
 Submit a Paper
Submit a Paper Propose a Special lssue
Propose a Special lssue Open Access
Open Access
ARTICLE

Acute Effects of Virtual Reality Exercise on Young Adults’ Blood Pressure and Feelings
1
School of Kinesiology, University of Minnesota-Twin Cities, Minneapolis, MN 55455, USA
2
Faculty of Teacher Training and Education, University of Oviedo, Asturias, 33001, Spain
3
School of Public Health, University of Minnesota-Twin Cities, Minneapolis, MN 55455, USA
4
Department of Physical Education, Shanghai Jiao Tong University, Shanghai, 200240, China
* Corresponding Author: Zan Gao. Email:
International Journal of Mental Health Promotion 2023, 25(5), 711-719. https://doi.org/10.32604/ijmhp.2023.027530
Received 03 November 2022; Accepted 18 November 2022; Issue published 28 April 2023
 View Full Text
View Full Text Download PDF
Download PDFAbstract
Virtual reality (VR) seems to have the potential to provide opportunities to promote physical activity (PA) in a fun way. This paper aimed to examine the acute effects of three different virtual reality-based exercise bikes on young adults’ blood pressure (BP) and feelings compared to a traditional exercise cycling session. Four exercise sessions (immersive VR cycling, two non-immersive VR cycling, and traditional cycling) were completed by 36 young adults (22 females; Mage = 23.6 years). BP was measured immediately before and after each session using a BP cuff and exercise-induced feelings were assessed via an established survey immediately after each session. Participants’ previous experience with VR was used as the covariate in the ANCOVA with repeated measures. Significant main effects were observed across cycling sessions for systolic blood pressure [F (2, 29) = 3.04, p = 0.02, η2= 0.38)] and feelings [F (3, 32) = 7.74, p < 0.01, η2 = .42]. In particular, immersive VR and traditional cycling significantly increased systolic blood pressure compared to the two non-immersive VR sessions. Moreover, immersive VR significantly increased feelings compared to the two non-immersive VR sessions, whereas these two nonimmersive VR exercises had significantly greater increased feelings compared to traditional cycling, respectively. Findings suggest immersive VR-based exercise cycling may lead to higher exercise intensities compared to nonimmersive VR cycling. Further, immersive VR cycling yielded higher feelings compared to non-immersive VR and traditional cycling. Thus, immersive VR-based exercise can be a fun and physically active health promotion tool among young adults.Keywords
Physical inactivity rates among young adults (20–35 years) have increased during the last several decades [1]. Consequently, the prevalence of obesity among U.S. young adults has reached 33.3 million [2]. While in college, 22% and 43% of students report not meeting the Physical Activity (PA) Guidelines for U.S. adults [3]. Thus, college students who meet the recommendations for moderate-intensity exercise, vigorous-intensity exercise, or a combination of both are below 46% [3]. This could be explained by the fact that college students make nutritional and PA decisions autonomously for the first time during this stage [4]. As a result, 38% of U.S. college students have a body mass index (BMI) in the overweight or obese range [3].
Insufficient physical activity is currently the 4th leading risk factor for mortality [5]. In addition, it is well known that PA in adults leads to reduced all-cause mortality rates, coronary heart disease, stroke, cancer, or high blood pressure (BP) [6–9]. BP is a measure of the pressure of blood pushing against the walls of the arteries when the heart beats (systolic BP) and when the heart rests between beats (diastolic BP) [10]. Maintaining cardiovascular health will help prevent cardiovascular disease, the leading cause of morbidity and mortality worldwide [11]. In this line, only 3.4% of college students report having been diagnosed or treated by a health professional for high BP within the last year [3]. However, 116 million of adults living in the U.S. have hypertension (47% of the population). Therefore, college is an ideal setting to focus on prevention efforts to avoid individuals from becoming ill.
Recent research has found technology to be a possible cause [12] and solution [13] to high BP. Over 90% of the U.S. population owns or has access to the Internet and a cellphone or smartphone [14]. In addition, 65% of adults play video games regularly [15]. Thus, recent health promotion programs have emphasized the use of gaming technology to increase motivation to engage in more PA at the population level [16–21]. Among these novel programs, virtual reality (VR) has gained momentum primarily as a resource to promote cognitive learning and psychological well-being [22,23]. However, the effectiveness of VR exercise on an individual’s physiological outcomes is starting to be analyzed, showing that it can be beneficial to improve physical fitness, muscle strength, balance, and extremity function [24–26].
