
 Submit a Paper
Submit a Paper Propose a Special lssue
Propose a Special lssue Open Access
Open Access
ARTICLE

Mechanisms and Heterogeneous Effects of Physical Activity on Mental Health: Evidence from the China Family Panel Studies
1 Department of Economics, University of Colorado Denver, Denver, CO 80217-3364, USA
2 International College Beijing, China Agricultural University, Beijing, 100083, China
* Corresponding Author: Chun-Chieh Hu. Email:
(This article belongs to the Special Issue: The Mind in Motion: Exploring Consumer Psychology for Mental Health, Well-being, and Sustainable Sport Futures)
International Journal of Mental Health Promotion 2026, 28(2), 6 https://doi.org/10.32604/ijmhp.2025.073744
Received 24 September 2025; Accepted 15 December 2025; Issue published 27 February 2026
 View Full Text
View Full Text Download PDF
Download PDFAbstract
Objectives: In recent years, mental health has emerged as a pressing public health concern in China, driven by mounting societal pressures and fast-paced urban lifestyles. Physical activity, a well-established means of enhancing psychological well-being, has received growing scholarly and policy attention. This study uses panel data from the 2020 and 2022 waves of the China Family Panel Studies (CFPS) to examine the impact of exercise frequency on mental health (with indicators such as CESD-8 depression scores) among college students and young employees, thereby providing empirical support for targeted mental health interventions. Methods: This study examines the relationship between individual exercise frequency and mental health among college students and young employees, using panel data from the 2020 and 2022 waves of the China Family Panel Studies (CFPS), with the Chinese version of the 8-item Center for Epidemiologic Studies Depression Scale (CESD-8) depression scores, self-rated health, and life satisfaction as outcome variables. Specifically, this study tests three hypotheses: (H1) increased exercise frequency significantly reduces depression symptoms and enhances well-being; (H2) the effects of exercise vary by social roles, with stronger mental health benefits among employed individuals and those with lower education; and (H3) lifestyle factors such as smoking amount, sleep duration, and Body Mass Index (BMI) partially mediate the relationship between exercise and mental health. Employing a two-way fixed effects model, baseline results indicate that a one-unit increase in exercise frequency significantly reduces the CESD-8 score by 0.183 points. To address potential endogeneity and spurious regression concerns, an instrumental variable (IV) approach is further applied. The heterogeneity analysis differentiates between students and employed individuals. Results: Among students, the effects of exercise on mental health are not statistically significant, regardless of education level. In contrast, for the employed, exercise demonstrates a significant positive impact on mental health, with particularly pronounced effects among those with lower educational attainment. These findings underscore the importance of promoting exercise as part of comprehensive mental health strategies. Mediation analysis indicates that the beneficial effect of exercise on mental health is partially transmitted through reductions in adverse health behaviors, especially smoking. Conclusions: Policymakers should integrate physical activity promotion into health interventions, prioritizing vulnerable groups to enhance psychological resilience and foster inclusive, health-oriented development.Keywords
In recent years, mental health has gained increasing attention, especially since the outbreak of COVID-19 in 2019. Beyond its physical and economic impacts, the pandemic has triggered widespread psychological distress. Studies show a significant rise in mental health problems such as depression, anxiety, stress, and insomnia. Hossain et al. found that people affected by COVID-19 often suffer from emotional disturbance, panic attacks, and even suicidal behavior [1,2,3]. These issues are linked to factors like age, health status, media exposure, and lack of support. Wu et al. [4] further revealed that around one-third of people experienced depression or anxiety during the pandemic, with higher risks among patients, the quarantined, and those with chronic illness. Social isolation also worsens mental well-being, especially for the elderly and children [5,6,7,8]. Beyond the general population, recent evidence shows that among 18,629 freshmen at a university in Chengdu from 2020 to 2023, the prevalence of depression averaged 30.39%, with academic and employment pressures identified as significant contributing factors [9]. At the same time, intensified job market competition in China has pushed many recent graduates to pursue further education, while youth unemployment rates exceeding 20% have created substantial psychological stress for the newly employed [10]. Altogether, these findings suggest a “mental health crisis” running parallel to the pandemic, with young people and students representing high-risk groups, calling for urgent attention.
Existing studies generally support the idea that physical activity improves mental health. AL Mutlaqah [11] found that both aerobic and resistance exercises are linked to reduced symptoms of depression, anxiety, and Post-traumatic stress disorder (PTSD) [12,13], largely through neurobiological and behavioral mechanisms. Similarly, Pujari [14] emphasized that physical activity enhances mood and emotional well-being by improving blood flow and reducing oxidative stress. Kpame and Richard [15] also showed that moderate aerobic exercise, such as walking and cycling, is associated with better self-esteem and lower depressive symptoms. However, these studies mainly rely on theoretical discussion, lacking empirical evidence on real-world outcomes—highlighting a gap this study aims to address. Although most of these studies are theoretical, some empirical research has also provided evidence for the mental-health benefits of exercise. For instance, Sharma et al. [16] reviewed clinical observations suggesting that moderate aerobic activity effectively reduces anxiety and depressive symptoms. However, though these reaserches, supportive of the positive association between exercise and mental health, they rely on dated or cross-sectional data and lack rigorous tests for endogeneity and causal mechanisms, highlighting the need for updated panel-based evidence.
This paper investigates the causal effect of exercise frequency on mental health outcomes using nationally representative panel data from the China Family Panel Studies (CFPS) in 2020 and 2022 [17]. We adopt a comprehensive empirical strategy that combines two-way fixed effects models, instrumental variable (IV) estimation, and heterogeneity analysis to validate the robustness and mechanisms of the observed relationship. Depression scores (CESD-8), self-rated health, and life satisfaction serve as the primary measures of psychological well-being. The baseline results from the fixed effects model suggest that increased exercise frequency significantly alleviates depression symptoms. To address potential endogeneity caused by reverse causality or omitted variable bias, we employ two exogenous instruments—urban green space per capita and the number of extreme temperature days. Heterogeneity analysis further demonstrates that the psychological benefits of physical activity are more pronounced among employed individuals and those with lower educational attainment, while students and highly educated individuals experience smaller gains. These empirical strategies collectively confirm both the effectiveness and transmission channels of physical activity in improving mental well-being. We also employed smoking, sleep, and BMI as mediating variables, and the results confirmed the mediating effect of daily cigarette consumption on exercise and mental health.
The remainder of this paper is organized as follows. Section 2 reviews the relevant theoretical background. Section 3 introduces the dataset and details the empirical model used for analysis. Section 4 documents the regression results, as well as endogenous treatment, heterogeneity examination. Section 5 provides a concise summary of the main conclusions. Finally, Section 6 offers policy recommendations informed by current events and discusses prospects for future research.
2.1 Factors Influencing Mental Health
Mental health is influenced by a wide spectrum of factors extending beyond biological and psychological mechanisms. For adults—particularly college students and young professionals—mental well-being is shaped by a combination of individual characteristics, family structure, living and social environment, and psychological and physiological mechanisms. Understanding these dimensions is essential for identifying population-specific vulnerabilities and for justifying the study’s focus on this demographic group.
2.1.1 Individual Characteristics
Individual attributes such as age, gender, education level, and socioeconomic status significantly affect mental health. For example, research indicates that young adults are more vulnerable to external stressors, especially during phases of occupational instability and role transitions [18,19,20,21]. Those with poorer economic conditions are also more likely to experience anxiety and depression [22,23]. For college students, academic pressure and identity issues are primary psychological risk factors, whereas working adults are more affected by workload and occupational burnout [24,25] Healthy lifestyle behaviors, such as regular exercise, a balanced diet, and sufficient sleep, further contribute to mental well-being and modulate individual susceptibility to stress. These differences suggest that mental health research should account for variation by age and social role.
Family environment forms an important social foundation for adult mental health. Individuals from supportive families tend to exhibit greater psychological resilience, while family conflict or divorce may increase the risk of mental disorders. Studies show that emotional support and stable intimate relationships can buffer the negative effects of stress, whereas their absence may exacerbate loneliness and anxiety [26,27,28,29,30]. For university students, parental expectations and the quality of family communication directly influence psychological adaptation; for working adults, marital quality and family responsibilities play key roles in psychological balance.
