
 Submit a Paper
Submit a Paper Propose a Special lssue
Propose a Special lssue Open Access
Open Access
ARTICLE

Is postoperative routine thoracic imaging necessary to detect thoracic complications in patients undergoing supracostal mini percutaneous nephrolithotomy (m-PCNL) surgery?
Department of Urology, Haseki Training and Research Hospital, Istanbul, 34096, Turkey
* Corresponding Author: Huseyin Burak Yazili. Email:
Canadian Journal of Urology 2026, 33(1), 165-171. https://doi.org/10.32604/cju.2025.069657
Received 27 June 2025; Accepted 15 September 2025; Issue published 28 February 2026
 View Full Text
View Full Text Download PDF
Download PDFAbstract
Objectives: Supracostal access during percutaneous nephrolithotomy (PCNL) increases the risk of pulmonary complications. Although routine postoperative thoracic imaging is commonly performed to detect these events, its clinical necessity remains controversial. This study aimed to assess the necessity of routine postoperative thoracic imaging for detecting pulmonary complications in patients undergoing supracostal mini percutaneous nephrolithotomy (m-PCNL) surgery. Methods: A retrospective analysis was conducted on data from patients who underwent supracostal m-PCNL between 2017 and 2022 in a tertiary center. Excluding patients under 18, with kidney/skeletal anomalies, or active thoracic disease, 112 eligible patients were included. Patients were divided into two groups: those with routine postoperative chest X-ray (CXR) (Group 1, n = 40) and those without (Group 2, n = 72). Complications and operative data were compared between groups. Results: Mean ages were 44.3 ± 11.4 (Group 1) and 42.6 ± 13.1 (Group 2), with no significant difference (p = 0.102). Stone sizes were 30.8 ± 8.6 mm (Group 1) and 24.8 ± 8.4 mm (Group 2), also not significantly different (p = 0.313). High fever occurred in 10% of Group 1 and 4% of Group 2 (p = 0.246). Minimal effusion was found in 10% of Group 1, with no treatment due to lack of symptoms. However, subsequent CXR revealed hydropneumothorax in 2.5% of cases, necessitating thoracic tube insertion. In Group 2, 5% developed postoperative respiratory symptoms, with significant pneumothorax in 1.3%, requiring thoracic tube placement. Thoracic tube insertion rates did not significantly differ between groups (Group 1: 2.5% vs. Group 2: 1.3%, p = 0.671). Conclusions: Routine postoperative thoracic imaging did not show any significant benefit in detecting pulmonary complications post-supracostal m-PCNL.Keywords
Urinary system stone disease is an important health problem that has a major place in urology practice, not only because of its high prevalence but also due to the significant morbidity, economic burden, and recurrence risk it imposes on affected individuals.1 In recent years, the incidence of the disease has continued to increase worldwide, and this rise has been attributed to several interrelated factors such as changing climate characteristics, dietary habits shifting toward higher protein and salt consumption, decreased fluid intake, and the increasing prevalence of obesity and metabolic syndrome.2 These multifactorial causes emphasize the importance of both preventive strategies and effective treatment modalities in daily urological practice.
