
 Submit a Paper
Submit a Paper Propose a Special lssue
Propose a Special lssue Open Access
Open Access
REVIEW

Intervention Characteristics to Improve Stress Coping in Healthcare Students: A Systematic Review and Meta-Analysis
1 College of Osteopathic Medicine, Western University of Health Sciences, Pomona, CA, USA
2 College of Osteopathic Medicine of the Pacific Northwest, Western University of Health Sciences, Lebanon, OR, USA
* Corresponding Author: Edie L. Sperling. Email:
(This article belongs to the Special Issue: Evidence-based Approaches to Managing Stress, Depression, Anxiety, and Suicide)
International Journal of Mental Health Promotion 2026, 28(2), 1 https://doi.org/10.32604/ijmhp.2026.074948
Received 22 October 2025; Accepted 25 December 2025; Issue published 27 February 2026
 View Full Text
View Full Text Download PDF
Download PDFAbstract
Objectives: Healthcare students experience significant stress due to their rigorous graduate school curricula. These levels of stress are associated with higher risks of depression, self-harm, and exhaustion. Coping interventions have been shown to help students develop healthy stress coping strategies. The purpose of this systematic review and meta-analysis was to examine the diverse array of coping interventions and what characteristics of coping interventions were most effective at decreasing stress among healthcare students. Methods: Any intervention designed to address coping for academic stress was included among medical, dental, nursing, physician assistant, allied health, veterinary, psychology, etc. students. A comprehensive literature search was completed to include multiple databases, Ancestry, and hand-searching from EBSCO and Google Scholar articles. A final total of 17 studies were included. Standardized mean difference effect sizes (ES) were synthesized across studies using a random-effects model in the Comprehensive Meta-Analysis Software for changes in coping levels in healthcare students. Moderator analyses were performed to explore the study, intervention, and participants’ characteristics. The risk of bias was assessed by RoB2 and ROBINS-I. Results: Coping interventions significantly reduced stress outcomes among healthcare students (d = 0.74; 95% CI [0.48–1.01], 95% PI [−0.41–1.90], p < 0.001, Q = 228.49, I2 = 93.0%, T = 0.52, T2 = 0.28, p < 0.001). Moderator analysis showed that interventions with stress education, established professional guidance, and fewer hours led to better stress management outcomes. Conclusions: This study demonstrates that coping interventions produce an overall moderate-to-large effect on stress reduction. Future research investigating coping interventions on academic and long-term outcomes would be beneficial.Keywords
Supplementary Material
Supplementary Material FileHealthcare professional students experience high stress levels during their training and career, which leads to a higher risk of psychological health problems [1,2]. Over 75% of medical students commonly report moderate-to-severe stress levels, and academic-related stressors are often the top cause [3,4,5]. Dental students report moderate to high stress from examinations and grading, while nursing students experience similar stress levels from academic demands and patient care responsibilities [6,7,8]. Intense academic demands and clinical training have also been shown to increase stress levels in veterinary, physical therapy, and occupational therapy students [9,10,11]. High stress levels can lead to burnout and depression [12,13,14]. Depression and burnout are also consistently reported to be high among medical, nursing, and dental students [15,16,17]. This trend can have long-term consequences, including increased medical errors [18,19].
Multiple studies have shown that healthy coping skills decrease during healthcare schooling [20,21,22,23]. Coping refers to the flexible, conscious thought patterns and behaviors that individuals use when in stressful situations [21]. When there is significant distress, low self-esteem, and/or difficult curriculum factors, students do not engage in effective coping strategies, making poor coping very common in medical school [22]. Students with lower coping skills also tend to report having higher stress, creating a vicious cycle of stress and ineffective coping [23]. There are different types of coping that have varying degrees of effectiveness on stress levels; four major categories of coping are problem-focused, emotion-focused, meaning-focused, and social coping [24]. There is also maladaptive coping, including disengagement, emotional suppression, avoidance, and denial, which are recognized as learnt in childhood and adolescence [25].
Common coping strategies healthcare students use include leaning on friends and family and mindset changing [26]. Medical students commonly seek social and emotional support to cope with stress [26]. Studies show that nursing students use problem-solving, social support, and cognitive restructuring [27,28]. For veterinary students, exercise and social activities, where social support and relationship quality were enhanced, were effective for coping with stress [9]. The most common coping strategies among dental students are acceptance, self-distraction, and positive reframing [29]. Occupational and physical therapy students’ coping strategies include exercise, strategic selection of peers, and modifying expectations [30]. Even though there are many healthy ways students cope with stress, there are maladaptive strategies students turn to, such as substance abuse, self-blame, and avoidance [31,32]. High stress and burnout among healthcare students and professionals are linked to attrition from health programs and the profession, contributing to the global staffing crisis in healthcare [4,16]. Therefore, it is important to educate and optimize coping interventions to support students with high levels of stress.
Prior meta-analyses show that problem-focused coping decreases stress levels and burnout in healthcare students [33,34,35,36] However, most meta-analyses only focused on one type of intervention or healthcare student group, leaving gaps in our understanding of coping strategies useful to health profession students as a whole [37,38,39,40,41] There was also wide variation in which coping strategies were measured in previous research, including both helpful and unhelpful coping strategies, and not all facets are investigated in every study [24,25,39,40,41,42,43]. Given these limitations, we identified the need for a more comprehensive review and meta-analysis. The purpose of this research is to analyze and identify the characteristics of coping interventions that are most effective at reducing stress in healthcare students. The research questions driving this meta-analysis were: (1) What interventions have been used to improve healthcare professional students’ coping (medical, nursing, dental, veterinary, allied health, pharmacy, physician assistant, clinical psychology)? (2) What effect have interventions had on coping among health profession students? (3) What characteristics of the populations or interventions make the interventions more or less effective?
The Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines were followed in this systematic review and meta-analysis [44]. The completed PRISMA checklist is provided as Supplementary Material. The review was not registered.
2.1 Inclusion & Exclusion Criteria
Inclusion criteria included articles which (1) described an intervention to improve coping skills, behaviors, and/or strategies, in the context of professional healthcare school; (2) had an outcome measure of coping in any form as long as it was identified and conceptualized as coping by the authors; (3) coping was conceptualized and measured as academic coping or coping with school-related stress, anxiety, depression, burnout, etc. (not limited as long as school-related); (4) healthcare student population globally including medical, dental, nursing, veterinary, physician assistant (PA), pharmacy, allied health (e.g., physical therapy, occupational therapy, speech therapy), and/or clinical psychology, in any year of school; (5) any study design with an intervention, including randomized controlled trial (RCT), non-randomized two-arm, or one-arm pre/post. No restrictions were placed on study location, date, or level of degree. When applicable, physiological measures of stress data were collected, coded, and included alongside subjective measures. Excluded criteria included (1) mixed populations without separately reporting outcomes (e.g., medical and engineering students in aggregate); (2) not published or primary studies (e.g., review articles, trade magazines); (3) coping addressed external factors that were not academic or school related (e.g., parenting). No limitation was placed on sample size or power of a primary study; establishing a fixed sample size based on a predetermined power level can bias results due to variation in effect sizes from study design, population, measurement tools, and intervention type, leading to the exclusion of small studies that may have insights to offer, and increasing publication bias [45,46].
Filters for English language and peer-reviewed articles were used. The following databases were searched by author ELS: EBSCOhost (inclusive of Academic Search Elite; Alt Healthwatch; Business Source Elite; CINAHL; eBook Collection; ERIC; Funk & Wagnalls New World Encyclopedia; Health Source–Consumer Edition; Health Source–Nursing/Academic Edition; Library, Information Science & Technology Abstracts; MAS Ultra–School Edition; Military & Government Collection; Newspaper Source; Primary Search; OpenDissertations; APA PsycInfo; MAS Reference eBook Collection; Primary Search Reference eBook Collection; and MEDLINE); PubMed; Web of Science; and Google Scholar. The search was carried out between March 6 and June 22, 2025 with the search terms: “cope or coping or coping strategies or coping skills or coping mechanisms or coping behaviors” AND “medical students or nursing students or healthcare professional students or allied health students or physical therapy students or physiotherapy students or dental students or veterinary students or occupational therapy students or speech language pathology students or physician assistant students or pharmacy students or graduate psychology students or psychology PhD students”.
Zotero (Corporation for Digital Scholarship; 8300 Boone Blvd Ste 500, Vienna, VA 22182, USA) was used for citation and duplicate tracking. Excel (Microsoft Corporation; One Microsoft Way, Redmond, VA 98052-6399, USA) was used for coding and applying inclusion and exclusion criteria.
2.4 Data Extraction and Coding
Cooper et al. [47] guidelines were used to develop an extensive codebook. All authors trained in meta-analytic methods and extracted data from eligible studies. Variable classifications include study identification, basic information (article title, authors, research design), population characteristics and demographics (student type, location, mean age, gender, race, ethnicity), reliability and validity (blinding, randomization), intervention details (name, characteristics (e.g., stress education, cognitive behavioral therapy), length of intervention, duration of sessions, total sessions, delivery mode), outcomes (e.g., outcome name, subjective or physiologic, time point, direction of effect), and results (e.g., sample size, mean, standard deviation, standard error, direction of effect). Pre-intervention measure and most proximal post-intervention measure were chosen as coding timepoints.
