
 Submit a Paper
Submit a Paper Propose a Special lssue
Propose a Special lssue Open Access
Open Access
ARTICLE

Psychometric Properties of the Shortened Committed Action Questionnaire (CAQ-8): Evidence from Classical Test Theory and Network Analysis
School of Educational Science, Anhui Normal University, Wuhu, 241000, China
* Corresponding Author: Shuanghu Fang. Email:
International Journal of Mental Health Promotion 2025, 27(1), 65-76. https://doi.org/10.32604/ijmhp.2024.059324
Received 04 October 2024; Accepted 02 December 2024; Issue published 31 January 2025
 View Full Text
View Full Text Download PDF
Download PDFAbstract
Objectives: This study aimed to assess the reliability and validity of the abbreviated Committed Action Questionnaire (CAQ-8) in a cohort of 1635 Chinese university students. Methods: Participants completed the Chinese version of the CAQ-8 along with other standardized measures, including the Acceptance and Action Questionnaire-II (AAQ-II), the Valuing Questionnaire (VQ), the Satisfaction with Life Scale (SWLS), the Depression Anxiety Stress Scales (DASS-21), and the World Health Organization Five-item Well-Being Index (WHO-5). A retest was conducted one month later with 300 valid responses. Results: Exploratory factor analysis (n = 818) identified a 2-factor structure, confirmed through validated factor analysis (n = 817), showing good fit indices (CFI = 0.990, RMSEA = 0.040). Measurement equivalence across genders was established. The CAQ-8 showed significant positive correlations with life satisfaction, mental health, and values, and negative correlations with depression, anxiety, stress, and experiential avoidance. The scale demonstrated good internal consistency (Cronbach’s α = 0.76) and retest reliability (ICC = 0.70). Network analysis confirmed the robustness of the 2-factor model, with item 4 in CAQ-8 identified as a core item. Conclusion: The CAQ-8 is a reliable and valid tool for measuring committed action within the psychological flexibility model in Chinese populations.Keywords
Psychological flexibility is at the heart of the third wave of cognitive behavioral therapy, Acceptance and Commitment Therapy (ACT) [1]. Psychological flexibility refers to the ability to adaptively respond to changing circumstances, thoughts, and emotions in order to pursue one’s values and goals [2]. Research has shown that psychological flexibility can play an important role in the treatment of psychological disorders such as depression [3], obsessive-compulsive disorder [4], chronic pain [5,6], body awareness [7], emotional well-being [8], and life satisfaction [9]. Meanwhile, the role of psychological flexibility has been demonstrated across a range of age groups [10–13]. Psychological flexibility enables individuals to adapt to diverse situational demands, shift their mindset or behavior in personal and social contexts, balance key life domains, and engage in value-driven behaviors with openness, awareness, and commitment [14]. A large body of research has shown that psychological flexibility significantly improves mental health in a variety of populations [15,16], and it is also receiving increasing attention in China [17].
Hayes developed a model of psychological flexibility based on fundamental concepts and the analysis of numerous clinical cases. This model includes six processes: acceptance, cognitive defusion, present moment awareness, self-as-context, value clarification, and committed action [18,19]. Of these, committed action, centered on effective and flexible behaviors aligned with valued life directions, is defined by a balanced approach that embraces failure and discomfort as integral to achieving goals [20]. Research suggests that committed action can have a positive impact on mental health by promoting resilience and persistence [20–23]. Moreover, committed action interacts synergistically with other psychological flexibility processes [24]. For instance, acceptance and cognitive defusion can help individuals maintain committed action by reducing the impact of distressing thoughts and emotions, while present moment awareness and self-as-context provide a mindful and flexible perspective. Value clarification ensures that actions are meaningful and aligned with personal values, enhancing motivation and commitment.
While several measures exist for assessing the core processes within the six dimensions of psychological flexibility, some dimensions have fewer validated options, particularly when considering the need for versions in multiple languages. The Acceptance and Action Questionnaire-II (AAQ-II) measures experiential avoidance [25]; the Anxiety Flexibility Questionnaire-Youth (AFQ-Y) assesses experiential avoidance and cognitive fusion in adolescents [26]; the Mindful Attention Awareness Scale (MAAS) evaluates attention to the present moment [27]; and the Brief Experiential Avoidance Questionnaire (BEAQ) tests experiential avoidance [28]. However, there is a notable lack of validated instruments for measuring the committed action dimension, particularly across different languages.
To address this gap, McCracken developed the first measure of committed action, the Committed Action Questionnaire (CAQ) [21]. Originally developed for assessing committed action in pain patients, the CAQ has garnered attention from various researchers who argue for its applicability across a broader spectrum of clinical and non-clinical populations [29–31]. As a result, the use of the CAQ has expanded significantly beyond its initial focus, demonstrating its relevance in diverse psychological contexts [24]. To streamline data collection and reduce the burden on patients, McCracken developed a shortened version, the CAQ-8 [20]. Although other instruments such as the Engaged Living Scale (ELS) exist to measure engagement with values, they do not specifically target committed action. The ELS aims primarily to assess valued living and life fulfillment [23], which may not adequately reflect the distinct process of committed action. In contrast, the CAQ-8 is explicitly tailored to evaluate how individuals maintain commitment to their valued behaviors despite various obstacles, making it a more appropriate choice for measuring committed action in ACT.
Different countries have validated both the original and the shortened version, demonstrating satisfactory reliability and validity [29–31]. Chinese culture emphasizes collectivism, social norms, and family values, which are markedly different from those of Western cultures [32,33]. These cultural factors may lead to varying levels of committed action. In collectivist societies, individuals often exhibit distinct patterns of committed action due to the emphasis on social harmony and family obligations. Research indicates that the interconnectedness within these cultures influences the expression and measurement of psychological flexibility. For instance, collectivist values can enhance commitment to group goals and adherence to social norms, impacting how committed action is practiced and perceived [34]. Consequently, when adapting psychological measures like the CAQ-8 for Chinese populations, it is crucial to consider these cultural nuances to ensure accurate assessment and relevance [35,36].
Chinese scholars have also verified Chinese version of CAQ-8, (ChCAQ-8) [37]. However, the ChCAQ-8 was designed for chronic pain patients, with a sample size of 210, while our study focuses on the general population, with a larger sample of 1700, enhancing its generalizability. Although previous research has validated the CAQ-8 in non-clinical samples, particularly among university students, these studies primarily relied on traditional psychometric evaluation methods [38]. Our research seeks to enhance this validation by employing network analysis, which allows for a more sophisticated exploration of the intricate relationships between scale items and other psychological constructs [39]. Network analysis illustrates the relationships between different scales or items by representing them as nodes, with the connections between these nodes depicted as lines [40]. This method for measuring the dimensionality of psychological data is called exploratory graph analysis [41]. According to this approach, an individual’s level of committed action does not stem from underlying factors alone but from the interactions between its observable indicators (scale items), which facilitates a better understanding of the mechanisms of committed action [42]. Numerous studies in psychology, including those on personality [43,44], emotion [45], empathy [46], mental disorders [47], and happiness [48], have employed the network analysis approach. Network analysis has demonstrated significant success in scale development and validation [49–51]. Through this innovative approach, our study aims to contribute significantly to the literature on committed action measurement among Chinese university students.
Our study aims to develop and validate Chinese measurement instruments for assessing committed action levels among Chinese university students, facilitating their broader application across Chinese populations. Fine-grained measures of psychological flexibility dimensions are essential for advancing research in China. Specifically, we adapt the CAQ-8 for Chinese contexts, testing its reliability and validity. Additionally, we use network analysis alongside traditional methods to comprehensively assess the CAQ-8’s applicability [52].
We recruited university students to complete the questionnaire online via the Internet (Questionnaire Star). The questionnaire links were distributed through social media groups (such as WeChat and QQ) to ensure broad reach and encourage participation. To ensure the quality of responses, we incorporated intentional screening questions after every 20 to 30 items in the questionnaire. These screening questions had fixed response requirements (for example, please select “strongly disagree”), and participants who answered incorrectly were considered to have not engaged carefully with the survey and were subsequently excluded from the study. Only those participants who correctly answered all screening questions had their questionnaires retained for analysis.
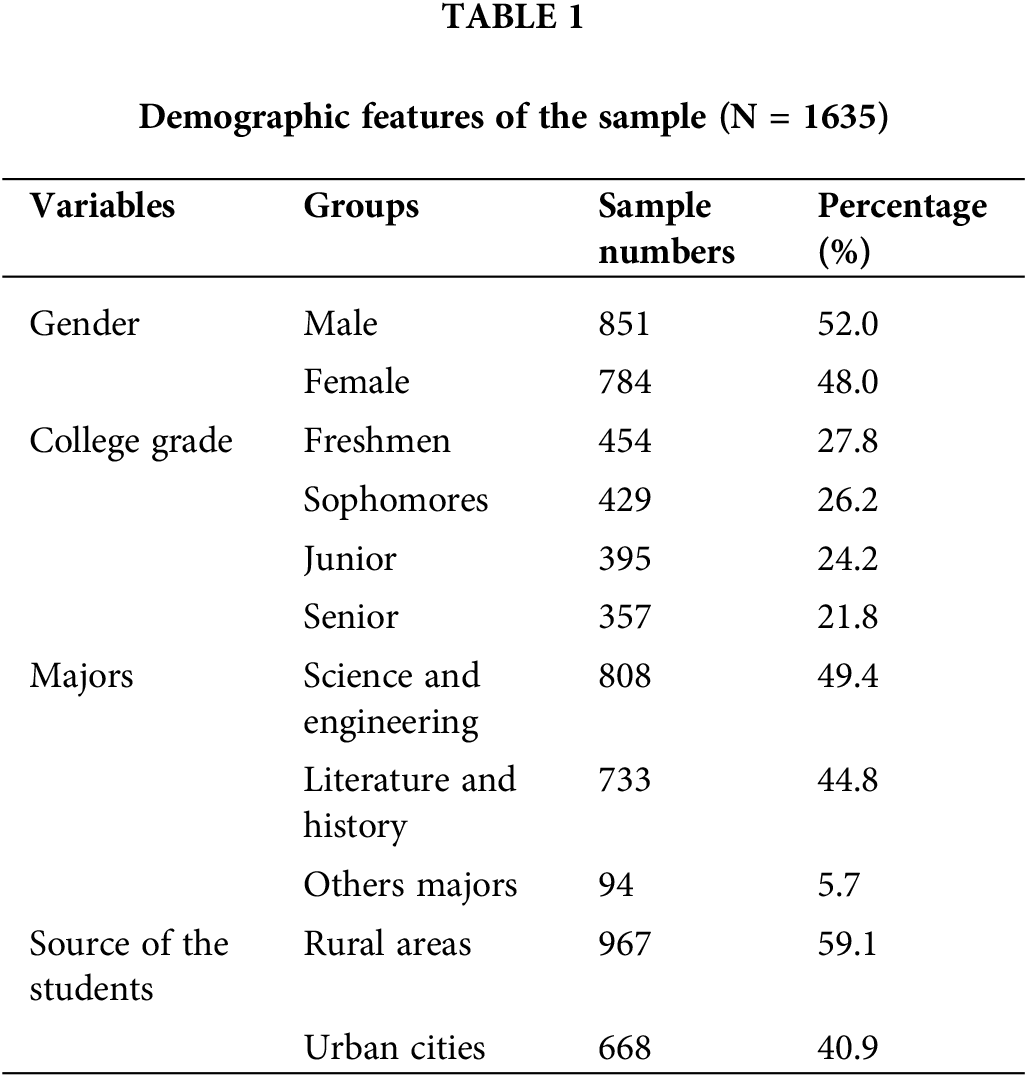
A priori, we calculated using G*Power version 3 that to detect a small effect size of 0.1 with a statistical power of 0.9, a sample size of 850 would be required [53]. A total of 1700 questionnaires were collected. After excluding invalid responses, 1635 valid questionnaires remained, resulting in an effective recovery rate of 96.18%. The mean age of the participants was 19.40 years, with a standard deviation of 1.14. Details are shown in Table 1.