2.1.3 Living and Social Environment
The living environment encompasses study, work, housing conditions, and social support systems. College students commonly face academic competition and social comparison, while working adults contend with job intensity, role conflict, and lack of social support [24,31,32,33]. The quality of social relationships, sense of community engagement, and perceived environmental safety have all been shown to correlate closely with mental health. Moreover, accelerated urban life and increasing social isolation have become significant sources of psychological stress for modern adults.
2.1.4 Psychological and Physiological Mechanisms
At the psychological level, self-esteem, self-efficacy, and coping strategies determine how individuals adapt to stress [22]. Physiological mechanisms—such as neurotransmitter regulation, genetic differences, and chronic health conditions—also affect mental states [26,34]. For instance, chronic illnesses not only impose physical burdens but may also trigger anxiety and depression. These psychological and physiological factors interact to shape individual mental health trajectories.
2.2 The Role of Exercise Frequency in Mental Well-Being
Building on the understanding that both biological vulnerabilities and psychological processes influence mental health, frequent physical activity has emerged as a significant protective factor. According to Wanjau et al., regular exercise is consistently associated with lower levels of depression and anxiety, with evidence suggesting a probable causal relationship between physical inactivity and the onset of these disorders [35]. Hallgren et al. found that even modest exercise—such as engaging in physical activity one to two times per week—was associated with significantly lower odds of experiencing symptoms of depression and anxiety compared to inactivity [36]. The mechanisms behind these benefits appear to be twofold: biologically, exercise enhances neuroplasticity, balances neurotransmitters, and regulates stress hormones, while psychologically, it bolsters self-esteem, emotional coping, and resilience [37,38,39]. Thus, exercise frequency effectively bridges the biological and psychological domains, offering a practical strategy to mitigate genetic predispositions, neurochemical imbalances, stress related to chronic illness, and maladaptive cognitive or emotional patterns.
2.3 Gaps in the Existing Literature
Based on the four studies utilizing the China Family Panel Studies (CFPS) data to examine the relationship between physical activity and depression [40,41,42,43], several important gaps in the existing literature can be identified.
First, while Gong et al. [40] explored mediation effects via self-rated health and life satisfaction, their reliance on cross-sectional data from a single wave (2020) limits the ability to infer causal relationships or dynamic patterns over time. Second, Ren et al. [41], Employing a larger 2016 sample and addressing endogeneity through fixed effects and matching techniques, found that physical activity significantly reduces depression, with stronger effects among older and more educated individuals. However, the study mainly focused on average treatment effects without examining underlying mechanisms and relied on a single cross-sectional wave, limiting causal and dynamic inferences. Chen et al. [42], using CFPS data from 2016, 2018, and 2020 with fixed effects and cross-lagged panel models, examined the bidirectional relationship between physical activity and depressive symptoms in older adults, finding that exercise reduced depression while depression in turn lowered subsequent physical activity. Nevertheless, the study was limited to older adults and lacked heterogeneity analysis across subgroups, restricting the generalizability and depth of its findings. Also, due to data limitations, it wasn’t until 2018 that the more scientifically rigorous CESD-8 questionnaire for assessing mental health status became available, resulting in an inherent data lag. Lastly, Gu [43] based on 2020 CFPS data, they found that lower frequency and shorter duration of exercise significantly increased the risk of depression among adolescents, while moderate exercise and housework were both associated with lower depression levels. Yet the study relied on a single cross-sectional wave and did not capture causal direction or heterogeneity mechanisms, limiting the robustness and explanatory power of its conclusions.
In addition to CFPS-based studies, several international works have examined the link between physical activity and mental health among younger populations, offering valuable insights yet leaving notable research gaps.
First, Ekeland et al. [44] conducted a Cochrane systematic review of 23 randomized controlled trials (RCTs) involving 1821 children and adolescents, concluding that exercise can improve self-esteem in the short term. However, most included trials were small-scale and of low methodological quality, with limited follow-up and inconsistent measures of psychological well-being. Consequently, the evidence for sustained or long-term mental health benefits remains weak. Second, Carter et al. [45] implemented an RCT testing a preferred-intensity aerobic exercise program for adolescents with depression. While findings indicated improved depressive symptoms and quality of life, the study’s small sample size (n = 158) and narrow age range (14–17 years) constrained its external validity, limiting generalization to young adults or broader population contexts. Finally, Pascoe et al. [46] conducted a scoping review of 30 controlled trials exploring physical activity as a mental health promotion strategy for young people. They found that both moderate-to-vigorous and light-intensity activities can alleviate anxiety and depressive symptoms. Yet, the evidence base was fragmented and methodologically heterogeneous, with few longitudinal or causal designs, preventing strong conclusions about the duration and persistence of effects. Taken together, these studies highlight that despite substantial attention to the relationship between physical activity and youth mental health, existing empirical research remains limited in scope, duration, and representativeness. Particularly, there is a lack of large-scale, longitudinal, and causally oriented analyses that can generalize findings to diverse social and demographic contexts.
Building on these findings, our research draws on a larger number of observations to enhance statistical power and robustness. In addition, we focus on a persistently active group to explore the sustained impact of exercise, and employ instrumental variable (IV) techniques alongside mediation analysis to better address potential endogeneity and uncover underlying pathways. These enhancements aim to improve causal inference and provide more nuanced insights into the relationship between exercise frequency and mental health.
Exercise has been widely recognized as a significant determinant of mental health, but the mechanisms and population heterogeneity remain underexplored. To address this gap, we ground our hypotheses in established psychological and behavioral theories.
H1: Direct Effect of Exercise on Mental Health
According to Self-Determination Theory (SDT) [47], exercise satisfies basic psychological needs of autonomy, competence, and relatedness, enhancing intrinsic motivation and well-being. Meanwhile, Social Cognitive Theory (SCT) [48] suggests that exercise strengthens self-efficacy and perceived behavioral control, which positively influence emotional regulation. Resilience theory [49,50,51] further posits that repeated engagement in adaptive behaviors, such as regular physical activity, enhances an individual’s ability to cope with stress and reduce depressive symptoms. Empirical evidence shows that aerobic and resistance exercises improve mood, self-esteem, and emotional regulation [11,14]. Based on this theoretical framework, we propose:
H1: Increased exercise frequency significantly reduces depression symptoms and enhances well-being.
H2: Heterogeneity by Social Roles
Stress-buffering theory [52] posits that social roles and resources moderate the impact of stress on mental health. Employed individuals may leverage exercise to buffer occupational stress, while students often experience academic pressures that can reduce the psychological benefits of physical activity. Lower-educated groups may have fewer alternative coping strategies, amplifying the relative mental health gains from exercise [15,53,54]. Accordingly, we hypothesize:
H2: Employed individuals and those with lower education exhibit stronger mental health responses to exercise than students or highly educated groups.
H3: Mediating Role of Lifestyle Factors
The Health Belief Model (HBM) [53,54,55,56] suggests that personal beliefs about health behaviors, including perceived benefits and barriers, influence engagement and subsequent outcomes. Lifestyle factors, including sleep duration, daily cigarette consumption, and Body Mass Index (BMI), remain theoretically plausible and supported by existing literature. First, the relationship between exercise and unhealthy behaviors, such as smoking, has been documented in the health behavior substitution literature, suggesting that increased physical activity may reduce tobacco dependence, thereby lowering the risk of anxiety and depression [57,58,59]. Second, sleep duration is widely recognized as a crucial physiological process for bodily recovery and emotional regulation, and physical activity may indirectly improve mental health by enhancing sleep patterns [60,61,62]. Finally, BMI serves as an important indicator of overall body weight and health status, and its association with mental health is well established, particularly in cases where abnormal weight may trigger self-image concerns and psychological distress [63,64,65,66]. Therefore, despite the lack of statistical significance in the current sample and model specifications, these mediators may still play meaningful roles in other contexts, warranting further investigation in future research. Therefore, we propose:
H3: Lifestyle factors such as sleep duration, smoking amount, and BMI partially mediate the relationship between exercise and mental health.
3.1.1 Inclusion Criteria and Exclusion Criteria
- 1.Population Eligibility: Participants aged 18–44 years, covering two core groups: students (including high school/secondary technical school/technical school/vocational high school students and undergraduate students) and employed individuals (including workers without university education, junior college graduate workers, bachelor’s graduate workers, and master/doctor graduate workers). This age range focuses on young adults facing typical life-stage pressures such as academic demands and career adaptation, which aligns with the study’s focus on mental health in high-risk young populations.