Comprehensive Meta-Analysis Software (CMA; Biostat, Inc., 14 North Dean Street, Englewood, NJ 07631, USA) was used for data analysis. The random-effects model was selected due to the expected heterogeneity in primary studies [46]. Cohen’s d for standardized mean difference effect sizes was used, as Hedges’ g can result in more bias in the meta-estimation [48]. Ninety-five percent confidence intervals (CI) and p-values for pooled estimates were calculated according to the random-effects model implemented in the software. P-values less than 0.05 was considered statistically significant. Effect sizes were classified as small (≤0.20), medium (~0.50), or large (≥0.80) [49]. A positive effect size was set to indicate improved coping and a negative effect size worse coping. Cochrane’s Risk of Bias tool version 2 (RoB2) was used to evaluate the risk of bias across RCT studies [50]. The ROBINS-I was used to evaluate the risk of bias across the quasi-experimental and pre/post studies [51].
Search results from databases included 6164 peer-reviewed manuscripts, so search terms were refined to the subject term and returned 584 articles (see Fig. 1). After title screening, 335 abstracts were retrieved and screened, leading to the retrieval of 34 full-text articles for screening. The final number of eligible articles was 17 (see Fig. 1). Articles are described in Table 1.
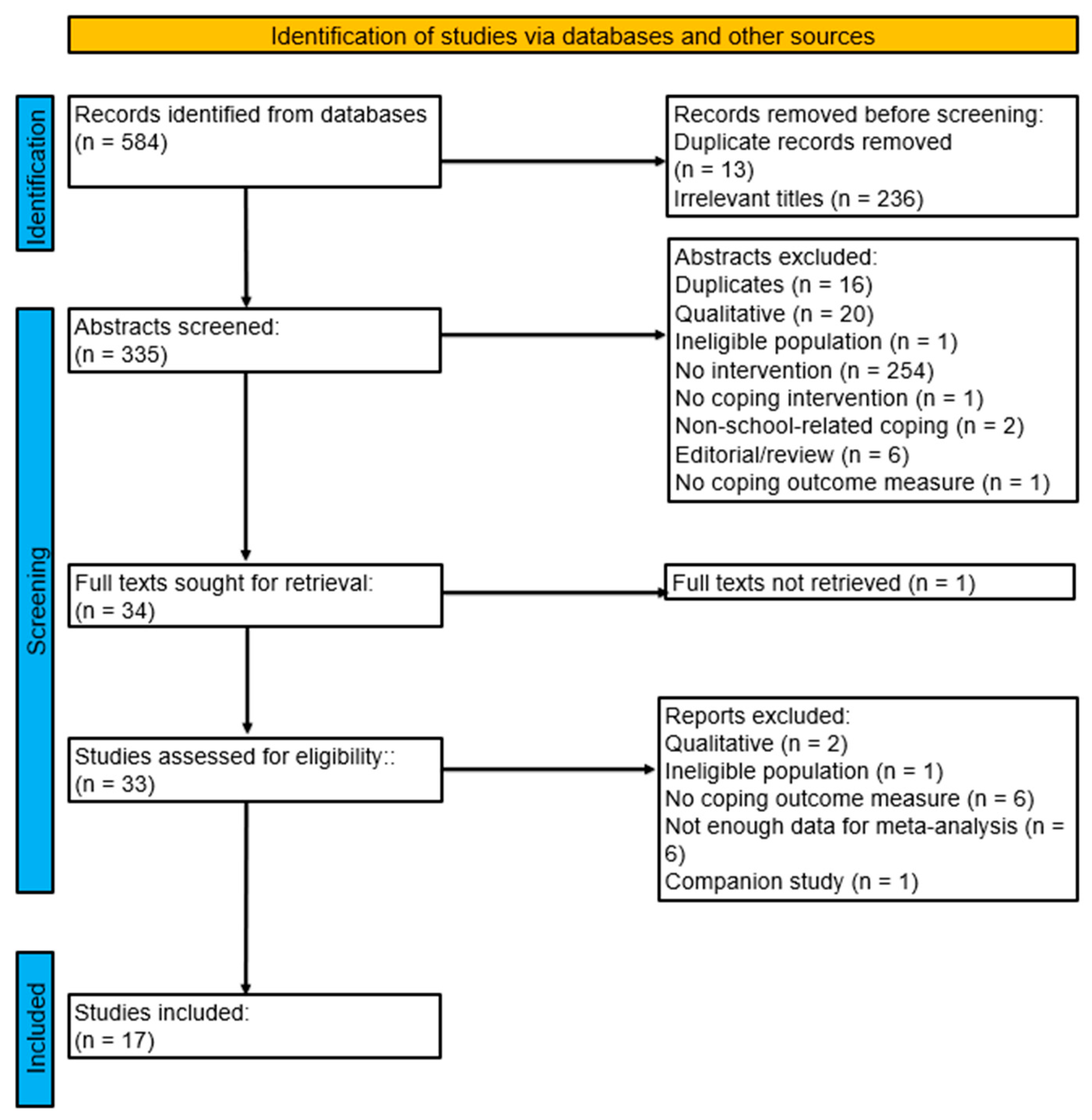
Figure 1: Preferred reporting items for systematic reviews and meta-analyses (PRISMA) flowchart of search.
Table 1: Characteristics of included articles on coping interventions for healthcare students.
| Study/Location | Design | Intervention | Sample Characteristics | Outcome Measure/Results |
|---|---|---|---|---|
| Ahmad and Meriç (2021) [52] Turkey | RCT | Online psychoeducational stress management program Duration: 6 weeks Frequency: Once per week for 60 min Total number of sessions: 7 | Nursing students Mean age: 20.02 years (SD 0.92); 68.3% Female (90% Black) n = 60 | Coping and Adaptation Processing Scale (CAPS): Short Form Mean capacity to cope level d = 0.907 |
| Çekiç and Ançel (2022) [53] Turkey | RCT | Interpersonal relational role analysis Duration: 10 weeks Frequency: Twice per week for 90 min Total number of sessions: 21 | Nursing students Mean age: 20.04 years (SD 1.52); 70% Female n = 10 | Coping Styles Inventory d = 1.465 |
| Demir and Ercan (2019) [54] Turkey | One arm pre/post | Self-awareness and communication techniques course Duration: 14 Weeks Frequency: Once per week for 180 min Total number of sessions: 14 | Nursing students Age range: (19–25); Mean age: 20 years (SD 1); 80.5% Female n = 123 | Ways of Coping with Stress Inventory d = 0.141 |
| Demir and Ercan (2022) [55] Turkey | RCT | Cognitive behavioral therapy-based group counseling Duration: 6 weeks Frequency: Once per week for 75 min Total number of sessions: 6 | Nursing students Mean age: 20.13 years (SD 1.54); 93.7% Female n = 63 | Ways of Coping Questionnaire d = 0.863 |
| Demir et al. (2014) [56] Turkey | One arm pre/post | Mentoring program Duration: 14 weeks Frequency: Once per week Total number of sessions: 14 | Nursing students Mean age: 18.8 years (SD 1.18); 92.4% Female n = 66 | Ways of Coping Inventory Mentoring Assessment Form d = 0.290 |
| Günaydin (2022) [57] Turkey | RCT | Group psychoeducation Duration: 7 weeks Frequency: Once per week for 60 min Total number of sessions: 7 | Nursing students Mean age: 19 years (SD 3.23); 71.1% Female n = 38 | Stress-Coping Styles Scales d = 1.827 |
| Halland et al. (2015) [58] Norway | RCT | Mindfulness training Duration: 7 weeks Frequency: Once per week for 90 min Total number of sessions: 7 | Psychology and medical students Mean age: 23.8 years (SD 5.1); 76% Female n = 265 | Ways of Coping Checklist d = 0.276 |
| Hiçdurmaz and Öz (2016) [59] Turkey | One arm pre/post | Cognitive-behavioral group counseling program Duration: 12 Weeks Fequency: Once per week for 90 min Total number of sessions: 12 | Nursing students n = 43 | Ways of Coping Inventory Automatic Thoughts Questionnaire d = 0.390 |
| Manning-Geist et al. (2019) [60] United States | Non-randomized control trial or quasi-experiment | Stress management workshops Duration: 1 weeks Frequency: One Session for 120 min Total number of sessions: 1 | Medical students n = 135 | Survey: Average confidence in stress coping d = 0.280 |
| Martín-Parrilla et al. (2025) [61] Spain | RCT | Simulation-based learning experiences Duration: 3 weeks Frequency: Once per week for 50 min Total number of sessions: 3 | Nursing students Mean age: 21.39 years (SD 4.06); 78.3% Female n = 240 | Bugen’s Coping with Death Scale (CDS) d = 1.219 |
| Nguyen et al. 2023 [31] Taiwan | Non-randomized control trial or quasi-experiment | Transforming stress program Duration: 10 weeks Frequency: Once every other week for 90 min Total number of sessions: 5 | Medical students Mean age: 18.1 years (SD 0.38); 36.9% Female n = 409 | Brief Coping Orientation to Problems Experienced (COPE) d = 1.503 |
| Onan et al. (2018) [62] Turkey | One arm pre/post | Stress coping course Duration: 14 Weeks Frequency: Once per week for 120 min Total number of sessions: 14 | University nursing students Mean age: 18.88 years (SD 0.85); 94.9% Female n = 78 | Psychological Resilience Questionnaire: Psychological resilience d = 0.767 |
| Ozan et al. (2020) [63] Turkey | RCT | Clinical education program based on Watson’s theory of human caring Duration: 12 weeks | Nursing students Mean age: 21.54 years (SD 2.7); 52.9% Female n = 106 | Ways of Coping Inventory d = 0.611 |
| Priyadharshini et al. (2021) [23] India | Non-randomized control trial or quasi-experiment | Intervention programs on stress level Duration: 4 weeks Frequency: Twice per week for 45 min Total number of sessions: 8 | Medical students Mean age: 19.98 years (SD 1.35); 62.2% Female n = 526 | Perceived Stress Scale d = 1.418 |
| Stoliker et al. (2022) [64] Canada | One arm pre/post | Online resilience training program Duration: 12 Weeks Total Number of sessions: 1 | BScN students Mean age: 32.25 years (SD 6.63) n = 70 | Coping Strategies Inventory-Short Form Measure of coping Resilience scale for adults d = 0.131 |
| Tunç and Orak (2024) [65] Turkey | RCT | Clinical adaptation psychoeducation program Duration: 6 weeks Frequency: Once per week for 90 min Total number of sessions: 6 | Nursing students Mean age: 19.39 years (SD 1.11); 71.2% Female n = 66 | Stress-Coping Behaviors Scale for Nursing Students d = 0.686 |
| Yüksel and Bahadır-Yılmaz (2019) [66] Turkey | Non-randomized control trial or quasi-experiment | Mentoring program Duration: 8 weeks Frequency: Once per week Total number of sessions: 8 | Nursing students Mean age: 18.56 years (SD 0.8); 62.6% Female n = 91 | Ways of Coping Inventory d = 0.533 |
3.1 Study and Participant Characteristics
The included studies were published between 2014 and 2025. Seven studies were RCTs [52,53,54,58,61,63,65], four studies were non-randomized control trials or quasi-experiments two-arm studies [23,31,60,66], and five studies used a one-arm pretest-posttest design [54,56,59,62,64] (see Table 1). Eleven studies were conducted in Turkey, and one each took place in Norway, the United States, Spain, Taiwan, South India, and Canada (see Table 1). The mean age of the participants across the studies ranged from 18.1 to 32.25 years. The percentage of participants who were female ranged from 36.9% to 94.9%. None of the studies reported a racially diverse sample, as in all cases, one racial group made up more than 60% of the participants.