In our study, we assessed the test-retest reliability of the CAQ-8 by conducting a follow-up assessment one month after the initial administration. This interval was chosen to allow sufficient time for participants to engage in their daily activities without substantial changes in their psychological states, while also ensuring the stability of their responses. When retesting, 323 questionnaires were distributed, and 300 valid questionnaires were collected.
With the original authors’ consent, we obtained the right to revise and use the CAQ-8 questionnaire in Chinese. We Chineseized the CAQ-8 using the translation-back-translation method. The Process of Chinese Translation: First, the CAQ-8 was translated into Chinese by the corresponding author of this paper, a psychology professor with more than 10 years of experience in ACT research and practice. Then, the first draft of the Chinese version of the scale was created by discussing and adjusting ambiguous items with members of the project team. Second, two other psychologists working in the United States translated the first draft of the Chinese version back into English. They referred to the comments of the project team and came up with the English version of the scale after back-translation. Third, a group of experts held several online meetings to compare and evaluate the differences between the original English version, the back-translated version, and the preliminary Chinese draft of the scale. Following these discussions, the Chinese draft was revised and improved to produce the final version. Subsequently, 30 undergraduate and graduate students from non-psychology fields were invited to review the Chinese version of the CAQ-8 for readability and clarity and to offer suggestions for refinement. The finalized Chinese version of the CAQ-8 was ultimately completed under the supervision of the corresponding author.
The Chinese version of the CAQ-8 retains the same items and scoring methods as the original version. The CAQ-8 consists of eight items that are categorized into positive and negative statements. For example, a positive statement is ‘I can remain committed to my goals even when there are times that I fail to reach them’, while a negative statement is ‘I find it difficult to carry on with an activity unless I experience that it is successful’. The questionnaire uses a 7-point scale ranging from 0 to 6 (0 = Never True, 6 = always True) to score each question. The four items 5, 6, 7, and 8 of the negative statements were reverse scored. The total score reflects the individual’s level of Committed Action.
Acceptance and action questionnaire–II (AAQ–II)-Chinese version
The Chinese version of the AAQ-II was used to assess individuals’ levels of experiential avoidance, comprises seven items [54]. The scale ranges from 1 to 7 (never to always), with cumulative scoring; higher scores denote greater levels of experiential avoidance. The scale has been widely used in the measurement of experiential avoidance among college students since its revision and has good applicability. The internal consistency Cronbach alpha coefficient of the scale in this study was 0.91.
Valuing questionnaire (VQ)-Chinese version
The Chinese version of the VQ was used [55], which demonstrates strong reliability and validity within the Chinese college student population. This questionnaire includes ten items across two dimensions, with a scoring range from 0 (not at all conforming) to 6 (fully conforming). Scores are cumulative, with higher totals reflecting greater awareness and enactment of personal values. The internal consistency, measured by Cronbach’s alpha, was 0.81 in this study.
Satisfaction with life scale (SWLS)-Chinese version
The Chinese version of the SWLS was revised into Chinese by Xiong et al. [56]. It has 5 items, with 7 levels of scoring from 1 to 7 (very non-conformity to very conformity), and the scores are cumulative, with the higher scores indicating the higher degree of subjective well-being of an individual, and has been widely used to measure the well-being of an individual since the revision of the scale. The scale has been widely used in the measurement of individual happiness index since its revision. In this study, the internal consistency Cronbach’s alpha coefficient of this scale was 0.88.
Depression anxiety stress scales (DASS-21)-Chinese version
The Chinese adaptation of the DASS-21, conducted by Gong et al. [57], serves as a tool to assess levels of depression, anxiety, and stress among individuals. Comprising 21 items distributed across three dimensions, this scale employs a four-point scoring system ranging from 0 (non-conformity) to 3 (always conformity), where higher scores indicate increased psychological distress. In this study, the Cronbach’s alpha coefficients for the overall scale and its subscales of depression, anxiety, and stress were found to be 0.94, 0.88, 0.84, and 0.85, respectively.
World health organization five-item well-being index (WHO-5)-Chinese version
The WHO-5 was refined for the assessment of individuals’ psychological well-being [58]. Participants completed the questionnaire based on their experiences over the past two weeks, responding to five questions with options ranging from 0 to 5 (none to all the time). The total score was calculated by summing the responses. The higher the total score, the more emotionally healthy they are. The internal consistency of the Cronbach’s alpha coefficient of the scale in this study was 0.93.
All items in the collected questionnaire were mandatory, hence, there were no missing values in this survey. First, the sample (n = 1635) was randomly divided into two sub-samples using SPSS 27.0 software’s random number generator. Second, Exploratory factor analysis was conducted on Sample 1 (n = 818); in Sample 2 (n = 817), confirmatory factor analysis was performed using Mplus 7.4 software with the maximum likelihood method. Then, a measurement equivalence test across genders was conducted in the total sample (n = 1635). finally, Pearson correlation analysis was used to test the criterion validity of CAQ-8 and the intraclass correlation coefficient (ICC) for test-retest reliability, and reliability tests were conducted using R version 4.0.5 with the “alpha” and “MBESS” packages to calculate Cronbach’s Alpha (α) and McDonald’s Omega (ω) coefficients [59]. The reference values for α and ω are as follows: below 0.50 (unacceptable), 0.50–0.60 (very poor), 0.60–0.70 (poor), 0.70–0.80 (acceptable), 0.80–0.90 (good), and above 0.90 (excellent).
Model fit was assessed using the Comparative Fit Index (CFI), Root Mean Square Error of Approximation (RMSEA), and Standardized Root Mean Square Residual (SRMR). Fit was evaluated against conventional benchmarks: a CFI of 0.90 or higher and RMSEA or SRMR values of 0.08 or lower indicate an acceptable model fit [60,61]. Additionally, if changes in ΔCFI (≤0.01) and ΔRMSEA (≤0.015) fell within acceptable thresholds [62], the simpler model was favored.
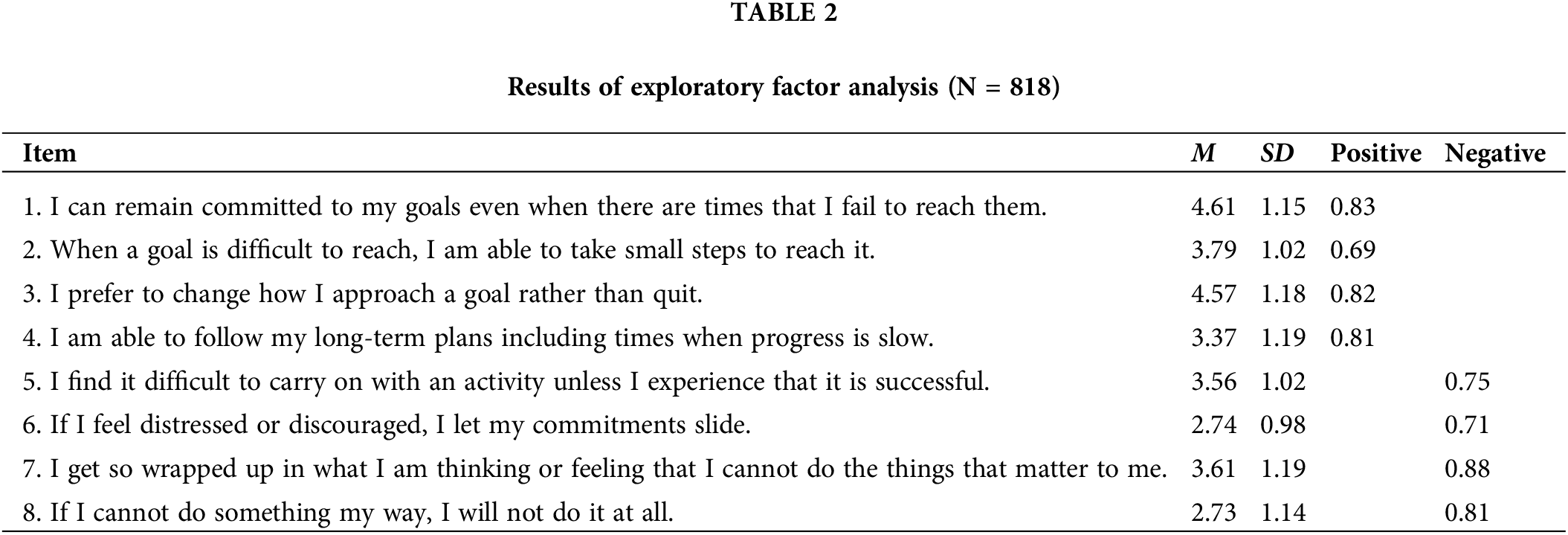
Exploratory factor analysis was conducted on sample 1 (n = 818). Firstly, a Kaiser-Meyer-Olkin (KMO) sample suitability test and Bartlett’s test of sphericity were performed, with KMO = 0.91, χ2 = 2624.92, and df = 19, indicating that the data were suitable for factor analysis. Principal component analysis and oblique rotation were used, and standard and gravel plots with eigenvalues greater than 1 showed that extracting two factors was appropriate, with a cumulative variance explained of 63.62%. Table 2 shows the factor loadings for each entry, which ranged from 0.69 to 0.88. Table 2 shows the factor loadings for each entry, which ranged from 0.69 to 0.88. We display only factor loadings above 0.5. Table 2 shows the factor loadings for each entry, which ranged from 0.69 to 0.88.