At present, a wide range of surgical and minimally invasive treatment options are available for the management of urinary system stones. Percutaneous nephrolithotomy (PCNL), flexible ureterorenoscopy (f-URS), extracorporeal shock wave lithotripsy (ESWL), open, and laparoscopic surgical approaches constitute the principal methods used in clinical practice.3 The choice of treatment in an individual patient is determined by multiple factors, including the characteristics of the stone (size, anatomical location, and chemical composition), anatomical features of the kidney and collecting system, patient-related parameters such as obesity or solitary kidney, and, in many cases, the clinical experience and preference of the surgeon.3
According to the most recent guideline of the European Association of Urology (EAU), PCNL continues to be regarded as the gold standard treatment method for kidney stones larger than 2 cm, owing to its high efficacy and durability of outcomes.4 In the literature, stone-free rates of up to 96% have been reported with PCNL, highlighting its superiority in achieving complete clearance compared to other modalities.5 Traditionally, PCNL was performed using a 30 Fr sheath at the time of its first description; however, as clinical experience grew, efforts were made to minimize perioperative morbidity and reduce complication rates by gradually introducing smaller caliber sheaths. In this regard, the evolution toward mini PCNL (m-PCNL), which employs instruments with sizes below 22 Fr, has provided urologists with a reliable option offering superior success rates and minimal complication profiles, particularly in selected patient populations.6
PCNL surgery can be performed with both supracostal and infracostal access methods, depending on the location of the stone and the individual renal anatomy.7 Each approach has its own advantages and drawbacks; however, in PCNL surgeries performed with the supracostal technique, the risk of pleural and pulmonary complications, such as hydrothorax, pneumothorax, or pleural effusion, is notably increased when compared to infracostal access. These potential complications have been a matter of clinical concern for decades.
The usefulness of routine early postoperative lung imaging, particularly chest radiography, for the detection of pulmonary or pleural complications following supracostal access is still controversial. While some clinicians advocate for routine imaging in order to avoid missing potentially serious complications, others argue that asymptomatic and clinically insignificant findings detected on chest X-ray (CXR) do not always alter management and may not justify routine use. Therefore, clarifying the role of postoperative CXR remains an important question in contemporary practice. Based on this background, the present study was designed to investigate the usefulness of routine postoperative CXR radiographs in both the diagnostic and therapeutic decision-making processes for the early detection of pleural injury or lung damage that may occur after supracostal m-PCNL surgery.
The data of patients who underwent supracostal (between the 11th and 12th ribs) m-PCNL in Haseki Training and Research Hospital Urology Clinic between 2017 and 2022 were evaluated retrospectively. Patients under the age of eighteen, with renal and skeletal system anomalies, and with active lung disease were excluded from the study. 112 patients who met the study criteria were included in the study. Written consent was obtained from all patients before the operation. Ethics committee approval was received from Haseki Training and Research Hospital ethics committee (date/No.: 23.12.2020/2020-69).
Demographic and clinical data of the patients, such as American Society of Anesthesiologists (ASA) score, body mass index (BMI), sex, and stone size, were recorded. Renal stone characteristics were evaluated preoperatively using abdominal computed tomography (CT) and/or intravenous pyelography (IVP). Quality of life was assessed using the Kidney Disease Quality of Life Short Form (KF-36) questionnaire. This validated instrument evaluates physical and mental health domains in patients with kidney disease.
All patients underwent supracostal m-PCNL by accessing between the 11th and 12th ribs. Peroperative and postoperative data such as operation time, fluoroscopy time, whether nephrostomy and Double J (DJ) catheter were applied, hospital stay, postoperative hemoglobin value, development of fever, need for transfusion, and need for a thorax tube were recorded. Operation time is defined as the time from the end of the patient’s intubation to the skin suturing.
The patients were divided into two groups: those who received routine postoperative CXR radiographs and those who did not. Routine CXR radiographs were taken at the bedside in the 4th postoperative hour for 40 patients in Group 1. CXR radiographs were taken for 72 patients in Group 2 in the presence of respiratory symptoms such as low saturation, dyspnea, and tachypnea. After discharge, the DJ catheter removal was performed in the 3rd postoperative week. Stone-free rates were checked with abdominal CT performed at the 3rd postoperative month.
In patients who underwent supracostal percutaneous access, complications and operative data were compared between patients who underwent routine CXR radiographs in the postoperative period and those who did not.
