
 Submit a Paper
Submit a Paper Propose a Special lssue
Propose a Special lssue Open Access
Open Access
ARTICLE

Study on the Relationship between Mental Health Literacy and Psychological Symptoms of University Students: Mediating Effect of Grit
1
Department of Nursing College of Nursing, Dongguk University, Gyeongju-si, 38066, Korea
2
Aeromedical Center of Korean Air, Seoul, 07505, Korea
3
Department of Nursing, Graduate School, Dongguk University, Gyeongju-si, 38066, Korea
* Corresponding Author: Jung-Ha Kim. Email:
International Journal of Mental Health Promotion 2023, 25(7), 813-821. https://doi.org/10.32604/ijmhp.2023.027383
Received 27 October 2022; Accepted 12 January 2023; Issue published 01 June 2023
 View Full Text
View Full Text Download PDF
Download PDFAbstract
Background: The occurrence of mental health symptoms is higher in individuals aged between 18 and 24 years than in other age groups. Mental health literacy is derived from health literacy, and focuses on the knowledge, attitudes, and competencies that individuals need to acquire to manage their own health effectively. Low mental health literacy is associated with poorer mental health. Grit is also a known protective factor against mental disorders. Despite a heightened focus on mental health literacy and grit as important factors for decreasing mental health symptoms, knowledge of the effect of mental health literacy and grit on mental health symptoms is very limited. This study aimed to evaluate the relationship between mental health literacy and psychological symptoms and the mediating effect of grit on these relationships. Methods: This cross-sectional descriptive study used survey data from 178 university students in Korea. Data were collected between March and May 2022. The SPSS PROCESS macro (Model 4) was used to analyze the data. Results: Mental health literacy was not directly associated with psychological symptoms. However, an indirect pathway was observed between mental health literacy, depression, and anxiety, through grit. Conclusion: Mental health literacy affects psychological symptoms through grit. Therefore, to improve the mental health of university students, it is necessary to develop programs that increase mental health literacy and grit.Keywords
With the increasing prevalence of mental disorders worldwide [1], approximately one-third of the world’s population experiences common mental disorders, such as anxiety and depression, at least once in their lifetime [2]. In the United States, the occurrence of mental disorders in individuals aged 18 to 24 years is approximately 3.56 times higher than that of other age groups [3]. In South Korea, a survey on mental illness in 2016 reported that 13.5% of the total population suffered from a mental illness (excluding alcohol and nicotine disorders) at least once in their lifetime. Moreover, depressive and anxiety disorders are predominant in individuals aged 18 to 24 years [4]. Therefore, young people’s mental health requires more attention.
As mental health problems among young people increase, recognizing warning signs early on and utilizing mental health services for early intervention is essential for recovery. However, compared to other countries, fewer people avail of mental health services in Korea. Only 9.6% of adults in Korea have used mental health services (psychiatric department, consultation with experts, etc.) for problems such as anxiety or depression during their lifetime [4]. In comparison, in the United States, 44.8% of adults have used mental health services in the past year [5]. The low utilization rate of mental health services hinders the early detection of mental disorders and worsens symptoms due to missed early intervention [6], thus increasing the risk of complications such as suicide [5,7].
The low utilization of mental health services may be attributed to a poor understanding of mental disorders, which delays early intervention. Particularly, among those diagnosed with anxiety disorder, the most common reasons for not consulting a specialist were “I thought that I did not have a mental illness” (77.5%) and “I thought that I could solve the problem by myself” (76.6%) [4]. Furthermore, it was found that young people felt reluctant to use mental health services due to stigma and lack of information from service organizations, as well as poor knowledge of mental disorders [8–10].
Mental health literacy, which is derived from health literacy focusing on the knowledge, attitudes, and competencies that individuals need to manage their health effectively, was first defined by Jorm et al. [11]: “knowledge and belief about mental disorders which aid their recognition, management, or prevention.” [11]. Later, Jorm [12] redefined it to include knowledge that benefits the mental health of individuals or others: (1) knowledge of how to prevent mental disorders, (2) recognition of when a disorder is developing, (3) knowledge of help-seeking options and treatments available, (4) knowledge of effective self-help strategies for milder problems, and (5) first-aid skills to support others developing mental disorders or in a mental crisis. Mental health literacy is an evolving concept that is gradually expanding, encompassing related research and sociocultural policies. Kutcher et al. [13] defined it as: (1) understanding how to obtain and maintain good mental health; (2) understanding mental disorders and their treatments; (3) decreasing stigma related to mental disorders; and (4) enhancing help-seeking efficacy (knowing when, where, and how to obtain good mental health care and developing necessary competencies for self-care). O’Connor and Casey developed a mental health literacy scale based on the conceptual components defined by Jorm et al. [11]. It comprises six domains: the ability to recognize disorders; attitudes that promote the recognition of appropriate help-seeking behavior; and knowledge of where to seek information, risk factors and causes, self-treatment, and available professional help [14]. According to previous studies, mental health literacy helps develop a positive attitude toward help-seeking behaviors, promotes the use of mental health services, and reduces mental illness and stigma [9,12,15,16]. Previous studies have reported that higher mental health literacy is associated with reduced depression, anxiety, and stress. People with inadequate mental health literacy had increased odds of approximately 60% for moderate to severe depression [17]. Anxiety due to COVID-19 is lower in people with higher health literacy [18]. Moreover, low health literacy has been associated with higher perceived stress [19,20]. However, there is strong evidence that mental health literacy has not been examined regarding anxiety or stress among Korean university students. Thus, it is essential to examine the relationship between mental health literacy and depression, anxiety, and stress among Korean university students.
Furthermore, Kutcher et al. [13] refer to “context” as the salient point to consider when developing methods to improve mental health literacy. An intervention method, evaluated and verified to improve all factors constituting mental health literacy, should be applied to appropriate individuals. Mental health literacy factors encompass knowledge about mental health based on the individual’s life history according to their current developmental stage in their life cycle, in terms of their sociocultural context, attitude, stigma, and help-seeking efficacy [13]. Moreover, before applying mental health literacy education, research on the most appropriate terms and educational content should be conducted among targeted college students, including evaluating their mental health literacy levels [15]. However, there are only three studies on the mental health literacy of Korean college students [15,21,22]. To our knowledge, no study has investigated the educational requirements for mental health literacy programs. As mentioned above, mental health problems such as depression, anxiety, and stress among university students have increased. There is thus an urgent need to develop educational programs to improve their mental health literacy. Therefore, it is necessary to confirm the educational needs of Korean university students when developing mental health literacy programs, considering their social context.