We used network analysis, an emerging research methodology that can provide new perspectives to demonstrate the relationship between scale structure and items, as shown in several studies, to identify the CAQ-8’s structure in a more subjective way [39–41]. Data from Sample 1 (n = 818) were included in the analytical plots, and Extended Bayesian Information criterium glasso (EBICglasso) regularization was used to estimate the sparse Gaussian plots using the EBICglasso regularization method. The network analysis plot showed two separate clusters, indicating a two-factor structure for CAQ-8, with items 1, 2, 3, and 4 as positive dimensions and items 5, 6, 7, and 8 as negative dimensions, consistent with the results of previous exploratory analyses. The network analysis diagram illustrates the relationships between the items, seen in Fig. 1. The strongest correlation was found between item 1 in CAQ-8 (I can remain committed to my goals even when there are times that I fail to reach them) and item 3 (I prefer to change how I approach a goal rather than quit) (0.38), as well as between item 7 (I get so wrapped up in what I am thinking or feeling that I cannot do the things that matter to me) and item 8 (If I cannot do something my way, I will not do it at all) (0.38). We developed a network centrality metrics graph to illustrate the relationship between the items in the CAQ-8. Fig. 2 shows that item 4 (I am able to follow my long-term plans including times when progress is slow) has the strongest intensity centrality and medium tightness centrality. The analysis shows that item 4, which measures the ability to carry out long-term plans, even if progress is slow, it is more central to the network. It has the most direct connections to other nodes in the network and maintains a high level of connectivity. The item 5 (I find it difficult to carry on with an activity unless I experience that it is successful) exhibits the strongest mediator centrality, measuring the difficulty of persisting in an activity unless perceived as successful. It plays a critical role in mediating and connecting the network, as indicated by its high score on this metric. The graph of the network centrality index shows that item 4 is the most central item on the scale, which warrants further analysis by psychological researchers. The global network stability analysis is displayed in Figs. 3 and 4. According to guidance on the Closeness Stability (CS) coefficient of strength centrality, the centrality index is considered robust if it is not less than 0.25 and preferably higher than 0.5 [63]. The global network CS of 0.517 for the CAQ-8 suggests that the centrality estimates are stable across the sample (Fig. 5).
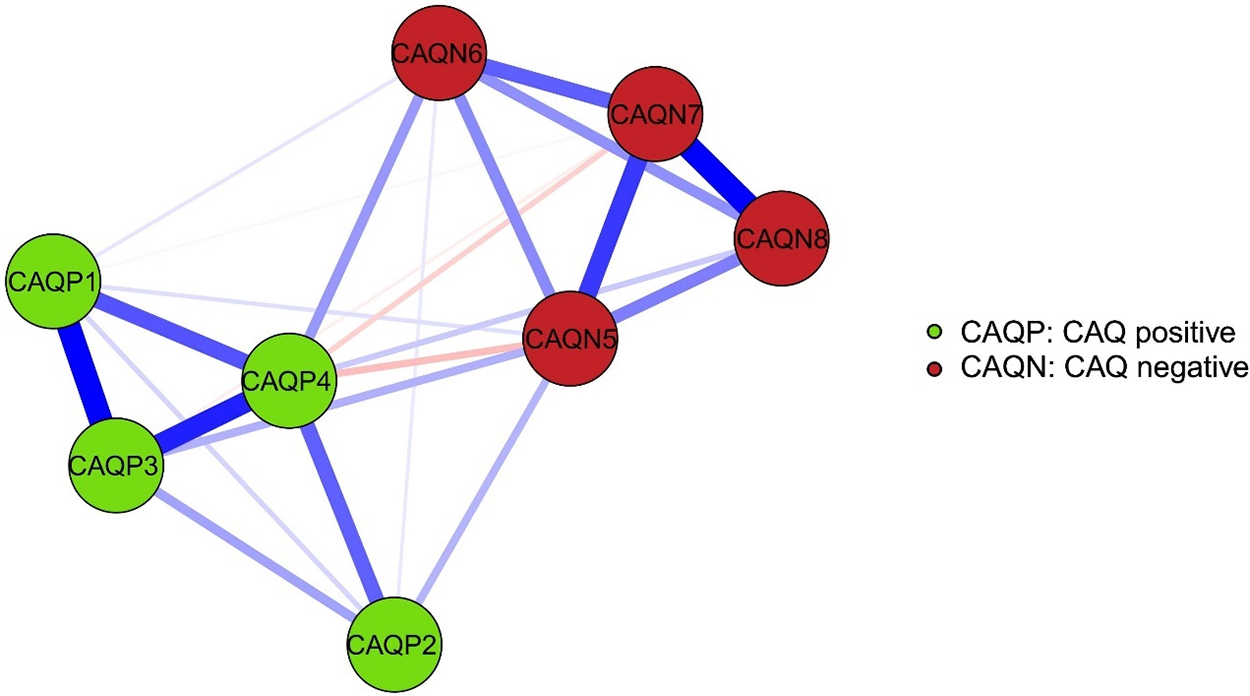
Figure 1: Sample 1 CFQ-8 network analysis graph.
Note: Each item of CFQ-8 as a node, the correlation between the nodes as a connecting line, the thickness of the connecting line represents the degree of correlation between the two nodes, the thicker the border line represents the higher the correlation. The colour is used to represent the correlation between the nodes, blue represents positive correlation and red represents negative correlation, to obtain the network analysis diagram Fig. 1.
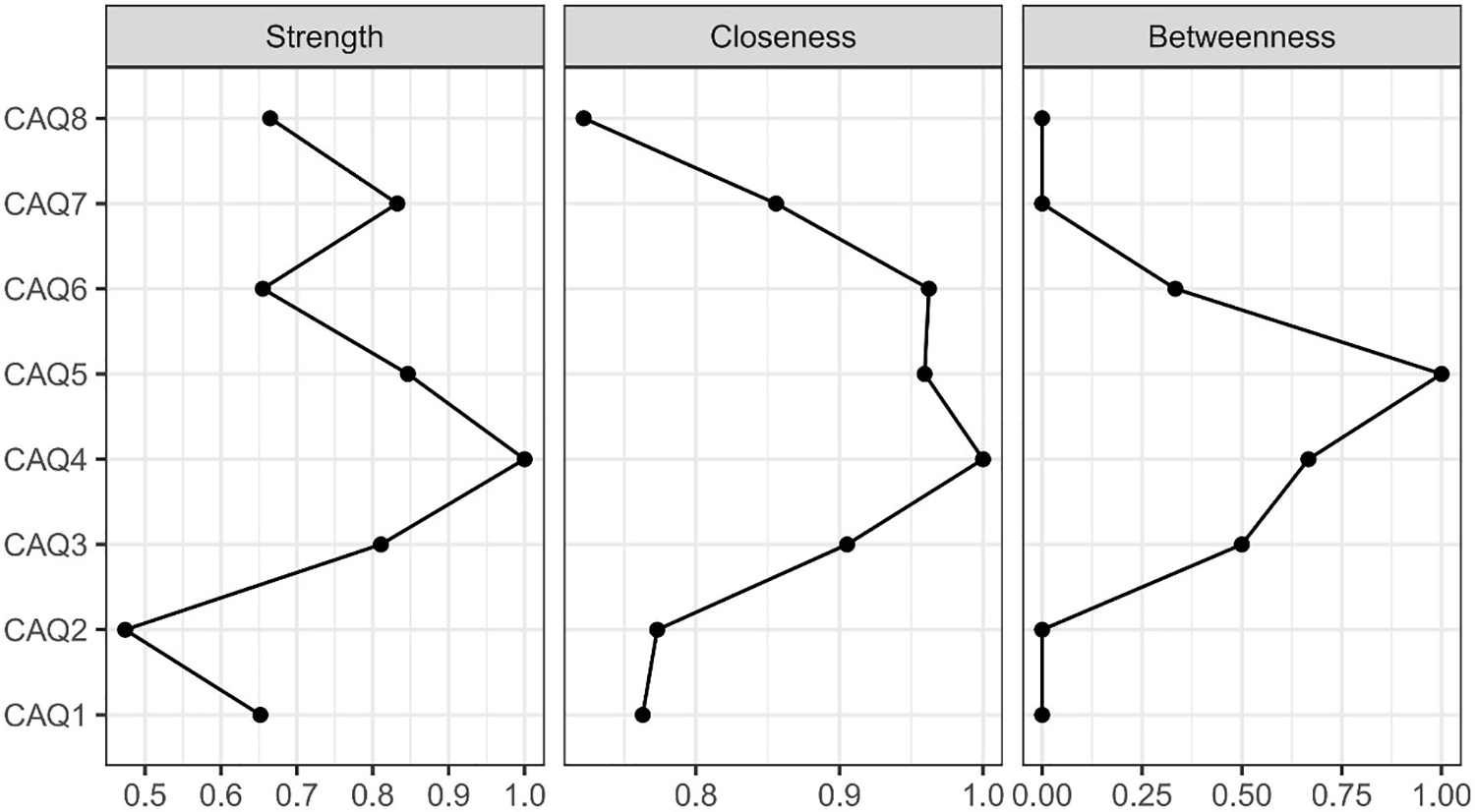
Figure 2: Sample 1 CAQ-8 centrality metrics graph.