The PCNL operation was explained to the patients in detail before the operation. All operations were performed by the same team experienced in endourology. Consent was obtained from the patients for the operation. All patients underwent general anesthesia. First of all, cystoscopy was performed on the patients in the lithotomy position, then a guide wire was sent to the side where the operation would be performed, a 5 Fr ureter catheter was applied, and checked with fluoroscopy. The patients were then placed in the prone position, and a sterile drape was applied again. Contrast material was administered through the ureteral catheter, and an 18-gauge percutaneous access needle was inserted into the calyx, which was deemed appropriate, using the triangulation technique under the guidance of fluoroscopy. Meanwhile, in conjunction with the anesthesiologist, serial dilation was performed up to 16 Fr or 21 Fr while the patients were in expiration, and the patients were taken into inspiration again. After the dilatation was completed, the access sheath was placed, and the calyceal system was accessed under the guidance of a nephroscope. Stones were fragmented using a laser lithotriptor. It was cleaned with the help of a basket and forceps. At the end of the operation, the operation was terminated following the insertion of an antegrade DJ catheter and nephrostomy, if deemed necessary.
Work rates analysis was calculated with the GPower 3.1.9.7 program (Faul, Erdfelder, Buchner, & Lang, 2009). SPSS version 25 (IBM Corp., Armonk, NY, USA) was used for the statistical analyses. Normality assessment of the data status was examined with the Kolmogorov-Smirnov test. An