- 2.Data Completeness: Individuals with complete data for core variables, including:
- (1)Outcome variables: Valid CESD-8 depression scores, CESD-20 depression scores, self-rated health status (HEALTH), and life satisfaction (LSATIS).
- (2)Explanatory variable: Exercise frequency (EXER) as measured by the CFPS questionnaire on physical activity participation over the past year.
- (3)Instrumental variables: Provincial-level per capita urban green space area (GREEN) and number of extreme temperature days (WEATHER).
- (4)Mediating variables: Sleep duration (SLEEP), daily cigarette consumption (SMOKE), and body mass index (BMI).
- (5)Control variables: Age (AGE), gender (MALE), urban/rural classification (URBAN), highest educational degree (EDU), and number of family members (FML).
- 3.Survey Wave Participation: Participants included in both the 2020 and 2022 waves of the China Family Panel Studies (CFPS), ensuring panel data consistency for longitudinal analysis.
- 4.Valid Mental Health Assessments: Participants with valid CESD-8 or CESD-20 scores, with raw data converted from the original 1–4 scale to the standard 0–3 scale to align with the original Center for Epidemiologic Studies Depression Scale (CES-D) specifications.
- 1.Age Exclusion: Individuals under 18 years or over 44 years old, as the study focuses on young adults.
- 2.Missing Core Data: Participants with missing values in any core variable (outcome, explanatory, instrumental, mediating, or control variables) to avoid bias from incomplete observations.
- 3.Special Population Exclusion: Graduate students (master’s/doctoral candidates) are excluded due to insufficient sample size.
- 4.Invalid Responses: Participants with logically inconsistent or extreme values (e.g., height < 30 cm or >240 cm, weight < 30.0 jin or >300.0 jin, sleep duration < 0.5 h or >24 h, daily cigarette consumption > 100 cigarettes) are excluded to ensure data reliability.
- 5.Non-Target Social Roles: Individuals not classified as either students or employed are excluded, as the study’s heterogeneity analysis focuses on these two core social roles.
3.1.2 China Family Panel Studies
Data from CFPS 2020 and 2022 were used in this study. The China Family Panel Studies (CFPS) is a national, comprehensive, and continuous social tracking survey program designed and implemented by the Institute of Social Science Survey Center (ISSS) at Peking University. The program aims to provide high-quality microdata support for academic research and public policy analysis by collecting multi-dimensional data on economic, health, education, and demographic characteristics of Chinese families and individuals over a long period of time. The data is tracked every two years and the survey covers a representative sample of 25 provinces across China. The data covers multiple modules and is suitable for multidisciplinary research in economics, sociology, public health, and other disciplines. Up to the current study, CFPS has released the results of seven surveys in 2010, 2012, 2014, 2016, 2018, 2020, and 2022 [67]. The CFPS data has become one of the core databases for researching the behavior of families and individuals in China because of its national representativeness, tracking design, and richness in health and socioeconomic variables. This study uses CFPS 2020 and 2022 data for research based on the following two aspects. First, selecting the most recent data can make this study current and reflect the current state of people’s mental health. Second, the data covers the main research subjects of this paper, i.e., the college student population and the working population.
Our core explained variable in the study was mental health, as measured by the CESD-8 and CESD-20. The CESD-8 and CESD-20 are both derived from the CES-D (Center for Epidemiologic Studies Depression Scale), a depression scale developed by the U.S. National Institute of Mental Health to assess depression symptoms experienced by the general population in the Depression symptoms experienced by the general population in the last week. The CESD-20 is the full version and consists of 20 questions covering a variety of emotional, cognitive, behavioral, and physical dimensions, each scored on a four-point scale (0–3). The total score ranges from 0–60, with higher scores indicating poorer mental status, and a score of 20 or greater is often used as a screening criterion for risk of depression [17]. In contrast, the CESD-8 is a simplified version. Only eight representative questions are retained for rapid screening of depressive symptoms, making it particularly suitable for use in large population-based surveys. The CESD-8 can be scored on the same four-point scale as the CESD-20. The total score ranges from 0–24, and a score greater than or equal to 8 is generally used as a basis for determining the possible presence of depressive symptoms [68]. Both instruments have good reliability and validity, with the CESD-20 being more precise and suitable for detailed studies and international comparisons, while the CESD-8 has been widely used in large-scale social surveys in China and other countries because of its simplicity and efficiency.
In the CFPS 2020 and 2022 databases used in this study, the CESD-8 measurements were provided. The CESD-20 scores in the database were calculated from the CESD-8 data. The official document explains that during the survey, they chose a random 1/5 of the sample of the respondent population to remain extended with CESD-20, leaving 4/5 of the sample with CESD-8 [67]. Based on this design, the data processors equated the scores of the suite of questions at a later stage, using the method of percentile equating (equipercentile equating), to generate a comparable score, CESD-20. This score maintains the scoring range of the CESD-20 and is also comparable to the CESD-20 scale scores. Therefore, we used both CESD-8 and CESD-20 as the core explanatory variables in our study. What’s more, the single-question scores in the original CES-D scale took values between 0–3, whereas the single-question scores in the CFPS dataset took values between 1–4, which made the total score range of the CES-D in the CFPS inconsistent with that in the original literature [17]. We transformed this by converting the single-question take values from 1–4 to 0–3 to make them consistent with those in the original scale.
In Table 1 We can see that a total of 18,604 respondents provided valid CESD-8 and CESD-20 scores. The mean of CESD-8 is 5.53 with a standard deviation of 3.74. The mean of CESD-20 is 13.12 with a standard deviation of 7.41. From the fact that the means of CESD-8 and CESD-20 are lower than 8 and 20, we can see that the overall average mental health status of the respondents is relatively good. The overall average mental health status is relatively good. If we use 8 and 20 as the cutoff, we can find that about 80% of the population is free from mental illness.
Table 1: Summary Statistics.
| Variables | Annotation | Obs | Mean | SD | Min | Max |
|---|---|---|---|---|---|---|
| I. Individual Level | ||||||
| CESD8 | Center for Epidemiologic Studies Depression Scale-8 | 18,604 | 5.53 | 3.740 | 0 | 24 |
| CESD20 | Center for Epidemiologic Studies Depression Scale-20 | 18,604 | 13.12 | 7.410 | 2 | 52 |
| HEALTH | Self-Reported Health Status | 18,604 | 2.580 | 1.010 | 1 | 5 |
| LSATIS | Life Satisfaction | 18,604 | 3.870 | 0.890 | 1 | 5 |
| EXER | Exercise Frequency | 18,604 | 1.590 | 2.060 | 0 | 7 |
| SCHOOL | Attending School = 1 | 18,604 | 0.110 | 0.310 | 0 | 1 |
| EMPLOY | Working Status | 16,787 | 1.225 | 0.679 | 0 | 3 |
| UNIVER | Whether Attending College or not | 18,604 | 0.060 | 0.230 | 0 | 1 |
| AGE | Age of the Individual | 18,604 | 31.64 | 7.210 | 18 | 44 |
| MALE | Male of the Individual (Male = 1) | 18,604 | 0.500 | 0.500 | 0 | 1 |
| URBAN | Urban and Rural Classification (Urban = 1) | 18,604 | 0.570 | 0.500 | 0 | 1 |
| EDU | Highest Academic Degree | 18,317 | 4.753 | 1.579 | 0 | 10 |
| FML | Number of Family Members | 18,604 | 4.310 | 2.110 | 1 | 16 |
| SLEEP | Sleep Duration | 13,835 | 7.553 | 1.138 | 0.5 | 24 |
| SMOKE | Daily Smoking Amount | 4970 | 12.634 | 8.146 | 1 | 80 |
| BMI | Body Mass Index | 17,293 | 23.161 | 3.589 | 8.081 | 47.750 |
| YEAR | Year | 18,604 | 2021 | 1.000 | 2020 | 2022 |
| HSS | High School/Secondary Technical School/Technical School/Vocational High School Student = 1 | 18,604 | 0.041 | 0.198 | 0 | 1 |
| UGS | Undergraduate Student = 1 | 18,604 | 0.050 | 0.220 | 0 | 1 |
| WNU | Worker without University Education = 1 | 18,604 | 0.523 | 0.499 | 0 | 1 |
| JCGW | Junior College Graduate Worker = 1 | 18,604 | 0.118 | 0.322 | 0 | 1 |
| BGW | Bachelor’s Graduate Worker = 1 | 18,604 | 0.113 | 0.317 | 0 | 1 |
| MDGW | Master/Doctor Graduate Worker = 1 | 18,604 | 0.019 | 0.135 | 0 | 1 |
| II. Provincial Level | ||||||
| PROVCD | Province | 18,604 | 38.62 | 15.69 | 11 | 65 |
| GREEN | Area of Urban Green Space Per Capita | 18,604 | 23.75 | 13.77 | 10.86 | 69.74 |
| WEATHER | Days above 30 Degrees and below 0 Degrees | 18,604 | 156.8 | 48.21 | 21 | 235 |
In the Chinese Family Panel Studies (CFPS), frequency of exercise is a core behavioral variable used to quantify the regularity of an individual’s participation in physical activity. This variable was obtained through questionnaires and mainly reflects the number of times respondents participated in physical activity during a specific time period. Exercise frequency is an important variable for measuring individual physical activity behavior, and was obtained by asking respondents, “How often have you participated in physical fitness activities in the past year? Categorical options are usually used (e.g., “less than once a month on average”, “more than once a month but less than once a week on average”, “1–2 times a week on average”, “3–4 times a week on average”, “5 times a week or more on average”, “1 time a day”, “twice a day or more”, “never attend”, These options are coded from 1 to 8.).