3.2 Intervention Characteristics
Across the 17 studies in this meta-analysis, eleven of the studies assigned homework. Eleven studies conducted interventions in small groups. Most interventions were delivered synchronously and in person, and three were conducted online. Out of the three online interventions, two were asynchronous, and one was synchronous. Intervention duration ranged from 1 to 14 weeks, with 1 to 21 sessions, and session length ranged from 30 to 180 min.
The most common protocol was stress education. Some included cognitive behavioral therapy and mindfulness training. The unique protocols include dialectical behavior therapy, psychotherapy, Maslow’s hierarchy of basic needs, and Watson’s theory of human caring.
The coded studies had eleven different self-reported stress outcome measures in total. Most studies (n = 7) used the Ways of Coping Inventory. Some studies included coping outcome measures such as the Automatic Thoughts Questionnaire and Mentoring Assessment Form.
Coping interventions (k = 17, n = 17) demonstrated a statistically significant, moderate to large positive effect on reducing stress outcomes in medical students from pretest to posttest, compared with controls (d = 0.74, 95% CI [0.48–1.01], 95% PI [−0.41–1.90], p < 0.001) (Fig. 2). Standardized difference in means or effect sizes of the individual studies ranged from 0.28 to 1.83 with a positive effect size indicating improved coping and a negative effect size indicating worse coping following the intervention. As expected, there was statistically significant heterogeneity of effects noted across studies (Q = 228.49, I2 = 93.0%, T = 0.52, T2 = 0.28, p < 0.001) from heterogeneity statistics.
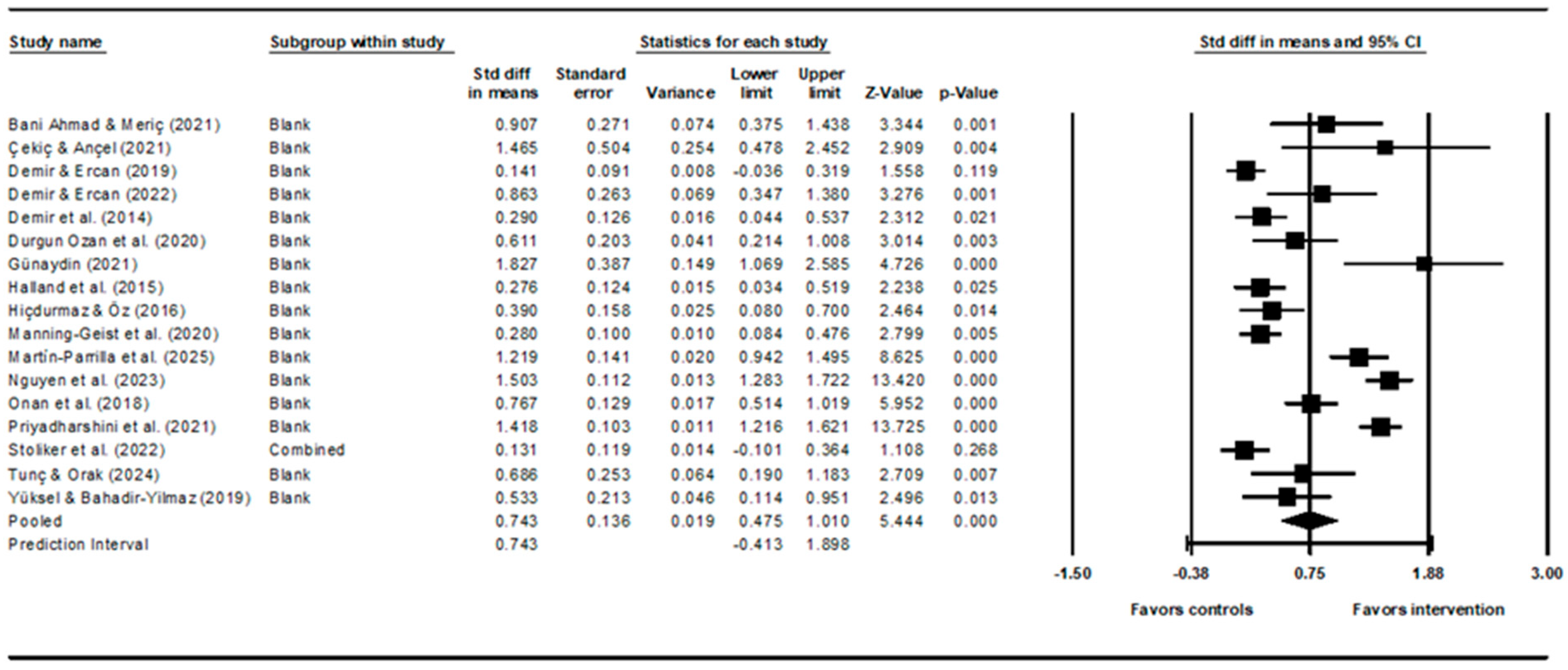
Figure 2: Forest plot showing the standardized mean effect sizes of all studies. Heterogeneity statistics: Q = 228.49 (p < 0.001), I2 = 93.0%, T = 0.52, T2 = 0.28.
Publication bias was assessed using three methods: funnel plot [67], Egger’s regression intercept [68], and Duvall and Tweedie’s trim & fill [69]. Multiple methods are recommended to provide more accuracy in the assessment of publication bias [46]. All tests were completed in Comprehensive Meta-Analysis (CMA). The funnel plot showed general symmetry but is missing effect sizes in the lower left corner of the plot, representing studies with lower effect sizes, demonstrating this meta-analysis may not include studies that faced publication bias due to lack of significant results (Fig. 3). Egger’s regression test (t = 0.84, p = 0.41, intercept 2.04) was not significant, suggesting that the data set was unlikely to be influenced by small sample bias [68]. Duval & Tweedie’s trim & fill identified one study trimmed, changing the point estimate (summary effect size) from 0.74 [0.48–1.01] to 0.69 [0.43–0.96]. A one-study-removed sensitivity analysis was run in CMA, and no studies were identified as affecting the summary effect sizes. These analyses together suggest a small-to-moderate amount of publication bias in the data.