VR has primarily been used as a training tool in medicine (e.g., surgery) and rehabilitation [27,28]. However, its utility for promoting healthy habits, such as PA engagement has been investigated [29–31]. College students in a VR-based PA program experienced higher situational motivation and enjoyment than those in a traditional cycling or treadmill program, although no positive effects were found for moderate-to-vigorous PA [25,26]. To our knowledge, only one study has tested the effects of VR exercise on young adults’ BP responses [25]. This exploratory study compared college students’ BP during VR, exergaming, and traditional cycling exercises. No significant differences were observed for BP between VR and stationary cycling. Both programs showed significantly greater systolic BP changes in comparison with exergaming cycling.
Based on the previous literature, this study’s purpose was to examine the effects of three types of VR exercises (one immersive VR and two non-immersive VR exercises) on young adults’ BP and emotions (i.e., feelings) as compared to a traditional exercise cycling session. The following hypotheses were proposed: (1) college students’ systolic BP changes would not differ significantly from traditional cycling and VR exercises; (2) immersive VR exercise would lead to significant improvements compared to the two non-immersive VR exercises; (3) immersive VR would exert significantly higher positive feelings than the two non-immersive VR modalities; (4) the two non-immersive VR exercises would have significantly more improved positive feelings compared to traditional cycling.
2.1 Participants and Study Design
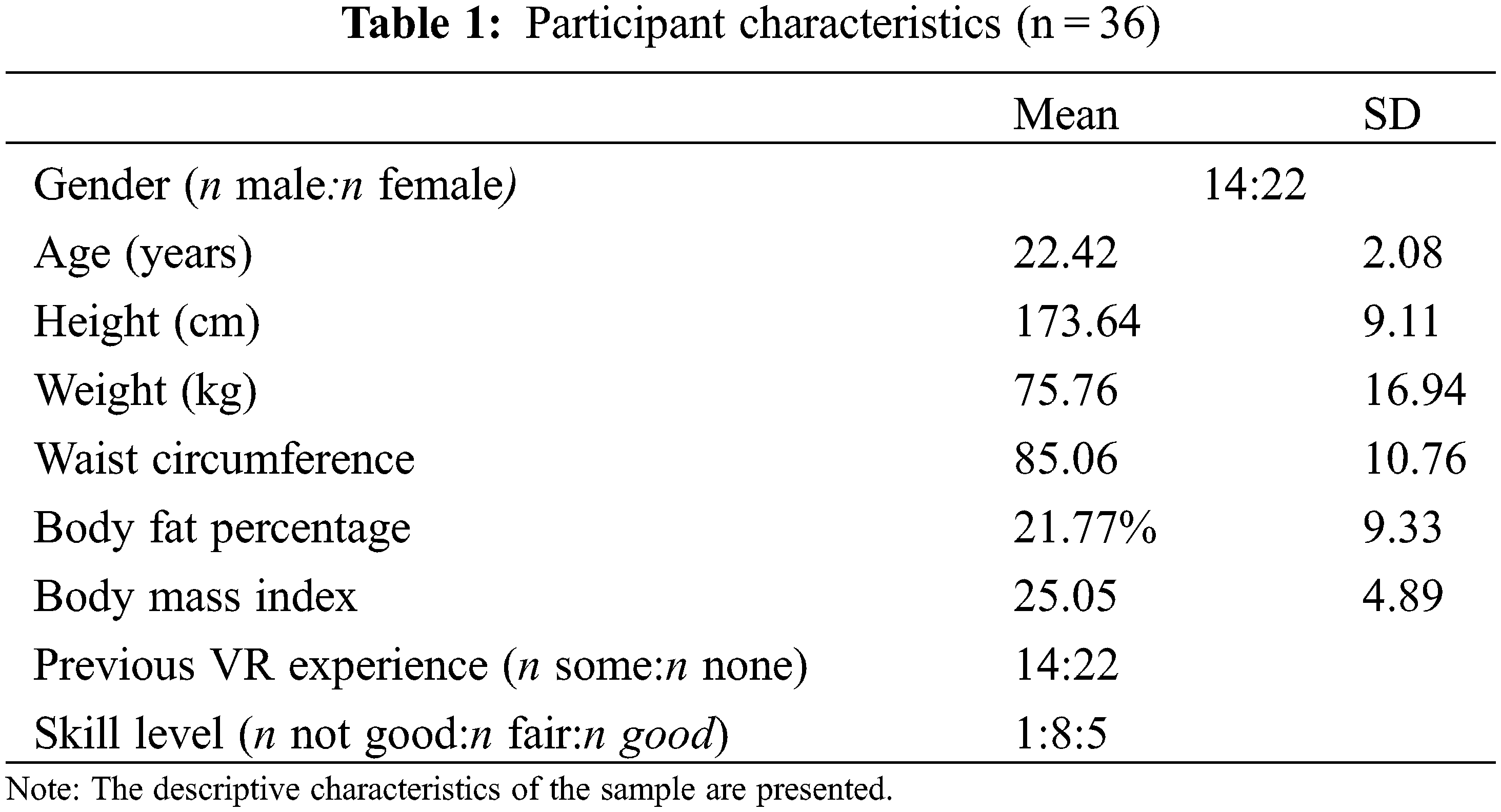
Data were collected in the Fall of 2019 and Spring of 2020. Participants were recruited via flyers posted around the University and word of mouth. The sample consisted of 36 young adults (14 female; Mean age = 22.4 ± 2.1 years) who met the following inclusion criteria: (1) 18 to 35 years old; (2) no self-reported diseases/conditions preventing PA participation; and (3) provision of informed consent. Prior to data collection, University of Minnesota Institutional Review Board approval (STUDY00006005) and informed consent were obtained. In addition, all procedures performed on participants followed the ethical standards of this institution and the Declaration of Helsinki and its subsequent amendments or comparable ethical standards [32]. Participants obtained a $20 ClinCard® (Greenphire Inc., Philadelphia, PA, USA) upon successful completion of the study.