Grit is defined as the perseverance and passion for long-term goals, entailing working strenuously toward challenges, and maintaining effort and interest despite failure, adversity, and plateaus [23]. However, different social factors (relationships with parents, friends, peers, etc.) affect high enthusiasm and perseverance toward long-term goals according to sociocultural contexts. Datu et al. [24] extended the theory to the concept of the triarchic model of grit, including adaptability to situations; that is, an individual’s ability to effectively adjust to changing life circumstances. It is characterized by expecting, and accepting changes, being flexible, and displaying an impetus to overcome any new difficulties. Recently, grit has been considered a factor that positively affects individual mental health (emotional, psychological, and social well-being) [25]. A negative correlation between depression, anxiety, suicide, hopelessness, and grit is postulated as a protective factor for poor mental health [26–28]. In sum, grit means pursuing one’s passions, investing time and psychological resources to do so, and potentially sacrificing many other things to keep this pursuit firmly established [29]. Investing time and effort in various activities (internet searches, visiting mental health service centers, counseling, etc.) to improve one’s understanding of mental health is expected to increase one’s mental health literacy; recognition of psychological problems such as depression, anxiety, and stress; and reduce their occurrence through early detection and intervention. In other words, grit is expected to play a mediating role between mental health literacy and the psychological problems of university students. However, no study has confirmed the association between mental health literacy and grit or the mediating effect of grit on the relationship between mental health literacy and mental disorders. The research question of this study is: What is the relationship between mental health literacy, mental disorders, and grit?
Based on previous research, the following hypotheses were proposed. Hypothesis 1 (H1): mental health literacy has a negative association with psychological problems, such as depression, anxiety, and stress. Hypothesis 2 (H2): grit has a mediating effect on the relationship between mental health literacy and psychological problems.
This study used a cross-sectional descriptive design and aimed to investigate the relationship between mental health literacy and depression, anxiety, and stress among university students, and the mediating effect of grit on this relationship. Participants were recruited from a university in G City using convenience sampling. We excluded students who had been diagnosed with a mental illness. For regression analysis, the sample size was calculated using G*Power 3.1.9.2. The minimum number of participants needed to facilitate a statistical power of 0.95 at a significance level of 0.05, with the number of predictors being 10 based on the conservative median effect size of 0.15, as proposed by Cohen [30], was 172. We recruited 200 participants, considering a 20% dropout rate. Among the 200 respondents who answered the questions in the survey, only 178 completed the questionnaires. Therefore, 178 respondents (50 men and 128 women) were used for the final analysis.
Depression, anxiety, and stress (DASS-21)
This study used the Korean version of the Depression, Anxiety & Stress Scale 21 (DASS-21) [31]. The Korean version subscales (depression, anxiety, and stress) comprised seven items each [32]. The stress scale comprised items related to tension, sensitivity, and negative emotions. The responses were recorded on a 4-point Likert scale, ranging from 0 (“Did not apply to me at all”) to 3 (“Applied to me very much or most of the time”). The subscale scores ranged from 0 to 21, and the higher the score, the more severe the depression, anxiety, and stress. The DASS-21 is highly reliable, showing higher convergent validity than the other scales [33]. Lee et al. [32] found through 431 participants that the DASS-21 Korean version showed reliability of 0.81, 0.84, 0.85, and 0.93 for depression, anxiety, stress, and in total, respectively. In this study, the reliability for depression, anxiety, stress, and in total was 0.87, 0.81, 0.87, and 0.94, respectively.
Mental health literacy scale (MHLS)
To measure participants’ ability to understand mental health information, the Korean version of the Mental Health Literacy Scale, initially developed by O’Connor et al. [14], was used. The Korean version was translated and verified by Kim [34] for Korean university students and comprises 18 items. Examples of the items are as follows: “Do you think this person has a major depressive disorder if they feel depressed for more than two weeks, or they experience decreased interest and enjoyment in daily life and changes in appetite and sleep duration?” “Do you think that cognitive behavior therapy is aimed at changing the negative thoughts and enhancing positive ones?” “Is mental disease a medical disease?” “Are you willing to employ people who have experienced a mental disorder?” and so forth. Furthermore, the first six questions were rated on a 4-point Likert scale (1 = “definitely not,” 4 = “definitely”), and the subsequent 12 questions were rated on a 5-point Likert scale (1 = “not at all,” 5 = “a lot”). Scores ranged from 18 to 84 points, and the higher the total score, the higher the mental health literacy ability. Cronbach’s α for the Korean version of the Mental Health Literacy Scale was 0.76 in a previous study [34], and 0.74 in this study.
To measure the grit of college students, the Korean version [35] of the Triarchic model of the Grit Scale [24], which modified and validated the Short Grit Scale of Duckworth et al. [23], was used. The questionnaire comprised three areas with a total of 10 items: three questions regarding the consistency of interests (e.g., “I can be obsessed with a certain idea or project for a short time but later lost interest”), three questions about the perseverance of effort (e.g., “I finish whatever I start,” “I am diligent”), and four questions regarding adaptability to situations (e.g., “I can cope with changing circumstances in life”). Responses were recorded on a 5-point Likert scale. The items regarding consistency of interests are described negatively and rated reversely; therefore, the higher the score, the greater the passion for the goal. Cronbach’s α was 0.72 at the time of development and 0.71 in a previous study targeting Korean university students [36]. In this study, Cronbach’s α was 0.76.
Education needs for mental health literacy
The participants were surveyed on the following three items related to the educational needs for mental health literacy: the need for mental health education, means, and contents of education. Means for education were assessed using three options: face to face, online, and self-learning (for example, mobile applications). The author developed the education contents based on previous studies [12,13]. It was assessed via five options: symptoms of mental illness, causes and risk factors of mental health, treatment or intervention for mental illness, how to help people with mental illness, and how to obtain mental health information.
Experience related to mental health
To measure experience related to mental health, we administered three questionnaires. Previous experiences related to mental health, such as mental health education, visiting mental health clinics, and contact with mental health patients, were included and assessed using the following respective questions: “Have you ever participated in mental health education?” “Have you ever used any mental health services or university student counseling center for your mental health problems?” and “Have you had any contact with mental health patients?”.
This study was approved by the Institutional Review Board of 000 University (IRB No. 000 IRB 20210018). The only survey using a structured questionnaire was conducted from March 2022 to May 2022. Direct links to questionnaires were posted in an online advertisement on the university’s website. Upon clicking the hyperlink, the background, purpose, data collection procedure, and inclusion criteria were displayed. The second screen displayed the voluntary nature and confidentiality of the study. If the participant pressed the button, “I agree,” signifying their consent on the second screen, then the questionnaires followed. The survey took approximately 20 min to complete, and when the participants included their contact numbers, they were sent a mobile coupon as a token of appreciation for their participation.