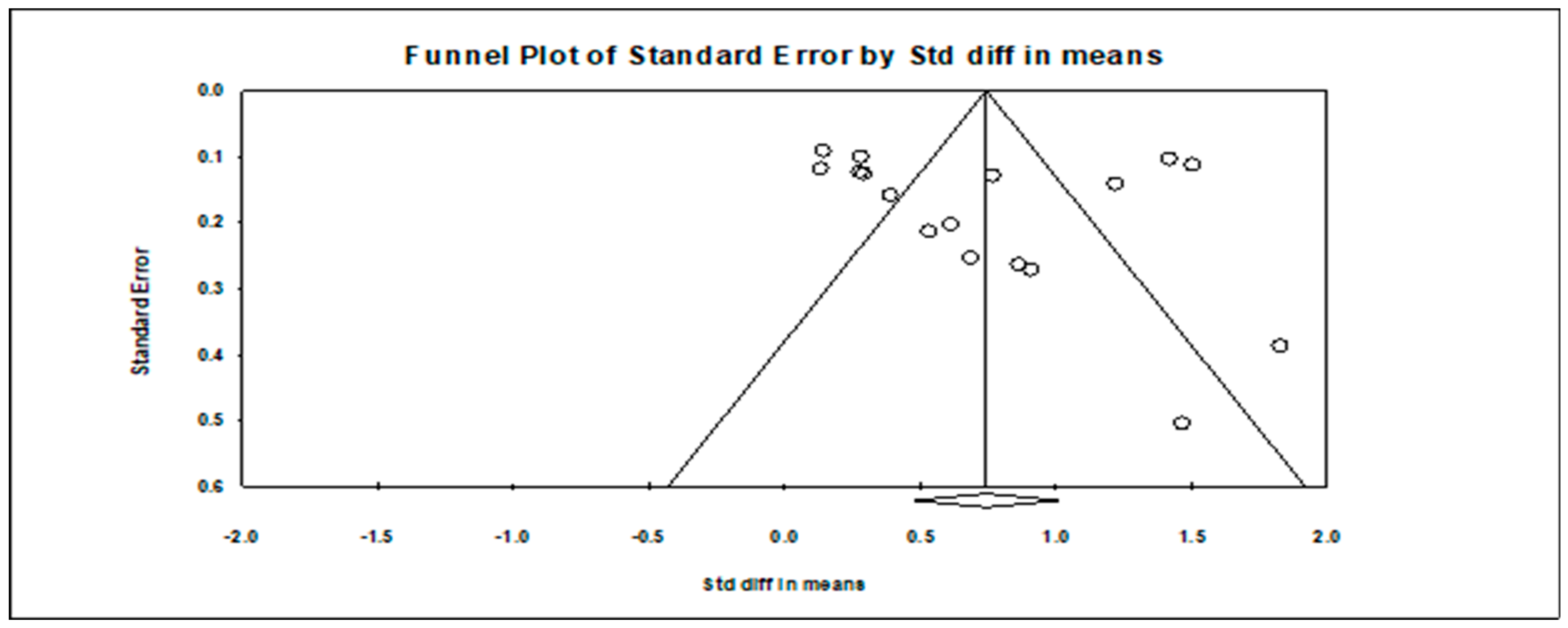
Figure 3: Funnel plot for publication bias in all studies.
Subgroups and meta-regression analyses were conducted to investigate heterogeneity (see Table 2). Subgroup analyses including study design, student discipline, in-person vs. online interventions, the inclusion of stress education, the inclusion of cognitive behavioral therapy (CBT), the inclusion of mindfulness, homework, small-group interventions, and the type of facilitator. Effect size significantly varied by study design (Q = 6.81, p = 0.03), with RCTs having the highest effect size (d = 0.91, 95% CI [0.55–1.27], 95% PI [−0.26–2.07], p < 0.001), non-randomized control-group studies the next highest (d = 0.80, 95% CI [0.20–1.40], 95% PI [−1.54–3.15], p < 0.01), and one-arm pre/post studies the lowest (d = 0.36, 95% CI [0.11–0.61], 95% PI [−0.77–1.49], p < 0.01). Effect size significantly differed by student discipline (Q = 7.19, p = 0.03) with medical students exhibiting a higher effect size (d = 1.07, 95% CI [0.28–1.86], 95% PI [−9.08–11.21], p < 0.01) compared to nursing students (d = 0.67, 95% CI [0.43–0.92], 95% PI [−0.23–1.57], p < 0.001). The inclusion of stress education had a significant impact on effect size (d = 0.85, 95% CI [0.48–1.21], 95% PI [−0.55–2.25], p < 0.001) compared to interventions without stress education (d = 0.44, 95% CI [0.25–0.63], 95% PI [−0.05–0.93], p < 0.001). Facilitator type significantly impacted effect size (Q = 4.39, p = 0.03) with interventions led by faculty, mental health professionals, or researchers having a higher effect size (d = 0.84, 95% CI [0.52–1.16], 95% PI [−0.43 = 2.11], p < 0.001) compared to those led by student peers or which were self-directed (d = 0.39, 95% CI [0.12–0.66], 95% PI [−0.71–1.49], p < 0.01). The inclusion of CBT, mindfulness, homework, and small groups was not significantly different than those without those elements (Table 2), though the small sample sizes of the studies with these modalities may have meant it was not possible to detect a significant difference, even if one existed. There were not enough subgroups to assess study location (country).
Meta-regression analyses were done for mean age, percent female participants, number of weeks in the intervention, total number of sessions, and average duration of sessions. The average duration of sessions was the only significant finding (F(1, 12) = 6.59, p = 0.03, n = 11, goodness-of-fit: T = 0.39, T2 = 0.15, I2 = 85.5%, Q = 62.0, p < 0.001, R2 = 44%), indicating that longer average sessions were less effective and explaining 44% of the variance (Fig. 4). However, removal of the single study with the highest average duration of sessions (180 min) [55] resulted in insignificance of the model (F(1, 11) = 2.02, p = 0.18, goodness-of-fit: T = 0.45, T2 = 0.20, I2 = 88.7%, Q = 97.1, p < 0.001, R2 = 23%).
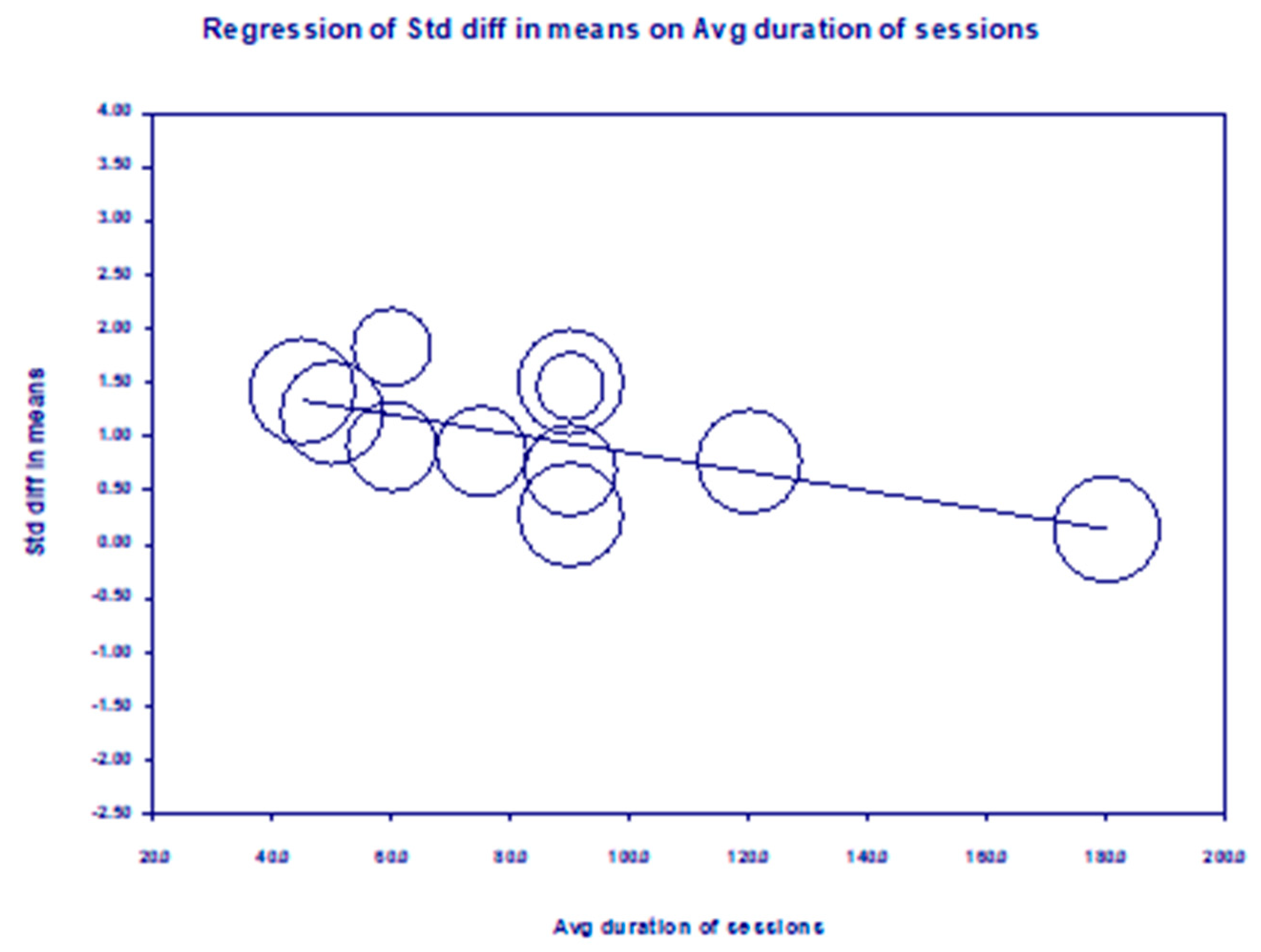
Figure 4: Meta-regression for average session duration.
