
 Submit a Paper
Submit a Paper Propose a Special lssue
Propose a Special lssue Open Access
Open Access
ARTICLE

Initial case series and perioperative outcomes of single-port robotic radical prostatectomy: the Italian experience
1 Department of Urology, Istituto Nazionale Tumori, IRCCS, “Fondazione G. Pascale”, Naples, 80136, Italy
2 Department of Urology, University of L’Aquila, L’Aquila, 67100, Italy
3 Department of Urology, San Carlo di Nancy Hospital, Rome, 00165, Italy
* Corresponding Author: Roberto Contieri. Email:
(This article belongs to the Special Issue: Prostate Cancer: Biomarkers, Diagnosis and Treatment)
Canadian Journal of Urology 2026, 33(1), 117-123. https://doi.org/10.32604/cju.2025.068026
Received 19 May 2025; Accepted 05 November 2025; Issue published 28 February 2026
 View Full Text
View Full Text Download PDF
Download PDFAbstract
Background: The Da Vinci Single-Port Robotic System (Da Vinci-SP), introduced by Intuitive (CA, USA) in 2018 in the USA and in 2024 in Europe, integrates advanced features like a flexible camera and articulating instruments. It has garnered significant interest in urology. Our report presents the first described European series of Radical Prostatectomies using the Da Vinci SP at the leading Italian center, Istituto Nazionale Tumori di Napoli, IRCCS “G. Pascale” Foundation, detailing the technical differences and challenges faced by experienced multiport robotic surgeons. Methods: Sixteen patients have been enrolled and underwent Single-Port (SP) Robot-Assisted Radical Prostatectomy (SP-RARP). Baseline characteristics of the patients were collected. We provided a step-by-step description of the surgical technique. Oncological outcomes have been evaluated and compared with magnetic resonance imaging (MRI) and biopsy results. Intraoperative, perioperative, and postoperative complications, surgical outcomes, functional outcomes, and technical issues of the new system were also documented. Results: All surgeries were successfully performed without the need for conversion. An extraperitoneal approach was used for all patients. Median Console time was 110 min. No complications were reported. The estimated median blood loss was 175 cc. Discharge from the hospital was on the first post-operative day for all patients. Bladder catheter removal was on day 7 without the need for cystography. Conclusions: We presented the first European case series of SP-RARP, reporting our experience and confirming the procedure’s feasibility for a highly experienced robotic surgeon. Experience with an extraperitoneal approach using the multiport (MP) platform, combined with well-conducted training for the SP system, may facilitate the transition to SP surgery. Further procedures and studies are needed to evaluate the oncological and functional outcomes.Keywords
The introduction of the Da Vinci Single-Port (Da Vinci SP) robotic system by Intuitive Surgical represents a major advancement in minimally invasive surgery. Building upon the proven success of the multi-port da Vinci platforms, the SP system is specifically designed to further reduce surgical invasiveness while maintaining the precision and dexterity that define robotic-assisted surgery. First launched in the U.S. market in 2018, the Da Vinci SP made its European debut in 2024.1 Initially employed for prostate and kidney surgeries, the SP platform has since demonstrated its adaptability in a range of reconstructive urological procedures.2–4 Its versatility is underscored by the absence of limitations regarding the types of surgeries it can support.5,6
The Da Vinci SP system features a single-arm robotic platform that introduces advanced surgical tools and a flexible 3D camera, improving precision and flexibility within the surgical field. A standout feature of this platform is its ability to consolidate all robotic instruments and the camera into a single 2.5 cm multichannel port, inserted through a single skin incision. This streamlined approach reduces postoperative pain and offers clear cosmetic benefits for patients, resulting in less scarring and faster recovery times.7,8
The objective of our study was to describe the first series of Radical Prostatectomies performed with the new Da Vinci SP in a high-volume center in Italy (Istituto Nazionale Tumori di Napoli, IRCCS “G. Pascale”), highlighting the technical differences and difficulties reported by an experienced multiport robotic surgeon, and to report the perioperative outcomes. We also aimed to describe our step-by-step surgical approach.