The data were analyzed using SPSS/WIN 25.0 (IBM Corp., Armonk, NY, USA) and SPSS PROCESS macro, Version 3.4. The general characteristics and main variables were analyzed using descriptive statistics. Correlations with the main variables were analyzed using Pearson’s correlation coefficient. The covariates included sex, age, grade, monthly income, and whether they lived with family members during the semester. To investigate the mediating effect of grit, the PROCESS macro for SPSS (Model 4) was used [37]. A 95% bias-corrected confidence interval from 5000 resamples was generated using the bias-corrected bootstrapping method. Significant indirect effects were identified when the confidence interval did not include zero [38].
The results of verifying this study’s research question and hypotheses are as follows.
General characteristics, experiences of mental health education, and level of main variables
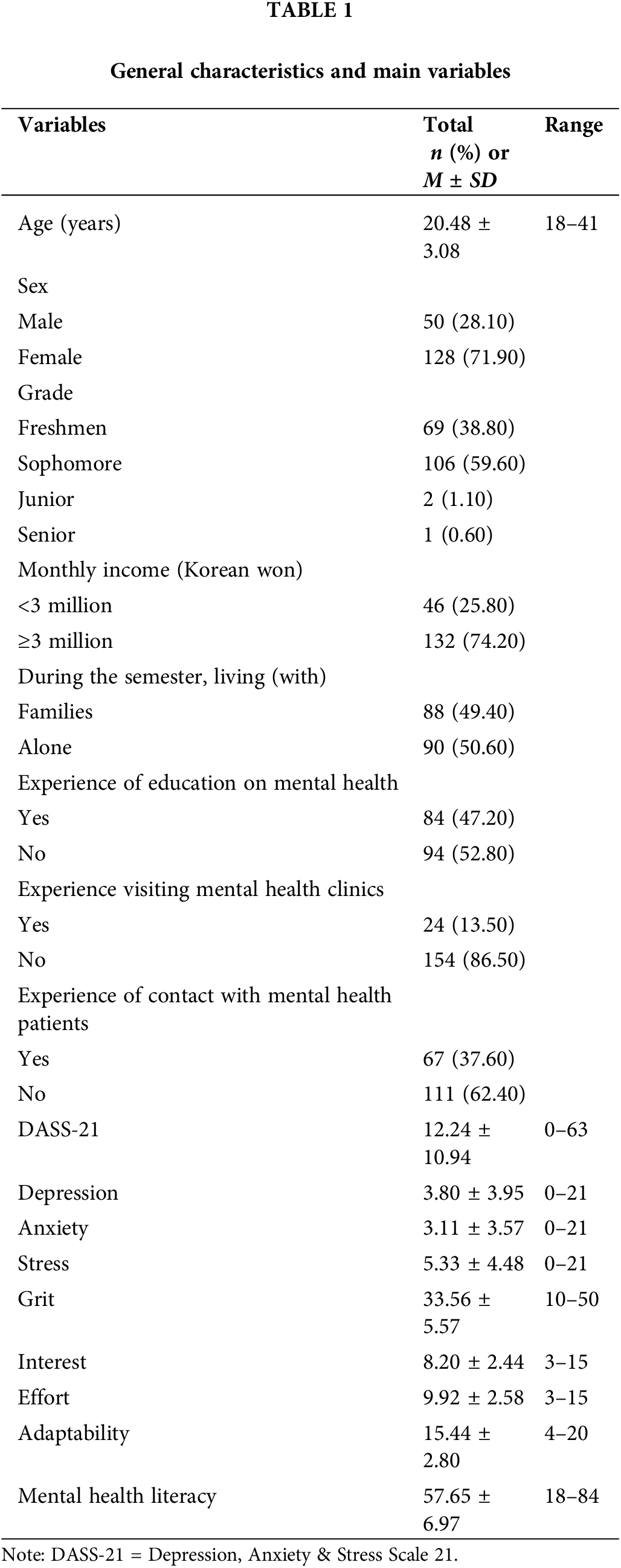
The mean age of the 178 participants was 20.48 years, with most students being freshmen and sophomores (98.7%). Ninety-four participants (52.8%) had no educational experience related to mental health, 24 (13.5%) had experience visiting mental health clinics, and 67 (32.6%) had contact with mental health patients. The mean scores for depression, anxiety, and stress were 3.80 ± 3.95, 3.11 ± 3.57, and 5.33 ± 4.48, respectively. Grit was 33.56 ± 5.57, and mental health literacy was 57.65 ± 6.97 (Table 1).
Education needs for mental health literacy
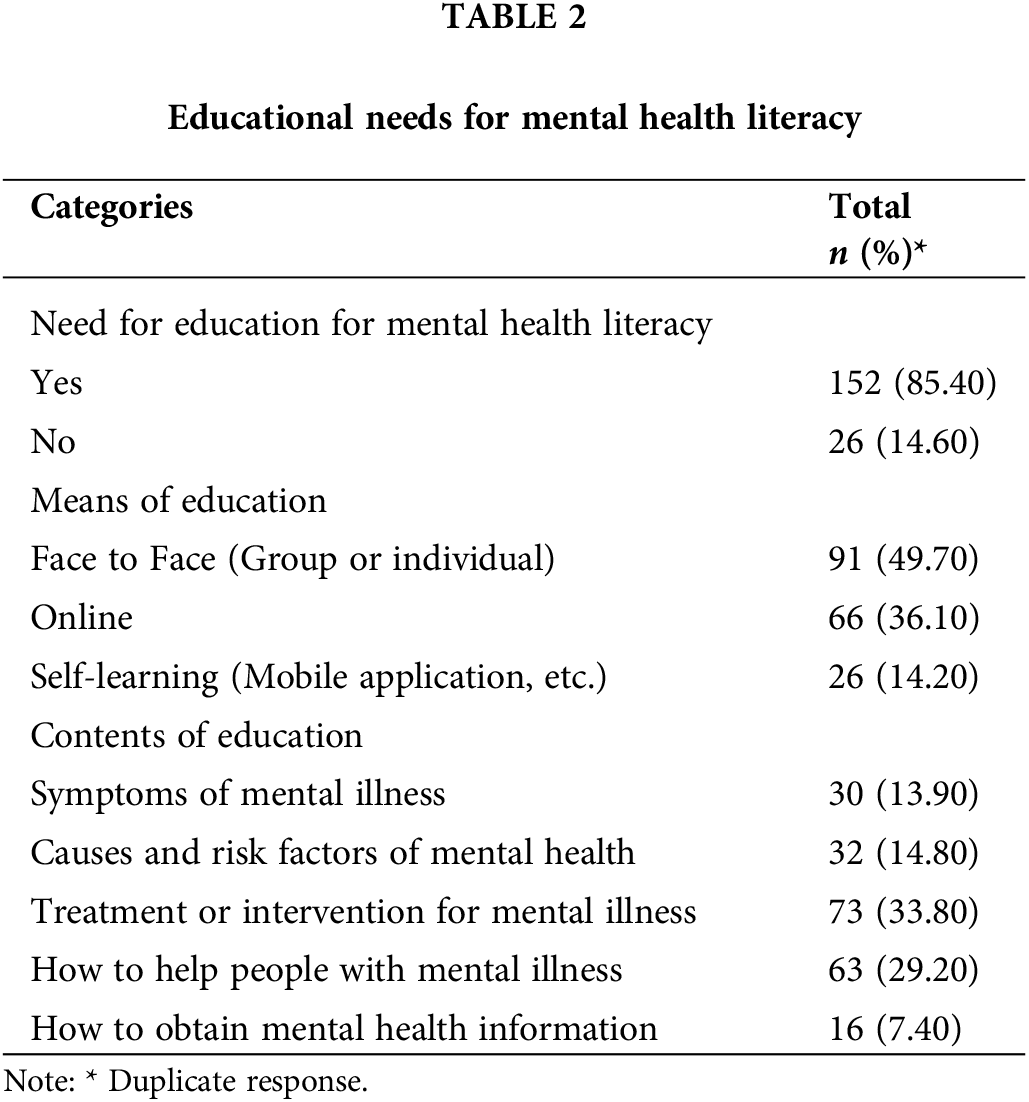
Of the participants, 85.4% indicated that education on mental health literacy was necessary. For the preferred educational method, 91 (49.7%) chose face to face education, whereas 66 (36.1%) preferred online education. Moreover, 73 (33.8%) participants wanted to learn about “Treatment or intervention for mental illness,” 63 (29.2%) wanted to know “How to help people with mental illness,” and 32 (14.8%) wanted to know “Causes and risk factors of mental health” (Table 2).