independent person’s t-test was used to compare variables with normal distribution, and the Mann-Whitney U test was chosen for existing data with varying normality. Our quantitative data are shown as mean ± standard deviation (SD). Those who apply the Chi-square test to meet qualitative leakage. For the comparison of KF-36 scores before and after the procedure, paired-sample t-tests were used in the study groups. Data were examined at a 95% confidence level (CI), and p-values of <0.05 were considered significant.
The patients’ sex, mean age, BMI, and ASA score were similar between the two groups (p = 0.951, p = 0.102, p = 0.628, and p = 0.973, respectively). The mean stone size was 30.8 ± 8.6 mm in Group 1 and 24.8 ± 8.4 mm in Group 2 (p = 0.313). The demographic and clinical data of the patients are given in Table 1 in detail.
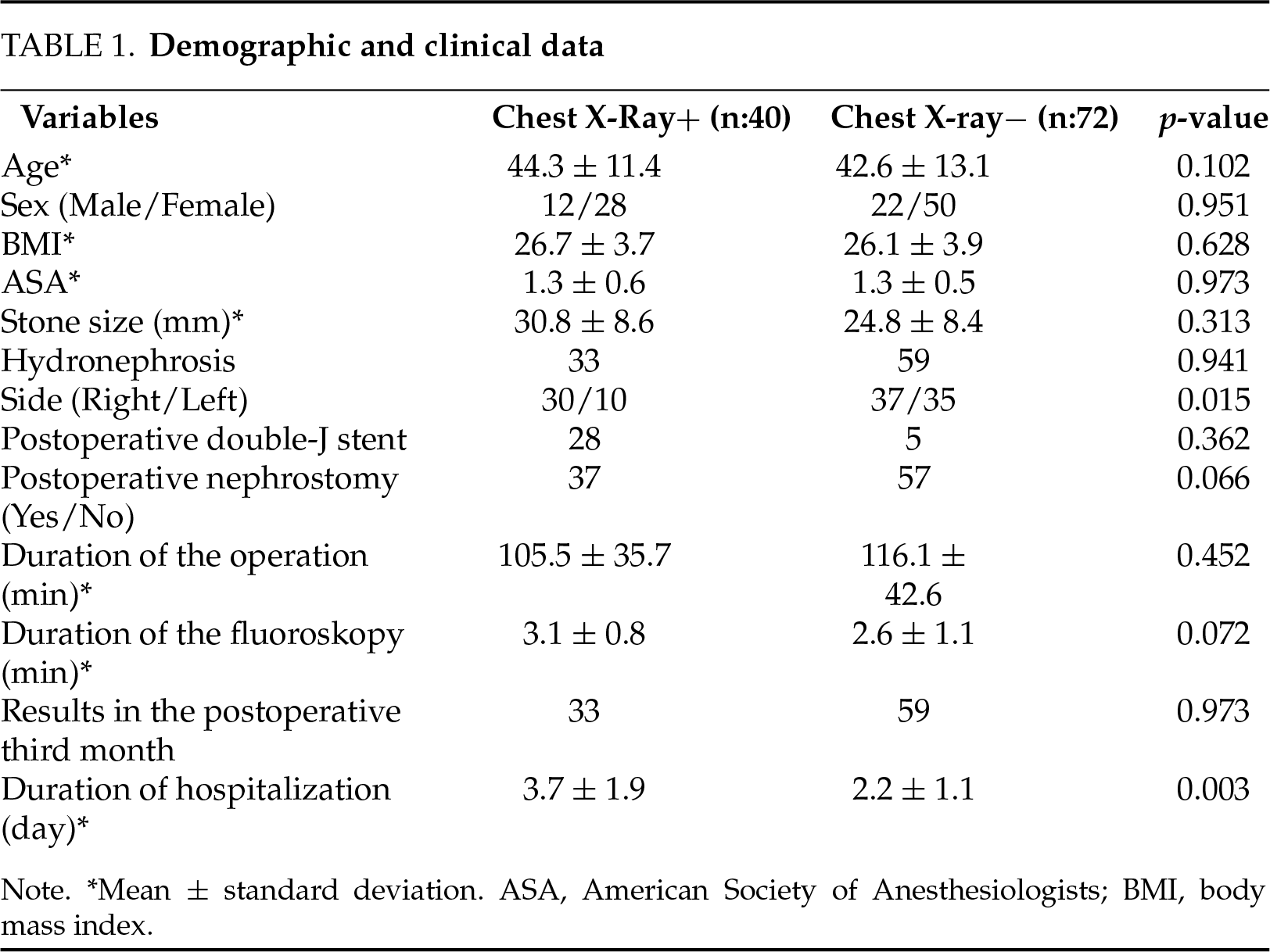
The duration of surgery was 105.5 ± 35.7 min in Group 1 and 116.1 ± 42.6 min in Group 2, and there was no significant difference between the groups (p = 0.452). The duration of fluoroscopy was 3.1 ± 0.8 min in Group 1 and 2.6 ± 1.1 min in Group 2, and there was no significant difference between the two groups (p = 0.072). Postoperative nephrostomy was applied to 37 (92%) patients in the first group and 57 (79%) patients in the second group, and they were statistically similar (p = 0.066). There was no statistically significant difference between the two groups in terms of stone-free rates at the postoperative 3rd month (p = 0.973). The duration of hospitalization of the patients in Group 1 was statistically significantly longer than Group 2 (3.7 ± 1.9 days vs. 2.2 ± 1.1 days, respectively, p = 0.003).