Prior to the start of the exercise sessions, data were collected regarding participants’ height, weight, body fat percentage, waist, previous experience with VR (yes/no), skill level on VR games, and demographic information. Participants then completed four separate 12-minute exercise sessions in a counterbalanced order during a single laboratory visit: (1) immersive VR biking on VirZoom VR bike using PlayStation 4; (2) non-immersive VR biking on Gamercize bike using Xbox 360; (3) non-immersive VR biking on Game Rider EZ Gaming Bike; and (4) traditional biking on Spirit Fitness XBU55 (see Figs. 1, 2). Between each session, 10-minute breaks allowed participants’ BP and heart rate to return to baseline levels [33,34], as well as to complete the questionnaire regarding their feelings.

Figure 1: Young adults working on exercise bikes (from left to right: Gamercize, VR VirZoom, Spirit, Game Rider)

Figure 2: Young adults working on exercise bikes (from right to left: Game Rider, Spirit, VR VirZoom, Gamercize)
Immersive VR Cycling Session. Participants in this study used the VirZoom VR exercise bike as their immersive VR cycling session. Through connection to the PlayStation 4 VR system and a VR headset, players experienced a fully-immersive environment. Following the previous literature [35], two games that were indicated as the most intense were chosen for this study. Participants played one cycling racing game called “Le Tour” and a virtual racecar game called “Race Car”. By pedaling and leaning their bodies left and right, the individuals controlled their VR character.
Non-Immersive VR Cycling Sessions. Two non-immersive VR cycling sessions were completed during this study. First, the Gamercize exercise bike connected to an Xbox 360 was used to play a game called “Motocross”. Participants used an Xbox 360 controller while pedaling to steer the motocross bike around a circuit. To ensure the intensity of the activity, if pedaling was not maintained above 60 rotations per minute the game automatically stopped.
The second non-immersive session was conducted on the Game Rider EZ Gaming Bike. This exercise bike is equipped with a swiveling handlebar that allows the players to steer the vehicle on different tracks while pedaling. Participants played the game “Motor Storm” in which they guided their character on a motorcycle trek.
Traditional Cycling Session. The Spirit Fitness XBU55 upright stationary bike was used for the traditional cycling session. During the immersive VR and non-immersive VR cycling sessions, the age-predicted heart rate was used to be between 65% and 85%. Therefore, it was decided to control the intensity of the traditional cycling session to ensure that the trainings in this study were comparable. For this purpose, the heart rate integrated into the bicycle was used.
2.4.1 Previous VR Experience, Demographic and Anthropometric Information
Self-reported demographic questionnaires were used to assess participants’ age, sex, and previous VR experience. Height was measured to the nearest half-centimeter by using a Seca stadiometer (Seca, Chino, CA). Weight and body fat were measured by using a Tanita BC-558 IRONMAN® Segmental Body Composition Monitor (Tokyo, Japan).