Correlation between depression, anxiety, stress, grit, and mental health literacy
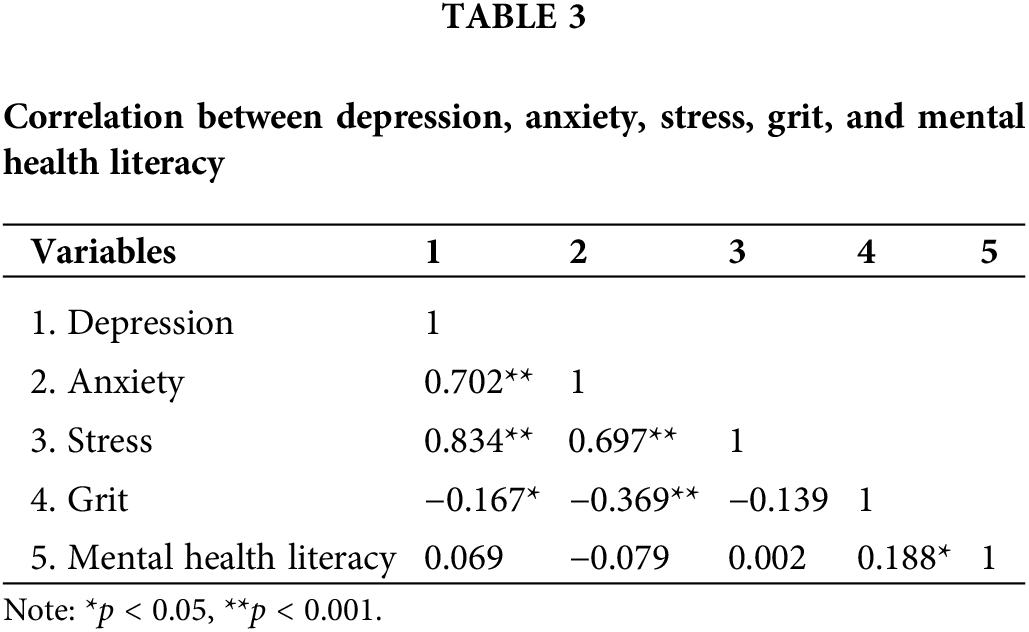
Mental health literacy was not correlated with depression, anxiety, or stress (r = −0.069, p = 0.357; r = −0.079, p = 0.297; r = 0.002, p = 0.981, respectively); however, it was positively correlated with grit (r = 0.19, p = 0.012). Thus, H1 was not supported. Grit was negatively correlated with depression (r = 0.37, p < 0.001) and anxiety (r = 0.17, p = 0.026) (Table 3).
Mediating effect of grit in the relationship between mental health literacy and depression, anxiety, and stress
As shown in Table 4, the mediation analysis showed that mental health literacy positively predicted grit (ß = −0.27, p < 0.001), and grit negatively predicted depression (ß = −0.27, p < 0.001) and anxiety (ß = −0.12, p = 0.012). The indirect effect of grit on stress was found to be insignificant because 0 was included in the boot CI phase. The index of mediation was significant, showing that the indirect effect of mental health literacy on depression and anxiety through grit was also significant (index = −0.04, −0.02, Boot SE = 0.02, 95% Boot CI: −0.09/−0.01, −0.05/−0.00, respectively). Thus, H2 was partially supported. Fig. 1 shows the mediating effect of grit on the relationship between mental health literacy and depression and anxiety.
