| None (Reference) | |||||
| 1 | 0.12 | −1.56 | 0.58 | 0.29 | 1.15 |
| 2 | 0.04 | −1.98 | 0.50 | 0.26 | 0.99 |
| 3 | <0.001 | −2.89 | 0.34 | 0.16 | 0.70 |
| Number of guidelines met | 0.004 | −2.88 | 0.74 | 0.61 | 0.91 |
3.2 Association between Adherence to 24-HMB Guidelines and Cognition
Table 3 illustrates the associations between meeting the 24-HMB guidelines and cognitive function among diabetes patients. Meeting the physical activity and sedentary behavior guidelines (β = 0.85, 95% CI: 0.12 to 1.56, p = 0.02), physical activity and sleep duration guidelines (β = 2.35, 95% CI: 1.29 to 3.42, p < 0.001), and all three guidelines (β = 0.93, 95% CI: 0.23 to 1.63, p < 0.001) were significantly associated with greater cognitive function, respectively. For general combinations of guideline, meeting two guidelines was significantly associated with better cognitive function (β = 0.89, 95% CI: 0.19 to 1.59, p < 0.001), and meeting all three guidelines was similarly associated with improved cognitive function (β = 1.09, 95% CI: 0.37 to 1.81, p = 0.003). Additionally, each additional guideline met was associated with a better cognitive function (β = 0.42, 95% CI: 0.25 to 0.60, p < 0.001), suggesting that greater adherence to 24-HMB guidelines is associated with improved cognitive function in diabetes patients.
Table 3: The association between meeting 24-HMB guidelines and cognition.
| Meeting 24-HMB Guidelines | p | t | β | 95% CI | ||
|---|---|---|---|---|---|---|
| Specific combinations | ||||||
| None (Reference) | ||||||
| SB | 0.42 | 0.81 | 0.29 | −0.42 | 1.00 | |
| SD | 0.92 | −0.11 | −0.05 | −1.06 | 0.96 | |
| PA | 0.79 | 0.27 | 0.13 | −0.84 | 1.11 | |
| PA and SB | 0.02 | 2.39 | 0.85 | 0.12 | 1.56 | |
| PA and SD | <0.001 | 4.30 | 2.35 | 1.29 | 3.42 | |
| SB and SD | 0.22 | 1.24 | 0.46 | −0.27 | 1.18 | |
| All three | <0.001 | 2.62 | 0.93 | 0.23 | 1.63 | |
| General combinations | ||||||
| None (Reference) | ||||||
| 1 | 0.59 | 0.54 | 0.20 | −0.52 | 0.91 | |
| 2 | <0.001 | 2.51 | 0.89 | 0.19 | 1.59 | |
| 3 | 0.003 | 2.66 | 1.09 | 0.37 | 1.81 | |
| Number of guidelines met | <0.001 | 4.75 | 0.42 | 0.25 | 0.60 | |
3.3 Association between Adherence to 24-HMB Guidelines and QoL
Table 4 presents the associations between adherence to the 24-h movement guidelines and QoL among diabetes patients. Meeting the sedentary behavior guideline (β = 2.54, 95% CI: 1.50 to 3.59, p < 0.001), physical activity guideline (β = 3.88, 95% CI: 2.45 to 5.30, p < 0.001), physical activity and sedentary behavior guidelines (β = 4.03, 95% CI: 3.01 to 5.06, p < 0.001), physical activity and sleep duration guidelines (β = 3.13, 95% CI: 1.56 to 4.71, p < 0.001), sedentary behavior and sleep duration guidelines (β = 3.92, 95% CI: 2.86 to 4.99, p < 0.001), and all three guidelines (β = 4.56, 95% CI: 3.54 to 5.58, p < 0.001) were all significantly related to higher QoL, respectively. For general combinations of guideline, meeting one guideline (β = 2.46, 95% CI: 1.43 to 3.49, p < 0.001), two guidelines (β = 4.01, 95% CI: 3.00 to 5.02, p < 0.001), and three guidelines (β = 4.69, 95% CI: 3.65 to 5.73, p < 0.001) was significantly associated with higher QoL, respectively. Additionally, there was a significant association between the overall number of guidelines met and higher QoL (β = 1.30, 95% CI: 1.04 to 1.55, p < 0.001), indicating that adherence to a greater number of movement guidelines is correlated with improved QoL among diabetes patients.