This retrospective study analyzed sixteen consecutive extraperitoneal SP-RARPs conducted between 08 May 2024 and 25 May 2024, using the da Vinci SP® Surgical System (Intuitive Surgical, Sunnyvale, CA, USA) in Istituto Nazionale Tumori di Napoli, IRCCS “G. Pascale”. All surgeries were performed by a single, highly experienced surgeon supported by a skilled surgical team who also completed comprehensive training in single-port (SP) robotic surgery. 3D reconstruction models were available for all the procedures (Medics 3D, HA3D®).
Patients with clinically localized prostate cancer were considered suitable for the procedure. Patients with high-risk disease or requiring extended pelvic lymph node dissection (PLND) were not considered for SP-RARP in this initial experience.
Preoperative evaluations included staging exams (computed tomography [CT], bone scan), routine blood tests, total prostate-specific antigen (PSA) measurement, and multiparametric magnetic resonance imaging (MRI) of the prostate.
All patients provided written informed consent for participation and for the use of their anonymized clinical data for research purposes. This retrospective study was conducted using fully anonymized data collected for clinical purposes. According to institutional and national regulations, ethical committee approval was not required.
A totally extraperitoneal approach for radical prostatectomy was performed, leveraging the advantages of the SP platform to overcome the limitations associated with the multiport system in this technique.9 The patient was placed in a supine position, eliminating the need for a Trendelenburg tilt. A 3 cm suprapubic midline incision was made approximately 2 cm below the umbilicus (Figure 1A). The rectus abdominis aponeurosis was identified and incised.

FIGURE 1. Access port and robot docking. (A) Suprapubic midline single incision of 3 cm; (B) The da vinci single-port robotic system (Da Vinci SP) access port; (C) Docked robot
The extraperitoneal space was created using blunt finger dissection, establishing just enough room to insert the internal ring (wound retractor) of the SP Access Port (SPAP) (Figure 1B). Once the SPAP was secured, an 8 mm AirSeal® trocar (ConMed, Utica, NY, USA) was placed through the balloon, and the preperitoneal space was insufflated to create the working field. In select cases (used only twice in our series), the “side-car” technique was employed. This involves inserting a 10/12 mm AirSeal trocar through the same skin incision but via a separate fascial entry, passing through the wound retractor.
The SP Patient Cart was docked laterally to the patient, with no specific side required (Figure 1C). The initial instrument configuration utilized the Camera Above setting, with monopolar scissors at the 3 o’clock position, Bipolar Maryland forceps at 9 o’clock, and Cadiere forceps at 6 o’clock. (Intuitive Surgical, Sunnyvale, CA, USA).
The Retzius space was developed to expose the anterior prostate surface, followed by defatting. The endopelvic fascia was identified but generally left unopened. The vesico-prostatic junction was incised to expose the vas deferens and seminal vesicles, which were carefully isolated. Prostate pedicles were controlled without the use of hem-o-lok clips, while the posterior plane was developed to the prostate apex. When feasible, a bilateral nerve-sparing technique was employed, using precise pinpoint coagulation.
The dorsal venous complex (DVC) was primarily controlled with subluxation, avoiding sutures unless bleeding occurred. In such cases, a 3-0 V-Loc™ barbed suture (Medtronic, Minneapolis, MN, USA) was used. Dissection continued at the prostate apex, ensuring maximal urethral length preservation—an essential factor for postoperative continence.
Prostatectomy was completed with a urethrovesical anastomosis using a two-needle barbed suture, following the Van Velthoven technique. Posterior reconstruction was not performed due to the small prostate size.
No surgical drains were placed postoperatively.
Data analysis employed descriptive statistics, with continuous variables presented as medians with corresponding first (Q1) and third (Q3) quartiles, while categorical variables were presented as frequencies and percentages.