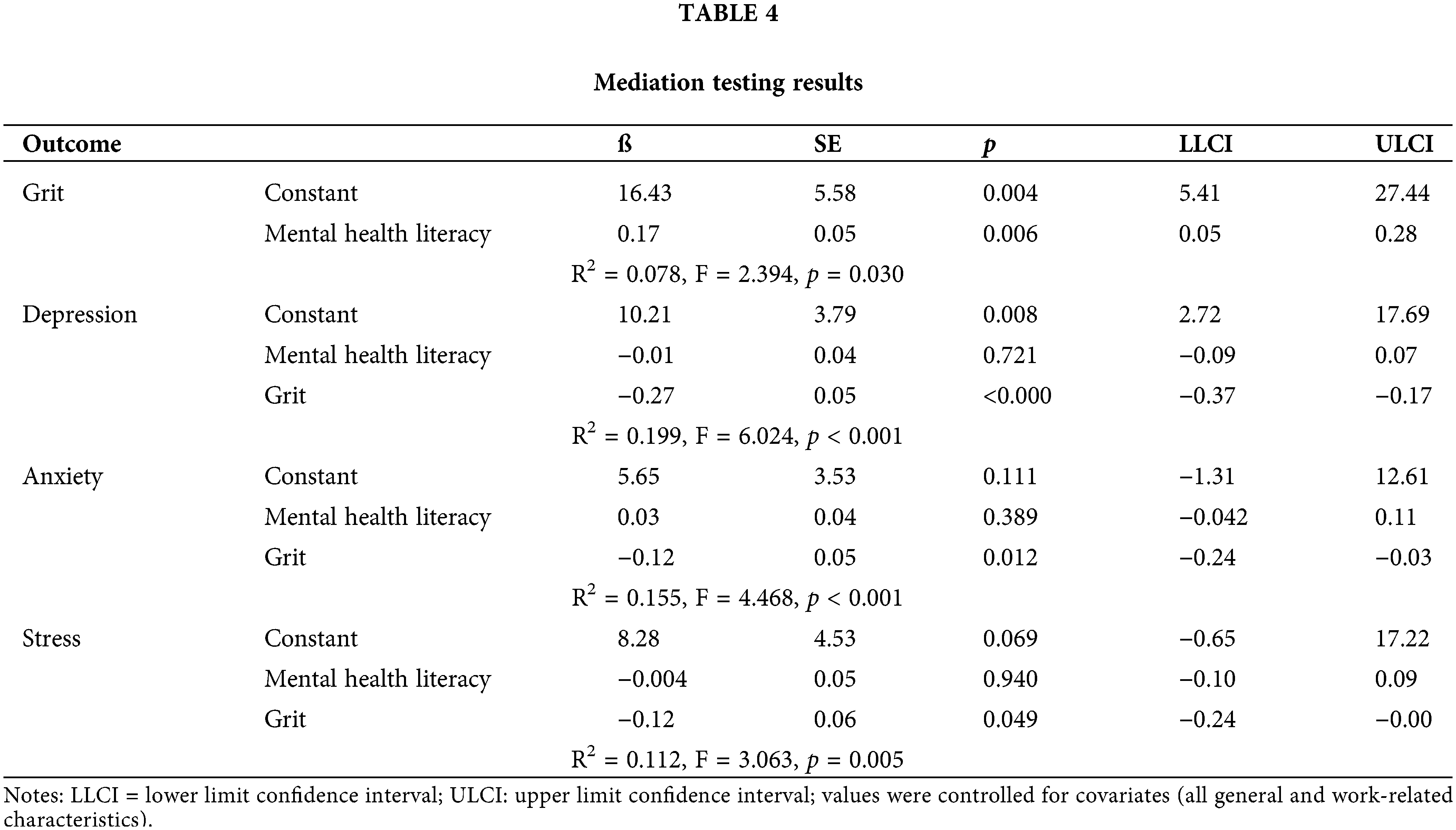
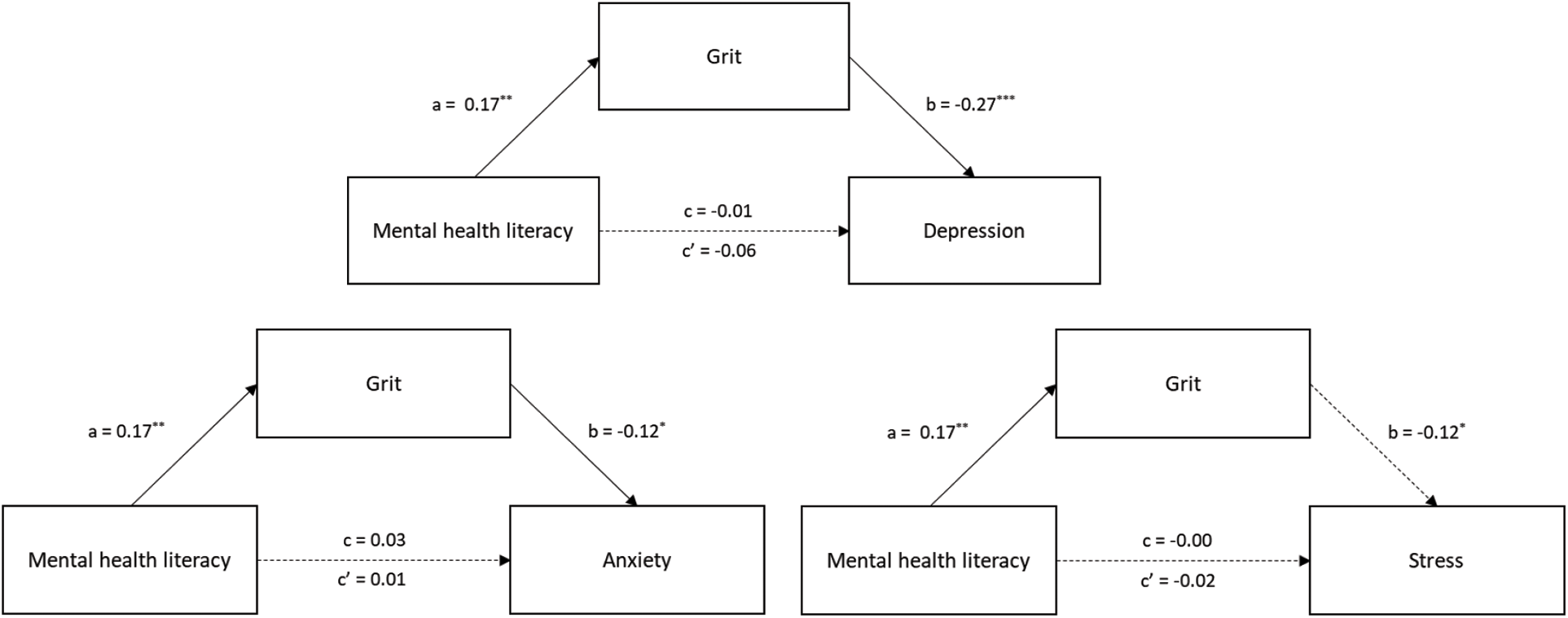
Figure 1: Mediating effect of Grit on the relationship between mental health literacy and depression, anxiety, and stress.
Notes: The solid arrow line represents a significant pathway; the dotted arrow line represents an insignificant pathway; the a & b coefficient signify indirect effect, the c coefficient signifies direct effect, the c′ coefficient represents the total effect of mental health literacy on depression, anxiety, or stress; *p < 0.05, **p < 0.01, ***p < 0.001.
The results partially support our hypothesis that grit has a mediating effect on the relationship between mental health literacy and depression and anxiety.