Table 2: Moderator analyses.
| Subgroups | Qbetween | k | Cohen’s d | 95% CI |
|---|---|---|---|---|
| Study design | 6.81* | |||
| RCT | 8 | 0.91*** | 0.55–1.27 | |
| Non-randomized w/control group | 6 | 0.80** | 0.20–1.40 | |
| One-arm pre/post | 4 | 0.36** | 0.11–0.61 | |
| Student discipline | 7.19* | |||
| Medical students | 3 | 1.07** | 0.28–1.86 | |
| Nursing students | 14 | 0.67*** | 0.43–0.92 | |
| Stress education | 3.77* | |||
| Included | 12 | 0.85*** | 0.48–1.21 | |
| Not included | 6 | 0.44*** | 0.25–0.63 | |
| Facilitator type | 4.39* | |||
| Faculty/MH professional/researcher | 13 | 0.84*** | 0.52–1.16 | |
| Peer/self-led | 5 | 0.39** | 0.12–0.66 | |
| CBT | 1.51 | |||
| Included | 5 | 1.03*** | 0.47–1.59 | |
| Not included | 13 | 0.63*** | 0.34–0.92 | |
| Mindfulness | 1.09 | |||
| Included | 4 | 0.98*** | 0.36–1.60 | |
| Not included | 14 | 0.63** | 0.40–0.86 | |
| Homework | 1.58 | |||
| Included | 11 | 0.86*** | 0.49–1.23 | |
| Not included | 7 | 0.54** | 0.20–0.88 | |
| Small groups | 0.43 | |||
| Included | 11 | 0.67*** | 0.35–0.99 | |
| Not included | 7 | 0.86*** | 0.40–1.31 | |
| In-person vs. online | 0.69 | |||
| In-person | 14 | 0.79*** | 0.48–1.09 | |
| Online | 4 | 0.53*** | 0.02–1.05 | |
| Meta-regression | coefficient | k | p value | 95% CI |
| Mean age | −0.16 | 16 | 0.22 | −0.44–0.12 |
| Percent female | −0.02 | 14 | 0.14 | −0.04–0.01 |
| # weeks of intervention | −0.05 | 16 | 0.30 | −0.16–0.06 |
| Total # sessions | −0.02 | 15 | 0.52 | −0.11–0.06 |
| Avg duration of sessions | −0.01 | 14 | 0.03 | −0.02–−0.00 |
3.7 Risk of Bias in Primary Studies
In the RCTs, there were some concerns of bias according to RoB2 (Fig. 5) [50]. Over half of the studies lacked trial registration or protocols, raising the possibility of selective reporting. All studies relied on self-reported outcome measures, which increases the risk of bias, and were subsequently coded as having “some concerns”.
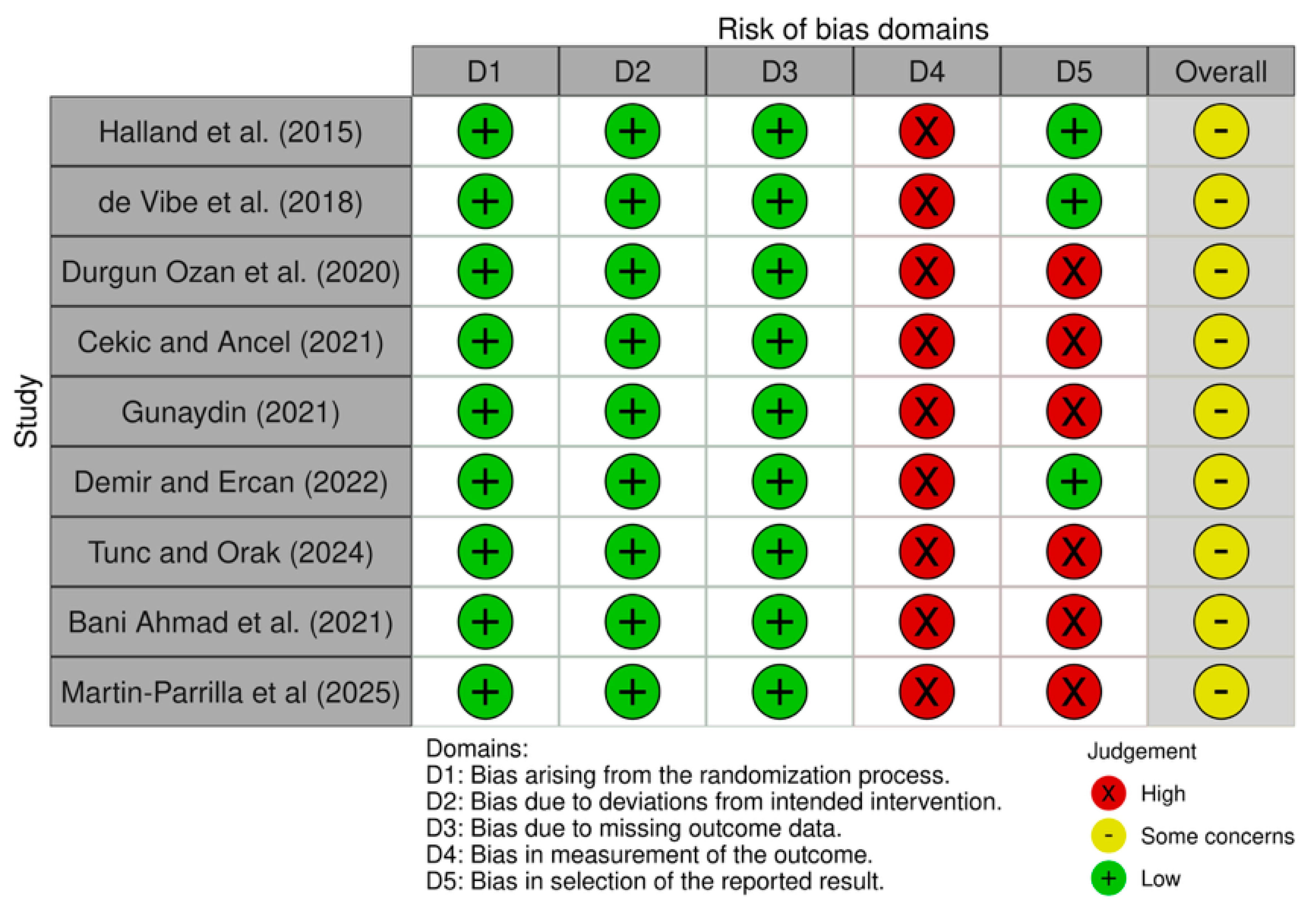
Figure 5: Risk of bias using RoB 2: A revised tool for assessing risk of bias in randomized trials for the RCT studies included in this meta-analysis. Note: RoB2: Version 2 of the Cochrane risk-of-bias tool for randomized trials; RCT: Randomized Controlled Trial.
There were some critical and serious risks of bias in the non-RCTs and pre/post studies of this meta-analysis as evaluated in ROBINS-I (Fig. 6) [51]. These studies did not have a controlled variable, such as baseline stress or prior mental health. None of the studies had pre-registered protocols, which increases bias in the outcome. Participants were not blinded to group assignment, nor had any objective or biomarker-based outcome measures, increasing the likelihood of reporting bias.
It is important to note here that the RoB2 and ROBINS-I tools both assume that a power calculation has been conducted and the sample is sufficiently powered to detect statistically significant differences [50,51]. The low power of many of the included studies should be recognized as a limitation to the accuracy of risk-of-bias results.
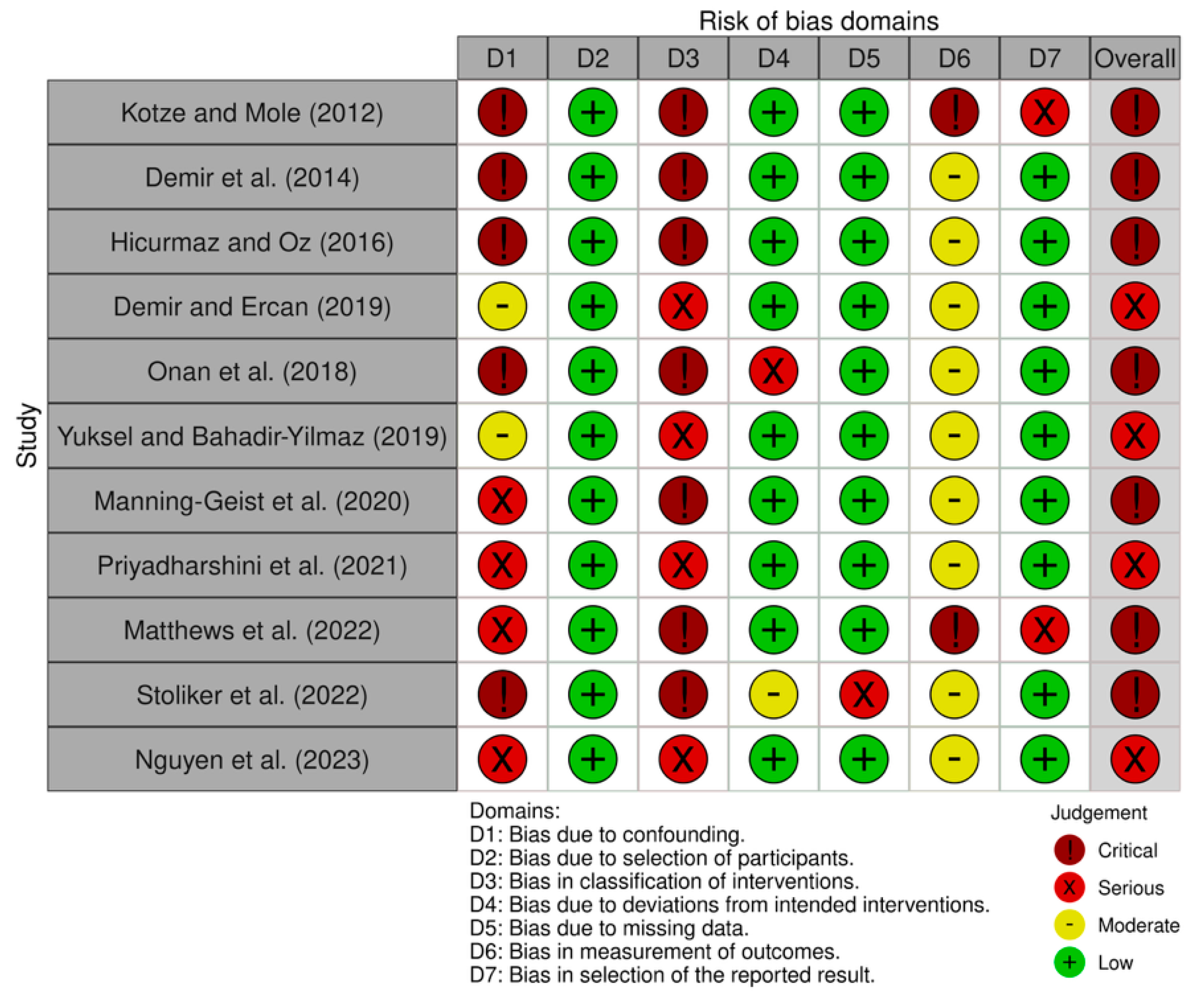
Figure 6: Risk of bias using ROBIN-I: A revised tool for assessing risk of bias in non-randomized studies for the non-RCT and pre/post studies in this meta-analysis. Note: ROBIN-I: Risk of Bias In Non-Randomized Studies—of Interventions; RCT: Randomized Controlled Trial.