Table 4: The association between meeting 24-HMB guidelines and QoL.
| Meeting 24-HMB Guidelines | p | t | β | 95% CI | |
|---|---|---|---|---|---|
| Specific combinations | |||||
| None (Reference) | |||||
| SB | <0.001 | 4.79 | 2.54 | 1.50 | 3.59 |
| SD | 0.22 | 1.22 | 0.90 | −0.55 | 2.34 |
| PA | <0.001 | 5.32 | 3.88 | 2.45 | 5.30 |
| PA and SB | <0.001 | 7.70 | 4.03 | 3.01 | 5.06 |
| PA and SD | <0.001 | 3.90 | 3.13 | 1.56 | 4.71 |
| SBand SD | <0.001 | 7.23 | 3.92 | 2.86 | 4.99 |
| All three | <0.001 | 8.77 | 4.56 | 3.54 | 5.58 |
| General combinations | |||||
| None (Reference) | |||||
| 1 | <0.001 | 4.68 | 2.46 | 1.43 | 3.49 |
| 2 | <0.001 | 7.81 | 4.01 | 3.00 | 5.02 |
| 3 | <0.001 | 8.84 | 4.69 | 3.65 | 5.73 |
| Number of guidelines met | <0.001 | 10.12 | 1.30 | 1.04 | 1.55 |
The present study provides novel insights to examine the associations between adherence to 24-HMB guidelines and psychological health outcomes (depression, cognition, and QoL) among adults with diabetes. The major results of this study indicate that adhering to relevant guidelines has significant positive impacts, specifically manifested as a negative relationship between the number of guidelines adhered and the risk of depression, and a positive correlation with cognitive function levels. Compared with earlier works, although there are no published research specifically exploring the relationship between adherence to 24-HMB guidelines and depression, cognition, and QoL in adults with diabetes. Our findings are consistent with previous studies, in which adherence to 24-HMB guidelines is robustly associated with reduced symptoms of depression [17], better cognitive function [40,41], and improved QoL [18] in adults in the Americas (e.g., US, Brazil) and Asia (e.g., China, Republic of Korea). Therefore, these findings provided the new evidence that meeting 24-HMB guidelines maybe a significant strategy in the management of psychological health in patients with diabetes.
4.1 Adherence to 24-HMB Guidelines and Depression
In the current study, our results revealed a robust protective relationship between adherence to 24-HMB guidelines and depression risk in adults with diabetes. Notably, meeting sleep duration alone, sedentary behavior and sleep duration, and all three guidelines were significantly associated with lower odds of depression, respectively. Our findings are largely in line with the previous results that replacing sedentary behavior with sleep duration benefits the health of diabetic patients in UK [42]. These findings seem to underscore the critical role of adhering to sleep guidelines, which may have significant impactions for promoting mental health. The findings of the present study align with the point in previous studies, showing that adults living in developed countries with adequate sleep duration had lower odds of depressive symptom [43,44]. Sufficient sleep has been demonstrated to enhance emotional regulation, diminish stress levels, and improve overall mood. All of these are pivotal factors in mitigating the susceptibility to depression [45]. Del Pozo Cruz et al. [46] examined the association between movement behaviors (physical activity and sedentary behavior) and depressive symptoms among adults. They found that the increase in sedentary behavior (e.g., screen time) was associated with a higher prevalence of depression. By contrast, reducing sedentary behavior is beneficial for promoting mental health [46]. Taken together, the combination of meeting both sedentary behavior and sleep duration guidelines was significantly associated with lower odds of depression. The interrelationship between reducing sedentary time and achieving adequate sleep duration may have a synergistic impact on mental health, as these both factors can mutually enhance each other [47]. Moreover, previous studies have highlighted the importance of physical activity in regulating the mental health (e.g., depression) [48,49]. In addition to promoting reduced sedentary behavior and ensuring adequate sleep duration, it is worth noting that meeting all three guidelines can significantly decrease the odds of diabetes patients developing depression. Additionally, the observed total number of compliance guidelines was significantly associated with lower odds of depression, indicating a dose-response relationship. That is, the more guidelines followed, the lower the likelihood of developing depression. This finding emphasizes the holistic benefit of a balanced 24-HMB approach for mental health management in individuals with diabetes.