A total of sixteen consecutive patients underwent SP-RARP. Baseline population data and tumor clinical characteristics are summarized in Table 1.
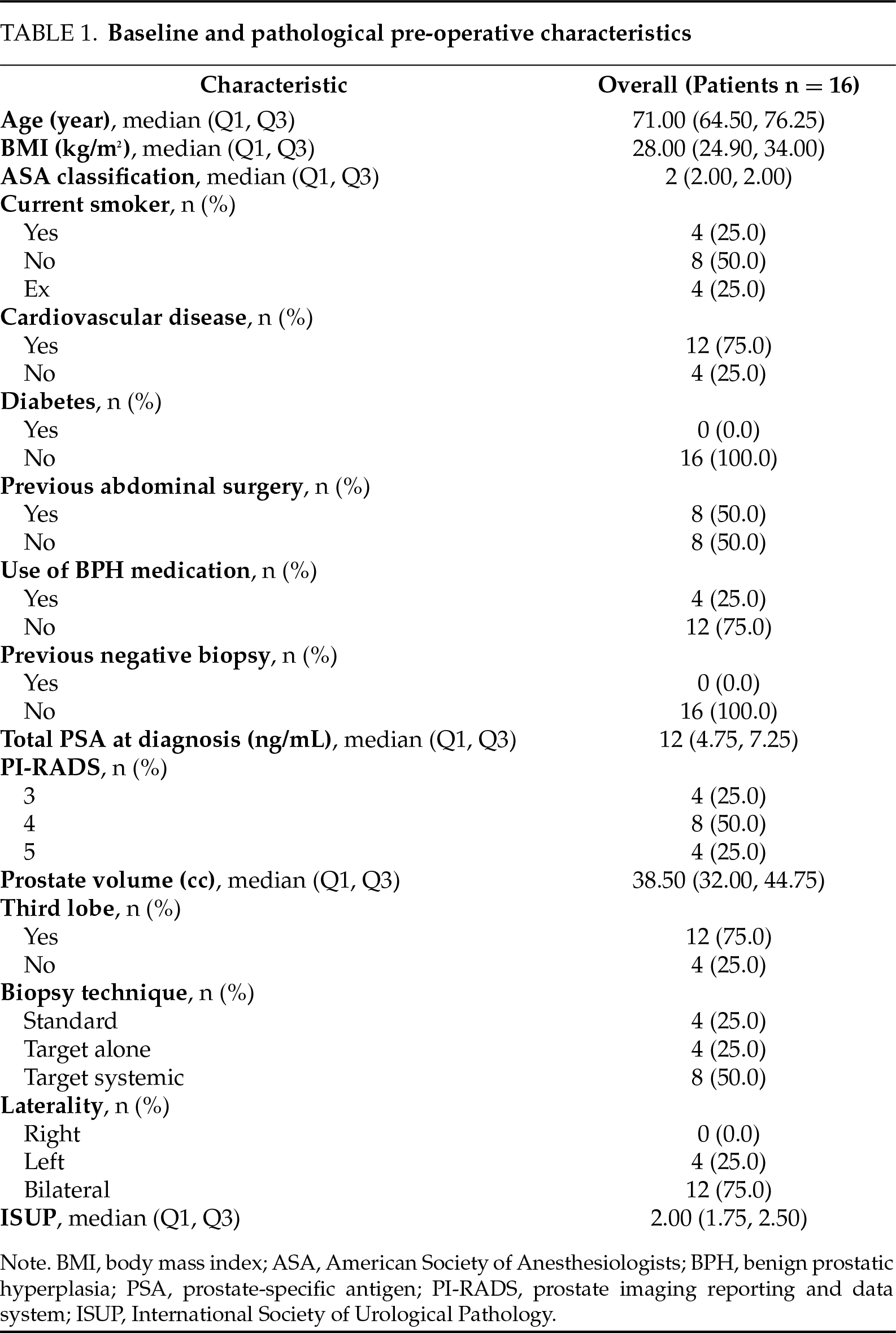
Preoperative MRI was conducted for all patients, revealing a median PI-RADS (Prostate Imaging Reporting and Data System) score of 3.5 (interquartile range [IQR] 3.00–4.25) and a median prostate volume of 38.50 cc (IQR 32.00–44.75), with 75% presenting a third lobe. Biopsy techniques varied, with 25% undergoing standard biopsy, 25% target-alone biopsy, and 50% target systemic biopsy. The median ISUP grade was 2 (IQR 1.75–2.50).