In the course of the study, we recoded the frequency of exercise variable in the original data in order to facilitate the quantitative analysis and ensure the logical consistency of the variable values. Specifically, we reassigned the option “never participate in sports”, which was originally coded as 8 in the questionnaire, to 0. This conversion was based on the following considerations: first, in terms of numerical meaning, 0 can more intuitively reflect the actual situation of a complete lack of sports behavior. The remaining category codes remain unchanged, so the exercise frequency codes have been adjusted from the original 1–8 to 0–7. Secondly, this conversion makes the variable show a monotonically increasing trend. That is, the larger value represents the higher frequency of exercise, thus ensuring a clearer and more explicit interpretation of the direction of the coefficients in the subsequent regression analysis. As can be seen from Table 1, the mean of EXER is 1.59, and the variance is 2.06. More than half of the observed subjects never participate in sports.
In this paper, urban green space per capita (GREEN) is selected as an instrumental variable, and the data are obtained from the National Bureau of Statistics (NBS). Urban green space area (GREEN) refers to the sum of all kinds of green space within the urban administrative area, including park green space, production green space, protection green space, subsidiary green space, and other green space. These green areas are mainly characterized by vegetation cover and have various functions such as ecological regulation and recreation. Its calculation usually covers the vertical projection area of trees, shrubs, lawns, and other plants, as well as the area occupied by waters and other supporting landscape facilities, but does not include special forms such as rooftop greening and vertical greening [69]. Urban green space area is an important indicator of the ecological quality and livability of a city, and one of the key data for urban planning and management.
In this study, the use of urban green space per capita as an instrumental variable is mainly based on the following logic: first, green space is closely related to exercise behavior. This is because more parks, greenways, and open spaces will improve the accessibility and convenience for residents to engage in outdoor exercise, thus increasing the frequency of exercise [70]. Second, urban green space area is usually determined by urban planning policies, land management, or natural geographic factors rather than as a direct result of an individual’s mental health status, and is therefore better exogenous [71].
In our study, we use data on provincial green space area. In order to make the data expression more precise as well as to reduce the error in the regression, we transformed the data into green space area per capita. In Table 1, we can see that the mean of green space area per capita is 23.75 hectares/person, and the standard deviation is 13.77 hectares/person.
Number of Days with Extreme Temperatures
We chose the number of extreme temperature days (WEATHER) as our other instrumental variable. In this paper, we select the temperature data measured by the National Center for Environmental Information (NCEI) under the National Oceanic and Atmospheric Administration (NOAA). Daily maximum and minimum temperature data from all meteorological observation stations involved in each year are combined and processed according to the year, and the China-wide stations are extracted [72]. The unit of data was also converted from degrees Fahrenheit (°F) to degrees Celsius (°C) to obtain the daily maximum as well as minimum temperature data from the meteorological stations nationwide. The day-by-day minimum and maximum temperature rasters within the administrative boundaries of prefecture-level cities were then averaged to obtain the day-by-day minimum and maximum temperatures at the provincial level.
In this study, the number of extreme temperature days is defined as the sum of days in a year when the daily temperature exceeds 30°C or the daily temperature is below 0°C. This indicator can objectively reflect the frequency and intensity of regional extreme temperature events. Among them, hot weather above 30°C easily triggers heat stress response and significantly reduces the willingness of residents to participate in outdoor activities. In contrast, severe cold weather below 0°C causes travel inconvenience and increases exercise risk. These two temperatures can effectively distinguish the effects of regular and extreme weather on human behavior. By counting the cumulative number of days that reached these two thresholds in each city over the years, a continuous variable reflecting temperature extremes can be constructed to provide a quantitative basis for analyzing the constraints of climatic conditions on exercise behavior.
The number of days with extreme temperatures can be a valid instrumental variable for studying the causal relationship between exercise and mental health because it fulfills two core conditions for an instrumental variable [73]. First, there is a significant correlation between extreme temperatures and exercise behavior. High and cold weather directly inhibits people’s willingness to exercise outdoors and reduces the actual exercise frequency [74]. Second, the number of extreme temperature days is determined by the natural climate and is characterized by exogeneity. Weather variability is not influenced by an individual’s mental health status or exercise habits, ruling out reverse causality [75]. This instrumental variable provides a natural experiment-style analytical framework for identifying causal effects of exercise on mental health. Table 1 shows that the weather data has a mean of 156.8 days and a standard deviation of 48.21 days, suggesting that on average, around 40% of the year is unsuitable for outdoor exercise.
This study adopts provincial-level data to incorporate two instrumental variables—per capita green space area and the number of extreme temperature days—into the database for matching analysis. Given the inaccessibility of county-level data in the CFPS database, the use of provincial-level data not only effectively addresses data availability issues but also further enhances the robustness of the model, rendering the research conclusions more practically meaningful and referential.
Sleep duration (SLEEP) was selected as a mediating variable between exercise frequency and mental health. In this study, the data on individuals’ sleep time were obtained from the Q403 series of questions in the CFPS questionnaire. The question was “What time do you usually go to bed at night?”. The question was split into two specific subsections: the Q403A recorded “hours” (0–24 pm) of time to fall asleep, and the Q403B recorded “minutes” (0–59 min). A 24-h format was used for all times to ensure uniformity of data. If a respondent had more than one period of sleep, the survey asked him or her to report the period of sleep that lasted the longest.
Daily cigarette consumption (smoke) was selected as a mediating variable between exercise frequency and mental health. In this study, the data on individuals’ daily cigarette use were obtained from the Q202 series of questions in the CFPS questionnaire. The question was “How many cigarettes do you smoke on average per day?”. Respondents were asked to provide a number between 1 and 100. If a respondent did not smoke, a value of 0 was recorded. This variable was used to capture the potential behavioral substitution effect of exercise on smoking, which may influence psychological well-being.
BMI was selected as a mediating variable to capture the potential physiological pathway between exercise frequency and mental health. In this study, data on height and weight were obtained from the P101 and P102 series of questions in the CFPS questionnaire. P101 asked “What is your current height in centimeters?”, and respondents were instructed to provide an integer value between 30 and 240 cm. P102 asked “What is your current weight in jin?”, and respondents provided a value between 30.0 and 300.0 jin, recorded with one decimal place. Height in centimeters was converted to meters, and weight in jin was converted to kilograms (1 jin = 0.5 kg) to calculate BMI using the standard formula.