4.2 Adherence to 24-HMB Guidelines and Cognitive Function
The findings from the present study are helpful in determining the 24-HMB guidelines, which can bring significant benefits to the cognitive function of diabetic patients. Meeting the physical activity and sedentary behavior, physical activity and sleep, and all three guidelines were significantly associated with higher cognitive function, respectively. Of which, meeting physical activity and sleep guidelines was associated with the strongest effects on cognitive function. These results support previous studies that have shown the beneficial effects of physical activity and sleep on cognitive health in adults [50,51]. The findings of a recent systematic review revealed a positive association between higher levels of objective-measured moderate-vigorous physical activity and cognitive function in older adults. While the longer the sedentary behavior were found to be negatively associated with cognitive function [52]. Insufficient sleep duration in the elderly is negatively correlated with cognitive function. In particular, both shorter and longer durations than the usual 7–9 h is associated with poorer cognitive function [53,54]. Fanning et al. discovered that substituting sedentary behaviors with sleep and moderate-to-vigorous physical activity is associated with enhanced cognitive function in a randomized controlled exercise trial [55]. Therefore, the findings of this study suggest that meeting all three guidelines is associated with improved cognitive function, providing support for the practical application of the 24-HMB guidelines in enhancing the cognitive function of patients with diabetes.
4.3 Adherence to 24-HMB Guidelines and QoL
QoL was significantly higher among individuals with diabetes who adhered to different combinations of the 24-HMB guidelines. Specifically, adherence to the sedentary behavior, physical activity, or different combinations of guidelines (e.g., physical activity and sedentary behavior, physical activity and sleep duration, and sedentary behavior and sleep duration) were significantly associated with improved QoL. Meeting all three guidelines was associated with the highest QoL. This further demonstrates the comprehensive health benefits brought by a balanced lifestyle, which includes adequate physical activity, limited sedentary behavior, and sufficient sleep. Our findings align with those reported in previous research. For instance, Akksilp et al. [56] found that engaging in higher level of physical activity and limited sedentary time can improve QoL among adults. Furthermore, Guallar-Castillón et al. found that the combination of adequate physical activity and sleep and limited sedentary behavior was associated with greater QoL for adults in Spain [57]. These positive associations between physical activity, sedentary behavior, and sleep may involve different and synergistic mechanisms by which these factors are believed to affect QoL. One probable explanation is that individuals engaging in higher levels of physical activity tend to have a better QoL. This is due to the positive effects on physical and psychological health, such as increasing physical fitness, reducing functional limitation, regulating blood glucose levels, improving self-efficacy and self-esteem, and alleviating symptoms of depression and anxiety [58]. Furthermore, previous observations have reported that adequate sleep is positively linked to the blood glucose control level of diabetic patients [59]. They can also reduce the risk of physical complications [60], thereby improving the health-related QoL of this specific patient population. Meanwhile, good sleep quality can contribute to a significant impact on overall QoL by reducing the symptoms of depression and anxiety [61]. Therefore, the results of this study indicate that adherence to 24-HMB guidelines can significantly enhance QoL, with full adherence providing the substantial benefits for individuals with diabetes.
This study exhibits specific limitations that need careful evaluation. First, the present study adopted a cross-sectional design, which can not accurately explore the causal associations between meeting 24-HMB guidelines and psychological health indicators. More longitudinal research is needed to examine potential causal mechanisms underlying the observed associations. Second, Self-reported measurement methods for physical activity, sedentary behavior and sleep duration may introduce systematic errors such as recall bias. self-reported measurement methods for 24-HMB may introduce systemic errors, such as recall bias. To reduce potential biases, further research should use objective measurement tools (e.g., actigraphy, etc.) to measure behavioral data. Third, the data collection period (between 2007 and 2010) may not reflect the recent health status, though ongoing public health concerns related to diabetes, sedentary lifestyles, and mental health remain pertinent. Finally, the results of this study may lack generalizability to other developed countries, and unmeasured confounding variables could influence epidemiological interpretations. Future research addressing these constraints would strengthen the validity and applicability of such findings.
The improvement of living standards and the rapid urbanization process have contributed to increasingly prolonged sitting time and inadequate physical activity levels, exacerbating the burden of diabetes and its adverse psychological effects in adults. The efforts made by the public health department to address these challenges should emphasize on meeting 24-HMB guidelines, as these guidelines have significant practical implications for promoting the psychological health of diabetic patients. In particular, our study highlights the benefits of: engaging in at least 150 min/week of moderate-to-vigorous physical activity, limiting <8 h/day of sedentary behavior, and ensuring sleep duration for 7 to 9 h a day within 24 h. Implementing these recommendations could reduce depressive symptoms, enhance cognitive function, and improve overall QoL in diabetic populations.
This study explores the relationship between adherence to 24-HMB guidelines and psychological health outcomes among diabetic adults, revealing significant associations between the them. These findings underscore that meeting 24-HMB guidelines is of great significance for reducing the odds of depression, improving cognitive function, and enhancing QoL in this population. However, the regional specificity of the sample limits the generalizability of these results. Further research should validate these associations in diverse populations using objective measurement tools (e.g., accelerometers) to strengthen reliability.