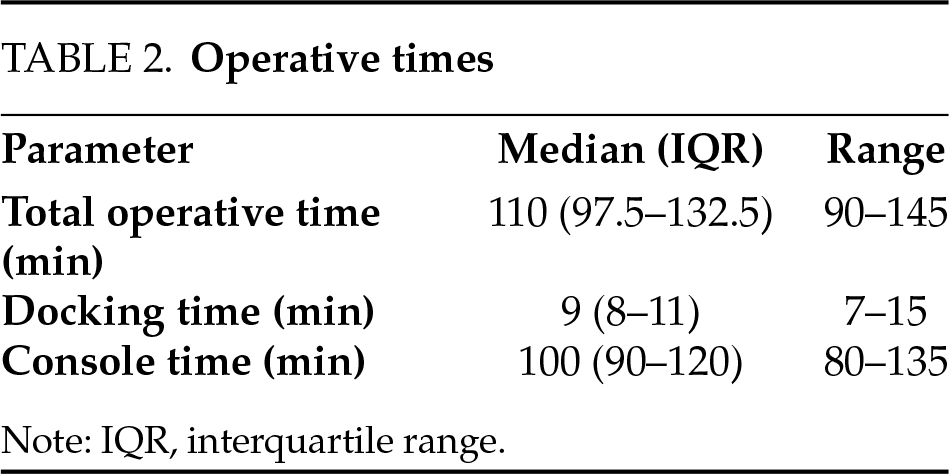
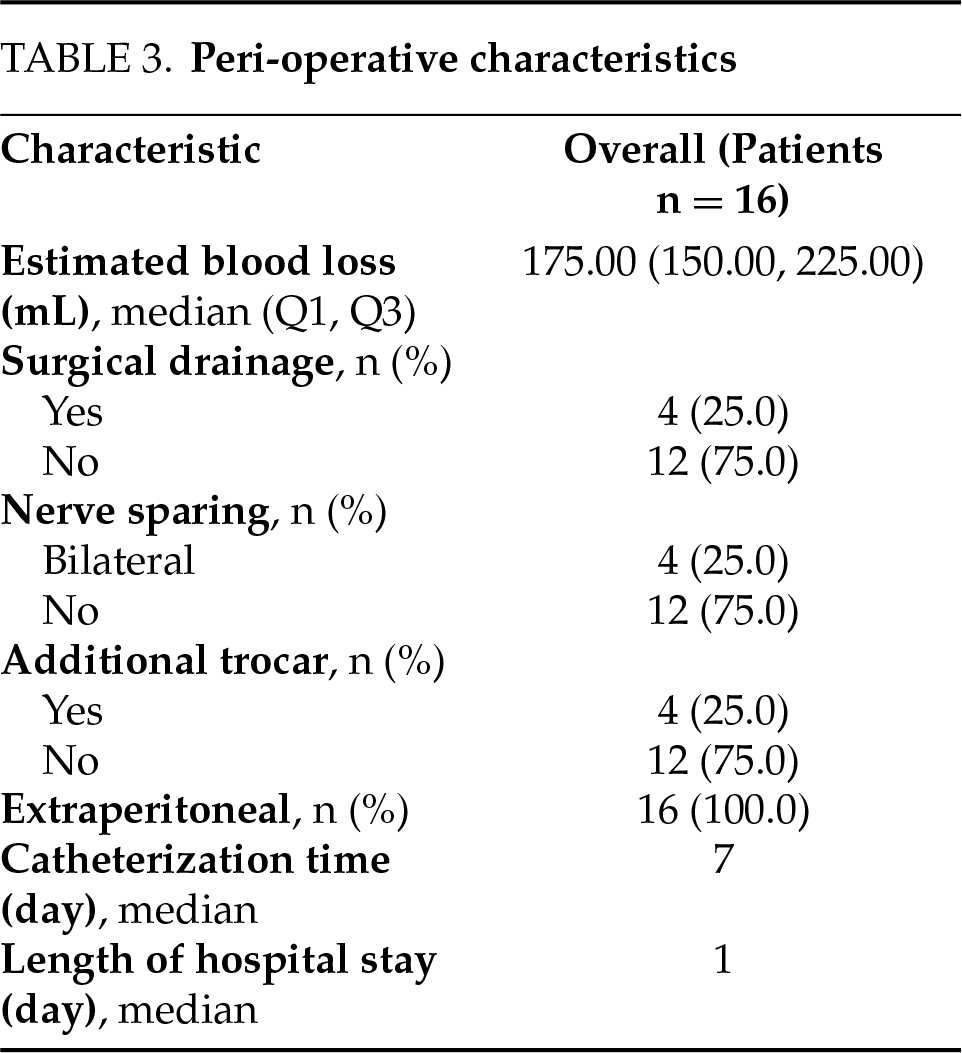
No intraoperative or perioperative complications according to the Clavien-Dindo classification were reported. Key perioperative characteristics included a median operative time of 110 min (IQR 97.5–132.5) with specific data regarding docking and console times reported in Table 2. A median estimated blood loss of 175 mL (IQR 150–225) was noted. In 75% of cases, bilateral nerve-sparing was performed after careful evaluation of tumor characteristics. All surgeries were conducted with an extraperitoneal approach, with an additional trocar used in 25% of procedures in a “sidecar” configuration. No conversion to open/laparoscopic surgery was needed or positioning of extra-port (“plus one”). No technical issues or failure of the system that compromised the completion of the surgery have been described. Mobilization of the patients occurred on the same night as the intervention, and the median length of hospital stay was one day (1–2 days). The mean pain score on the first postoperative day of 2.5 (IQR 2–3). At discharge, the mean pain score was 0 (IQR 0–1), and the median cumulative postoperative opioid use was 32 mg (IQR 14–55) total morphine equivalent. Opioid administration was limited to the immediate postoperative period, mainly to facilitate early mobilization and discharge. No patient required opioids beyond the first postoperative week. No patients required postoperative adjuvant treatment. The bladder catheter was always removed on 7th post-operative day prior to cystography. Pathological examination revealed no positive margins in all cases.
Detailed perioperative outcomes are provided in Table 3.