Inconsistent with H1, our findings revealed that mental health literacy is not associated with depression, anxiety, or stress. This result is consistent with the findings of previous studies. Beatie et al. [39] reported that mental health literacy was not associated with psychological symptoms measured using DASS-21 or distress [40]. However, the results contradicted previous studies showing that mental health literacy is associated with psychological symptoms [17–20,41]. A possible explanation for these contradictory results may be the psychological characteristics of the participants. Previous studies have reported that individuals with previous or present mental illness have higher levels of mental health literacy than those with no history of mental health symptoms [33,40]. In another study, mental health literacy was significantly lower in students with symptoms of depression [41]. However, in this study, the participants had never been diagnosed with a mental illness. Moreover, their depression, anxiety, and stress levels were low. In a previous study, which found a significant association between mental health literacy or health literacy and psychological symptoms measured by the DASS-21, the depression, anxiety, and stress of renal failure patients were 12.8 ± 9.8, 13.3 ± 8.5, and 12.4 ± 9.1, respectively [42]. Furthermore, in the study by Chaudhuri et al. [43], depression, anxiety, and stress of medical students were 10.82 ± 8.4, 12.34 ± 8.5, and 13.07 ± 8.01, respectively. The DASS-21 scores of these previous studies were 2.5–4 times higher than in our study; therefore, it is thought that there was no relationship between mental health literacy and psychological symptoms. Thus, future research could investigate the relationship between mental health literacy and psychological symptoms in persons with and without mental illness.
One notable finding was mental health literacy affects depression and anxiety (not stress) through grit, partially supporting H2. That is, mental health literacy is not directly affected by psychological symptoms; however, the mediation of grit promotes mental health literacy, which can increase grit and lead to decreased depression and anxiety. No studies have examined the relationship between mental health literacy and grit; therefore, a direct comparison is difficult. One study found that healthcare management skills, such as tracking illness, managing medication, and talking with providers, were positively associated with grit [44]. Moreover, grit is also strengthened by college experience, skills, and attitude about learning [45]. Moreover, when correct knowledge is sufficiently established, one’s belief that the goal of maintaining positive mental health can be achieved is fortified [46]. This can be explained by previous studies demonstrating that greater experience in learning about mental health, such as knowledge, symptoms, management (including treatment), and help-seeking, leads to higher mental health literacy [39,40]. Additionally, recognizing one’s mental health problems early and endeavoring to engage in various activities, such as searching for information related to mental health problems, engaging in treatment, or asking for help from professionals, aids the goal of recovery.
In our study, grit was negatively associated with depression and anxiety. This is consistent with previous studies demonstrating that higher grit is related to lower levels of depression and anxiety [26,28,47]. Gritty people are more likely to realize the meaning of life and are less likely to be depressed [47]. Similarly, grit is positively associated with life satisfaction [36]; individuals with anxiety are less likely to have lower levels of optimism and life satisfaction [48]. Although these factors were not investigated in this study, it is recommended that how grit affects psychological problems should be explored in the future.
However, grit was not associated with stress in this study. Therefore, grit did not have a mediating effect on the relationship between mental health literacy and stress. Wong et al. [49] also showed that perceived stress and grit were not significantly correlated. This may be because Korean university students view stress-related symptoms as daily stress and dismiss it as a minor problem; therefore, they do not view it as a mental illness [15]. Moreover, an individual’s grit and stress may vary over time, and the relationship between grit and stress may change significantly [49]. Therefore, the self-report questionnaire may not clearly reveal mental health factors such as stress. However, another study showed a relationship between grit and stress [50]. Regarding contrasting findings, several studies are needed to confirm the relationship between grit and stress.
We found that the need for mental health literacy education was high, consistent with a previous study [51]. This may be because many participants had received mental health education. A previous study reported that participants who had experience in mental health education responded that they needed it more often than participants without experience. Experience with mental health education in our study was higher (47.2%) than that in the previous study (26.4%). Furthermore, program content to help increase grit was in high demand. Regarding the contents of mental health literacy programs, the participants in our study wanted to learn about “treatment or intervention for mental illness” the most, followed by “how to help people with mental illness,” “causes and risk factors of mental health,” “symptoms of mental illness,” and “how to obtain mental health information”. To apply this to a school environment, universities should develop, promote, implement, and evaluate related educational content, including the “stigma-reduction strategy” [52] and core facets of grit. Furthermore, universities should secure a budget and human and material resources for mental health programs. Future research should also evaluate the development and effectiveness of mental health literacy programs.
Although this study provides a valuable preliminary assessment of the role of grit in the relationship between mental health literacy and psychological symptoms, a few limitations should be considered. First, this study had a cross-sectional design; therefore, it does not allow the interpretation of the causality of the relationship between mental health literacy, grit, and psychological symptoms. Future studies using a longitudinal design may contribute to a useful understanding of how the relationships between these variables, especially stress, change over time. Additionally, self-reported data were collected based on participants’ perceptions. Psychological symptoms may vary over time [49], and it is linked with recall bias; therefore, we may not be able to accurately gauge the levels of psychological symptoms and grit in university students. Finally, the effects of other confounding variables (i.e., relationship with friends, academic achievement, and adapting to university) on psychological symptoms or grit were not controlled for in this study. Therefore, such variables should be controlled for in future studies.
Despite these limitations, our results contribute to the literature on the relationship between mental health literacy and psychological symptoms. It suggests that grit plays an important role in university students’ mental health and literacy. The findings showed that grit had a mediating effect on the relationship between mental health literacy and depression and anxiety among university students.
University students commonly experience psychological problems such as depression, anxiety, and stress as they transition into adulthood and adapt to new environments [26,44]. Therefore, recognizing and developing the competence to overcome mental health problems faced by university students should be prioritized. Our results suggest that mental health literacy can decrease depression and anxiety in university students through grit. As university students recognize information on mental health, treatment methods, and help-seeking, and actively participate in mental health management with their efforts and continuous interest in overcoming them, psychological problems such as depression and anxiety decrease. Accordingly, it is necessary to develop and implement education programs to improve grit and mental health literacy for university students who suffer from psychological discomfort early in their university life.
Acknowledgement: This work was supported by the Dongguk University Research Fund of 2021.
Funding Statement: The authors received no specific funding for this study.
Author Contributions: The authors confirm contribution to the paper as follows: study conception and design: J.Y.W.; data collection: P.H.K.; analysis and interpretation of results: J.Y.W., and P.H.K.; draft manuscript preparation: J.Y.W., and K.J.H. All authors reviewed the results and approved the final version of the manuscript.
Conflicts of Interest: The authors declare that they have no conflicts of interest to report regarding the present study.