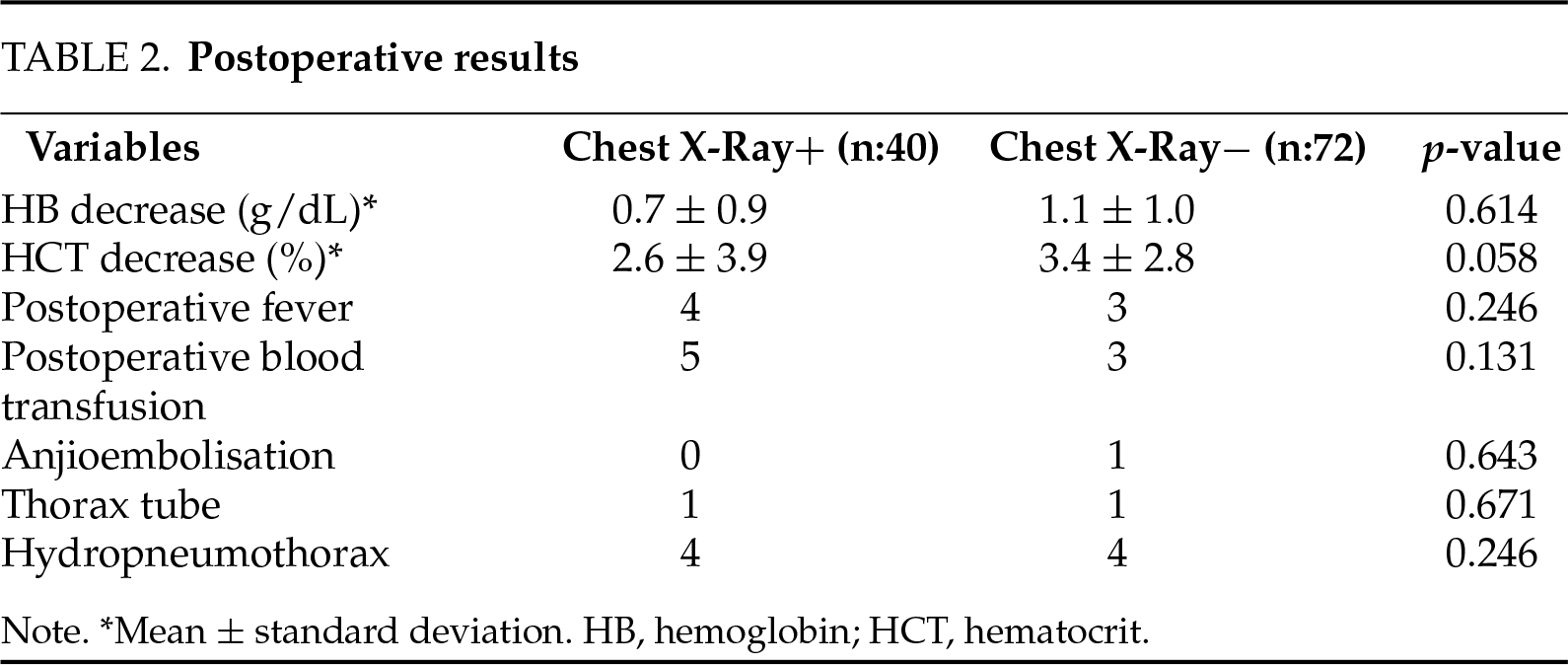
When complications were evaluated, postoperative fever developed in 4 (10%) patients in Group 1 and in 3 (4%) patients in Group 2 (p = 0.246). Postoperative transfusion was applied to 5 (12%) patients in Group 1 and 3 (4%) patients in Group 2, and angioembolization was applied to 1 (1.3%) patient in Group 2 (p = 0.131 vs. p = 0.643), respectively. Postoperative hemoglobin decrease was 0.7 ± 0.9 g/dl in Group 1 and 1.1 ± 1.0 g/dl in Group 2, and there was no significant difference between the groups (p = 0.614).
Minimal effusion was detected in the routine postoperative CXR of 4 (10%) patients in Group 1, but no additional intervention or treatment was planned due to the absence of symptoms. In the follow-up of these patients in whom effusion was detected, hydropneumothorax was detected in 1 (2.5%) patient in the postoperative 36th hour due to the development of symptoms. The thorax tube was removed two days later, and the patient was discharged on the 5th postoperative day. Other asymptomatic patients were followed up to postoperative 3 and 4 days.
Due to the development of postoperative respiratory symptoms in Group 2, CXR was performed in 4 (5%) patients. Hydropneumothorax was detected in the CXR of 1 (1.3%) patient in Group 2, who developed symptoms at the postoperative 16th hour, and the patient was treated with a thorax tube. The patient was discharged on the 4th postoperative day, with significant resolution of hydropneumothorax in the follow-up CXR. There was no significant difference between the two groups in terms of treatment with a thorax tube (Group 1: 2.5% vs. Group 2: 1.3%, p = 0.671). Postoperative data of the patients are given in Table 2.