BP was measured before (BPPre) and immediately after (BPPost) each exercise session via occlusion of the brachial artery by an Omron HEM-705CP Automatic BP Cuff (Omron Health Care, Lake Forest, IL), with participants seated, legs uncrossed, and feet flat on the floor. Mean change for each session was then calculated for systolic BP (systolic BPPost-systolic BPPre) and diastolic BP (diastolic BPPost-diastolic BPPre).
A self-reported scale was used to capture four distinct feeling states: revitalization, tranquility, positive engagement, and physical exhaustion [36] This instrument uses 15 items on a 5-point Likert scale, from “do not feel” to “feel very strongly”. The 15 items included: (1) “refreshed”, (2) “calm”, (3) “fatigued” (4) “enthusiastic”, (5) “relaxed”, (6) “energetic”, (7) “happy”, (8) “tired”, (9) “revived”, (10) “peaceful”, (11) “worn out”, (12) “upbeat”, (13) “miserable”, (14) “discouraged”, (15) “crummy”. The negative items were reversely coded and then all items were calculated to capture the mean score for each participant’s feelings.
Statistical analyses were performed using IBM-SPSS 25.0 (IBM, Inc., Armonk, NY). First, descriptive statistics were calculated for each session. A multivariate analysis of variance with repeated measures was then performed (within-subjects factor: cycling session (three levels)) to evaluate differences between cycling sessions for systolic and diastolic BP and feelings. Eta-squared (g2) was used to estimate effect sizes: small (0.10), medium (0.25), and large (0.40) [37] Finally, Bonferroni post hoc analyses were performed to determine the individual differences between the three sessions. The significance level was set at 0.05.
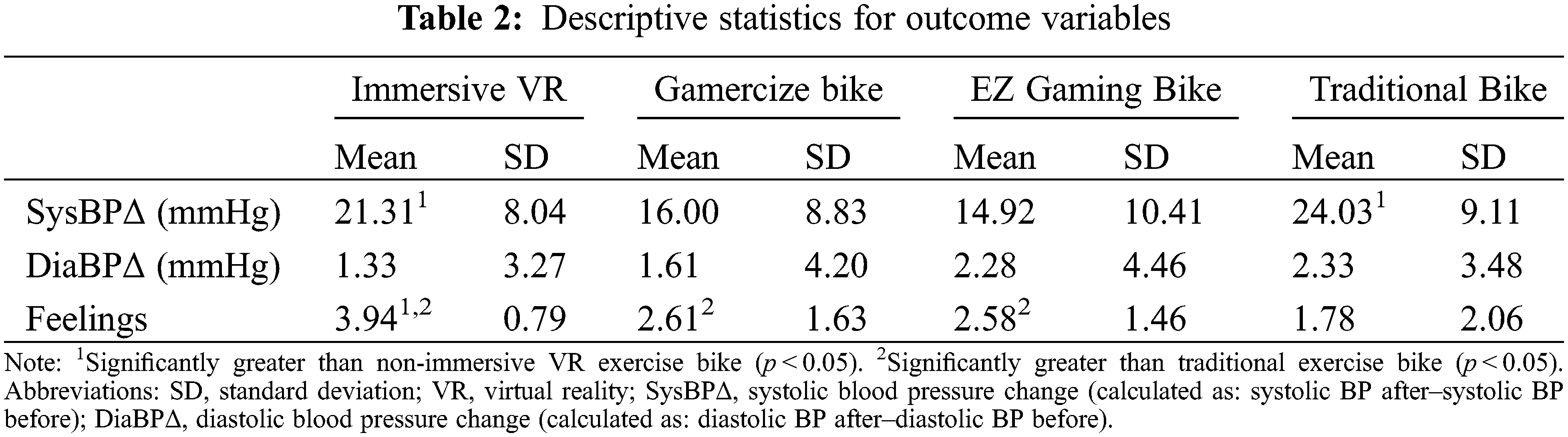
Participant characteristics are presented in Table 1. Table 2 presents descriptive characteristics of cycling sessions. Overall, significant main effects were observed between cycling sessions for pre-/post-systolic BPs [F (2, 29) = 3.04, p = 0.02, η2 = 0.38)] and feelings [F (3, 32) = 7.74, p < 0.01, η2 = 42]. Post-hoc LSD comparisons suggested that immersive VR (21.31 ± 8.04 mmHg) and traditional cycling (24.02 ± 9.11 mmHg) had significantly greater increased systolic BPs compared to two non-immersive VR exercises (16.00 ± 8.83 mmHg vs. 14.92 ± 10.41 mmHg, p < 0.05, respectively). No significant differences were found between sessions for diastolic BP change (p > 0.05). Moreover, immersive VR (3.94 ± 0.79, p < 0.01) had significantly greater increased positive feelings than the two non-immersive VR (2.61 ± 1.63; 2.58 ± 1.46), whereas these two non-immersive VR exercises had significantly greater increased positive feelings compared to traditional cycling (1.78 ± 2.06, p < 0.05), respectively.