References
1. World Health Organization. Depression and other common mental disorders: global health estimates [Internet]. Geneva; World Health Organization; 2017. [Google Scholar]
2. Steel Z, Marnane C, Iranpour C, Chey T, Jackson JW, Patel V, et al. The global prevalence of common mental disorders: a systematic review and meta-analysis 1980–2013. Int J Epidemiol [Internet]. 2014;43(2):476–93. [Google Scholar] [PubMed]
3. Czeisler MÉ, Lane RI, Wiley JF, Czeisler CA, Howard ME, Rajaratnam SMW. Follow-up survey of US adult reports of mental health, substance use, and suicidal ideation during the COVID-19 pandemic, September 2020. JAMA Netw Open [Internet]. 2021;4(2):e2037665. [Google Scholar] [PubMed]
4. Ministry of Health and Welfare and Samsung Medical Center. The survey of mental disorders in Korea [Internet]. Sejong: Ministry of Health and Welfare; 2017. [Google Scholar]
5. McCance-Katz EF. The national survey on drug use and health: 2017 [Internet]. Substance Abuse and Mental Health Services Administration; 2019. [Google Scholar]
6. de Girolamo G, Dagani J, Purcell R, Cocchi A, McGorry PD. Age of onset of mental disorders and use of mental health services: needs, opportunities and obstacles. Epidemiol Psych Sci [Internet]. 2012;21(1):47–57. [Google Scholar]
7. World Health Organization. Comprehensive mental health action plan 2013–2020 [Internet]. Geneva: World Health Organization; 2013. [Google Scholar]
8. Shahwan S, Lau JH, Goh CMJ, Ong WJ, Tan GTH, Kwok KW, et al. The potential impact of an anti-stigma intervention on mental health help-seeking attitudes among university students. BMC Psychiatry [Internet]. 2020;20(1):1–14. [Google Scholar]
9. Jung H, von Sternberg K, Davis K. The impact of mental health literacy, stigma, and social support on attitudes toward mental health help-seeking. Int J Ment Health Pr [Internet]. 2017;19(5):252–67. [Google Scholar]
10. Pompeo-Fargnoli A. Mental health stigma among college students: misperceptions of perceived and personal stigmas. J Am Coll Health [Internet]. 2020;70(4):1030–9. [Google Scholar] [PubMed]
11. Jorm AF, Korten AE, Jacomb PA, Christensen H, Rodgers B, Pollitt P. Mental health literacy: a survey of the public’s ability to recognise mental disorders and their beliefs about the effectiveness of treatment. Med J Australia [Internet]. 1997;166(4):182–6. [Google Scholar] [PubMed]
12. Jorm AF. Mental health literacy: empowering the community to take action for better mental health. Am Psychol [Internet]. 2012;67(3):231–243. [Google Scholar] [PubMed]
13. Kutcher S, Wei Y, Coniglio C. Mental health literacy: past, present, and future. Can J Psychiatry [Internet]. 2016;61(3):154–8. [Google Scholar] [PubMed]
14. O’Connor M, Casey L. The Mental Health Literacy Scale (MHLSa new scale-based measure of mental health literacy. Psychiat Res [Internet]. 2015;229(1–2):511–6. [Google Scholar]
15. Kim HC. Mental health literacy as a mediator on the relationship between depression and actual mental health help-seeking behaviors among university students in South Korea. Ment Health Soc Work [Internet]. 2020;48(2). doi:https://doi.org/10.24301/MHSW.2020.06.48.2.5. [Google Scholar] [CrossRef]
16. Schnyder N, Panczak R, Groth N, Schultze-Lutter F. Association between mental health-related stigma and active help-seeking: systematic review and meta-analysis. Br J Psychiatry [Internet]. 2017;210(4):261–8. [Google Scholar] [PubMed]
17. Lam LT. Mental health literacy and mental health status in adolescents: a population-based survey. Child Adol Psych Men [Internet]. 2014;8(1):1–8. [Google Scholar]
18. Duplaga M, Grysztar M. The association between future anxiety, health literacy and the perception of the COVID-19 pandemic: a cross-sectional study. Healthcare [Internet]. 2021;9(1):43. [Google Scholar] [PubMed]
19. Hoover DS, Vidrine JI, Shete S, Spears CA, Cano M. Health literacy, smoking, and health indicators in African American adults. J Health Commun [Internet]. 2015;20(Suppl 2):24–33. [Google Scholar] [PubMed]
20. Michou M, Panagiotakos DB, Lionis C, Costarelli V. Low health literacy and perceived stress in adults: is there a link? Cent Eur J Publ Heal [Internet]. 2021;29(3):195–200. doi:https://doi.org/10.21101/cejph.a6692. [Google Scholar] [PubMed] [CrossRef]
21. Cho S, Choi S. Mental health literacy among people with mental disorder: correlations with socio-demographic factors, self-esteem, family support. Korean Assoc Heal Med Soc [Internet]. 2017;44:165–86. [Google Scholar]
22. Baik J, Lee HY, Nam HE. Nam, research trend analysis of health and mental health literacy in Korea: 2007–2017. Korean J Heal Serv Manag [Internet]. 2018;12(3):95–106. doi:https://doi.org/10.12811/kshsm.2018.12.3.095. [Google Scholar] [CrossRef]
23. Duckworth AL, Peterson C, Matthews MD, Kelly DR. Grit: perseverance and passion for long-term goals. J Pers Soc Psychol [Internet]. 2007;92(6):1087–101. doi:https://doi.org/10.1037/0022-3514.92.6.1087. [Google Scholar] [PubMed] [CrossRef]
24. Datu JAD, Yuen M, Chen G. Development and validation of the Triarchic Model of Grit Scale (TMGSevidence from Filipino undergraduate students. Pers Indiv Differ [Internet]. 2017;114(5):198–205. doi:https://doi.org/10.1016/j.paid.2017.04.012. [Google Scholar] [CrossRef]
25. Chung JH, Yang S. The relationship between grit and mental well-being among young adults: the mediating effects of career calling and job-seeking stress. Korean J Dev Psychol [Internet]. 2019;32(3):37–59. doi:https://doi.org/10.35574/KJDP.2019.09.32.3.37. [Google Scholar] [CrossRef]
26. Musumari PM, Tangmunkongvorakul A, Srithanaviboonchai K, Techasrivichien T, Suguimoto SP, Ono-Kihara M, et al. Grit is associated with lower level of depression and anxiety among university students in Chiang Mai, Thailand: a cross-sectional study. PLoS One [Internet]. 2018;13(12):e0209121. doi:https://doi.org/10.1371/journal.pone.0209121. [Google Scholar] [PubMed] [CrossRef]
27. Pennings SM, Law KC, Green BA, Anestis MD. The impact of grit on the relationship between hopelessness and suicidality. Int J Cogn Ther [Internet]. 2015;8(2):130–42. doi:https://doi.org/10.1521/ijct.2015.8.2.130. [Google Scholar] [CrossRef]
28. Umucu E, Villegas D, Viramontes R, Jung H, Lee B. Measuring grit in veterans with mental illnesses: examining the model structure of grit. Psychiatr Rehabil J [Internet]. 2021;44(1):87–92. doi:https://doi.org/10.1037/prj0000420. [Google Scholar] [PubMed] [CrossRef]