The success of PCNL surgery is highly dependent on providing direct and optimal access to the collecting system. With the intercostal approach, direct access to upper-pole and ureteral stones, as well as complicated stones such as staghorn stones, can be achieved, and stone intervention is greatly facilitated. The upper part of the kidney is located behind the 11th and 12th ribs and is adjacent to the parietal pleura in this region. The pleura is located laterally in the upper part of the ribs. The visceral pleura remains at the level of the 12th rib in deep inspiration and descends to the level of the 8th rib in expiration.8 This anatomical situation increases the risk of pleural and lung injury in supracostal PCNL compared to the subcostal approach. To reduce this risk, it is recommended that the access be made during expiration and from the lateral midscapular line. Maintaining low-pressure irrigation during surgery can help reduce fluid leakage from the access sheath and minimize the risk of pleural effusion. Access just below the ribs should be avoided to protect the intercostal vessels and reduce hemorrhagic complications.9 In addition, adequate drainage of the kidney and buffering of the tract with a nephrostomy tube after surgery also reduces the risk of pleural effusion.
Standard posteroanterior and lateral chest radiography remains the most important technique for the initial diagnosis of pleural effusion.10 A blunt costophrenic angle can be seen when 200 mL of fluid accumulates on the posteroanterior radiograph and approximately 50 mL on the lateral radiograph.10 Ogan et al. reported the sensitivity and specificity of CXR as 18.9% and 98.4%, respectively, in the diagnosis of hydropneumothorax after PNL. However, they reported that most of the intrathoracic fluid collections that could not be detected were clinically meaningless and did not require intervention.11 In addition, as in our study, the probability of detecting effusion in the CXR radiograph taken in the postoperative supine position is further reduced. Therefore, in the early postoperative period, CXR is insufficient to predict intrathoracic pathology that will require intervention.
Intrathoracic complications after percutaneous nephrolithotomy can be seen as hydrothorax, hemothorax, hydropneumothorax, or pelvic effusion. Studies have reported higher hydropneumothorax rates with the supracostal approach (0%–12%) compared to the subcostal approach (0.5%–2.6%). In our study, intrathoracic complications were found in 8 (7%) patients, consistent with the literature. However, since these complications were clinically insignificant or asymptomatic in most of the patients, they were followed conservatively, and only two (1.7%) of the patients had to be treated with a thoracic tube. In support of these findings, Picus et al. reported that although 20% of their patients had signs on postoperative CXR, only 8% of patients required intervention.12 Similarly, Semins et al. evaluated all patients with CT after PNL in their study of 197 patients and found pleural effusion in 17, pneumothorax in 3, hemothorax in 2, and hydrothorax in 1 patient. Only one of these patients was treated with a thoracic tube.13 In light of these findings, although more intrathoracic complications are detected in postoperative imaging compared to the subcostal approach in PCNL cases with supracostal access, most of them are treated conservatively because they are clinically insignificant. Therefore, in appropriate cases, supracostal PCNL can be safely applied in experienced centers with the appropriate surgical technique.