Acknowledgement:
Funding Statement: The authors received no specific funding for this study.
Author Contributions: The authors confirm contribution to the paper as follows: conceptualization, Wenjiao Li and Yanjie Zhang; methodology, Wenjiao Li and Yanjie Zhang; software, Wenjiao Li and Xinxing Li; validation, Shiliang Chen, Shihui Chen and Yanjie Zhang; formal analysis, Wenjiao Li, Xinxing Li and Yanjie Zhang; investigation, Wenjiao Li, Xinxing Li and Yanjie Zhang; data curation, Wenjiao Li, Xinxing Li and Yanjie Zhang; writing—original draft preparation, Wenjiao Li, Shiliang Chen and Yanjie Zhang; writing—review and editing, Wenjiao Li, Shiliang Chen, Shihui Chen, Xinxing Li and Yanjie Zhang; project administration, Yanjie Zhang. All authors reviewed and approved the final version of the manuscript.
Availability of Data and Materials: The data that support the findings of this study are openly available in https://apps.who.int/healthinfo/systems/surveydata/index.php/catalog/?page=1&ps=15.
Ethics Approval: Not applicable.
Conflicts of Interest: The authors declare no conflicts of interest.
Supplementary Materials: The supplementary material is available online at https://www.techscience.com/doi/10.32604/ijmhp.2026.072912/s1.
References
1. Rahim NE , Flood D , Marcus ME , Theilmann M , Aung TN , Agoudavi K , et al. Diabetes risk and provision of diabetes prevention activities in 44 low-income and middle-income countries: a cross-sectional analysis of nationally representative, individual-level survey data. Lancet Glob Health. 2023; 11( 10): e1576– 86. doi:10.1016/S2214-109X(23)00348-0. [Google Scholar] [CrossRef]
2. Lim S , Nam GE , Sharma AM . Differences between type 2 diabetes mellitus and obesity management: medical, social, and public health perspectives. Diabetes Metab J. 2025; 49( 4): 565– 79. doi:10.4093/dmj.2025.0278. [Google Scholar] [CrossRef]
3. Magliano DJ , Boyko EJ . IDF diabetes atlas. 10th ed. Brussels, Belgium: International Diabetes Federation; 2021. [Google Scholar]
4. Sun H , Saeedi P , Karuranga S , Pinkepank M , Ogurtsova K , Duncan BB , et al. IDF diabetes atlas: global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res Clin Pract. 2022; 183: 109119. doi:10.1016/j.diabres.2021.109119. [Google Scholar] [CrossRef]
5. Manning KM , Hall KS , Sloane R , Magistro D , Rabaglietti E , Lee CC , et al. Longitudinal analysis of physical function in older adults: the effects of physical inactivity and exercise training. Aging Cell. 2024; 23( 1): e13987. doi:10.1111/acel.13987. [Google Scholar] [CrossRef]
6. Meisters R , Albers J , Sezer B , de Galan BE , Eussen SJPM , Stehouwer CDA , et al. Socioeconomic inequalities in health-related functioning among people with type 2 diabetes: longitudinal analyses in the Maastricht study. BMC Public Health. 2024; 24( 1): 73. doi:10.1186/s12889-023-17553-z. [Google Scholar] [CrossRef]
7. McInerney AM , Lindekilde N , Nouwen A , Schmitz N , Deschênes SS . Diabetes distress, depressive symptoms, and anxiety symptoms in people with type 2 diabetes: a network analysis approach to understanding comorbidity. Diabetes Care. 2022; 45( 8): 1715– 23. doi:10.2337/dc21-2297. [Google Scholar] [CrossRef]
8. Tamornpark R , Utsaha S , Apidechkul T , Panklang D , Yeemard F , Srichan P . Quality of life and factors associated with a good quality of life among diabetes mellitus patients in northern Thailand. Health Qual Life Outcomes. 2022; 20( 1): 81. doi:10.1186/s12955-022-01986-y. [Google Scholar] [CrossRef]
9. He J , Liu F , Xu P , Xu T , Yu H , Wu B , et al. Aerobic exercise improves the overall outcome of type 2 diabetes mellitus among people with mental disorders. Depress Anxiety. 2024; 2024( 1): 6651804. doi:10.1155/da/6651804. [Google Scholar] [CrossRef]
10. Dove A , Shang Y , Xu W , Grande G , Laukka EJ , Fratiglioni L , et al. The impact of diabetes on cognitive impairment and its progression to dementia. Alzheimers Dement. 2021; 17( 11): 1769– 78. doi:10.1002/alz.12482. [Google Scholar] [CrossRef]