This systematic review and meta-analysis summarizes the current evidence based on the effectiveness of stress coping interventions among international healthcare students. The findings directly address the research questions outlined in the introduction: (1) interventions used to improve healthcare professional students included stress education, cognitive behavioral therapy, and mindfulness training; (2) stress coping interventions improved students’ ability to have a self-confident approach or have a more problem-focused coping when dealing with stress; (3) characteristics of the populations that influenced the effectiveness of the interventions were inconclusive as most of the studies were from Turkey and had limited diversity in the type of students and the impact of specific intervention characteristics on students’ stress coping are detailed below. Significant findings include a significant, moderate-to-large positive summary effect size of d = 0.74 across the 17 primary studies. There was a large variation in the type of coping interventions, duration in weeks, time allotted per session, and delivery method, which were assessed with moderator analyses. The inclusion of homework and small groups did not appear to enhance coping abilities, though sample sizes were small and the number of studies was quite limited. The data suggest that decreasing the hours of intervention improved coping, although removing the intervention with the highest amount of time resulted in insignificance in the model, which may suggest that interventions over two hours do not significantly enhance outcomes. Alternatively, because healthcare students have limited free time, shorter interventions may be more manageable. Interventions led by faculty, mental health professionals, or researchers were more helpful than those led by student peers or programs that were self-directed. This could be because programs led by someone who is more established help in the organization and direction of the intervention. Stress education was the most studied intervention and demonstrated the most positive effect on improving coping outcomes compared to interventions without stress education.
Interventions varied significantly, but many contained stress education. Stress education that was synchronously taught was mainly facilitated by instructors who had training in psychiatry [57,62]. The interventions were reported to effectively increase students’ ability to cope with stress compared to stress education interventions that were taught through a mentorship program or an online module [52,64,66]. In two studies, students were instructed to practice stress-reduction skills between sessions and report their experiences in the follow-up sessions [31,57]. Home practice showed improved stress coping and management immediately after the intervention and in the 6-month follow-up [31,57]. The home practice assignments included writing assignments, such as a stress diary [23], a gratitude journal, self-reflection, and deep breathing [31], or a short reflective assignment on different stress topics, such as nonverbal behaviors, explaining emotions and thoughts, assertiveness, and social skills [56]. Online interventions variously contained readings, videos, and questionnaires pertaining to stress [52,64].
Many interventions included didactic information on stress and burnout, such as definitions, stress and its effects, hypothesized contributors, recognition in self and others, management, and approaches [23,56,60]. One study included a panel discussion and small group breakout session, which was helpful in improving students’ confidence and attitudes on coping with stress, but was not effective for long-term management [60]. One intervention had students create a written report and book presentation with visual materials and handouts in addition to their weekly homework throughout the program, which was successful in improving active coping skills in the short-term [56]. Other activities included breathing and stretching exercises reinforced twice a week, which were reported to significantly decrease perceived stress [23].
Stress education was also used in combination with other coping strategies, such as Mindfulness-Based Stress Reduction [70], which includes mindfulness and yoga, or the Transforming Stress program, which combines cognitive behavioral training and dialectical behavioral training with stress education [31,58]. There were also successful online programs, such as the Student Success Program that used Zoom to conduct the sessions and the Online Resilience Resource that is designed as a web-based, self-paced course [64] that could help students avoid commute time or complete the program while ill or on a leave-of-absence.
Several important limitations must be mentioned. There were relatively few studies eligible for the meta-analysis. There was unequal sampling across geographic location, with 11 of the 17 studies taking place in Turkey and published in the same journal, which makes it difficult to draw conclusions about the differences between countries or cultures, increases publication bias, and results in less generalizable conclusions. The studies were English-language or English translations, so non-English studies could have been missed, contributing to language and country bias. Very few studies have been done among veterinary and allied health students, limiting comparisons between disciplines. Furthermore, the risk of bias was moderate to high overall; there were eight RCTs among the primary articles, and only three of those were clearly adequately powered to detect a significant difference between groups [58,61,63]. Of the remaining RCTs, sample sizes were very small (n = 1053 and n = 3857), there was no power calculation done [52], or there was a power calculation noted but without adequate detail to assess its accuracy [55]. Heterogeneity was quite high, as is typical among studies drawn from the literature, but cultural differences, measurement tool variation (11 different tools among 17 studies), and significant differences across interventions make even moderation analyses less reliable.
All studies except one included primarily white individuals, and demographic data on LGBTQIA+ individuals, gender identity, socioeconomic status, and religion were absent. Future research focusing on and including non-white, LGBTQIA+, gender minorities, and other underrepresented groups of healthcare students is important to determine who would likely benefit from coping interventions.
The current study presents a systematic review and meta-analysis examining the effect of coping interventions for academic stress among healthcare students, including medical, dental, nursing, physician assistant, allied health, veterinary, and clinical psychology students. After a comprehensive literature search, 17 studies were included, finding that coping interventions significantly reduced stress outcomes among healthcare students as a whole (d = 0.74; 95% CI [0.48–1.01], 95% PI [−0.41–1.90], p < 0.001, Q = 228.49, I2 = 93.0%, T = 0.52, T2 = 0.28, p < 0.001). Moderator analysis suggested that interventions with stress education and professional guidanceled to better stress management outcomes. However, there is a clear lack of sufficiently powered RCTs from which to draw conclusions, as many studies were underpowered and not randomized. Future research investigating coping interventions with robust, sufficiently powered, RCTs is needed. Research is also particularly lacking among non-medical and marginalized health care students.
Acknowledgement:
Funding Statement: The authors received no specific funding.
Author Contributions: The authors confirm contribution to the paper as follows: Conceptualization, Edie L. Sperling; methodology, Natalie Y. Luo, Juliette Lum, Edie L. Sperling; validation, Natalie Y. Luo, Juliette Lum, Edie L. Sperling; investigation, Natalie Y. Luo, Juliette Lum, Edie L. Sperling; data curation, Natalie Y. Luo, Juliette Lum, Edie L. Sperling; writing the original draft, Natalie Y. Luo, Juliette Lum, Edie L. Sperling; reviewing and editing, Natalie Y. Luo, Juliette Lum, Edie L. Sperling; visualization, Natalie Y. Luo, Juliette Lum, Edie L. Sperling; supervision, Edie L. Sperling; project administration, Edie L. Sperling. All authors reviewed and approved the final version of the manuscript.
Availability of Data and Materials: The authors confirm that the data supporting the findings of this study are available within the article and its Supplementary Materials.
Ethics Approval: Not applicable.
Conflicts of Interest: The authors declare no conflicts of interest to report.
Supplementary Materials: The supplementary material is available online at https://www.techscience.com/doi/10.32604/ijmhp.2026.074948/s1.