Even if there is no significant finding on CXR taken in the early postoperative period, intrathoracic fluid may accumulate within days or hours later, which may become clinically significant and cause symptoms in patients.14 In our study, minimal effusion was detected in four (10%) patients with routine postoperative CXR. However, in one (2.5%) patient, respiratory symptoms developed at the postoperative 36th hour, and CXR was repeated, and it was decided to treat with a thoracic tube when the effusion was found to increase. In the group in which routine postoperative radiographs were not taken, one (1.3%) patient was treated with a thorax tube when a significant hydropneumothorax was detected in the CXR performed after symptom development at the postoperative 16th hour. In the study of Bjurlin et al., postoperative hydropneumothorax developed in 4.3% (n = 2) of 46 supracostal PCNL cases. The first of these patients was detected during postoperative fluoroscopy, and hydropneumothorax was detected on the 3rd postoperative day in the other patient, although postoperative CXR was normal.15 Similarly, Ogan et al. reported that 2% (n = 2) of the patients were diagnosed with hydropneumothorax by intraoperative fluoroscopy and 5% (n = 5) of the patients were diagnosed by CXR after respiratory symptoms developed.11 The authors concluded that routine postoperative radiographs do not affect clinical management. In addition, clinically insignificant pleural effusion observed in patients with routine CXRs and radiographs may be effective in the clinician’s decision to discharge the patient. In our study, the longer hospital stay in the group with routine CXR supports this situation (3.7 ± 1.9 vs. 2.2 ± 1.1, p = 0.003). In addition, reactive effusion can be detected without pleural injury, especially with more sensitive techniques such as CT, and may mislead clinicians. In light of these findings, we believe that it is more appropriate to perform diagnostic procedures and plan treatment by evaluating possible complications in patients who develop symptoms instead of the postoperative routine CXR.
The limitations of our study include its retrospective nature and the relatively small number of patients. Additionally, it can be noted that in our clinical practice, we frequently insert nephrostomy tubes in percutaneous nephrolithotomy surgeries, although it should be considered that this practice is decreasing in frequency in current medical practice.
In our study, no additional benefit of routine postoperative CXR was found in the early diagnosis of possible pulmonary complications in patients who underwent m-PCNL with supracostal access. It seems more appropriate to plan diagnostic tests and treatments by evaluating possible complications in patients who develop respiratory symptoms instead of routine postoperative CXR.
Acknowledgement
The authors would like to thank all colleagues and staff members who contributed to this study.
Funding Statement
The authors received no financial support for the research, authorship, and publication of this article.
Author Contributions
Study conception and design were performed by Huseyin Burak Yazili, Faruk Ozgor and Ufuk Caglar. Material preparation and data collection were performed by Abdullah Esmeray, Mucahit Gelmis, Nazim Furkan Gunay, Caglar Dizdaroglu and Yasar Pazir. Data analysis and interpretation were performed by Huseyin Burak Yazili and Faruk Ozgor. The first draft of the manuscript was written by Huseyin Burak Yazili and Abdullah Esmeray, and the manuscript was critically revised by Faruk Ozgor and Ufuk Caglar. All authors reviewed the results and approved the final version of the manuscript.
Availability of Data and Materials
The datasets generated or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval
This study was conducted in accordance with the Declaration of Helsinki. Ethical approval was obtained from the Haseki Training and Research Hospital ethics committee (date/No.: 23.12.2020/2020-69).
Informed Consent
Written informed consent was obtained from all participants prior to enrollment.
Conflicts of Interest
The authors declare no conflicts of interest to report regarding the present study.