11. Jacobson AM , Ryan CM , Braffett BH , Gubitosi-Klug RA , Lorenzi GM , Luchsinger JA , et al. Cognitive performance declines in older adults with type 1 diabetes: results from 32 years of follow-up in the DCCT and EDIC study. Lancet Diabetes Endocrinol. 2021; 9( 7): 436– 45. doi:10.1016/S2213-8587(21)00086-3. [Google Scholar] [CrossRef]
12. Dutta BJ , Singh S , Seksaria S , Das Gupta G , Singh A . Inside the diabetic brain: insulin resistance and molecular mechanism associated with cognitive impairment and its possible therapeutic strategies. Pharmacol Res. 2022; 182: 106358. doi:10.1016/j.phrs.2022.106358. [Google Scholar] [CrossRef]
13. Zhang Y , Kuang J , Luo X , Zhao M , Liu X . Association between meeting 24-hour movement guidelines and psychological features of Chinese emerging adults. Int J Ment Health Promot. 2024; 26( 5): 399– 406. doi:10.32604/ijmhp.2024.048925. [Google Scholar] [CrossRef]
14. Yang Z , Li X , Song W , Zhang Y . Associations between meeting 24-h movement guidelines and sarcopenia risk among adults aged ≥55 years in five low- and middle-income countries. Complement Ther Clin Pract. 2024; 57: 101887. doi:10.1016/j.ctcp.2024.101887. [Google Scholar] [CrossRef]
15. Willems I , Verbestel V , Dumuid D , Stanford TE , Calders P , Lapauw B , et al. Cross-sectional associations between 24-hour movement behaviors and cardiometabolic health among adults with type 2 diabetes mellitus: a comparison according to weight status. J Sci Med Sport. 2024; 27( 3): 179– 86. doi:10.1016/j.jsams.2023.11.010. [Google Scholar] [CrossRef]
16. Zhang X , Mao F , Wu L , Zhang G , Huang Y , Chen Q , et al. Associations of physical activity, sedentary behavior and sleep duration with anxiety symptoms during pregnancy: an isotemporal substitution model. J Affect Disord. 2022; 300: 137– 44. doi:10.1016/j.jad.2021.12.102. [Google Scholar] [CrossRef]
17. Tebar WR , Aguilar BAS , Delfino LD , Beretta VS , Brazo-Sayavera J , Silva DRP , et al. Association of meeting 24-hour movement guidelines with anxiety and depressive symptoms in adults. BMC Public Health. 2024; 24( 1): 3509. doi:10.1186/s12889-024-21038-y. [Google Scholar] [CrossRef]
18. Groves CI , Huong C , Porter CD , Summerville B , Swafford I , Witham B , et al. Associations between 24-h movement behaviors and indicators of mental health and well-being across the lifespan: a systematic review. J Act Sedentary Sleep Behav. 2024; 3( 1): 9. doi:10.1186/s44167-024-00048-6. [Google Scholar] [CrossRef]
19. Ross R , Chaput JP , Giangregorio LM , Janssen I , Saunders TJ , Kho ME , et al. Canadian 24-hour movement guidelines for adults aged 18–64 years and adults aged 65 years or older: an integration of physical activity, sedentary behaviour, and sleep. Appl Physiol Nutr Metab. 2020; 45( 10): S57– 102. doi:10.1139/apnm-2020-0467. [Google Scholar] [CrossRef]
20. Blodgett JM , Ahmadi MN , Atkin AJ , Pulsford RM , Rangul V , Chastin S , et al. Device-measured 24-hour movement behaviors and blood pressure: a 6-part compositional individual participant data analysis in the ProPASS consortium. Circulation. 2025; 151( 2): 159– 70. doi:10.1161/CIRCULATIONAHA.124.069820. [Google Scholar] [CrossRef]
21. Liang W , Wang Y , Huang Q , Shang B , Su N , Zhou L , et al. Adherence to 24-hour movement guidelines among Chinese older adults: prevalence, correlates, and associations with physical and mental health outcomes. JMIR Public Health Surveill. 2024; 10: e46072. doi:10.2196/46072. [Google Scholar] [CrossRef]
22. Patience M , Janssen X , Kirk A , McCrory S , Russell E , Hodgson W , et al. 24-hour movement behaviours (physical activity, sedentary behaviour and sleep) association with glycaemic control and psychosocial outcomes in adolescents with type 1 diabetes: a systematic review of quantitative and qualitative studies. Int J Environ Res Public Health. 2023; 20( 5): 4363. doi:10.3390/ijerph20054363. [Google Scholar] [CrossRef]