References
1. Al-Dabal BK , Koura MR , Rasheed P , Al-Sowielem L , Makki SM . A comparative study of perceived stress among female medical and non-medical university students in Dammam, Saudi Arabia. Sultan Qaboos Univ Med J. 2010; 10( 2): 231– 40. doi:10.18295/2075-0528.1192. [Google Scholar] [CrossRef]
2. Rink LC , Oyesanya TO , Adair KC , Humphreys JC , Silva SG , Sexton JB . Stressors among healthcare workers: a summative content analysis. Glob Qual Nurs Res. 2023; 10: 23333936231161127. doi:10.1177/23333936231161127. [Google Scholar] [CrossRef]
3. Al-Shahrani MM , Alasmri BS , Al-Shahrani RM , Al-Moalwi NM , Al Qahtani AA , Siddiqui AF . The prevalence and associated factors of academic stress among medical students of king khalid university: an analytical cross-sectional study. Healthcare. 2023; 11( 14): 2029. doi:10.3390/healthcare11142029. [Google Scholar] [CrossRef]
4. Yalim AC , Daly K , Bailey M , Kay D , Zhu X , Patel M , et al. Wellness and stress management practices among healthcare professionals and health professional students. Am J Health Promot. 2025; 39( 2): 204– 14. doi:10.1177/08901171241275868. [Google Scholar] [CrossRef]
5. Voltmer E , Köslich-Strumann S , Voltmer JB , Kötter T . Stress and behavior patterns throughout medical education—a six year longitudinal study. BMC Med Educ. 2021; 21( 1): 454. doi:10.1186/s12909-021-02862-x. [Google Scholar] [CrossRef]
6. Ibnian D , Barba A , Mojtahedi S , Friesen D , Oyoyo U , Kwon SR . Assessment of stress levels and coping strategies among students at a dental school in southern California. J Calif Dent Assoc. 2025; 53: 2539525. doi:10.1080/19424396.2025.2539525. [Google Scholar] [CrossRef]
7. Labrague LJ . Umbrella review: stress levels, sources of stress, and coping mechanisms among student nurses. Nurs Rep. 2024; 14( 1): 362– 75. doi:10.3390/nursrep14010028. [Google Scholar] [CrossRef]
8. Alamoush RA , Al-sawaeir S , Abu Baker D , Aljamani SA , Alomoush SA , AL-Omiri MK . Stress experienced by dental students performing clinical training in different dental disciplines: a cross-sectional study. J Occup Health. 2024; 66: uiae006. doi:10.1093/joccuh/uiae006. [Google Scholar] [CrossRef]
9. Islam RK , Cobb EK , McCowan HK , Watson K , Bhattacharya K , Chandra A , et al. Exploring mental health in veterinary students: common stressors and effective coping strategies: a narrative review. Front Vet Sci. 2025; 12: 1470022. doi:10.3389/fvets.2025.1470022. [Google Scholar] [CrossRef]
10. Frese E , Hawthorne K , Kettenbach G , FitzGerald J , Katz I . Professional physical therapist student well-being and career attitudes. J Allied Health. 2021; 50( 4): 307– 13. [Google Scholar]
11. Pfeifer TA , Kranz PL , Scoggin AE . Perceived stress in occupational therapy students. Occup Ther Int. 2008; 15( 4): 221– 31. doi:10.1002/oti.256. [Google Scholar] [CrossRef]
12. Russ SJ , Morrison I , Bell C , Morse JC , MacKenzie RK , Johnston MK . Relationship between acute stress and clinical performance in medical students: a pilot simulation study. BMJ Simul Technol Enhanc Learn. 2018; 4( 4): 171– 8. doi:10.1136/bmjstel-2017-000276. [Google Scholar] [CrossRef]
13. Girotti M , Bulin SE , Carreno FR . Effects of chronic stress on cognitive function—from neurobiology to intervention. Neurobiol Stress. 2024; 33: 100670. doi:10.1016/j.ynstr.2024.100670. [Google Scholar] [CrossRef]
14. Anton NE , Rendina MA , Hennings JM , Stambro R , Stanton-Maxey KJ , Stefanidis D . Association of medical students' stress and coping skills with simulation performance. Sim Healthcare. 2021; 16( 5): 327– 33. doi:10.1097/sih.0000000000000511. [Google Scholar] [CrossRef]
15. Mhata NT , Ntlantsana V , Tomita AM , Mwambene K , Saloojee S . Prevalence of depression, anxiety and burnout in medical students at the University of Namibia. S Afr J Psychiatr. 2023; 29: 2044. doi:10.4102/sajpsychiatry.v29i0.2044. [Google Scholar] [CrossRef]
16. Almutairi H , Alsubaiei A , Abduljawad S , Alshatti A , Fekih-Romdhane F , Husni M , et al. Prevalence of burnout in medical students: a systematic review and meta-analysis. Int J Soc Psychiatry. 2022; 68( 6): 1157– 70. doi:10.1177/00207640221106691. [Google Scholar] [CrossRef]
17. Mangoulia P , Kanellopoulou A , Manta G , Chrysochoou G , Dimitriou E , Kalogerakou T , et al. Exploring the levels of stress, anxiety, depression, resilience, hope, and spiritual well-being among Greek dentistry and nursing students in response to academic responsibilities two years after the COVID-19 pandemic. Healthcare. 2024; 13( 1): 54. doi:10.3390/healthcare13010054. [Google Scholar] [CrossRef]
18. Dutheil F , Aubert C , Pereira B , Dambrun M , Moustafa F , Mermillod M , et al. Suicide among physicians and health-care workers: a systematic review and meta-analysis. PLoS One. 2019; 14( 12): e0226361. doi:10.1371/journal.pone.0226361. [Google Scholar] [CrossRef]
19. Pereira-Lima K , Mata DA , Loureiro SR , Crippa JA , Bolsoni LM , Sen S . Association between physician depressive symptoms and medical errors: a systematic review and meta-analysis. JAMA Netw Open. 2019; 2( 11): e1916097. doi:10.1001/jamanetworkopen.2019.16097. [Google Scholar] [CrossRef]
20. Cummerow J , Obst K , Voltmer E , Kötter T . Medical students' coping with stress and its predictors: a cross-sectional study. Int J Med Educ. 2023; 14: 11– 8. doi:10.5116/ijme.63de.3840. [Google Scholar] [CrossRef]
21. Silverman J , Aafjes-van Doorn K . Coping and defense mechanisms: a scoping review. Clin Psychol Sci Pract. 2023; 30( 4): 381– 92. doi:10.1037/cps0000139. [Google Scholar] [CrossRef]
22. Manley AE , Biddle L , Savović J , Moran P . The positive and negative consequences of stress and its relationship with coping in medical students: a qualitative study. Med Teach. 2025; 47( 2): 323– 8. doi:10.1080/0142159X.2024.2333799. [Google Scholar] [CrossRef]
23. Priyadharshini KM , George N , Britto DR , Nirmal SR , Tamilarasan M , Kulothungan K . Assessment of stress, resilience, and coping style among medical students and effectiveness of intervention programs on stress level in south India: a non-randomized control trial. Indian J Community Med. 2021; 46( 4): 735– 8. doi:10.4103/ijcm.IJCM_157_21. [Google Scholar] [CrossRef]
24. Folkman S , Moskowitz JT . Coping: pitfalls and promise. Annu Rev Psychol. 2004; 55: 745– 74. doi:10.1146/annurev.psych.55.090902.141456. [Google Scholar] [CrossRef]
25. Compas BE , Jaser SS , Bettis AH , Watson KH , Gruhn MA , Dunbar JP , et al. Coping, emotion regulation, and psychopathology in childhood and adolescence: a meta-analysis and narrative review. Psychol Bull. 2017; 143( 9): 939– 91. doi:10.1037/bul0000110. [Google Scholar] [CrossRef]
26. Sattar K , Yusoff MSB , Arifin WN , Yasin MAM , Nor MZM . Effective coping strategies utilised by medical students for mental health disorders during undergraduate medical education—a scoping review. BMC Med Educ. 2022; 22( 1): 121. doi:10.1186/s12909-022-03185-1. [Google Scholar] [CrossRef]
27. Onieva-Zafra MD , Fernández-Muñoz JJ , Fernández-Martínez E , García-Sánchez FJ , Abreu-Sánchez A , Parra-Fernández ML . Anxiety, perceived stress and coping strategies in nursing students: a cross-sectional, correlational, descriptive study. BMC Med Educ. 2020; 20: 370. doi:10.1186/s12909-020-02294-z. [Google Scholar] [CrossRef]
28. Lavoie-Tremblay M , Sanzone L , Aubé T , Paquet M . Sources of stress and coping strategies among undergraduate nursing students across all years. Can J Nurs Res. 2022; 54( 3): 261– 71. doi:10.1177/08445621211028076. [Google Scholar] [CrossRef]
29. Ramachandran S , Soheilipour S , Ford NL , Brondani MA . Exploring stressors and coping strategies among dental students during COVID-19 pandemic in British Columbia. J Dent Educ. 2023; 87( 10): 1427– 36. doi:10.1002/jdd.13312. [Google Scholar] [CrossRef]
30. Webber SC , Wener P , MacDonald LL , Tittlemier BJ , Hahn F , Cooper JE . This program should come with a warning sign!: mental wellness in occupational therapy and physical therapy students. J Am Coll Health. 2022; 70( 8): 2491– 8. doi:10.1080/07448481.2020.1865983. [Google Scholar] [CrossRef]
31. Nguyen T , Pu C , Waits A , Tran TD , Ngo TH , Huynh QTV , et al. Transforming stress program on medical students’ stress mindset and coping strategies: a quasi-experimental study. BMC Med Educ. 2023; 23( 1): 587. doi:10.1186/s12909-023-04559-9. [Google Scholar] [CrossRef]
32. Hirsch JD , Nemlekar P , Phuong P , Hollenbach KA , Lee KC , Adler DS , et al. Patterns of stress, coping and health-related quality of life in doctor of pharmacy students. Am J Pharm Educ. 2020; 84( 3): 7547. doi:10.5688/ajpe7547. [Google Scholar] [CrossRef]
33. Lee HF , Kuo CC , Chien TW , Wang YR . A meta-analysis of the effects of coping strategies on reducing nurse burnout. Appl Nurs Res. 2016; 31: 100– 10. doi:10.1016/j.apnr.2016.01.001. [Google Scholar] [CrossRef]
34. Maresca G , Corallo F , Catanese G , Formica C , Lo Buono V . Coping strategies of healthcare professionals with burnout syndrome: a systematic review. Medicina. 2022; 58( 2): 327. doi:10.3390/medicina58020327. [Google Scholar] [CrossRef]