References
1. Allam EA. Urolithiasis unveiled: pathophysiology, stone dynamics, types, and inhibitory mechanisms: a review. Afr J Urol 2024;30(1):34. doi:10.1186/s12301-024-00436-z. [Google Scholar] [CrossRef]
2. Raheem OA, Khandwala YS, Sur RL, Ghani KR, Denstedt JD. Burden of urolithiasis: trends in prevalence, treatments, and costs. Euro Urol Focus 2017;3(1):18–26. doi:10.1016/j.euf.2016.10.001. [Google Scholar] [CrossRef]
3. Marcovich R, Smith AD. Renal pelvic stones: choosing shock wave lithotripsy or percutaneous nephrolithotomy. Int Braz J Urol 2003;29(3):195–207. doi:10.1590/S1677-55382003000300002. [Google Scholar] [PubMed] [CrossRef]
4. Zheng C, Xiong B, Wang H et al. Retrograde intrarenal surgery versus percutaneous nephrolithotomy for treatment of renal stones >2 cm: a meta-analysis. Urol Int 2014;93(4):417–424. doi:10.1159/000357630. [Google Scholar] [CrossRef]
5. Mishra S, Sharma R, Garg C, Kurien A, Sabnis R, Desai M. Prospective comparative study of miniperc and standard PNL for treatment of 1 to 2 cm size renal stone. BJU Int 2011;108(6):896–900. doi:10.1111/j.1464-410X.2010.09975.x. [Google Scholar] [CrossRef]
6. Ruhayel Y, Tepeler A, Dabestani S et al. Tract sizes in miniaturized percutaneous nephrolithotomy: a systematic review from the European association of urology urolithiasis guidelines panel. Euro Urol 2017;72(2):220–235. doi:10.1016/j.eururo.2017.01.046. [Google Scholar] [PubMed] [CrossRef]
7. He Z, Tang F, Lu Z et al. Comparison of supracostal and infracostal access for percutaneous nephrolithotomy: a systematic review and meta-analysis. Urol J 2019;16(2):107–114. doi:10.22037/uj.v0i0.4727. [Google Scholar] [PubMed] [CrossRef]
8. Gupta R, Kumar A, Kapoor R, Srivastava A, Mandhani A. Prospective evaluation of safety and efficacy of the supracostal approach for percutaneous nephrolithotomy. BJU Int 2002;90(9):809–813. doi:10.1046/j.1464-410x.2002.03051.x. [Google Scholar] [PubMed] [CrossRef]
9. McAllister M, Lim K, Torrey R, Chenoweth J, Barker B, Baldwin DD. Intercostal vessels and nerves are at risk for injury during supracostal percutaneous nephrostolithotomy. J Urol 2010;184(2):449–454. doi:10.1016/j.juro.2010.09.007. [Google Scholar] [PubMed] [CrossRef]
10. Karkhanis VS, Joshi JM. Pleural effusion: diagnosis, treatment, and management. Open Access Emerg Med 2012;4:31–52. doi:10.2147/OAEM.S29942. [Google Scholar] [PubMed] [CrossRef]
11. Ogan K, Corwin TS, Smith T et al. Sensitivity of chest fluoroscopy compared with chest CT and chest radiography for diagnosing hydropneumothorax in association with percutaneous nephrostolithotomy. Urology 2003;62(1):30–33. doi:10.1016/s0090-4295(03)00171-7. [Google Scholar] [CrossRef]
12. Picus D, Weyman PJ, Clayman RV et al. Intercostal space nephrostomy for percutaneous stone removal. AJR Am J Roentgenol 1986;147(2):393–397. doi:10.2214/ajr.147.2.393. [Google Scholar] [PubMed] [CrossRef]
13. Semins MJ, Bartik L, Chew BH, Hyams ES, Shah O, Matlaga BR. Multicenter analysis of postoperative CT findings after percutaneous nephrolithotomy: defining complication rates. Urology 2011;78(2):291–294. doi:10.1016/j.urology.2011.02.050. [Google Scholar] [CrossRef]
14. Ufuk UF, Ocak İ., Chelala L, Landeras L. Postoperative pulmonary complications: clinical and imaging insights. Balkan Med J 2025;42(5):405–418. doi:10.4274/balkanmedj.galenos.2025.2025-7.135. [Google Scholar] [PubMed] [CrossRef]
15. Bjurlin MA, O’Grady T, Kim R, Jordan MD, Goble SM, Hollowell CMP. Is routine postoperative chest radiography needed after percutaneous nephrolithotomy? Urology 2011;78(2):291–294. doi:10.1016/j.urology.2011.08.053. [Google Scholar] [PubMed] [CrossRef]
Cite This Article
 Copyright © 2026 The Author(s). Published by Tech Science Press.
Copyright © 2026 The Author(s). Published by Tech Science Press.This work is licensed under a Creative Commons Attribution 4.0 International License , which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
 Downloads
Downloads
 Citation Tools
Citation Tools