23. Liese AD , Ma X , Maahs DM , Trilk JL . Physical activity, sedentary behaviors, physical fitness, and their relation to health outcomes in youth with type 1 and type 2 diabetes: a review of the epidemiologic literature. J Sport Health Sci. 2013; 2( 1): 21– 38. doi:10.1016/j.jshs.2012.10.005. [Google Scholar] [CrossRef]
24. Teno SC , Silva MN , Júdice PB . Physical activity and sedentary behaviour-specific domains and their associations with mental health in adults: a systematic review. Adv Ment Health. 2024; 22( 3): 738– 65. doi:10.1080/18387357.2024.2324099. [Google Scholar] [CrossRef]
25. Jiang Y , Zhang M , Cui J . The relationship between sedentary behavior and depression in older adults: a systematic review and meta-analysis. J Affect Disord. 2024; 362: 723– 30. doi:10.1016/j.jad.2024.07.097. [Google Scholar] [CrossRef]
26. Khan A , Ezeugwa J , Ezeugwu VE . A systematic review of the associations between sedentary behavior, physical inactivity, and non-motor symptoms of Parkinson’s disease. PLoS One. 2024; 19( 3): e0293382. doi:10.1371/journal.pone.0293382. [Google Scholar] [CrossRef]
27. Swindell N , Rees P , Fogelholm M , Drummen M , MacDonald I , Martinez JA , et al. Compositional analysis of the associations between 24-h movement behaviours and cardio-metabolic risk factors in overweight and obese adults with pre-diabetes from the PREVIEW study: cross-sectional baseline analysis. Int J Behav Nutr Phys Act. 2020; 17( 1): 29. doi:10.1186/s12966-020-00936-5. [Google Scholar] [CrossRef]
28. García-Hermoso A , López-Gil JF , Ezzatvar Y , Ramírez-Vélez R , Izquierdo M . Twenty-four-hour movement guidelines during middle adolescence and their association with glucose outcomes and type 2 diabetes mellitus in adulthood. J Sport Health Sci. 2023; 12( 2): 167– 74. doi:10.1016/j.jshs.2022.08.001. [Google Scholar] [CrossRef]
29. Xie H , Chen E , Zhang Y . Association of walking pace and fall-related injury among Chinese older adults: data from the SAGE survey. Complement Ther Clin Pract. 2023; 50: 101710. doi:10.1016/j.ctcp.2022.101710. [Google Scholar] [CrossRef]
30. Bull FC , Maslin TS , Armstrong T . Global physical activity questionnaire (GPAQ): nine country reliability and validity study. J Phys Act Health. 2009; 6( 6): 790– 804. doi:10.1123/jpah.6.6.790. [Google Scholar] [CrossRef]
31. Zhang Y , Liu X , Ma Y , Li X . Physical activity, sedentary behavior, fruit and vegetable consumption, and sarcopenia in older Chinese adults: a cross-sectional study. Nutrients. 2023; 15( 15): 3417. doi:10.3390/nu15153417. [Google Scholar] [CrossRef]
32. Ganapathy A , Nieves JW . Nutrition and sarcopenia—what do we know? Nutrients. 2020; 12( 6): 1755. doi:10.3390/nu12061755. [Google Scholar] [CrossRef]
33. Muhammad T , Sruthi Anil Kumar AH , Sekher TV . Gender-specific associations between sleep quality, sleep duration and cognitive functioning among older Indians: findings from WHO-SAGE study. Sleep Sci Pract. 2024; 8( 1): 6. doi:10.1186/s41606-024-00100-z. [Google Scholar] [CrossRef]
34. Gildner TE , Liebert MA , Kowal P , Chatterji S , Josh Snodgrass J . Sleep duration, sleep quality, and obesity risk among older adults from six middle-income countries: findings from the study on global ageing and adult health (SAGE). Am J Hum Biol. 2014; 26( 6): 803– 12. doi:10.1002/ajhb.22603. [Google Scholar] [CrossRef]
35. Kessler RC , Ustün TB . The world mental health (WMH) survey initiative version of the World Health Organization (WHO) composite international diagnostic interview (CIDI). Int J Methods Psychiatr Res. 2004; 13( 2): 93– 121. doi:10.1002/mpr.168. [Google Scholar] [CrossRef]