In this study, we used a two-way fixed-effects model to analyze the relationship between exercise frequency and mental health as follows:
We further used the instrumental variables approach for estimation and the models are as follows:
According to the results of previous studies, it is known that exercise has both direct and indirect effects on mental health. Regarding indirect effects, exercise can affect people’s mental health by influencing their lifestyle. Therefore, exercise→healthy lifestyle habits→improved psychological well-being constitutes a reasonable pathway of the “mediating mechanism”. To verify the mediating role of lifestyle, we used the Baron and Kenny method [76], which allows us to test the mediating effect in three steps:
This study adopts a multi-step data analysis process, combining descriptive statistics, regression modeling, instrumental variable method and mediating effect test to verify the research hypotheses. The specific software and methods are detailed as follows:
Stata 17.0 (StataCorp LLC, College Station, TX, USA) is used for all empirical analyses, including data cleaning, variable recoding, descriptive statistics, regression estimation, and mediation effect testing. Provincial-level per capita urban green space area and extreme temperature days are matched with individual-level CFPS data by province and year using Stata’s ‘merge’ command. Excel 2021 (Microsoft Corp., Redmond, Washington, DC, USA) is used for preliminary data sorting, including checking for duplicate observations, and converting non-standard variable formats.
This study’s data analysis follows a structured workflow: first, data cleaning and preprocessing are conducted to exclude missing values, recode variables, and identify and remove extreme outliers. Second, descriptive statistics are used to characterize the distribution of core variables. Third, a two-way fixed-effects model is applied to estimate the baseline relationship between exercise frequency and mental health, complemented by instrumental variable (IV) estimation to address endogeneity, grouped regressions to explore heterogeneity by social role and education level, and the Baron and Kenny three-step method to test the mediating effects of smoking amount, sleep duration, and BMI.
4.1 Statistical Description Results
In this paper, the data of CFPS in 2020 and 2022 are selected as the research data. And two data, urban green space area and extreme weather, are introduced as instrumental variables. Among them, the data of urban green space area is from the National Bureau of Statistics (NBS). The extreme weather data comes from the National Center for Environmental Information (NCEI) under the National Oceanic and Atmospheric Administration (NOAA) of the U.S.A. Table 1 shows the results of the descriptive statistical analysis. We can see that there are mainly individual-level and provincial-level data. Since our primary focus is on college students and recent graduates, we will first concentrate on the adult demographic, specifically those aged 18 to 44. Therefore, we excluded data points for individuals under 18 and over 44 years of age. Additionally, this study removed observations containing missing values in the core explanatory variables, the dependent variable, or any of the control variables. It can be seen that the average age of the respondents in the sample is 31.64 years old, indicating that the main group of the sample is young adults. It is important to note that the education level is divided into elementary school, junior high school, high school/secondary school/technical school/vocational high school, college, bachelor’s degree, master’s degree, and doctoral degree based on the highest level of education in the most recent survey. Self-rated health and life satisfaction were both assigned values from 1 to 5, with higher values being happier. Age, gender, urban/rural categorization, and number of family members were also selected as control variables in this paper.
Table 2 demonstrates the preliminary regression results. The relationship between sports exercise and mental health was explored by using a two-way fixed effects approach, controlling for year and province. Columns (1) to (4) of the table show the results of the regression analysis using different explained variables, respectively. They are CESD-8, CESD-20, self-rated health and life satisfaction. All these variables are able to reflect the mental health status of an individual.
The regression results in column (1) of Table 2 show that the regression coefficient for frequency of exercise is −0.183 and is significant at the 0.1% level. This indicates that there is a significant negative correlation between exercise frequency and depression level. For every notch increase in physical activity frequency, the level of depression decreases by 0.183. This result remains robust after controlling for variables such as age, gender, urban/rural and family size. It is worth noting that increasing age was significantly associated with increased depressive symptoms, while men, urban dwellers and those with more family members had relatively lower levels of depression.
Table 2: Two-Way Fixed Effects Regression Results.
| Column Number | (1) | (2) | (3) | (4) |
|---|---|---|---|---|
| Estimation Method | HDFE | HDFE | HDFE | HDFE |
| Variables | CESD8 | CESD20 | HEALTH | LSATIS |
| EXER | −0.183*** | −0.362*** | 0.0135*** | 0.0138*** |
| (0.014) | (0.027) | (0.004) | (0.003) | |
| AGE | 0.0340*** | 0.0677*** | −0.0255*** | 0.00506*** |
| (0.004) | (0.008) | (0.001) | (0.001) | |
| MALE | −0.279*** | −0.554*** | 0.153*** | −0.0240 |
| (0.054) | (0.108) | (0.015) | (0.013) | |
| URBAN | −0.168** | −0.335** | −0.0620*** | −0.0119 |
| (0.059) | (0.116) | (0.016) | (0.014) | |
| FML | −0.0622*** | −0.122*** | 0.0151*** | 0.0366*** |
| (0.014) | (0.027) | (0.004) | (0.004) | |
| CONSTANT | 13.25*** | 32.55*** | 1.905*** | 3.545*** |
| (0.141) | (0.280) | (0.037) | (0.033) | |
| Year FE | √ | √ | √ | √ |
| Province FE | √ | √ | √ | √ |
| Obs | 18,604 | 18,604 | 18,604 | 18,604 |
| R-squared | 0.030 | 0.030 | 0.050 | 0.023 |
With reference to Zhu et al. [77], we recognize that physical activity may have endogenous issues with mental health. Simply put, the group that participates in physical activity is likely to be the group with good mental health. This group usually has lower levels of depression. In contrast, a group with depression would rarely participate in physical activity. In order to address the possible effects of this endogenous problem, this paper adopts the instrumental variable method, selecting the variables of urban green space area (GREEN) and extreme temperature days (WEATHER) as instrumental variables. It should be noted that since the two instrumental variables we used are provincial data, they are the same in the same province at the same time and have very little change between the two years 2020 and 2022. Therefore if we continue to take the fixed effects of adding year and province it will lead to unestimation. So we removed the year and province fixed effects for IV estimation.
Columns (1) and (4) of Table 3 represent the results of the first-stage regressions using urban green space per capita and extreme temperature days as instrumental variables, respectively. From column (1) we can see that the coefficient of urban green space per capita is 0.006 and significant at 0.1% level. This indicates that urban green space per capita has a significant positive effect on the frequency of physical activity. For every increase of 1 hectare of green space per capita, the frequency of physical activity will increase by 0.006. From column (4) we can see that the coefficient of weather is −0.00158 and is significant at 0.1% level, which indicates that the number of days with extreme temperatures is significantly negatively correlated with the frequency of physical activity. For each increase in the number of extreme temperature days, the frequency of exercise decreases by 0.00158. The results of the first stage regression in these two columns indicate that the correlations of the instrumental variables are satisfied. Columns (2), (3), (5), and (6) of Table 3 show the second stage regression results, respectively. We can see that the coefficients on exercise in columns (2) and (5) are −2.289 and 1.111, which are significantly larger in absolute value than the −0.183 in column (1) of Table 2. The improvement effect of exercise on mental health shown by the IV estimates is significantly stronger than that estimated in Table 2. This suggests that the traditional approach may have underestimated the intervention effect of exercise. The statistics of 26.26 and 26.75 for the SW multivariate F test exclude the problem of weak instrumental variables and indicate the validity of instrumental variables. This not only confirms the effect of exercise on mental health, but also provides an empirical basis for urban planning and climate adaptation measures.
We can also see that the estimation using GREEN as an instrumental variable shows that the negative effect of exercise on the level of depression is significant at the 0.1% level, while the estimation using WEATHER as an instrumental variable is significant at the 5% level. This indicates that the estimation using urban green space per capita as an instrumental variable is better.