Note: Strength centrality is the sum of a node’s direct connections to other nodes, indicating the node’s activity and influence in the network. Closeness centrality is the average distance between a node and all other nodes in the network. A node with high closeness centrality can influence other nodes in the network more quickly. Betweenness centrality is the frequency of occurrence of a node on all shortest paths in the network. A node with high betweenness centrality plays the role of a ‘bridge’ in the network, connecting nodes that are not directly connected.
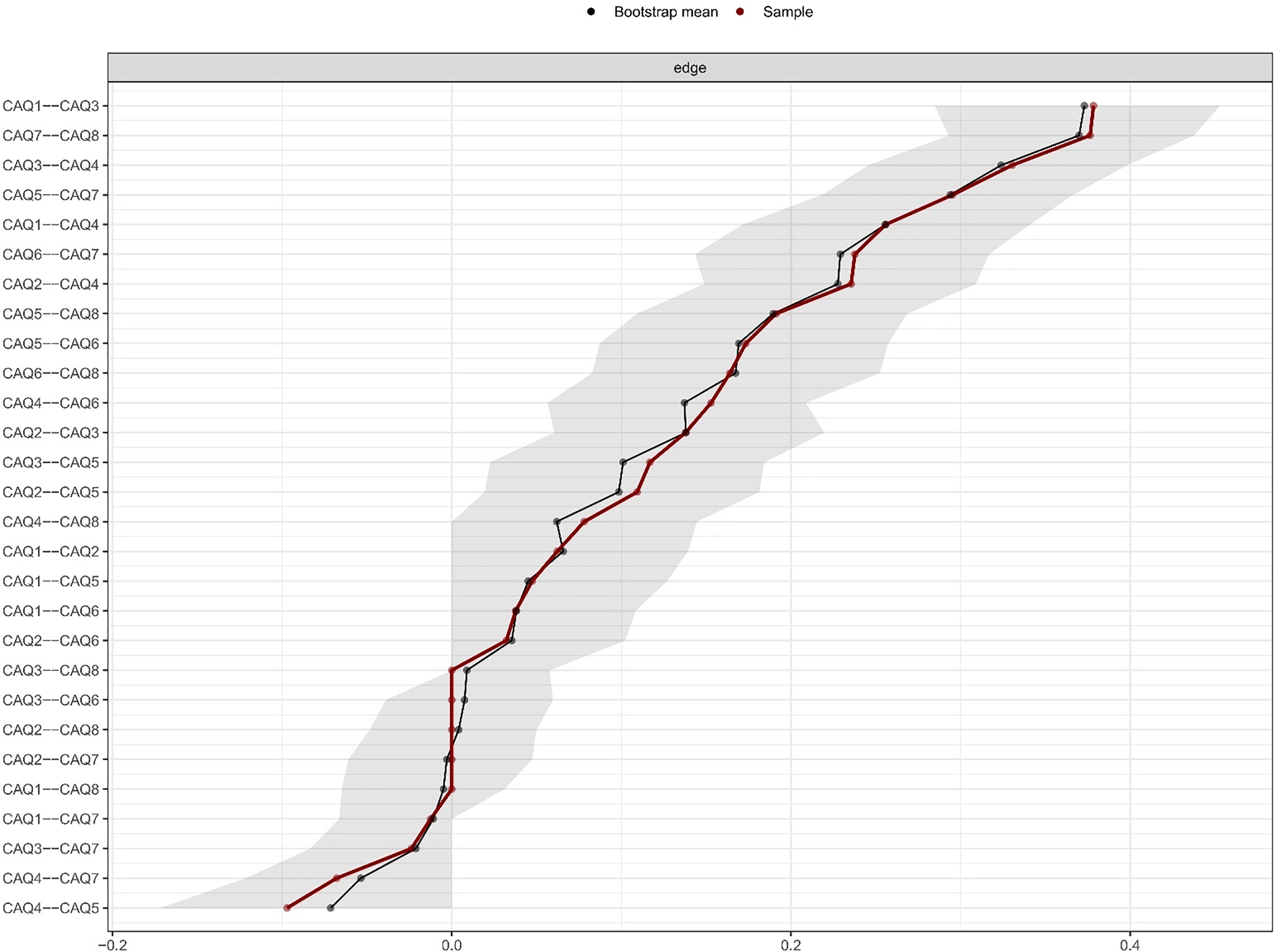
Figure 3: Bootstrapped edge weights for each pairwise node comparison.
Note: The black line represents the bootstrapped mean, the red line represents the point estimates of each edge weight, and the grey shading shows the edge weight at the 95% confidence interval.
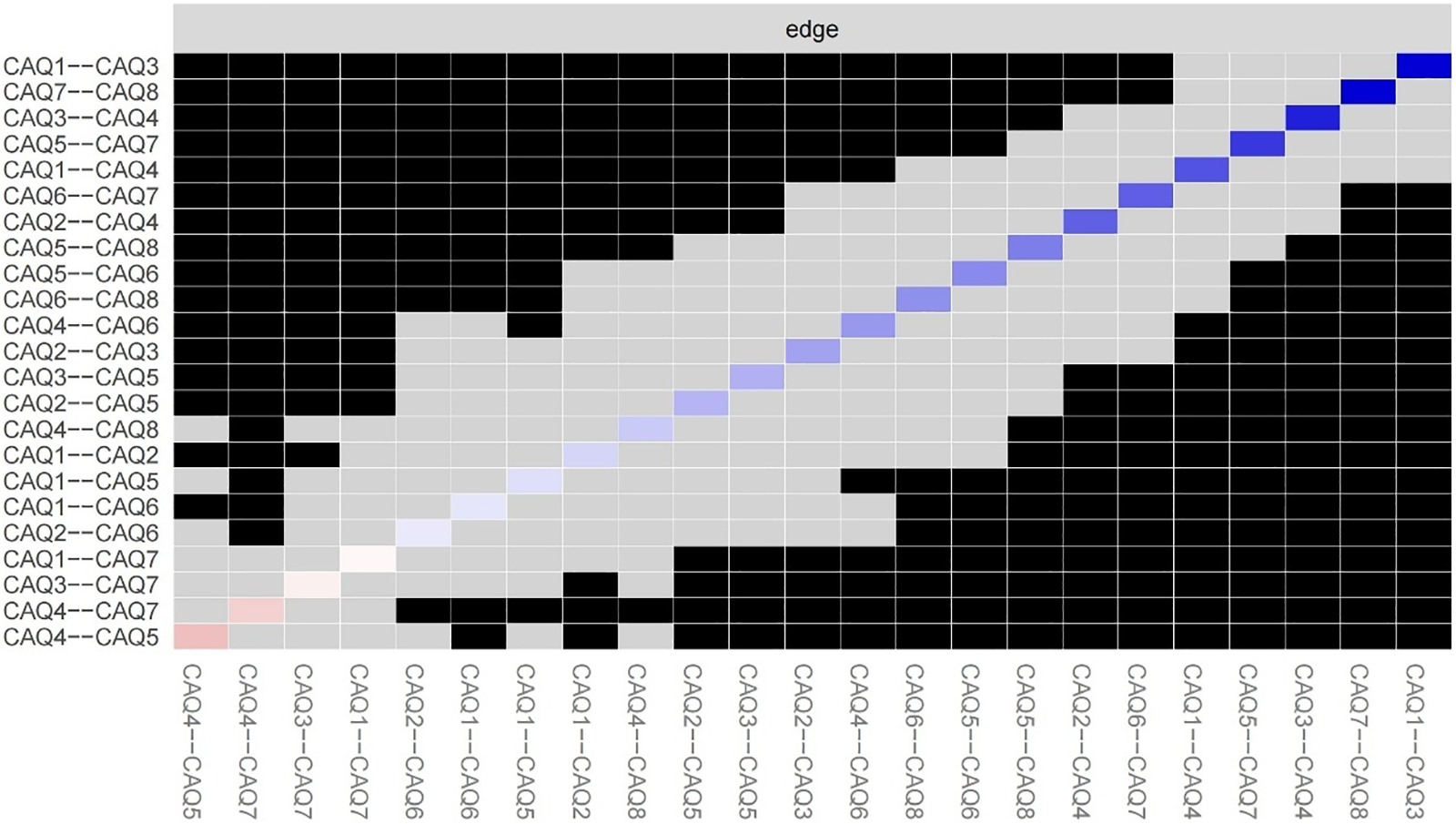
Figure 4: Bootstrapped difference test for edge weights.
Note: This test indicates the bootstrapped significance between pairwise edges in the global CAQ-8 network for each pairwise node comparison (α = 0.05). Significant differences are indicated by black boxes and nonsignificant differences by grey boxes, while the diagonal coloured boxes indicate the strength of the edge weight in the network plot (darker blue indicates stronger connection).
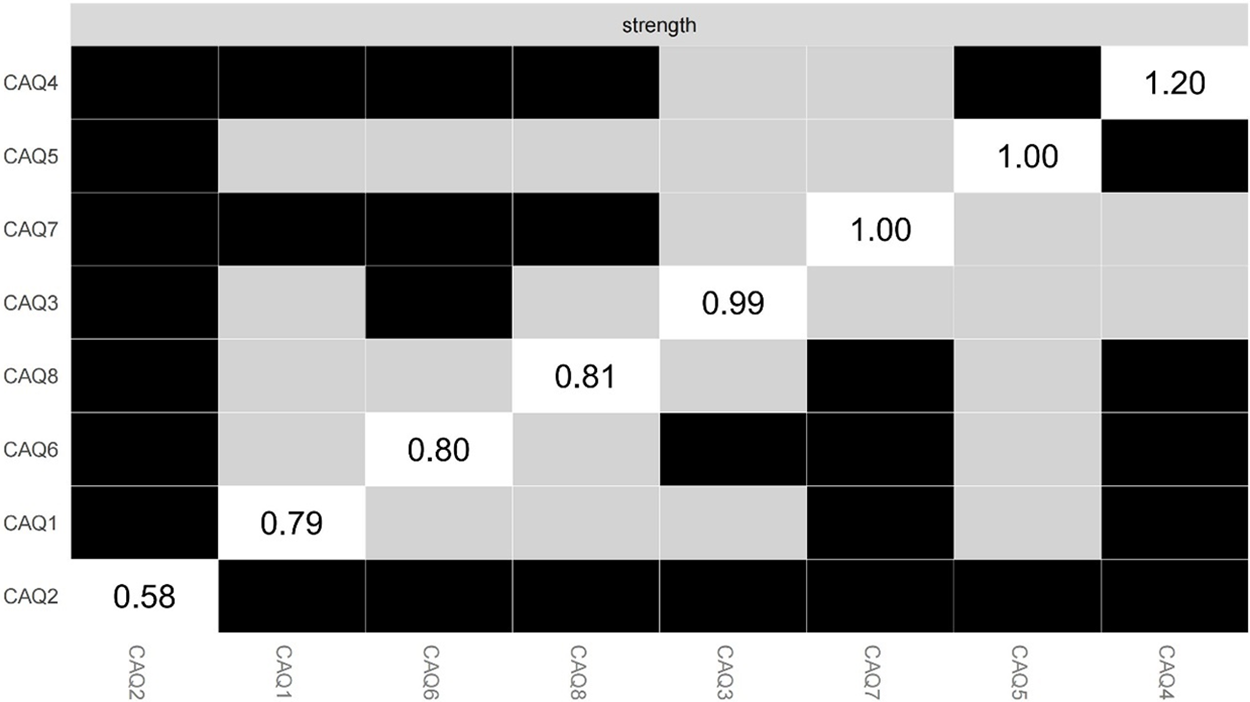
Figure 5: Bootstrap centrality difference test.