Launch of the Da Vinci Single Port platform on the European market represents a notable leap forward in minimally invasive urological surgeries. The first described SP-RALP was reported by Kaouk et al. using a transumbilical approach. Since then, various techniques have been described for SP-RALP, including transperitoneal, extraperitoneal, perineal, transvesical, and Retzius-sparing approaches, each offering distinct benefits.1
The advancement of technology, coupled with increased surgeon expertise, has rendered the transition to the da Vinci SP robotic system safe and effective, even during the learning curve, when compared to previous platforms.10,11 Preliminary findings from a narrative review conducted in January 2023, indicate that SP-RARP is safe and feasible, with a rapid transition from MP to SP in expert hands, and it may provide outcomes comparable to standard multiport RARP.8
In our series, all procedures were also supported by 3D reconstruction models. These tools can facilitate preoperative planning and intraoperative decision-making by improving the surgeon’s understanding of patient-specific anatomy. In particular, they may assist in tailoring the nerve-sparing approach and could help reduce the risk of positive surgical margins in selected cases. 3D reconstructions have also been explored in the literature as intraoperative aids to guide secondary resections when margin involvement is suspected, with encouraging early oncological results. Nevertheless, the available evidence remains heterogeneous, as some studies report improved outcomes and fewer complications while others show conflicting findings, underlining the need for larger controlled investigations. From a technical perspective, current intraoperative overlays of 3D models onto the surgical field are static and manually aligned, lacking dynamic tracking of anatomical structures. This limits their real-time usefulness during complex dissections. Future developments in augmented reality may help overcome these challenges by allowing real-time integration of 3D reconstructions with intraoperative anatomy, potentially enhancing surgical precision and balancing oncological radicality with functional preservation.12–14
Moreover, the SP system offers significant advantages for extraperitoneal RARP, particularly in terms of precision when operating in confined spaces. Importantly, oncological outcomes are comparable between extraperitoneal and transperitoneal SP-RARP.1,15 In our series, all SP-RARPs were performed extraperitoneally. Patients were consistently discharged on the first postoperative day, aligning with findings in the literature. In settings where robust outpatient care is available, same-day discharge could also be feasible. The absence of pneumoperitoneum and the reduced intra-abdominal pressure contribute to a lower incidence of postoperative ileus and a reduced need for narcotics. Avoiding peritoneal entry makes this technique particularly advantageous for patients with prior abdominal surgeries.
Additionally, the supine positioning without the need for Trendelenburg tilt enhances anesthetic outcomes and accelerates recovery. The single skin incision minimizes the risk of wound infections and results in superior cosmetic outcomes. In two cases, we employed the side-car technique, which involves the placement of an additional trocar through the single incision but via a separate fascial entry. Compared with the plus-one configuration, this approach is technically more demanding and offers the assistant a narrower range of motion. However, it allows the surgeon to maintain a pure single-port strategy with a single scar while still providing important intraoperative advantages, such as the possibility of using rigid or flexible suction, applying clips with an acceptable angle of movement, and assisting in tissue handling. The main benefit of this configuration is the more dynamic and versatile support it provides from the bedside assistant, while avoiding an additional access site that could negatively affect cosmesis and postoperative comfort.
Our perioperative results align with those reported in the literature, except for operative time, which appears to be shorter. This may be attributed to the limited sample size and specific patient characteristics in our cohort.16
An important limitation of our series is that only patients with relatively small prostate volumes and clinically localized disease were included, with no indication for PLND. This reflects a cautious approach for the initial European experience with the SP platform.
The feasibility of SP-RARP in more complex scenarios, such as in patients with larger prostates, high-risk disease, or when PLND is required, remains to be determined. Early reports suggest that PLND with the SP system is technically feasible,17 but it may increase operative complexity and instrument crowding. Larger series and dedicated studies are needed to assess whether SP-RARP can be safely and effectively extended to these patient populations.
Although our report was not designed to assess the learning curve, this remains a key aspect in the adoption of the SP system. Previous experiences indicate that surgeons already proficient with the multiport platform may require fewer cases to reach proficiency with SP-RARP compared to their initial robotic training. A recent study18 showed that perioperative outcomes can stabilize after a relatively limited number of procedures, suggesting a shorter learning process in expert hands. Nevertheless, the true learning curve is still debated, as it may vary depending on the approach (extraperitoneal vs. transperitoneal), institutional volume, and available training. Larger comparative studies with adequate follow-up are warranted to define how the transition from multiport to single-port affects surgical performance and patient outcomes.
Among the additional limitations of our study are its primarily descriptive design and the absence of a comparative multiport group, which may reduce the generalizability of the findings. Furthermore, although this experience can be considered innovative within the European context due to the very recent introduction of the SP platform, it should be acknowledged that the system has already been available for several years in the United States, which reduces the overall novelty of our series.