We observed immersive VR and traditional cycling sessions to elicit higher systolic BP compared to the two non-immersive VR sessions. Moreover, findings suggested that participants experienced significantly greater positive feelings during the immersive VR than during the non-immersive VR sessions and significantly greater positive feelings during the two non-immersive VR exercises compared to traditional cycling.
Our first hypothesis for this study was that college students’ systolic BP changes would not differ significantly from traditional cycling and VR exercises. Incongruent with our hypothesis, findings indicated that traditional cycling prompted significantly greater systolic BP changes compared to non-immersive VR. In line with our hypothesis, previous research found that VR sessions did not have a significantly greater impact on systolic BP changes than traditional cycling [25]. One possible explanation for this difference is that the pedal resistance could not be matched through the sessions, since the bikes were different. The second hypothesis stated that immersive VR exercise would lead to significant improvements compared to the two non-immersive VR exercises. In line with our hypothesis, participants experienced greater systolic BP changes during immersive VR cycling when compared to non-immersive VR. On the other hand, immersive VR found no significant differences in systolic BP compared to traditional cycling. These results indicate that immersive VR could be as effective as traditional cycling in improving cardiovascular health.
The third hypothesis stated that immersive VR would exert significantly higher positive feelings than the two non-immersive VR modalities, whereas these two non-immersive VR exercises would have significantly greater increased positive feelings compared to traditional cycling. Findings were congruent with this hypothesis. Immersive VR exerted significantly greater positive feelings than all other sessions. Moreover, the fourth hypothesis was that the two non-immersive VR exercises would have significantly more improved positive feelings compared to traditional cycling. Participants experienced significantly greater positive feelings during the non-immersive VR session than during the traditional cycling session. Positive emotion (i.e., feelings) during PA is well-established to lead to long-term PA adherence [38] Thus, the findings of this study suggest that immersive VR could be an effective tool to promote PA engagement among young adults in comparison with non-immersive VR and traditional cycling.
Overall, this study has several strengths. This is, to our knowledge, the first study to analyze the effects of immersive VR on blood pressure and feelings. The design allows for comparing the efficacy of this technology with non-immersive VR and traditional cycling. The results indicate that immersive VR experiences can have a significantly positive effect compared to non-immersive VR and traditional cycling sessions. Specifically, the immersive VR-based session elicited significantly greater changes in systolic BP compared to non-immersive VR. No differences in BP were found between immersive VR and traditional cycling, indicating that the use of this technology does not impair exercise quality. However, feelings during the immersive VR session were significantly higher than during the VR and traditional cycling sessions. Therefore, the results of the present study provided empirical evidence supporting the efficacy of immersive VR in promoting quality PA as well as incentivizing positive experiences that promote future participation. Nevertheless, this study is not without limitations. First, the study design does not allow for inferring the efficacy or effectiveness of the VR bike exercise over time. Second, although the sample consisted of healthy individuals, it was limited to young adults (university students), and thus the findings may not be generalized to other populations. Socioeconomic status influences the physical fitness of young adults and, therefore, may have had an impact on the study outcomes [39,40]. In addition, the previous PA levels of the participants, which could also have influenced the results, were not accounted for. Third, pedal resistance was not able to be equated across sessions, as the bicycles were different. Because we emphasized external validity, some internal validity was compromised in the process. Thus, although this makes our results more generalizable to real-world application, not being able to have comparable resistance of the pedals across modalities needs to be addressed as a limitation. Lastly, although it reflects the reality of off-the-counter games in the real world, the systems being studied have many confounding variables including differences in the games being played and degrees of control that could have influenced the results. Therefore, future studies may implement a longitudinal design in a larger sample of young adults (not only college students), with different socioeconomic backgrounds, taking into account previous PA levels and using more homogeneous systems in order to reduce the confounding variables
The findings of this study suggest that immersive VR-based exercise bikes could lead to higher exercise intensity and positive feelings among healthy young adults in comparison with non-immersive VR bike exercise. It also yielded greater positive feelings than traditional cycling. Thus, immersive VR-based exercise can be a fun and physically active health promotion approach for young adults. With this information, college campuses may consider implementing immersive VR-integrated stationary cycle ergometers in their Student Recreation Centers as an exciting and effective alternative for students to engage in PA. Moreover, based on findings from the present study, college students may choose to purchase VR-based exercise devices as an alternative to sedentary-based video games, thereby reducing physical inactivity and engaging in enjoyable PA. Future experimental and longitudinal research designs assessing these outcomes are warranted.