Note: This tests the bootstrap significance (α = 0.05) of the centrality estimates for each pairwise node comparison in the global CAQ-8 network. Black boxes indicate significant differences, grey boxes indicate non-significant differences, and diagonal boxes indicate node strength values.
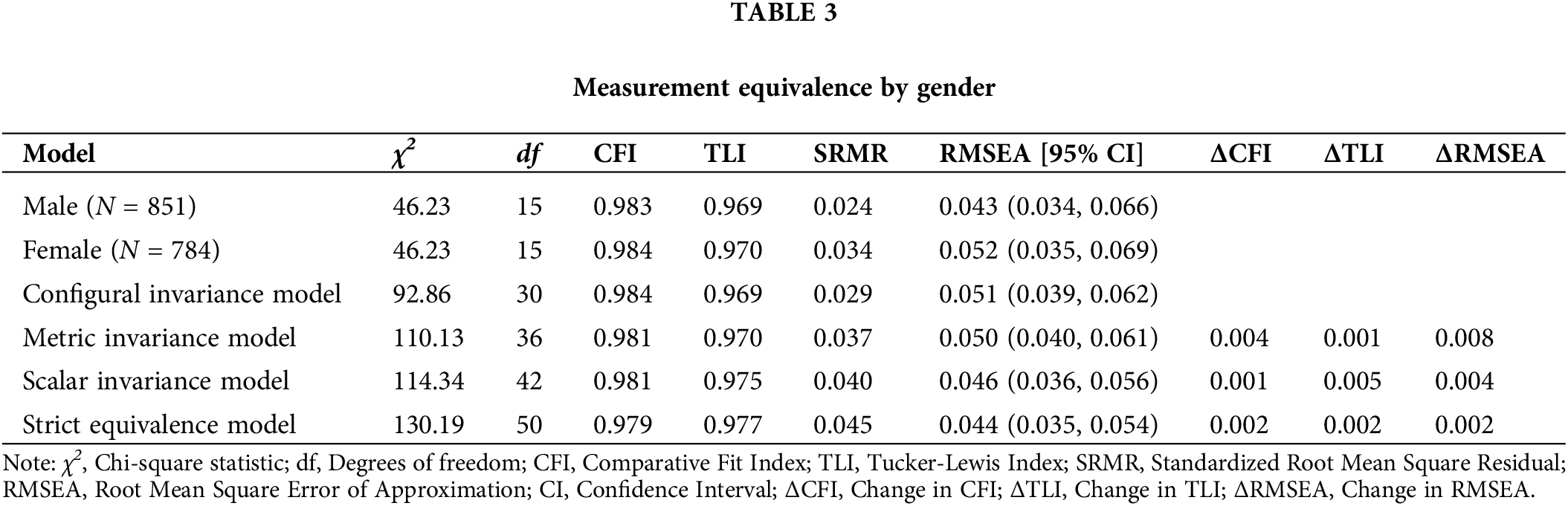
Validated factor analysis in sample two (N = 817) showed that the 2-factor model of CAQ-8 fitted well: χ2 = 46.23, df = 15, CFI = 0.990, TLI = 0.981, RMSEA = 0.040, RMSEA 95% CI ranged from 0.023 to 0.058, and SRMR = 0.024, indicating that the 2-factor model of CAQ-8 fitted the data well.
A measurement equivalence test was performed on the complete sample (n = 1635) to test whether CAQ-8 was equivalent between different genders (male/female), as described in Table 3. The configural invariance model test yielded an acceptable model fit, meeting the conditions for the subsequent equivalence analysis. Sequentially, factor loading equivalence (metric invariance model), indicator intercept equivalence (scalar invariance model), and error equivalence (strict equivalence model) was established based on the previous model. The study found that the CAQ-8 demonstrated strict equivalence across genders, as evidenced by the CFI, TLI, and RMSEA values being less than 0.01 for the configural invariance model, metric invariance model, scalar invariance model, and strict equivalence model. Therefore, the scale scores can be used to compare different groups, such as males and females.
Validity of validity scale correlation
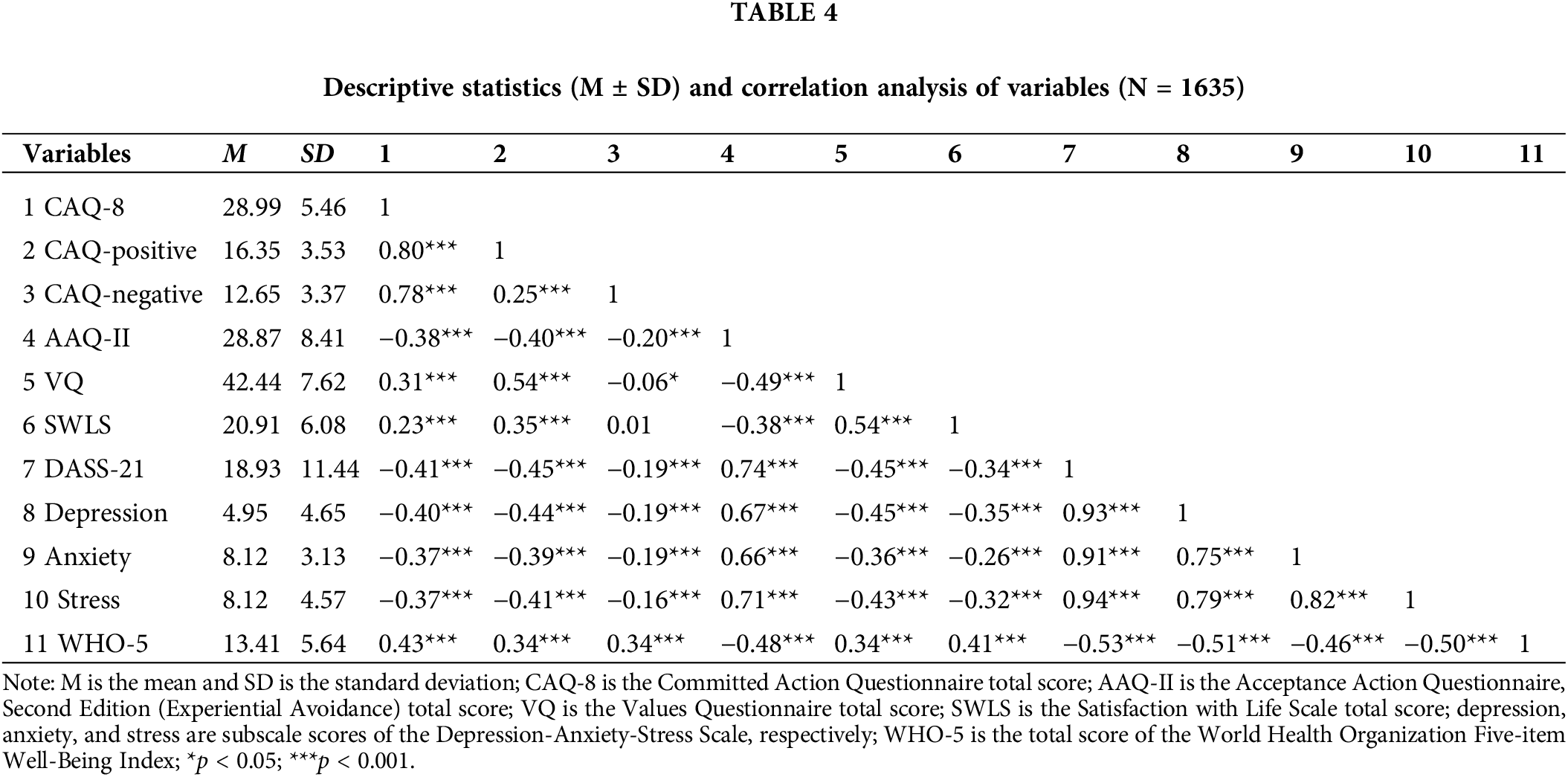
Table 4 shows the correlation coefficients between the Chinese version of the CAQ-8 and the total scores of the AAQ-II, VQ, SWLS, DASS-21, and WHO-5 scales. The CAQ-8 scores are significantly and positively correlated with values, life satisfaction, and physical and mental health. Additionally, they are significantly and negatively correlated with the level of experiential avoidance, depression, anxiety, and stress. The results indicate that the Chinese version of the CAQ-8 demonstrates good convergent validity.