Table 3: Instrument Variable Regression Results.
| Column Number | (1) | (2) | (3) | (4) | (5) | (6) |
|---|---|---|---|---|---|---|
| Estimation Method | HDFE | IV | IV | HDFE | IV | IV |
| Variables | EXER | CESD8 | CESD20 | EXER | CESD8 | CESD20 |
| GREEN | 0.006*** | |||||
| (0.001) | ||||||
| WEATHER | −0.00158*** | |||||
| (0.0003) | ||||||
| EXER | −2.289*** | −4.515*** | 1.111* | 2.166* | ||
| (0.548) | (1.083) | (0.435) | (0.859) | |||
| AGE | −0.045*** | −0.0625* | −0.123* | −0.04409*** | 0.0880*** | 0.173*** |
| (0.002) | (0.025) | (0.049) | (0.002) | (0.020) | (0.039) | |
| MALE | 0.323*** | 0.416* | 0.819* | 0.32234*** | −0.691*** | −1.358*** |
| (0.029) | (0.197) | (0.389) | (0.030) | (0.157) | (0.309) | |
| URBAN | 0.478*** | 0.818** | 1.609** | 0.5046*** | −0.905*** | −1.776*** |
| (0.031) | (0.290) | (0.574) | (0.030) | (0.231) | (0.456) | |
| FML | −0.027*** | −0.111*** | −0.218*** | −0.03545*** | 0.00241 | 0.00415 |
| (0.007) | (0.027) | (0.054) | (0.007) | (0.022) | (0.043) | |
| CONSTANT | 2.562*** | 18.95*** | 43.81*** | 2.9417*** | 9.821*** | 25.86*** |
| (0.078) | (1.486) | (2.938) | (0.089) | (1.181) | (2.330) | |
| Year FE | × | × | × | × | × | × |
| Province FE | × | × | × | × | × | × |
| SW multivariate F test | 26.26 | 26.26 | 26.75 | 26.75 | ||
| Obs | 18,604 | 18,604 | 18,604 | 18,604 | 18,604 | 18,604 |
4.4.1 Current Students vs. Employed People
After cleaning, the CFPS 2020 and 2022 surveys had a total sample size of 18,604. In order to explore the impact between people with different social statuses. We divided two subgroups from the sample by schooling and employment status. In the CFPS data, the variable SCHOOL has three statuses, “not attending school”, “in the middle of the semester”, and “on vacation”. We mark “in semester” and “on vacation” as 1 to indicate that the group is a student, and 0 for the rest of the variables. The variable EMPLOY also has three statuses, “unemployed”, ‘employed’ and “out of the labor market”, and we mark “employed” as 1 to indicate the working population and 0 for the others. So that we have two groups, the school-going group and the working group. There are a total of 2040 observations for the school-going group and 14,380 observations for the working group. It can be seen that most of our samples are from the working population.
Table 4 reveals significant differences in exercise intervention effects across populations through grouped instrumental variable regressions. Columns (1) through (4) show the regression results for the group of school students and columns (5) through (8) show the regression results for the working population. We can see that the coefficients on physical activity in columns (1) to (4) of Table 4 are all insignificant. This indicates that for school students the effect of frequency of physical activity on depression levels is not significant whether GREEN or WEATHER is used as an instrumental variable. This indicates that exercise is not effective in alleviating depression in school students. As shown in the Fig. A1 (see Appendix A), the distribution of exercise frequency exhibits distinct clustering characteristics rather than a uniform gradient distribution. It predominantly manifests as two concentrated intervals: “low frequency (e.g., 0 times/week)” and “specific medium-to-high frequency (e.g., 1–2 times/week)”. Meanwhile, intermediate frequencies such as Exercise Frequency = 1, 2, 4, or 5 account for an extremely low proportion, with distribution gaps even observed. This distribution pattern directly weakens the statistical association between exercise and mental health: On one hand, the absence of mid-range frequency samples prevents capturing the differentiated improvement effects of “gradual changes in exercise frequency” on mental states; On the other hand, the concentrated distribution indicates insufficient variability in exercise behavior. A large number of students either completely abstain from exercise or maintain a fixed frequency. The psychological state differences between these two groups may be masked by other factors such as academic pressure and social environment, making it difficult for the independent effect of exercise to stand out statistically. Ultimately, this results in exercise showing no significant impact on mental health.
And from columns (5) to (8) of Table 4, we can see that the results of estimation using GREEN and WEATHER as instrumental variables are significant for the employed population. In columns (5) and (6), the coefficients on exercise are −2.073 and −4.083. this indicates that exercise has a significant negative effect on the level of depression when GREEN is used as an instrumental variable. In columns (7) and (8), the coefficients of exercise are 2.140 and 4.216, which indicates that exercise has a significant positive effect on the level of depression when WEATHER is used as an instrumental variable. This indicates that exercise has a significant effect on depression relief among employed people. Exercise can significantly contribute to the mental health of the employed population. This may be due to the fact that the employed population relies more on exercise to alleviate their mental health problems, and it becomes a more accessible avenue of stress relief for the employed population as compared to school students.
Table 4: Results of School vs. Employ.
| Column Number | (1) | (2) | (3) | (4) | (5) | (6) | (7) | (8) |
|---|---|---|---|---|---|---|---|---|
| Subsample Category | SCHOOL | SCHOOL | SCHOOL | SCHOOL | EMPLOY | EMPLOY | EMPLOY | EMPLOY |
| Estimation Method | IV-GREEN | IV-GREEN | IV-WEATHER | IV-WEATHER | IV-GREEN | IV-GREEN | IV-WEATHER | IV-WEATHER |
| Variables | CESD8 | CESD20 | CESD8 | CESD20 | CESD8 | CESD20 | CESD8 | CESD20 |
| EXER | −4.698 | −9.208 | 1.640 | 3.151 | −2.073*** | −4.083*** | 2.140* | 4.216* |
| (11.060) | (21.690) | (1.189) | (2.318) | (0.499) | (0.986) | (1.008) | (1.992) | |
| AGE | −0.138 | −0.271 | 0.0940 | 0.182 | −0.0194 | −0.0376 | 0.0409* | 0.0814* |
| (0.409) | (0.803) | (0.052) | (0.102) | (0.010) | (0.020) | (0.016) | (0.032) | |
| MALE | 4.227 | 8.289 | −1.545 | −2.968 | 0.137 | 0.268 | −0.749** | −1.478** |
| (10.080) | (19.770) | (1.104) | (2.152) | (0.137) | (0.271) | (0.234) | (0.462) | |
| URBAN | 1.202 | 2.374 | −0.117 | −0.198 | 0.763* | 1.493* | −1.630** | −3.221** |
| (2.343) | (4.596) | (0.329) | (0.641) | (0.298) | (0.588) | (0.582) | (1.149) | |
| FML | −0.165 | −0.324 | 0.0557 | 0.107 | −0.124*** | −0.243*** | 0.0476 | 0.0943 |
| (0.404) | (0.793) | (0.072) | (0.141) | (0.030) | (0.058) | (0.047) | (0.094) | |
| CONSTANT | 27.00 | 39.51 | 6.259 | −0.939 | 17.27*** | 20.48*** | 10.25*** | 26.65*** |
| (36.210) | (71.030) | (3.952) | (7.703) | (0.869) | (1.717) | (1.703) | (3.364) | |
| Year FE | × | × | × | × | × | × | × | × |
| Province FE | × | × | × | × | × | × | × | × |
| SW multivariate F test | 0.19 | 0.19 | 4.02 | 4.02 | 29.02 | 29.02 | 8.73 | 8.73 |
| Obs | 2040 | 2040 | 2040 | 2040 | 14,380 | 14,380 | 14,380 | 14,380 |
4.4.2 Student Population Segmentation
In order to further investigate the effects of exercise on mental health in the student population, we further segmented the student population by using the variables “highest level of education” (EDU) and SCHOOL. They are HSS (High School/Secondary Technical School/Technical School/Vocational High School Student) and UGS (Undergraduate Student). Due to the small sample of students enrolled in master’s and doctoral programs, we do not analyze them here.
Table 5 shows the regression results for enrolled students grouped by different educational stages. Columns (1) through (4) represent the regression results for the group of high school or middle school students, and columns (5) through (8) represent the regression results for the group of undergraduate students. We can see that the coefficients of EXER are not significant for either high school or undergraduate students using GREEN and WEATHER as instrumental variables. This suggests that for the student population, the effect of exercise frequency on depression is not significant across the different stages of education. This is contrary to the results for the overall sample. Looking at the results of this analysis in conjunction with the results of columns (1) to (4) of Table 4, we find that for the range of the school student population, the effect of exercise on mental health is not significant for students at all levels of education.