Funding Statement: The authors received no specific funding for this study.
Conflicts of Interest: The authors declare that they have no conflicts of interest to report regarding the present study.
References
1. Owen, N., Sparling, P. B., Healy, G. N., Dunstan, D. W., Matthews, C. E. (2010). Sedentary behavior: Emerging evidence for a new health risk. Mayo Clinic Proceedings, 85(12), 1138–1141. https://doi.org/10.4065/mcp.2010.0444 [Google Scholar] [PubMed] [CrossRef]
2. CDC (2022). Adult obesity facts. In: Centers for disease control and prevention. Atlanta, GA: Division of Nutrition, Physical Activity, and Obesity, National Center for Chronic Disease Prevention and Health Promotion. https://www.cdc.gov/obesity/data/adult.html [Google Scholar]
3. American College Health Association (2019). American college health association. American college health association-national college health assessment II: Reference group executive summary spring 2019. [Google Scholar]
4. Desai, M. N., Miller, W. C., Staples, B., Bravender, T. (2008). Risk factors associated with overweight and obesity in college students. Journal of American College Health, 57(1), 109–114. https://doi.org/10.3200/JACH.57.1.109-114 [Google Scholar] [PubMed] [CrossRef]
5. WHO. Physical inactivity. https://www.who.int/data/gho/indicator-metadata-registry/imr-details/3416 [Google Scholar]
6. WHO. Global recommendations on physical activity for health. https://www.who.int/publications/i/item/9789241599979 [Google Scholar]
7. Physical Activity Guidelines Advisory Committee (2008). Physical activity guidelines advisory committee report, 2008. [Google Scholar]
8. Sheng, M., Yang, J., Bao, M., Chen, T., Cai, R. et al. (2021). The relationships between step count and all-cause mortality and cardiovascular events: A dose-response meta-analysis. Journal of Sport and Health Science, 10(6), 620–628. https://doi.org/10.1016/j.jshs.2021.09.004 [Google Scholar] [PubMed] [CrossRef]
9. Santos-Lozano, A., Barran, A. T., Fernandez-Navarro, P., Valenzuela, P. L., Castillo-García, A. et al. (2021). Association between physical activity and cardiovascular risk factors: Dose and sex matter. Journal of Sport and Health Science, 10(5), 604–606. https://doi.org/10.1016/j.jshs.2021.03.002 [Google Scholar] [PubMed] [CrossRef]
10. CDC (2021). High blood pressure symptoms, causes, and problems | cdc.gov. In: Centers for disease control and prevention, Atlanta, GA: National Center for Chronic Disease Prevention and Health Promotion, Division for Heart Disease and Stroke Prevention. https://www.cdc.gov/bloodpressure/about.htm [Google Scholar]
11. Benjamin, E. J., Virani, S. S., Callaway, C. W., Chamberlain, A. M., Chang, A. R. et al. (2018). Heart disease and stroke statistics–2018 update: A report from the American heart association. Circulation, 137(12), E67–E492. https://doi.org/10.1161/CIR.0000000000000558 [Google Scholar] [PubMed] [CrossRef]
12. Zou, Y., Xia, N., Zou, Y., Chen, Z., Wen, Y. (2019). Smartphone addiction may be associated with adolescent hypertension: A cross-sectional study among junior school students in China. BMC Pediatrics, 19(1), 310. https://doi.org/10.1186/s12887-019-1699-9 [Google Scholar] [PubMed] [CrossRef]
13. Parati, G., Torlasco, C., Omboni, S., Pellegrini, D. (2017). Smartphone applications for hypertension management: A potential game-changer that needs more control. Current Hypertension Reports, 19(6), 48. https://doi.org/10.1007/s11906-017-0743-0 [Google Scholar] [PubMed] [CrossRef]
14. Pew research center use of internet, social media, digital devices plateau in US. https://www.pewresearch.org/fact-tank/2018/09/28/internet-social-media-use-and-device-ownership-in-u-s-have-plateaued-after-years-of-growth/ [Google Scholar]
15. Entertainment Software Association (2019). 2019 essential facts about the computer and video game industry. https://www.theesa.com/wp-content/uploads/2019/05/2019-Essential-Facts-About-the-Computer-and-Video-Game-Industry.pdf [Google Scholar]