36. Arokiasamy P , Uttamacharya U , Jain K , Biritwum RB , Yawson AE , Wu F , et al. The impact of multimorbidity on adult physical and mental health in low- and middle-income countries: what does the study on global ageing and adult health (SAGE) reveal? BMC Med. 2015; 13: 178. doi:10.1186/s12916-015-0402-8. [Google Scholar] [CrossRef]
37. Ashdown-Franks G , Koyanagi A , Vancampfort D , Smith L , Firth J , Schuch F , et al. Sedentary behavior and perceived stress among adults aged ≥50 years in six low- and middle-income countries. Maturitas. 2018; 116: 100– 7. doi:10.1016/j.maturitas.2018.08.005. [Google Scholar] [CrossRef]
38. Selvamani Y , Arokiasamy P , Chaudhary M . Association between food insecurity and quality of life among older adults (60+) in six low and middle-income countries. Arch Gerontol Geriatr. 2023; 114: 105079. doi:10.1016/j.archger.2023.105079. [Google Scholar] [CrossRef]
39. Smith L , Shin JI , Barnett Y , Allen PM , Lindsay R , Pizzol D , et al. Association of objective visual impairment with suicidal ideation and suicide attempts among adults aged ≥50 years in low/middle-income countries. Br J Ophthalmol. 2022; 106( 11): 1610– 6. doi:10.1136/bjophthalmol-2021-318864. [Google Scholar] [CrossRef]
40. Dooley EE , Palta P , Wolff-Hughes DL , Martinez-Amezcua P , Staudenmayer J , Troiano RP , et al. Higher 24-h total movement activity percentile is associated with better cognitive performance in U.S. older adults. Med Sci Sports Exerc. 2022; 54( 8): 1317– 25. doi:10.1249/MSS.0000000000002927. [Google Scholar] [CrossRef]
41. Marent PJ , Cardon G , Dumuid D , Albouy G , van Uffelen J . 24-hour movement behaviours are cross-sectionally associated with cognitive function in healthy adults aged 55 years and older. Sci Rep. 2025; 15( 1): 38619. doi:10.1038/s41598-025-22541-x. [Google Scholar] [CrossRef]
42. Covenant A , Yates T , Rowlands AV , Dempsey PC , Edwardson CL , Hall AP , et al. Replacing sedentary time with sleep and physical activity: associations with physical function and wellbeing in type 2 diabetes. Diabetes Res Clin Pract. 2024; 217: 111886. doi:10.1016/j.diabres.2024.111886. [Google Scholar] [CrossRef]
43. Dong L , Xie Y , Zou X . Association between sleep duration and depression in US adults: a cross-sectional study. J Affect Disord. 2022; 296: 183– 8. doi:10.1016/j.jad.2021.09.075. [Google Scholar] [CrossRef]
44. Zhai L , Zhang H , Zhang D . Sleep duration and depression among adults: a meta-analysis of prospective studies. Depress Anxiety. 2015; 32( 9): 664– 70. doi:10.1002/da.22386. [Google Scholar] [CrossRef]
45. Chellappa SL , Aeschbach D . Sleep and anxiety: from mechanisms to interventions. Sleep Med Rev. 2022; 61: 101583. doi:10.1016/j.smrv.2021.101583. [Google Scholar] [CrossRef]
46. Del Pozo Cruz B , Alfonso-Rosa RM , McGregor D , Chastin SF , Palarea-Albaladejo J , Del Pozo Cruz J . Sedentary behaviour is associated with depression symptoms: compositional data analysis from a representative sample of 3233 US adults and older adults assessed with accelerometers. J Affect Disord. 2020; 265: 59– 62. doi:10.1016/j.jad.2020.01.023. [Google Scholar] [CrossRef]
47. Kracht CL , Burkart S , Groves CI , Balbim GM , Pfledderer CD , Porter CD , et al. 24-hour movement behavior adherence and associations with health outcomes: an umbrella review. J Act Sedentary Sleep Behav. 2024; 3( 1): 25. doi:10.1186/s44167-024-00064-6. [Google Scholar] [CrossRef]
48. Su J , Wei E , Clark C , Liang K , Sun X . Physical exercise, sedentaary behaviour, sleep and depression symptoms in Chinese young adults during the COVID-19 pandemic: a compositional isotemporal analysis. Int J Ment Health Promot. 2022; 24( 5): 759– 69. doi:10.32604/ijmhp.2022.020152. [Google Scholar] [CrossRef]
49. Hakimi S , Martin LJ , Rosenberg MW . Impacts of physical activity, sedentary behaviour, and sleep on depression symptoms in Canadian older adults 65 years of age and above: a compositional data analysis of the Canadian longitudinal study on aging. J Act Sedentary Sleep Behav. 2024; 3( 1): 8. doi:10.1186/s44167-024-00047-7. [Google Scholar] [CrossRef]