Table 5: Student Population Segmentation Results.
| Column Number | (1) | (2) | (3) | (4) | (5) | (6) | (7) | (8) |
|---|---|---|---|---|---|---|---|---|
| Subsample Category | HSS | HSS | HSS | HSS | UGS | UGS | UGS | UGS |
| Estimation Method | IV-GREEN | IV-GREEN | IV-WEATHER | IV-WEATHER | IV-GREEN | IV-GREEN | IV-WEATHER | IV-WEATHER |
| Variable | CESD8 | CESD20 | CESD8 | CESD20 | CESD8 | CESD20 | CESD8 | CESD20 |
| EXER | −0.965 | −1.904 | 6.810 | 13.14 | 4.556 | 8.816 | 1.705 | 3.274 |
| (1.356) | (2.681) | (25.560) | (49.450) | (16.980) | (32.940) | (1.401) | (2.726) | |
| AGE | 0.0206 | 0.0405 | 0.180 | 0.348 | 0.233 | 0.454 | 0.117* | 0.228* |
| (0.058) | (0.114) | (0.560) | (1.083) | (0.695) | (1.348) | (0.067) | (0.130) | |
| MALE | 1.038 | 2.046 | −5.817 | −11.22 | −4.425 | −8.589 | −1.835 | −3.554 |
| (1.224) | (2.421) | (22.560) | (43.640) | (15.440) | (29.940) | (1.307) | (2.542) | |
| URBAN | 0.166 | 0.332 | 0.482 | 0.942 | −1.118 | −2.127 | −0.239 | −0.419 |
| (0.271) | (0.536) | (1.470) | (2.845) | (5.269) | (10.22) | (0.527) | (1.025) | |
| FML | −0.0329 | −0.0675 | 0.280 | 0.537 | 0.0759 | 0.147 | −0.00144 | −0.00340 |
| (0.092) | (0.181) | (1.067) | (2.065) | (0.492) | (0.955) | (0.093) | (0.181) | |
| CONSTANT | 14.37*** | 14.80* | −9.532 | −31.44 | −3.417 | −19.79 | 5.919 | −1.639 |
| (4.308) | (8.518) | (78.680) | (152.200) | (55.650) | (107.900) | (4.672) | (9.088) | |
| Year FE | × | × | × | × | × | × | × | × |
| Province FE | × | × | × | × | × | × | × | × |
| SW multivariate F test | 1.83 | 1.83 | 0.08 | 0.08 | 0.08 | 0.08 | 2.92 | 2.92 |
| Observations | 758 | 758 | 758 | 758 | 1070 | 1070 | 1070 | 1070 |
Using the same methodology described above, we also segmented the employment groups. We divided the employed population into four groups, which are WNU (Worker without University Education), JCGW (Junior College Graduate Worker), BGW (Bachelor’s Graduate Worker) and MDGW (Master/Doctor Graduate Worker).
Table 6 shows the regression results for the employed population grouped by different educational qualifications. Since it was mentioned earlier that the estimation results using WEATHER as an instrumental variable are not as good as using GREEN as an instrumental variable, we use GREEN as an instrumental variable for estimation here. Columns (1) and (2) show the regression results for the group of laborers who have not attended college. We can see that the coefficients of EXER for CESD-8 and CESD-20 are −2.250 and −4.411, respectively, and are significant at the 1% level. This suggests that for laborers who have not attended college, sports and exercise can significantly reduce the level of depression. Mental health can be improved through exercise. While in columns (3) to (8), all the coefficients of EXER are not significant, which indicates that for working people with college education and above, exercise is not able to improve mental health. However, the results in Table 7 show that the first-stage F-statistics of the instrumental variable WEATHER for the core explanatory variable EXER are all below 10, indicating a risk of weak instrumental variables, and the reliability of the results should be viewed with caution. There is significant sample heterogeneity: only in the WNU group, EXER has a marginally significant positive impact on the depression scales (CESD8/CESD20) at the 5% significance level, while in the other groups (JCGW/BGW/MDGW), the relationship among the core variables is not significant. Thus we can find that exercise has a significant improvement effect on mental health only for workers with low education levels. As the level of education increases, this effect becomes less significant. This may be due to the fact that highly educated workers have more alternative means of psychological adjustment. It is also possible that this is because this group has lower levels of raw depression or that the levels of depression in the highly educated group are more related to work stress than to physical activity.
Table 6: Employment Groups Segmentation Results.
| Column Number | (1) | (2) | (3) | (4) | (5) | (6) | (7) | (8) |
|---|---|---|---|---|---|---|---|---|
| Subsample Category | WNU | WNU | JCGW | JCGW | BGW | BGW | MDGW | MDGW |
| Estimation Method | IV-GREEN | IV-GREEN | IV-GREEN | IV-GREEN | IV-GREEN | IV-GREEN | IV-GREEN | IV-GREEN |
| Variable | CESD8 | CESD20 | CESD8 | CESD20 | CESD8 | CESD20 | CESD8 | CESD20 |
| EXER | −2.250** | −4.411** | −3.904 | −7.807 | 2.694 | 5.199 | −0.508 | −1.017 |
| (0.845) | (1.665) | (2.909) | (5.813) | (2.656) | (5.169) | (0.596) | (1.186) | |
| AGE | −0.0240 | −0.0463 | −0.0148 | −0.0285 | 0.0424 | 0.0855 | −0.0153 | −0.0301 |
| (0.013) | (0.026) | (0.032) | (0.064) | (0.039) | (0.075) | (0.044) | (0.087) | |
| MALE | −0.0516 | −0.106 | 1.408 | 2.820 | −1.457 | −2.835 | −0.121 | −0.218 |
| (0.168) | (0.331) | (1.276) | (2.550) | (1.276) | (2.483) | (0.617) | (1.228) | |
| URBAN | 0.620 | 1.205 | 0.659 | 1.320 | −1.132 | −2.216 | −0.167 | −0.327 |
| (0.334) | (0.658) | (0.848) | (1.694) | (0.628) | (1.223) | (0.819) | (1.630) | |
| FML | −0.111*** | −0.218*** | −0.150 | −0.302 | −0.177* | −0.347* | 0.212 | 0.423 |
| (0.032) | (0.063) | (0.135) | (0.270) | (0.088) | (0.171) | (0.133) | (0.266) | |
| CONSTANT | 17.43*** | 20.76*** | 20.68*** | 27.39*** | 7.895 | 22.16 | 14.32*** | 14.64*** |
| (1.218) | (2.400) | (4.897) | (9.788) | (4.060) | (7.903) | (2.057) | (4.095) | |
| Year FE | × | × | × | × | × | × | × | × |
| Province FE | × | × | × | × | × | × | × | × |
| SW multivariate F test | 11.63 | 11.63 | 2.06 | 2.06 | 1.60 | 1.60 | 12.71 | 12.71 |
| Obs | 9732 | 9732 | 2193 | 2193 | 2107 | 2107 | 348 | 348 |
Table 7: Employment Groups Segmentation Results.
| Column Number | (1) | (2) | (3) | (4) | (5) | (6) | (7) | (8) |
|---|---|---|---|---|---|---|---|---|
| Subsample Category | WNU | WNU | JCGW | JCGW | BGW | BGW | MDGW | MDGW |
| Estimation Method | IV-WEATHER | IV-WEATHER | IV-WEATHER | IV-WEATHER | IV-WEATHER | IV-WEATHER | IV-WEATHER | IV-WEATHER |
| Variable | CESD8 | CESD20 | CESD8 | CESD20 | CESD8 | CESD20 | CESD8 | CESD20 |
| EXER | 3.264* | 6.402* | 0.464 | 0.908 | −1.448 | −2.675 | −3.957 | −7.762 |
| (1.851) | (3.641) | (0.798) | (1.581) | (1.933) | (3.730) | (3.595) | (7.072) | |
| AGE | 0.0397 | 0.0785 | −0.0140 | −0.0269 | 0.0839** | 0.164** | −0.0967 | −0.189 |
| (0.024) | (0.048) | (0.015) | (0.029) | (0.027) | (0.052) | (0.120) | (0.235) | |
| MALE | −0.865** | −1.702** | −0.429 | −0.845 | 0.485 | 0.857 | 2.469 | 4.846 |
| (0.313) | (0.617) | (0.374) | (0.741) | (0.925) | (1.785) | (2.835) | (5.577) | |
| URBAN | −1.431* | −2.818* | −0.441 | −0.874 | −0.354 | −0.737 | 3.640 | 7.118 |
| (0.706) | (1.388) | (0.279) | (0.554) | (0.442) | (0.853) | (4.092) | (8.048) | |
| FML | 0.00883 | 0.0169 | −0.00852 | −0.0185 | −0.114 | −0.226* | −0.305 | −0.588 |
| (0.054) | (0.106) | (0.051) | (0.101) | (0.059) | (0.0114) | (0.576) | (1.132) | |
| CONSTANT | 9.754*** | 25.72*** | 13.48*** | 33.04*** | 14.08*** | 33.91*** | 22.30* | 50.25** |
| (2.613) | (5.139) | (1.393) | (2.761) | (2.944) | (5.679) | (8.883) | (17.472) | |
| Year FE | × | × | × | × | × | × | × | × |
| Province FE | × | × | × | × | × | × | × | × |
| SW multivariate F test | 4.52 | 4.52 | 5.67 | 5.67 | 1.32 | 1.32 | 1.41 | 1.41 |
| Obs | 9732 | 9732 | 2193 | 2193 | 2107 | 2107 | 348 | 348 |
4.5 Mediation Effects Analysis
Having confirmed the significant effect of exercise frequency (EXER) on mental health, this section examines the potential mediating role of daily cigarette consumption (SMOKE). Prior research suggests that regular exercise may reduce smoking behavior, while smoking is known to exacerbate depression and negatively affect mental well-being.