16. Bort-Roig, J., Gilson, N. D., Puig-Ribera, A., Contreras, R. S., Trost, S. G. (2014). Measuring and influencing physical activity with smartphone technology: A systematic review. Sports Medicine, 44(5), 671–686. https://doi.org/10.1007/s40279-014-0142-5 [Google Scholar] [PubMed] [CrossRef]
17. Gao, Z., Lee, J. E. (2019). Emerging technology in promoting physical activity and health: Challenges and opportunities. Journal of Clinical Medicine, 8(11), 1830. https://doi.org/10.3390/jcm8111830 [Google Scholar] [PubMed] [CrossRef]
18. Sousa, C. V., Hwang, J., Cabrera-Perez, R., Fernandez, A., Misawa, A. et al. (2022). Active video games in fully immersive virtual reality elicit moderate-to-vigorous physical activity and improve cognitive performance in sedentary college students. Journal of Sport and Health Science, 11(2), 164–171. https://doi.org/10.1016/j.jshs.2021.05.002 [Google Scholar] [PubMed] [CrossRef]
19. Pasco, D., Roure, C. (2022). Situational interest impacts college students’ physical activity in a design-based bike exergame. Journal of Sport and Health Science, 11(2), 172–178. https://doi.org/10.1016/j.jshs.2021.03.003 [Google Scholar] [PubMed] [CrossRef]
20. Gao, Z., Wang, R. (2022). Application of e-health programs in physical activity and health promotion. Journal of Sport and Health Science, 11(2), 131–132. https://doi.org/10.1016/j.jshs.2021.09.007 [Google Scholar] [PubMed] [CrossRef]
21. Gao, Z., Lee, J. E., McDonough, D. J., Albers, C. (2020). Virtual reality exercise as a coping strategy for health and wellness promotion in older adults during the COVID-19 pandemic. Journal of Clinical Medicine, 9(6), 1986. https://doi.org/10.3390/jcm9061986 [Google Scholar] [PubMed] [CrossRef]
22. Hamilton, D., McKechnie, J., Edgerton, E., Wilson, C. (2021). Immersive virtual reality as a pedagogical tool in education: A systematic literature review of quantitative learning outcomes and experimental design. Journal of Computers in Education, 8(1), 1–32. https://doi.org/10.1007/s40692-020-00169-2 [Google Scholar] [CrossRef]
23. Jerdan, S. W., Grindle, M., van Woerden, H. C., Boulos, M. N. K. (2018). Head-mounted virtual reality and mental health: Critical review of current research. JMIR Serious Games, 6(3), e14. https://doi.org/10.2196/games.9226 [Google Scholar] [PubMed] [CrossRef]
24. Qian, J., McDonough, D. J., Gao, Z. (2020). The effectiveness of virtual reality exercise on individual’s physiological, psychological and rehabilitative outcomes: A systematic review. International Journal of Environmental Research and Public Health, 17(11), 4133. https://doi.org/10.3390/ijerph17114133 [Google Scholar] [PubMed] [CrossRef]
25. McDonough, D. J., Pope, Z. C., Zeng, N., Liu, W., Gao, Z. (2020). Comparison of college students’ blood pressure, perceived exertion, and psychosocial outcomes during virtual reality, exergaming, and traditional exercise: An exploratory study. Games for Health Journal, 9(4), 290–296. https://doi.org/10.1089/g4h.2019.0196 [Google Scholar] [PubMed] [CrossRef]
26. Liu, W., Zeng, N., Pope, Z. C., McDonough, D. J., Gao, Z. (2019). Acute effects of immersive virtual reality exercise on young adults’ situational motivation. Journal of Clinical Medicine, 8(11), 1947. https://doi.org/10.3390/jcm8111947 [Google Scholar] [PubMed] [CrossRef]
27. McCloy, R., Stone, R. (2001). Virtual reality in surgery. British Medical Journal, 323(73), 912–915. [Google Scholar] [PubMed]
28. Laver, K. E., Lange, B., George, S., Deutsch, J. E., Saposnik, G. et al. (2017). Virtual reality for stroke rehabilitation. Cochrane Database of Systematic Reviews, 11, CD008349. https://doi.org/10.1002/14651858.CD008349.pub4 [Google Scholar] [PubMed] [CrossRef]