To assess the validity of the validity scale correlation of the CAQ-8 scales, the relationships between the scales were further visualized using two network analysis diagrams (Fig. 6). Fig. 6A illustrates the relationship between the CAQ-8 scale and other mental health scales’ total scores. The diagram depicts the different scale total scores as nodes, with the strength and direction of the correlations between them indicated by the thickness and color of the connecting lines. The network analysis graph demonstrates the connections between the CAQ-8 scales and the SWLS, VQ, WHO-5, AAQ-II, and DASS-21 scales. The visual representation of the strength of positive and negative correlations confirms the convergent validity of the CAQ-8 in predicting and assessing mental health status. Fig. 6B displays a more detailed item-level network using the question scores for each scale as nodes. The figure shows that the questions in the CAQ-8 scale form distinct clusters within the network, indicating a high level of consistency within the scale and a strong correlation between the questions. Furthermore, the correlations between the CAQ-8 scale and other scale topics demonstrate its external validity in measuring mental health-related constructs.
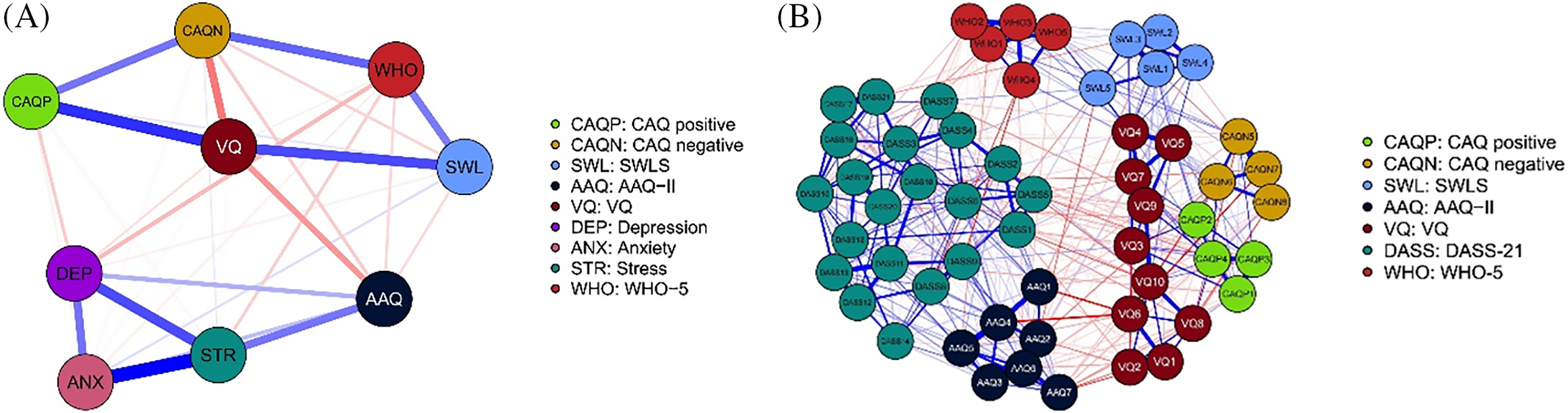
Figure 6: Network analysis diagrams. (A) The total scores of each scale for the CAQ-8. (B) Network analysis diagrams of the items of each scale.
Note: The network analysis diagrams provide a clear visual representation of the data. In the 6A, the nodes represent the total scores of each scale or subscale. In the 6B, the nodes represent all the items of each scale. The borderline represents the correlation of the nodes, with blue indicating a positive correlation and red indicating a negative correlation. The thickness of the border line represents the degree of correlation, with thicker lines indicating a stronger correlation. The correlation between variables is represented by the thickness of the borderline. A thicker line indicates a stronger correlation.
The reliability test results for the CAQ-8 were good. Cronbach’s α was 0.76 (95% CI: 0.75, 0.78) for the complete questionnaire, 0.76 (95% CI: 0.78, 0.80) for the positive subscales, and 0.78 (95% CI: 0.76, 0.79) for the negative subscales. McDonald’s ω was 0.75 (95% CI: 0.71, 0.79) for the complete questionnaire, 0.79 (95% CI: 0.77, 0.81) for the positive subscale, and 0.78 (95% CI: 0.76, 0.81) for the negative subscale. The full questionnaire retest reliability was found to be ICC = 0.70, 95% CI (0.64, 0.76). The retest reliability for the positive subscale was ICC = 0.69, 95% CI (0.62, 0.74), while for the negative subscale it was ICC = 0.73, 95% CI (0.67, 0.78).
Given the close relationship between levels of committed action and people’s mental health, it is particularly important to introduce and revise the short version of the CAQ-8, which has good reliability and validity in foreign populations. This study examined the reliability of the Chinese version of the CAQ-8 using a group of Chinese university students as subjects.
Exploratory factor analysis revealed a 2-factor structure for the CAQ-8, consistent with the original scale in both structure and content. This analysis indicated that the items could more accurately reflect the scale’s overall measurement intent. Furthermore, it demonstrated the scale’s ability to gauge individuals’ commitment to action from two distinct aspects. Additionally, this study tested the equivalence of the CAQ-8 across genders (male = 851; female = 784) using multi-group models (configural invariance model, metric invariance model, scalar invariance model, and strict equivalence model) based on validated factor analysis of the total sample (N = 1635). The results demonstrate the strict equivalence of the CAQ-8 across genders, making it a useful tool for comparing groups of different genders. The CAQ-8 scale’s validity analysis revealed significant positive correlations with positive indicators of individual mental health, such as life satisfaction and physical and mental health indicators. On the other hand, we observed significant negative correlations with negative indicators of individual mental health, such as depression, anxiety, and stress. Additionally, the CAQ-8 scale was significantly and negatively correlated with avoidance of experience in other processes of psychological flexibility and significantly and positively correlated with values clarification. These findings are in line with previous studies. This study found that the correlations between the CAQ-8 and negative indicators such as depression, anxiety, and stress were significantly weaker than those observed for the AAQ-II. This suggests a meaningful distinction between the two instruments: while the CAQ-8 focuses on measuring committed action—an essential component of psychological flexibility—the AAQ-II has been shown to primarily assess psychological distress rather than inflexibility itself [64,65]. The key advantage of the CAQ-8 lies in its specific focus on commitment to values-driven action, which is aligned with ACT principles. This enables the CAQ-8 to capture an individual’s proactive engagement with their goals, regardless of psychological distress. In contrast, the AAQ-II may inadvertently emphasize the experience of distress, potentially overshadowing the importance of committed action in promoting mental well-being. Thus, the CAQ-8 offers a nuanced approach that complements and expands upon the insights provided by the AAQ-II.
The reliability analysis study results indicate that the CAQ-8 scale has good internal consistency, high α, ω, and retest reliability, demonstrating its reliability and stability over time. The factor structure of the short version of the CAQ-8 tested in a population of Chinese university students was found to be consistent with the original scale, enhancing confidence in its multidimensional presentation. Besides, the graphical representations generated through network analysis provide a visual framework that enhances our understanding of the CAQ-8’s psychometric properties by illustrating the interconnectedness of different scales and items. This visualization allows researchers to identify not only the strength and direction of relationships but also to pinpoint core items, such as CAQ4, which is crucial for measuring committed action [66]. Moreover, these analyses contribute significantly to the overall validation of the CAQ-8 by demonstrating its convergent validity. By revealing how the CAQ-8 correlates with other established measures, such as the AAQ-II and VQ, the network analysis supports the notion that the CAQ-8 effectively captures the construct of committed action within the broader framework of psychological flexibility. This comprehensive understanding ultimately strengthens the argument for the CAQ-8’s utility as a reliable tool for assessing psychological constructs in both clinical and research settings.
The findings of this study enhance our theoretical understanding of committed action and its measurement within the context of Chinese university students. Validating the CAQ-8 in this population contributes to the literature on culturally tailored psychological assessment tools, enriching our comprehension of psychological constructs across diverse populations. Practically, the validated CAQ-8 provides a reliable and valid means of assessing committed action among Chinese university students, with implications for both research and clinical practice. In research, it enables investigation into the correlates and outcomes of committed action in this demographic, facilitating cross-cultural comparisons and advancing knowledge in the field. Clinically, the CAQ-8 serves as a valuable assessment tool for psychologists and counselors working with Chinese university students. By identifying individuals with low levels of committed action, practitioners can tailor interventions to enhance behavioral commitment and promote psychological well-being, potentially incorporating ACT techniques to foster greater committed action and resilience.
While our study has yielded valuable insights, several limitations should be acknowledged. Primarily, the sample predominantly comprised Chinese university students, potentially limiting the generalizability of our findings to broader populations. University students typically represent a unique demographic, often characterized by specific psychological traits and behavioral patterns that may differ from those observed in other age groups or populations. For instance, the experiences and coping strategies of university students might not be reflective of younger adolescents or older adults, who may face different life challenges and developmental concerns [67]. Consequently, the generalizability of our findings to broader populations—such as working professionals, older adults, or individuals from varying cultural backgrounds—requires cautious interpretation. Future research should aim to include more diverse samples to enhance the applicability of these findings across different demographic groups. Additionally, the reliance on self-reported measures introduces the possibility of subjective bias and memory distortion. Integrating objective physiological indicators or behavioral observations in subsequent research endeavors could bolster the reliability and validity of findings. Furthermore, the cross-sectional design employed in our study precludes causal inferences. Future inquiries employing longitudinal or experimental methodologies could offer deeper insights into the causal relationships between CAQ-8 and associated variables.
Moving forward, several avenues for future research can be identified. First, it would be beneficial to explore the role of the CAQ-8 in relation to various mental health issues, such as anxiety and depression. Understanding how committed action influences these conditions can provide valuable insights for therapeutic interventions. Cross-cultural comparative studies could elucidate the applicability and effectiveness of CAQ-8 across diverse cultural milieus, augmenting its cross-cultural utility and validity. Longitudinal investigations may delve into the enduring impact of CAQ-8 on individuals’ psychological well-being and behavioral tendencies, as well as its predictive capabilities concerning mental health outcomes. Intervention studies could assess the efficacy of behavior interventions or psychotherapeutic modalities in enhancing individuals’ psychological health, guided by CAQ-8 assessments. Additionally, endeavors to refine and enhance the measurement properties of CAQ-8, alongside the development of culturally sensitive iterations for diverse populations, could advance its utility in both research and practice domains. Exploring alternative applications of CAQ-8 in clinical diagnostics, psychological interventions, and organizational management could broaden its scope and relevance across various realms of mental health research and practice. Through these avenues of inquiry, a more comprehensive understanding of CAQ-8’s characteristics and applications can be attained, furnishing invaluable insights and support for mental health research and practice.