We present our initial experience with the Da Vinci SP platform, performing an Extraperitoneal Radical Prostatectomy and detailing our surgical technique. To the best of our knowledge, this is the first described European SP-RARP Series. Based on our observations, we find the platform readily accessible to a seasoned robotic surgeon, requiring minimal time to acclimate. However, further procedures are warranted to attain proficiency and comprehensively assess oncological and functional outcomes. This early case series confirms the feasibility and safety of extraperitoneal SP-RARP in a high-volume referral setting. While these data represent only a first step, ongoing studies with expanded cohorts are underway to define learning curves, optimal patient selection, and comparative outcomes with existing approaches.
Acknowledgement
We thank Alessandra Trocino, librarian at the Istituto Nazionale Tumori di Napoli, IRCCS “G. Pascale”, Italy, for her bibliographic assistance.
Funding Statement
The authors received no specific funding for this study.
Author Contributions
Gianluca Spena: Conceptualization, Methodology, Data curation, Writing—original draft. Francesco Passaro: Methodology, Data collection, Writing—review & editing. Achille Aveta: Data collection, Formal analysis. Roberto Contieri: Statistical analysis, Data validation, Writing—review & editing. Alessandro Izzo: Data collection, Resources. Giuseppe Quarto: Data collection, Visualization. Giovanni Grimaldi: Data collection, Resources. Luigi Castaldo: Data collection, Resources. Dario Franzese: Data collection, Resources. Raffaele Muscariello: Data collection, Resources. Savio Domenico Pandolfo: Supervision, Writing—review & editing. Antonio Tufano: Supervision, Critical revision. Sisto Perdonà: Conceptualization, Supervision, Project administration. All authors reviewed the results and approved the final version of the manuscript.
Availability of Data and Materials
Available at https://zenodo.org/records/17152936 (accessed on 01 January 2025).
Ethics Approval
This retrospective study was conducted using fully anonymized data collected for clinical purposes. According to institutional and national regulations, ethical committee approval was not required.
Informed Consent
All patients provided written informed consent for participation and for the use of their anonymized clinical data for research purposes.
Conflicts of Interest
The authors declare no conflicts of interest to report regarding the present study.
References
1. Kaouk J, Bertolo R, Eltemamy M et al. Single-port robot-assisted radical prostatectomy: first clinical experience using the SP surgical system. Urology 2019;124:309. doi:10.1016/j.urology.2018.10.025. [Google Scholar] [PubMed] [CrossRef]
2. Valenzi FM, Santarelli V, Haberal HB et al. Advances in robotic surgery: in favor of the single port platform. Eur Urol Focus 2025;11(1):3–4. doi:10.1016/j.euf.2025.04.002. [Google Scholar] [PubMed] [CrossRef]
3. Perdonà S, Izzo A, Tufano A et al. Advancing surgical management of penile cancer: single port bilateral inguinal lymph node dissection. Int Braz J Urol 2025;51(3):e20240663. doi:10.1590/s1677-5538.ibju.2024.0663. [Google Scholar] [PubMed] [CrossRef]
4. Izzo A, Spena G, Grimaldi G et al. Single-port robot-assisted nephroureterectomy via a supine anterior approach: step-by-step technique. BJU Int 2025;135(3):535–538. doi:10.1111/bju.16537. [Google Scholar] [PubMed] [CrossRef]
5. Ge S, Zeng Z, Li Y et al. Comparing the safety and efficacy of single-port versus multi-port robotic-assisted techniques in urological surgeries: a systematic review and meta-analysis. World J Urol 2024;42(1):18. doi:10.1007/s00345-023-04711-6. [Google Scholar] [PubMed] [CrossRef]