29. Ng, Y. L., Ma, F., Ho, F. K., Ip, P., Fu, K. (2019). Effectiveness of virtual and augmented reality-enhanced exercise on physical activity, psychological outcomes, and physical performance: A systematic review and meta-analysis of randomized controlled trials. Computers in Human Behavior, 99, 278–291. https://doi.org/10.1016/j.chb.2019.05.026 [Google Scholar] [CrossRef]
30. Neumann, D. L., Moffitt, R. L., Thomas, P. R., Loveday, K., Watling, D. P. et al. (2018). A systematic review of the application of interactive virtual reality to sport. Virtual Reality, 22(3), 183–198. https://doi.org/10.1007/s10055-017-0320-5 [Google Scholar] [CrossRef]
31. Miller, K. J., Adair, B. S., Pearce, A. J., Said, C. M., Ozanne, E. et al. (2014). Effectiveness and feasibility of virtual reality and gaming system use at home by older adults for enabling physical activity to improve health-related domains: A systematic review. Age and Ageing, 43(2), 188–195. https://doi.org/10.1093/ageing/aft194 [Google Scholar] [PubMed] [CrossRef]
32. World Medical Association (2013). World medical association declaration of Helsinki ethical principles for medical research involving human subjects. JAMA, 310(20), 2191–2194. https://doi.org/10.1001/jama.2013.281053 [Google Scholar] [PubMed] [CrossRef]
33. Goto, K., Nagasawa, M., Yanagisawa, O., Kizuka, T., Ishii, N. et al. (2004). Muscular adaptations to combinations of high-and low-intensity resistance exercises. Journal of Strength and Conditioning Research, 18(4), 730–737. https://doi.org/10.1519/00124278-200411000-00008 [Google Scholar] [CrossRef]
34. Whelton, S. P., Chin, A., Xin, X., He, J. (2002). Effect of aerobic exercise on blood pressure: A meta-analysis of randomized, controlled trials. Annals of Internal Medicine, 136(7), 493–503. https://doi.org/10.7326/0003-4819-136-7-200204020-00006 [Google Scholar] [PubMed] [CrossRef]
35. Zeng, N., Pope, Z., Gao, Z. (2017). Acute effect of virtual reality exercise bike games on college students’ physiological and psychological outcomes. Cyberpsychology Behavior and Social Networking, 20(7), 453–457. https://doi.org/10.1089/cyber.2017.0042 [Google Scholar] [PubMed] [CrossRef]
36. Gauvin, L., Rejeski, W. (1993). The exercise-induced feeling inventory-development and initial validation. Journal of Sport & Exercise Psychology, 15(4), 403–423. https://doi.org/10.1123/jsep.15.4.403 [Google Scholar] [CrossRef]
37. Richardson, J. T. E. (2011). Eta squared and partial eta squared as measures of effect size in educational research. Educational Research Review, 6(2), 135–147. https://doi.org/10.1016/j.edurev.2010.12.001 [Google Scholar] [CrossRef]
38. Rhodes, R. E., Kates, A. (2015). Can the affective response to exercise predict future motives and physical activity behavior? A systematic review of published evidence. Annals of Behavioral Medicine, 49(5), 715–731. https://doi.org/10.1007/s12160-015-9704-5 [Google Scholar] [PubMed] [CrossRef]
39. Shishehbor, M. H., Gordon-Larsen, P., Kiefe, C. I., Litaker, D. (2008). Association of neighborhood socioeconomic status with physical fitness in healthy young adults: The coronary artery risk development in young adults (CARDIA) study. American Heart Journal, 155(4), 699–705. https://doi.org/10.1016/j.ahj.2007.07.055 [Google Scholar] [PubMed] [CrossRef]
40. Freitas, D., Maia, J., Beunen, G., Claessens, A., Thomis, M. et al. (2007). Socio-economic status, growth, physical activity and fitness: The Madeira growth study. Annals of Human Biology, 34(1), 107–122. https://doi.org/10.1080/03014460601080983 [Google Scholar] [PubMed] [CrossRef]
Cite This Article
 Copyright © 2023 The Author(s). Published by Tech Science Press.
Copyright © 2023 The Author(s). Published by Tech Science Press.This work is licensed under a Creative Commons Attribution 4.0 International License , which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
 Downloads
Downloads
 Citation Tools
Citation Tools