35. Spaan P , van den Boogert F , Bouman YHA , Hoogendijk WJG , Roza SJ . How are you coping? Stress, coping, burnout, and aggression in forensic mental healthcare workers. Front Psychol. 2024; 14: 1301878. doi:10.3389/fpsyg.2023.1301878. [Google Scholar] [CrossRef]
36. Fitzgibbon K , Murphy KD . Coping strategies of healthcare professional students for stress incurred during their studies: a literature review. J Ment Health. 2023; 32( 2): 492– 503. doi:10.1080/09638237.2021.2022616. [Google Scholar] [CrossRef]
37. Liu M , Yan Z , Wu C . Comparative efficacy and acceptability of resilience-focused interventions for nurses: a systematic review and network meta-analysis of randomized controlled trials. BMC Nurs. 2025; 24( 1): 418. doi:10.1186/s12912-025-03090-0. [Google Scholar] [CrossRef]
38. Yusoff MSB . Interventions on medical students’ psychological health: a meta-analysis. J Taibah Univ Med Sci. 2014; 9( 1): 1– 13. doi:10.1016/j.jtumed.2013.09.010. [Google Scholar] [CrossRef]
39. Bennett-Weston A , Keshtkar L , Jones M , Sanders C , Lewis C , Nockels K , et al. Interventions to promote medical student well-being: an overview of systematic reviews. BMJ Open. 2024; 14( 5): e082910. doi:10.1136/bmjopen-2023-082910. [Google Scholar] [CrossRef]
40. Sperling EL , Hulett JM , Sherwin LB , Thompson S , Bettencourt BA . The effect of mindfulness interventions on stress in medical students: a systematic review and meta-analysis. PLoS One. 2023; 18( 10): e0286387. doi:10.1371/journal.pone.0286387. [Google Scholar] [CrossRef]
41. Alzahem AM , Van der Molen HT , Alaujan AH , De Boer BJ . Stress management in dental students: a systematic review. Adv Med Educ Pract. 2014; 5: 167– 76. doi:10.2147/AMEP.S46211. [Google Scholar] [CrossRef]
42. Mayberry K , Zapata LV , Byers M , Thurston MM . A scoping review of well-being assessment and interventions in student pharmacists. Am J Pharm Educ. 2022; 86( 6): 8793. doi:10.5688/ajpe8793. [Google Scholar] [CrossRef]
43. Ji X , Guo X , Soh KL , Japar S , He L . Effectiveness of stress management interventions for nursing students: a systematic review and meta-analysis. Nurs Health Sci. 2024; 26( 2): e13113. doi:10.1111/nhs.13113. [Google Scholar] [CrossRef]
44. Page MJ , McKenzie JE , Bossuyt PM , Boutron I , Hoffmann TC , Mulrow CD , et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021; 372: n71. doi:10.1136/bmj.n71. [Google Scholar] [CrossRef]
45. Folk D , Dunn E . A systematic review of the strength of evidence for the most commonly recommended happiness strategies in mainstream media. Nat Hum Behav. 2023; 7( 10): 1697– 707. doi:10.1038/s41562-023-01651-4. [Google Scholar] [CrossRef]
46. Sperling EL , Khoury B , Sutton A , Price-Blackshear MA , Bettencourt BA . Enhancing rigor in quantitative meta-analyses for mindfulness research: a comprehensive guide. Mindfulness. 2025; 16( 2): 315– 31. doi:10.1007/s12671-025-02517-8. [Google Scholar] [CrossRef]
47. Cooper H . Research synthesis and meta-analysis: a step-by-step approach. Thousand Oaks, CA, USA: SAGE Publications; 2017. doi:10.4135/9781071878644. [Google Scholar] [CrossRef]
48. Lin L , Aloe AM . Evaluation of various estimators for standardized mean difference in meta-analysis. Stat Med. 2021; 40( 2): 403– 26. doi:10.1002/sim.8781. [Google Scholar] [CrossRef]
49. Cohen J . Statistical power analysis for the behavioral sciences. London, UK: Routledge; 2013. doi:10.4324/9780203771587. [Google Scholar] [CrossRef]
50. Sterne JAC , Savović J , Page MJ , Elbers RG , Blencowe NS , Boutron I , et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019; 366: l4898. doi:10.1136/bmj.l4898. [Google Scholar] [CrossRef]
51. Sterne JA , Hernán MA , Reeves BC , Savović J , Berkman ND , Viswanathan M , et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ. 2016; 355: i4919. doi:10.1136/bmj.i4919. [Google Scholar] [CrossRef]
52. Bani Ahmad T , Meriç M . The effect of an online psychoeducational stress management program on international students' ability to cope and adapt. Perspect Psychiatr Care. 2021; 57( 4): 1673– 84. doi:10.1111/ppc.12735. [Google Scholar] [CrossRef]
53. Çekiç Y , Ançel G . Effects of interpersonal relational role analysis on nursing students’ depressive symptoms and coping styles. Perspect Psychiatr Care. 2022; 58( 4): 1587– 98. doi:10.1111/ppc.12966. [Google Scholar] [CrossRef]
54. Demir S , Ercan F . The effect of a self-awareness and communication techniques course on the communication skills and ways of coping with stress of nursing students: an interventional study in Ankara, Turkey. J Pak Med Assoc. 2019; 69( 5): 659– 65. [Google Scholar]
55. Demir S , Ercan F . The effectiveness of cognitive behavioral therapy-based group counseling on depressive symptomatology, anxiety levels, automatic thoughts, and coping ways Turkish nursing students: a randomized controlled trial. Perspect Psychiatr Care. 2022; 58( 4): 2394– 406. doi:10.1111/ppc.13073. [Google Scholar] [CrossRef]
56. Demir S , Demir SG , Bulut H , Hisar F . Effect of mentoring program on ways of coping with stress and locus of control for nursing students. Asian Nurs Res. 2014; 8( 4): 254. doi:10.1016/j.anr.2014.10.004. [Google Scholar] [CrossRef]
57. Günaydin N . Effect of group psychoeducation on depression, anxiety, stress and coping with stress of nursing students: a randomized controlled study. Perspect Psychiatr Care. 2022; 58( 2): 640– 50. doi:10.1111/ppc.12828. [Google Scholar] [CrossRef]
58. Halland E , de Vibe M , Solhaug I , Friborg O , Rosenvinge JH , Tyssen R , et al. Mindfulness training improves problem-focused coping in psychology and medical students: Results from a random-ized controlled trial. Coll Stud J. 2015; 49( 3): 387– 98. [Google Scholar]
59. Hiçdurmaz D , Öz F . Interpersonal sensitivity, coping ways and automatic thoughts of nursing students before and after a cognitive-behavioral group counseling program. Nurse Educ Today. 2016; 36: 152. doi:10.1016/j.nedt.2015.09.006. [Google Scholar] [CrossRef]
60. Manning-Geist B , Meyer F , Chen J , Pelletier A , Kosman K , Chen XP , et al. Pre-clinical stress management workshops increase medical students’ knowledge and self-awareness of coping with stress. Med Sci Educ. 2020; 30( 1): 235. doi:10.1007/s40670-019-00881-4. [Google Scholar] [CrossRef]
61. Martín-Parrilla MÁ , Durán-Gómez N , López-Jurado CF , Montanero-Fernández J , Cáceres MC . Impact of simulation-based learning experiences on enhancing coping with death in nursing students: an experimental study. Clin Simul Nurs. 2025; 103: 101740. doi:10.1016/j.ecns.2025.101740. [Google Scholar] [CrossRef]
62. Onan N , Karaca S , Unsal Barlas G . Evaluation of a stress coping course for psychological resilience among a group of university nursing students. Perspect Psychiatr Care. 2019; 55( 2): 233– 8. doi:10.1111/ppc.12340. [Google Scholar] [CrossRef]
63. Durgun Ozan Y , Duman M , Çiçek Ö , Baksi A . The effects of clinical education program based on Watson’s theory of human caring on coping and anxiety levels of nursing students: a randomized control trial. Perspect Psychiatr Care. 2020; 56( 3): 621– 8. doi:10.1111/ppc.12477. [Google Scholar] [CrossRef]
64. Stoliker BE , Vaughan AD , Collins J , Black M , Anderson GS . Building personal resilience following an online resilience training program for BScN students. West J Nurs Res. 2022; 44( 8): 755. [Google Scholar]
65. Tunç E , Orak OS . The impact of a “clinical adaptation psychoeducation program” grounded in the psychological flexibility model on perceived stress and coping behaviors among nursing students: a randomized controlled experimental study. Nurse Educ Today. 2024; 139: 106230. doi:10.1016/j.nedt.2024.106230. [Google Scholar] [CrossRef]
66. Yüksel A , Bahadir-Yilmaz E . The effect of mentoring program on adjustment to university and ways of coping with stress in nursing students: a quasi-experimental study. Nurse Educ Today. 2019; 80: 52. doi:10.1016/j.nedt.2019.06.006. [Google Scholar] [CrossRef]
67. Kossmeier M , Tran US , Voracek M . Visual inference for the funnel plot in meta-analysis. Z Für Psychol. 2019; 227( 1): 83– 9. doi:10.1027/2151-2604/a000358. [Google Scholar] [CrossRef]
68. Egger M , Smith GD , Schneider M , Minder C . Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997; 315( 7109): 629– 34. doi:10.1136/bmj.315.7109.629. [Google Scholar] [CrossRef]
69. Duval S , Tweedie R . Trim and fill: a simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics. 2000; 56( 2): 455– 63. doi:10.1111/j.0006-341x.2000.00455.x. [Google Scholar] [CrossRef]
70. Kabat-Zinn J . Mindfulness Based Stress Reduction (MBSR). Constr Hum Sci. 2003; 8( 2): 73– 107. [Google Scholar]
Cite This Article
 Copyright © 2026 The Author(s). Published by Tech Science Press.
Copyright © 2026 The Author(s). Published by Tech Science Press.This work is licensed under a Creative Commons Attribution 4.0 International License , which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
 Downloads
Downloads
 Citation Tools
Citation Tools