Based on a survey and analysis of 1635 samples, this study developed and validated Chinese CAQ-8 among university students. Both exploratory factor analysis and network analysis confirmed that CAQ-8 has a two-factor structure, aligning with the original scale’s content and intent. This indicates that the scale effectively captures individuals’ commitment to action from two distinct perspectives. Furthermore, the study demonstrated strict equivalence of the CAQ-8 across genders, making it a valuable tool for comparative research. The scale showed significant positive correlations with indicators of mental well-being, such as life satisfaction and overall health, while negatively correlating with markers of psychological distress like depression and anxiety. These findings highlight the CAQ-8’s unique focus on values-driven action, distinguishing it from instruments like the AAQ-II, which primarily assess psychological distress. Thus, the CAQ-8 provides a nuanced understanding of committed action, reinforcing its utility in promoting mental well-being.
Acknowledgement: The authors thank research participants for their participation in this study.
Funding Statement: This study was funded by the National Social Science Fund of China (grant number 23BSH132).
Author Contributions: Study conception and design: Haiyan Hu, Shuanghu Fang; data collection: Haiyan Hu, Shuanghu Fang; analysis and interpretation of results: Haiyan Hu, Shuanghu Fang, Qilin Zheng, Dongyan Ding; draft manuscript preparation: Haiyan Hu, Shuanghu Fang, Qilin Zheng, Dongyan Ding. All authors reviewed the results and approved the final version of the manuscript.
Availability of Data and Materials: The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval: All the methods were performed in accordance with the Declaration of Helsinki. The study was approved by the Ethical Committee of Anhui Normal University. All participants signed the informed consent in this study.
Conflicts of Interest: The authors declare no conflicts of interest to report regarding the present study.
References
1. Hayes SC, Strosahl KD, Strosahl K. A practical guide to acceptance and commitment therapy. New York: Springer Science & Business Media; 2004. [Google Scholar]
2. Hayes SC, Barnes-Holmes D, Wilson KG. Contextual behavioral science: creating a science more adequate to the challenge of the human condition. J Contextual Behav Sci. 2012;1:1–16. doi:10.1016/j.jcbs.2012.09.004. [Google Scholar] [CrossRef]
3. Zemestani M, Mozaffari S. Acceptance and commitment therapy for the treatment of depression in persons with physical disability: a randomized controlled trial. Clin Rehabil. 2020;34:938–47. doi:10.1177/0269215520923135. [Google Scholar] [PubMed] [CrossRef]
4. Schubert C, Hilbert S, Favreau M, Wolstein J, Voderholzer U. Psychological flexibility as a potential change factor in cognitive behavioural therapy of OCD. Behav Cogn Psychother. 2022;50:381–91. doi:10.1017/s1352465822000091. [Google Scholar] [PubMed] [CrossRef]
5. Gentili C, Rickardsson J, Zetterqvist V, Simons LE, Lekander M, Wicksell RK. Psychological flexibility as a resilience factor in individuals with chronic pain. Front Psychol. 2019;10:2016. doi:10.3389/fpsyg.2019.02016. [Google Scholar] [PubMed] [CrossRef]
6. Barke A, Riecke J, Rief W, Glombiewski JA. The Psychological Inflexibility in Pain Scale (PIPS)—validation, factor structure and comparison to the Chronic Pain Acceptance Questionnaire (CPAQ) and other validated measures in German chronic back pain patients. BMC Musculoskelet Disord. 2015;16:171. doi:10.1186/s12891-015-0641-z. [Google Scholar] [PubMed] [CrossRef]
7. Givehki R, Afshar H, Goli F, Scheidt CE, Omidi A, Davoudi M. Effect of acceptance and commitment therapy on body image flexibility and body awareness in patients with psychosomatic disorders: a randomized clinical trial. Electron Physician. 2018;10:7008–16. doi:10.19082/7008. [Google Scholar] [PubMed] [CrossRef]
8. Marshall EJ, Brockman RN. The relationships between psychological flexibility, self-compassion, and emotional well-being. J Cogn Psychother. 2016;30:60–72. doi:10.1891/0889-8391.30.1.60. [Google Scholar] [PubMed] [CrossRef]
9. Lucas JJ, Moore KA. Psychological flexibility: positive implications for mental health and life satisfaction. Health Promot Int. 2020;35:312–20. doi:10.1093/heapro/daz036. [Google Scholar] [PubMed] [CrossRef]
10. Fang S, Ding D. A meta-analysis of the efficacy of acceptance and commitment therapy for children. J Contextual Behav Sci. 2020;15:225–34. doi:10.1016/j.jcbs.2020.01.007. [Google Scholar] [CrossRef]
11. Uddin LQ. Cognitive and behavioural flexibility: neural mechanisms and clinical considerations. Nat Rev Neurosci. 2021;22:167–79. doi:10.1038/s41583-021-00428-w. [Google Scholar] [PubMed] [CrossRef]
12. Tindle R, Hemi A, Moustafa AA. Social support, psychological flexibility and coping mediate the association between COVID-19 related stress exposure and psychological distress. Sci Rep. 2022;12:8688. doi:10.1038/s41598-022-12262-w. [Google Scholar] [PubMed] [CrossRef]
13. Plys E, Jacobs ML, Allen RS, Arch JJ. Psychological flexibility in older adulthood: a scoping review. Aging Mental Health. 2023;27:453–65. doi:10.1080/13607863.2022.2036948. [Google Scholar] [PubMed] [CrossRef]
14. Kashdan TB, Rottenberg J. Psychological flexibility as a fundamental aspect of health. Clin Psychol Rev. 2010;30:865–78. [Google Scholar] [PubMed]
15. Baer RA. Mindfulness training as a clinical intervention: a conceptual and empirical review. Clin Psychol: Sci Pract. 2003;10:125–43. [Google Scholar]
16. Hayes SC, Luoma JB, Bond FW, Masuda A, Lillis J. Acceptance and commitment therapy: model, processes and outcomes. Behav Res Ther. 2006;44:1–25. doi:10.1016/j.brat.2005.06.006. [Google Scholar] [PubMed] [CrossRef]
17. Fang S, Ding D. Which outcome variables are associated with psychological inflexibility/flexibility for chronic pain patients? A three level meta-analysis. Front Psychol. 2022;13:1069748. doi:10.3389/fpsyg.2022.1069748. [Google Scholar] [PubMed] [CrossRef]
18. Hayes SC. Acceptance and commitment therapy: towards a unified model of behavior change. World Psychiat. 2019;18:226–7. doi:10.1002/wps.20626. [Google Scholar] [PubMed] [CrossRef]
19. Hayes SC. Constructing a liberated and modern mind: six pathways from pathology to euthymia. World Psychiat. 2020;19:51–2. doi:10.1002/wps.20715. [Google Scholar] [PubMed] [CrossRef]
20. McCracken LM, Chilcot J, Norton S. Further development in the assessment of psychological flexibility: a shortened Committed Action Questionnaire (CAQ-8). Eur J Pain. 2015;19:677–85. doi:10.1002/ejp.589. [Google Scholar] [PubMed] [CrossRef]
21. McCracken LM. Committed action: an application of the psychological flexibility model to activity patterns in chronic pain. J Pain. 2013;14:828–35. doi:10.1016/j.jpain.2013.02.009. [Google Scholar] [PubMed] [CrossRef]
22. Michelson SE, Lee JK, Orsillo SM, Roemer L. The role of values-consistent behavior in generalized anxiety disorder. Depress Anxiety. 2011;28:358–66. doi:10.1002/da.20793. [Google Scholar] [PubMed] [CrossRef]
23. Trompetter HR, Ten Klooster PM, Schreurs KM, Fledderus M, Westerhof GJ, Bohlmeijer ET. Measuring values and committed action with the engaged living scale (ELSpsychometric evaluation in a nonclinical sample and a chronic pain sample. Psychol Assess. 2013;4:1235–46. doi:10.1037/a0033813. [Google Scholar] [PubMed] [CrossRef]
24. Hayes SC, Strosahl KD, Wilson KG. Acceptance and commitment therapy: the process and practice of mindful change. 2nd ed. New York: Guilford Press; 2012. [Google Scholar]
25. Bond FW, Hayes SC, Baer RA, Carpenter KM, Guenole N, Orcutt HK, et al. Preliminary psychometric properties of the acceptance and action questionnaire-II: a revised measure of psychological inflexibility and experiential avoidance. Behav Ther. 2011;42:676–88. doi:10.1016/j.beth.2011.03.007. [Google Scholar] [PubMed] [CrossRef]
26. Greco LA, Lambert W, Baer RA. Psychological inflexibility in childhood and adolescence: development and evaluation of the avoidance and fusion questionnaire for youth. Psychol Assess. 2008;20:93–102. doi:10.1037/1040-3590.20.2.93. [Google Scholar] [PubMed] [CrossRef]
27. Deng YQ, Li S, Tang YY. Psychometric properties of the Chinese translation of the Mindful Attention Awareness Scale (MAAS). Mindfulness. 2012;3:10–4. doi:10.1007/s12671-011-0074-1. [Google Scholar] [CrossRef]
28. Gámez W, Chmielewski M, Kotov R, Ruggero C, Suzuki N, Watson D. The brief experiential avoidance questionnaire: development and initial validation. Psychol Assess. 2014;26:35–45. doi:10.1037/a0034473. [Google Scholar] [PubMed] [CrossRef]
29. Terhorst Y, Baumeister H, McCracken LM, Lin J. Further development in the assessment of psychological flexibility: validation of the German committed action questionnaire. Health Qual Life Outcomes. 2020;18:260. doi:10.1186/s12955-020-01497-8. [Google Scholar] [PubMed] [CrossRef]
30. Trindade IA, Marta-Simões J, Ferreira C, Pinto-Gouveia J. Developments on committed action: validity of the CAQ-8 and analysis of committed action’s role in depressive symptomatology in breast cancer patients and healthy individuals. Clin Psychol Psychother. 2018;25:e42–50. doi:10.1002/cpp.2125. [Google Scholar] [PubMed] [CrossRef]