29. Bashant J. Developing grit in our students: why grit is such a desirable trait, and practical strategies for teachers and schools. J Leadersh Instr [Internet]. 2014;13(2):14–7. [Google Scholar]
30. Cohen J. Statistical power analysis. Curr Dir Psychol Sci [Internet]. 1992;1(3):98–101. doi:https://doi.org/10.1111/1467-8721.ep10768783. [Google Scholar] [CrossRef]
31. Lovibond SH, Lovibond PF. Manual for the depression anxiety stress scales [Internet]. 2nd ed. Sydney: Psychology Foundation; 1995. [Google Scholar]
32. Lee EH, Moon SH, Cho MS, Park ES, Kim SY. The 21-item and 12-item versions of the depression anxiety stress scales: psychometric evaluation in a Korean population. Asian Nurs Res [Internet]. 2019;13(1):30–7. doi:https://doi.org/10.1016/j.anr.2018.11.006. [Google Scholar] [PubMed] [CrossRef]
33. Henry JD, Crawford JR. The short-form version of the Depression Anxiety Stress Scales (DASS-21construct validity and normative data in a large non-clinical sample. Brit J Clin Psychol [Internet]. 2005;44(2):227–39. doi: https://doi.org/10.1348/014466505X29657. [Google Scholar] [PubMed] [CrossRef]
34. Kim HC. A validation study on the Korean version of Mental Health Literacy Scale (MHLS-K) in a sample of university students. Ment Health Soc Work [Internet]. 2019;47(2). [Google Scholar]
35. Kim J, Ryu Y, Choi H, Yang S. A validation study of the Korean triarchic model of grit scale (K-TMGS) in university students. In: Annual Conference of the Korean Society for Developmental Psychology [Internet]; 2017;Seoul, Korea. [Google Scholar]
36. Ryu Y, Yang S. On the mediating effects of grit and prosocial behavior in the relationship between intrinsic vs. prosocial motivation and life satisfaction. Korean J Dev Psychol [Internet]. 2017;30(4):93–115. [Google Scholar]
37. Hayes AF. Introduction to mediation, moderation, and conditional process analysis: a regression-based approach [Internet]. New York: Guilford Publications; 2017. [Google Scholar]
38. Hayes AF, Rockwood NJ. Regression-based statistical mediation and moderation analysis in clinical research: observations, recommendations, and implementation. Behav Res Ther [Internet]. 2017;98:39–57. doi:https://doi.org/10.1016/j.brat.2016.11.001. [Google Scholar] [PubMed] [CrossRef]
39. Beatie BE, Stewart DW, Walker JR. A moderator analysis of the relationship between mental health help-seeking attitudes and behaviours among young adults. Can J Couns Psychother Res [Internet]. 2016;50(3):290–314. [Google Scholar]
40. Gorczynski P, Sims-Schouten W, Hill D, Wilson JC. Examining mental health literacy, help seeking behaviours, and mental health outcomes in UK university students. J Ment Health Train Educ Pract [Internet]. 2017;12(2):111–20. doi:https://doi.org/10.1108/JMHTEP-05-2016-0027. [Google Scholar] [CrossRef]
41. Thai TT, Vu NLLT, Bui HHT. Mental health literacy and help-seeking preferences in high school students in Ho Chi Minh City, Vietnam. Sch Ment Health [Internet]. 2020;12(2):378–87. doi:https://doi.org/10.1007/s12310-019-09358-6. [Google Scholar] [CrossRef]
42. Qobadi M, Besharat MA, Rostami R, Rahiminezhad A, Pourgholami M. Health literacy, negative emotional status, and self-care behaviors in dialysis. J Fundam Mental Health [Internet]. 2014;17(1):46–51. [Google Scholar]
43. Chaudhuri A, Paul S, Saha E. A comparative study to assess mental health literacy, impact of event, depression, anxiety, and stress levels of medical and other students during the second wave of the COVID-19 pandemic. J Sci Soc [Internet]. 2022;49(1):35–9. doi:https://doi.org/10.4103/jss.jss_143_21. [Google Scholar] [CrossRef]
44. Sharkey CM, Bakula DM, Gamwell KL, Mullins AJ, Chaney JM, Mullins LL. The role of grit in college student health care management skills and health-related quality of life. J Pediatr Psychol [Internet]. 2017;42(9):952–61. doi:https://doi.org/10.1093/jpepsy/jsx073. [Google Scholar] [PubMed] [CrossRef]
45. Weisskirch RS. Grit, self-esteem, learning strategies and attitudes and estimated and achieved course grades among college students. Curr Psychol [Internet]. 2018;37(1):21–7. doi:https://doi.org/10.1007/s12144-016-9485-4. [Google Scholar] [CrossRef]
46. Lee HW, Tak JH, Lee MR. The differences of pre-service early childhood teachers’ big five personality factors and self-efficacy according to cluster types based on the grit. J Early Child Educ Res [Internet]. 2017;37(3):249–68. doi:https://doi.org/10.18023/kjece.2017.37.3.012. [Google Scholar] [CrossRef]
47. Datu JAD, King RB, Valdez JPM, Eala MSM. Grit is associated with lower depression viad meaning in life among Filipino high school students. Youth Soc [Internet]. 2019;51(6):865–76. doi:https://doi.org/10.1177/0044118X18760402. [Google Scholar] [CrossRef]
48. Tuckwiller B, Dardick WR. Mindset, grit, optimism, pessimism, and life satisfaction in university students with and without anxiety and/or depression. J Interdiscip Stud Educ [Internet]. 2018;6(2):32–48. [Google Scholar]
49. Wong ML, Anderson J, Knorr T, Joseph JW, Sanchez LD. Grit, anxiety, and stress in emergency physicians. Am J Emerg Med [Internet]. 2018;36(6):1036–9. doi:https://doi.org/10.1016/j.ajem.2018.02.021. [Google Scholar] [PubMed] [CrossRef]
50. Lee WWS. Relationships among grit, academic performance, perceived academic failure, and stress in associate degree students. J Adolescence [Internet]. 2017;60(1):148–52. doi:https://doi.org/10.1016/j.adolescence.2017.08.006. [Google Scholar] [PubMed] [CrossRef]
51. Park JM, Jeong WI. Health education needs and mental health education of college student. J Korea Contents Assoc [Internet]. 2013;13(10):385–93. doi:https://doi.org/10.5392/JKCA.2013.13.10.385. [Google Scholar] [CrossRef]
52. Kutcher S, Wei Y, Costa S, Gusmão R, Skokauskas N. Enhancing mental health literacy in young people. Eur Child Adoles Psy [Internet]. 2016;25(6):567–9. doi:https://doi.org/10.1007/s00787-016-0867-9. [Google Scholar] [PubMed] [CrossRef]
Cite This Article
 Copyright © 2023 The Author(s). Published by Tech Science Press.
Copyright © 2023 The Author(s). Published by Tech Science Press.This work is licensed under a Creative Commons Attribution 4.0 International License , which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
 Downloads
Downloads
 Citation Tools
Citation Tools