50. Mellow ML , Smith AE , Dumuid D , Stanford T , Keage H , Wade A , et al. Cross-sectional associations between use of time and cognition in healthy older adults. Alzheimers Dement. 2023; 19( S8): e060963. doi:10.1002/alz.060963. [Google Scholar] [CrossRef]
51. Mellow ML , Crozier AJ , Dumuid D , Wade AT , Goldsworthy MR , Dorrian J , et al. How are combinations of physical activity, sedentary behaviour and sleep related to cognitive function in older adults? A systematic review. Exp Gerontol. 2022; 159: 111698. doi:10.1016/j.exger.2022.111698. [Google Scholar] [CrossRef]
52. Rojer AGM , Ramsey KA , Amaral Gomes ES , D’Andrea L , Chen C , Szoeke C , et al. Objectively assessed physical activity and sedentary behavior and global cognitive function in older adults: a systematic review. Mech Ageing Dev. 2021; 198: 111524. doi:10.1016/j.mad.2021.111524. [Google Scholar] [CrossRef]
53. Yaffe K , Falvey CM , Hoang T . Connections between sleep and cognition in older adults. Lancet Neurol. 2014; 13( 10): 1017– 28. doi:10.1016/S1474-4422(14)70172-3. [Google Scholar] [CrossRef]
54. Bloomberg M , Brocklebank L , Hamer M , Steptoe A . Joint associations of physical activity and sleep duration with cognitive ageing: longitudinal analysis of an English cohort study. Lancet Healthy Longev. 2023; 4( 7): e345– 53. doi:10.1016/S2666-7568(23)00083-1. [Google Scholar] [CrossRef]
55. Fanning J , Porter G , Awick EA , Ehlers DK , Roberts SA , Cooke G , et al. Replacing sedentary time with sleep, light, or moderate-to-vigorous physical activity: effects on self-regulation and executive functioning. J Behav Med. 2017; 40( 2): 332– 42. doi:10.1007/s10865-016-9788-9. [Google Scholar] [CrossRef]
56. Akksilp K , Müller-Riemenschneider F , Teerawattananon Y , Chen C . The association of physical activity and sedentary behaviour on health-related quality of life: a cross-sectional study from the physical activity at work (PAW) trial. J Act Sedentary Sleep Behav. 2023; 2( 1): 22. doi:10.1186/s44167-023-00031-7. [Google Scholar] [CrossRef]
57. Guallar-Castillón P , Bayán-Bravo A , León-Muñoz LM , Balboa-Castillo T , López-García E , Gutierrez-Fisac JL , et al. The association of major patterns of physical activity, sedentary behavior and sleep with health-related quality of life: a cohort study. Prev Med. 2014; 67: 248– 54. doi:10.1016/j.ypmed.2014.08.015. [Google Scholar] [CrossRef]
58. Luo X , Zhao M , Zhang Y , Zhang Y . Effects of baduanjin exercise on blood glucose, depression and anxiety among patients with type II diabetes and emotional disorders: a meta-analysis. Complement Ther Clin Pract. 2023; 50: 101702. doi:10.1016/j.ctcp.2022.101702. [Google Scholar] [CrossRef]
59. Schipper SBJ , Van Veen MM , Elders PJM , van Straten A , Van Der Werf YD , Knutson KL , et al. Sleep disorders in people with type 2 diabetes and associated health outcomes: a review of the literature. Diabetologia. 2021; 64( 11): 2367– 77. doi:10.1007/s00125-021-05541-0. [Google Scholar] [CrossRef]
60. Laverty B , Puthezhath Jayanandan S , Smyth S . Understanding the relationship between sleep and quality of life in type 2 diabetes: a systematic review of the literature. J Health Psychol. 2023; 28( 8): 693– 710. doi:10.1177/13591053221140805. [Google Scholar] [CrossRef]
61. Lee S , Kim JH , Chung JH . The association between sleep quality and quality of life: a population-based study. Sleep Med. 2021; 84: 121– 6. doi:10.1016/j.sleep.2021.05.022. [Google Scholar] [CrossRef]
Cite This Article
 Copyright © 2026 The Author(s). Published by Tech Science Press.
Copyright © 2026 The Author(s). Published by Tech Science Press.This work is licensed under a Creative Commons Attribution 4.0 International License , which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
 Downloads
Downloads
 Citation Tools
Citation Tools