31. Rodrigues TF, Vieira AI, Vaz AR, Brandão I, Timóteo S, Nunes P, et al. The factorial structure and psychometric properties of the Committed Action Questionnaire (CAQ-8) in a Portuguese clinical sample with eating disorders. Clin Psychol Psychother. 2021;29:222–9. doi:10.1002/cpp.2621. [Google Scholar] [PubMed] [CrossRef]
32. Cheng C, Wang F, Golden DL. Unpacking cultural differences in interpersonal flexibility: role of culture-related personality and situational factors. J Cross Cult Psychol. 2011;42:425–44. doi:10.1177/0022022110362755. [Google Scholar] [CrossRef]
33. Xiang P, Zhang H, Geng L, Zhou K, Wu Y. Individualist-collectivist differences in climate change inaction: the role of perceived intractability. Front Psychol. 2019;10:752. doi:10.3389/fpsyg.2019.00187. [Google Scholar] [PubMed] [CrossRef]
34. Hofstede G. Culture’s consequences: comparing values, behaviors, institutions and organisations across nations. Australian J Manage. 2001;27:89–94. doi:10.1177/031289620202700105. [Google Scholar] [CrossRef]
35. Drake CE, Masuda A, Dalsky D, Stevens KT, Kramer S, Primeaux SJ, et al. Examining U.S. and Japanese College Students’ differences in psychological distress: the mediating roles of valued action and experiential avoidance. Int J Adv Counsel. 2019;41:25–40. doi:10.1007/s10447-018-9342-2. [Google Scholar] [CrossRef]
36. Lu L, Gilmour R. Culture and conceptions of happiness: individual oriented and social oriented SWB. J Happiness Stud. 2004;5:269. doi:10.1007/s10902-004-8789-5. [Google Scholar] [CrossRef]
37. Wong W-S, McCracken L, Wong S, Chen P-P, Chow Y-F, Fielding R. The Chinese version of the 8-item Committed Action Questionnaire (ChCAQ-8a preliminary analysis of the factorial and criterion validity. Psychol Assess. 2016;28:e111–8. doi:10.1037/pas0000187. [Google Scholar] [PubMed] [CrossRef]
38. Li Y, Yang FL, Pan C, Chu QQ, Tang QP. Validation of the committed action questionnaire-8 and its mediating role between experiential avoidance and life satisfaction among chinese university students. Front Psychol. 2021;12:655518. doi:10.3389/fpsyg.2021.655518. [Google Scholar] [PubMed] [CrossRef]
39. Borsboom D, Cramer AOJ. Network analysis: an integrative approach to the structure of psychopathology. Annu Rev Clin Psychol. 2013;9:91–121. doi:10.1146/annurev-clinpsy-050212-185608. [Google Scholar] [PubMed] [CrossRef]
40. Epskamp S, Cramer AOJ, Waldorp LJ, Schmittmann VD, Borsboom D. qgraph: network visualizations of relationships in psychometric data. J Stat Softw. 2012;48:1–18. doi:10.18637/jss.v048.i04. [Google Scholar] [CrossRef]
41. Janková J, Van de Geer S. Inference in high-dimensional graphical models; 2018. doi: 10.48550/arXiv.1801.08512. [Google Scholar] [CrossRef]
42. Schmittmann VD, Cramer AOJ, Waldorp LJ, Epskamp S, Kievit RA, Borsboom D. Deconstructing the construct: a network perspective on psychological phenomena. New Ideas Psychol. 2013;31:43–53. doi:10.1016/j.newideapsych.2011.02.007. [Google Scholar] [CrossRef]
43. Costantini G, Richetin J, Borsboom D, Fried EI, Rhemtulla M, Perugini M. Development of indirect measures of conscientiousness: combining a facets approach and network analysis. Eur J Pers. 2015;29:548–67. doi:10.1002/per.2014. [Google Scholar] [CrossRef]
44. Beck ED, Jackson JJ. Network approaches to representing and understanding personality dynamics. In: Wood D, Read SJ, Harms PD, Slaughter A, editors. Measuring and modeling persons and situations. San Diego, CA, USA: Academic Press; 2021. p. 465–97. [Google Scholar]
45. Lange J, Dalege J, Borsboom D, Van Kleef GA, Fischer AH. Toward an integrative psychometric model of emotions. Perspect Psychol Sci. 2020;15:444–68. doi:10.1177/1745691619895057. [Google Scholar] [PubMed] [CrossRef]
46. Briganti G, Kempenaers C, Braun S, Fried EI, Linkowski P. Network analysis of empathy items from the interpersonal reactivity index in 1973 young adults. Psychiat Res. 2018;265:87–92. doi:10.1016/j.psychres.2018.03.082. [Google Scholar] [PubMed] [CrossRef]
47. Contreras A, Nieto I, Valiente C, Espinosa R, Vazquez C. The study of psychopathology from the network analysis perspective: a systematic review. Psychother Psychosom. 2019;88:71–83. doi:10.1159/000497425. [Google Scholar] [PubMed] [CrossRef]
48. Govorova E, Benítez I, Muñiz J. Predicting student well-being: network analysis based on PISA 2018. Int J Environ Res Public Health. 2020;17:4014. doi:10.3390/ijerph17114014. [Google Scholar] [PubMed] [CrossRef]
49. Svicher A, Gori A, Di Fabio A. The sustainable development goals psychological inventory: a network analysis in italian university students. Int J Environ Res Public Health. 2022;19:10675. doi:10.3390/ijerph191710675. [Google Scholar] [PubMed] [CrossRef]
50. Song Z, Ye J, Song X, Zhang Z, Xu P, Shen H. Development and psychometric properties of work information anxiety questionnaire. Psychol Res Behav Manage. 2023;16:4629–46. doi:10.2147/PRBM.S435356. [Google Scholar] [PubMed] [CrossRef]
51. Van Zyl CJ. A network analysis of the general health questionnaire. J Health Psychol. 2021;26:249–59. doi:10.1177/1359105318810113. [Google Scholar] [PubMed] [CrossRef]
52. Borsboom D. A network theory of mental disorders. World Psychiat. 2017;16:5–13. doi:10.1002/wps.20375. [Google Scholar] [PubMed] [CrossRef]
53. Faul F, Erdfelder E, Lang A-G, Buchner A. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007;39:175–91. doi:10.3758/bf03193146. [Google Scholar] [PubMed] [CrossRef]
54. Cao J, Ji Y, Zhu Z. Reliability and validity of the Chinese version of the Acceptance and Action Questionnaire-Second Edition (AAQ-II) in college students. Chin Mental Health J. 2013;27:873–7. doi:10.3969/j.issn.1000-6729.2013.11.014. [Google Scholar] [CrossRef]
55. Bi D, Ding Q, Zhang J, Chen J, Li X. Validity and reliability test of Chinese version of value assessment questionnaire in college students. Chin J Mental Health. 2021;35:417–22 (In Chinese). doi:10.3969/j.issn.1000-6729.2021.05.011. [Google Scholar] [CrossRef]
56. Xiong C, Xu Y. Reliability and validity of the stisfaction with life scale for Chinese demos. China J Health Psychol. 2009;17:948–9 (In Chinese). doi:10.13342/j.cnki.cjhp.2009.08.026. [Google Scholar] [CrossRef]
57. Gong X, Xie X-Y, Rui X, Yue-Jia L. Psychometric properties of the Chinese versions of DASS-21 in Chinese college students. Chinese J Clin Psychol. 2010;18:443–7 (In Chinese). doi:10.16128/j.cnki.1005-3611.2010.04.020. [Google Scholar] [CrossRef]
58. Wang Z, Bian Q. Validity and reliability of the world health organization five-item well-being index in identifying depression among high school students. Chin J Mental Health. 2011;25:279–83 (In Chinese). [Google Scholar]
59. R Core Team. R: a language and environment for statistical computing; 2016. Available from: https://www.r-project.org/. [Accessed 2024]. [Google Scholar]
60. Byrne BM. Structural equation modeling with Mplus: basic concepts, applications, and programming. New York: Routledge; 2013. [Google Scholar]
61. Marsh HW, Hau K-T, Wen Z. In search of golden rules: comment on hypothesis-testing approaches to setting cutoff values for fit indexes and dangers in overgeneralizing Hu and Bentler’s, 1999 findings. Struct Equ Modeling. 2004;11:320–41. doi:10.1207/s15328007sem1103_2. [Google Scholar] [CrossRef]
62. Chen FF. Sensitivity of goodness of fit indexes to lack of measurement invariance. Struct Eq Model. 2007;14:464–504. doi:10.1080/10705510701301834. [Google Scholar] [CrossRef]
63. Stochl J, Soneson E, Wagner AP, Khandaker GM, Goodyer I, Jones PB. Identifying key targets for interventions to improve psychological wellbeing: replicable results from four UK cohorts. Psychol Med. 2019;49:2389–96. doi:10.1017/S0033291718003288. [Google Scholar] [PubMed] [CrossRef]
64. Kashdan TB, Disabato DJ, Goodman FR, Doorley JD, McKnight PE. Understanding psychological flexibility: a multimethod exploration of pursuing valued goals despite the presence of distress. Psychol Assess. 2020;32:829–50. doi:10.1037/pas0000834. [Google Scholar] [PubMed] [CrossRef]
65. Ong CW, Pierce BG, Petersen JM, Barney JL, Fruge JE, Levin ME, et al. A psychometric comparison of psychological inflexibility measures: discriminant validity and item performance. J Contextual Behav Sci. 2020;18:34–47. doi:10.1016/j.jcbs.2020.08.007. [Google Scholar] [CrossRef]
66. Golino H, Shi D, Christensen AP, Garrido LE, Nieto MD, Sadana R, et al. Investigating the performance of exploratory graph analysis and traditional techniques to identify the number of latent factors: a simulation and tutorial. Psychol Methods. 2020;25:292–320. doi:10.1037/met0000255. [Google Scholar] [PubMed] [CrossRef]
67. Arnett JJ. Emerging adulthood: a theory of development from the late teens through the twenties. Am Psychol. 2000;55:469–80. doi:10.1037/0003-066X.55.5.469. [Google Scholar] [CrossRef]
Cite This Article
 Copyright © 2025 The Author(s). Published by Tech Science Press.
Copyright © 2025 The Author(s). Published by Tech Science Press.This work is licensed under a Creative Commons Attribution 4.0 International License , which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
 Downloads
Downloads
 Citation Tools
Citation Tools