6. Orsini A, Lasorsa F, Bignante G et al. Outpatient robotic urological surgery: an evidence-based analysis. Eur Urol Focus 2025;11(2):337–346. doi:10.1016/j.euf.2024.10.003. [Google Scholar] [PubMed] [CrossRef]
7. Vigneswaran HT, Schwarzman LS, Francavilla S et al. A comparison of perioperative outcomes between single-port and multiport robot-assisted laparoscopic prostatectomy. Eur Urol 2020;77(6):671–674. doi:10.1016/j.eururo.2020.03.031. [Google Scholar] [PubMed] [CrossRef]
8. Franco A, Pellegrino AA, De Nunzio C et al. Single-port robot-assisted radical prostatectomy: where do we stand? Curr Oncol 2023;30(4):4301–4310. doi:10.3390/curroncol30040328. [Google Scholar] [PubMed] [CrossRef]
9. Kaouk J, Valero R, Sawczyn G et al. Extraperitoneal single-port robot-assisted radical prostatectomy: initial experience and description of technique. BJU Int 2020;125(1):182–189. doi:10.1111/bju.14885. [Google Scholar] [PubMed] [CrossRef]
10. Francavilla S, Veccia A, Dobbs RW et al. Radical prostatectomy technique in the robotic evolution: from da Vinci standard to single port—a single surgeon pathway. J Rob Surg 2022;16(1):21–27. doi:10.1007/s11701-021-01194-8. [Google Scholar] [PubMed] [CrossRef]
11. Pellegrino AA, Pellegrino F, Cannoletta D et al. Learning curve for single-port robot-assisted urological surgery: single-center experience and implications for adoption. Eur Urol Focus 2025;11(1):136–141. doi:10.1016/j.euf.2024.09.005. [Google Scholar] [PubMed] [CrossRef]
12. Checcucci E, Pecoraro A, Amparore D et al. The impact of 3D models on positive surgical margins after robot-assisted radical prostatectomy. World J Urol 2022;40(9):2221–2229. doi:10.1007/s00345-022-04038-8. [Google Scholar] [PubMed] [CrossRef]
13. Sarhan K, Khan N, Prezzi D et al. Reduction of surgical complications via 3D models during robotic assisted radical prostatectomy: review of current evidence and meta-analysis. J Robot Surg 2024;18(1):304. doi:10.1007/s11701-024-02041-2. [Google Scholar] [PubMed] [CrossRef]
14. Quarta L, Cannoletta D, Pellegrino F et al. The role of robot-assisted, imaging-guided surgery in prostate cancer patients. Cancers 2025;17(9):1401. doi:10.3390/cancers17091401. [Google Scholar] [PubMed] [CrossRef]
15. Wilson CA, Aminsharifi A, Sawczyn G et al. Outpatient extraperitoneal single-port robotic radical prostatectomy. Urology 2020;144(Suppl 1):142–146. doi:10.1016/j.urology.2020.06.029. [Google Scholar] [PubMed] [CrossRef]
16. Checcucci E, De Cillis S, Pecoraro A et al. Single-port robot-assisted radical prostatectomy: a systematic review and pooled analysis of the preliminary experiences. BJU Int 2020;126(1):55–64. doi:10.1111/bju.15069. [Google Scholar] [PubMed] [CrossRef]
17. Lambertini L, Pacini M, Calvo RS et al. Extraperitoneal single port vs transperitoneal multiport robot assisted radical prostatectomy in frail patients: a propensity score matched comparative analysis. Eur J Surg Oncol 2024;50(12):108741. doi:10.1016/j.ejso.2024.108741. [Google Scholar] [PubMed] [CrossRef]
18. Lambertini L, Pacini M, Avesani G et al. Basic skills for single-port robotic surgery. Cent European J Urol 2024;77(4):693. doi:10.5173/ceju.2024.0161. [Google Scholar] [PubMed] [CrossRef]
Cite This Article
 Copyright © 2026 The Author(s). Published by Tech Science Press.
Copyright © 2026 The Author(s). Published by Tech Science Press.This work is licensed under a Creative Commons Attribution 4.0 International License , which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
 Downloads
Downloads
 Citation Tools
Citation Tools