Column (1) of Table 8 replicates the benchmark regression, with EXER significantly reducing CESD-8 (coefficient = −0.158, p < 0.001), confirming the total effect. Column (2) examines the effect of EXER on SMOKE, showing a strong and significant negative association (coefficient = −0.389, p < 0.001), suggesting that increased exercise frequency reduces smoking. Column (3) incorporates both EXER and SMOKE into the model. The coefficient of SMOKE on CESD-8 is positive and significant (0.037, p < 0.001), while EXER remains significant. These results indicate that cigarette consumption partially mediates the relationship between exercise and mental health. EXER significantly reduces smoking frequency, and smoking is positively correlated with higher depression scores. This suggests that exercise improves mental health partially by reducing smoking. Table 9 shows the direct effect accounts for 90.97% of the total effect, while the indirect effect through smoking contributes 9.03% of the total reduction in depression.
Table 8: Smoke consumption mediation effect results.
| Column Number | (1) | (2) | (3) |
|---|---|---|---|
| Variable | CESD8 | SMOKE | CESD8 |
| EXER | −0.158*** | −0.389*** | −0.144*** |
| (0.029) | (0.057) | (0.029) | |
| MALE | −1.689*** | 6.700*** | −1.935*** |
| (0.372) | (0.471) | (0.372) | |
| AGE | 0.008 | 0.211*** | 0.001 |
| (0.009) | (0.017) | (0.009) | |
| URBAN | −0.175 | −0.711** | −0.149 |
| (0.119) | (0.241) | (0.119) | |
| FML | −0.138*** | 0.047 | −0.140*** |
| (0.027) | (0.054) | (0.027) | |
| SMOKE | 0.037*** | ||
| (0.007) | |||
| CONSTANT | 16.001*** | −0.163 | 16.007*** |
| (0.475) | (0.718) | (0.473) | |
| Year FE | √ | √ | √ |
| Province FE | √ | √ | √ |
| Obs | 4906 | 4906 | 4906 |
Table 9: Effect table of smoke mediation effect.
| Effect Value | Std. Err. | p Value | Effect Proportion | |
|---|---|---|---|---|
| Total effect | −0.158 | 0.0292 | 6.0 × 10−8 | - |
| Direct effect | −0.144 | 0.0293 | 9.0 × 10−7 | 90.97% |
| Indirect effect | −0.014 | 0.004 | 0.000064 | 9.03% |
Next, this paper investigates whether sleep duration (SLEEP) mediates the effect of exercise on mental health. Evidence indicates that regular exercise improves sleep quality and duration, and sufficient sleep is associated with reduced depressive symptoms.
Column (1) of Table 10 reproduces the benchmark result, with EXER significantly reducing CESD-8 (coefficient = −0.172, p < 0.001). Column (2) examines the effect of EXER on SLEEP, which is not significant (coefficient = 0.00203, p > 0.1), suggesting that exercise does not strongly predict sleep duration in this sample. Column (3) includes both EXER and SLEEP. SLEEP has a significant negative effect on CESD-8 (−0.398, p < 0.001), while EXER remains significant. These findings suggest that sleep duration does not mediate the relationship between exercise and mental health in this sample.
Table 10: Sleep duration mediation effect results.
| Column Number | (1) | (2) | (3) |
|---|---|---|---|
| Variable | CESD8 | SLEEP | CESD8 |
| EXER | −0.172*** | 0.002 | −0.171*** |
| (0.000) | (0.679) | (0.000) | |
| MALE | −0.349*** | −0.173*** | −0.418*** |
| (0.000) | (0.000) | (0.000) | |
| AGE | 0.009 | −0.023*** | −0.000009 |
| (0.078) | (0.000) | (0.999) | |
| URBAN | −0.181** | −0.135*** | −0.235*** |
| (0.009) | (0.000) | (0.001) | |
| FML | −0.071*** | 0.013** | −0.066*** |
| (0.000) | (0.008) | (0.000) | |
| SLEEP | −0.398*** | ||
| (0.000) | |||
| CONSTANT | 14.320*** | 8.418*** | 17.674*** |
| (0.000) | (0.000) | (0.000) | |
| Year FE | √ | √ | √ |
| Province FE | √ | √ | √ |
| Obs | 13,835 | 13,835 | 13,835 |
Finally, the potential mediating role of Body Mass Index (BMI) is examined.
Column (1) of Table 11 shows the baseline effect of EXER on CESD-8 (coefficient = −0.173, p < 0.001). Column (2) examines the effect of EXER on BMI, which is not significant (coefficient = 0.013, p > 0.1). Column (3) includes both EXER and BMI; BMI does not significantly predict CESD-8 (−0.0003, p > 0.1), and EXER remains significant. These findings suggest that BMI does not mediate the relationship between exercise and mental health in this sample.
Table 11: BMI mediation effect results.
| Column Number | (1) | (2) | (3) |
|---|---|---|---|
| Variable | CESD8 | BMI | CESD8 |
| EXER | −0.173*** | 0.013 | −0.173*** |
| (0.000) | (0.318) | (0.000) | |
| MALE | −0.321*** | 1.563*** | −0.320*** |
| (0.000) | (0.000) | (0.000) | |
| AGE | 0.011* | 0.111*** | 0.011* |
| (0.021) | (0.000) | (0.025) | |
| URBAN | −0.231*** | 0.119* | −0.231*** |
| (0.000) | (0.030) | (0.000) | |
| FML | −0.066*** | 0.047*** | −0.066*** |
| (0.000) | (0.000) | (0.000) | |
| BMI | −0.0003 | ||
| (0.969) | |||
| CONSTANT | 14.143*** | 18.453*** | 14.150*** |
| (0.000) | (0.000) | (0.000) | |
| Year FE | √ | √ | √ |
| Province FE | √ | √ | √ |
| Obs | 17,293 | 17,293 | 17,293 |
This study evaluates whether the three hypotheses in Section 2.4 are supported by the empirical results. The main hypothesis, Hypothesis 1 (H1), was fully supported, demonstrating that increased exercise frequency significantly reduces depression symptoms while also enhancing self-rated health and life satisfaction. Hypothesis 2 (H2) was supported, revealing a difference in effects by group: the positive mental health impact of exercise was stronger among employed individuals and those with lower education (specifically non-university educated workers), but was found to be statistically insignificant for students or higher-educated employed groups. Finally, Hypothesis 3 (H3) was partially supported. Daily cigarette consumption was confirmed as a significant mediator (exercise reduces smoking, which improves mental health), but sleep duration and BMI did not exhibit a statistically significant mediating role in the relationship between exercise and mental health in this sample. Its benefits vary significantly across socio-demographic groups, with employed individuals with lower education levels experiencing more pronounced improvements.
Our finding that greater green space availability promotes physical activity aligns with prior research in the built environment and public health literature. According to social-ecological models, accessible and attractive green spaces reduce barriers to physical activity by providing safe, enjoyable environments, thereby facilitating health-promoting behaviors at the environmental level [78]. This provides empirical support for urban planning policies aimed at improving public health outcomes.
Perhaps the most insightful finding is the heterogeneity of exercise benefits across groups. Contrary to studies emphasizing the universal benefits of physical activity [79], we find that the marginal mental health gains for students and highly educated individuals are limited. This may be attributed to differences in dominant stressors. According to stress-buffering theory, exercise effectively mitigates routine and moderate stress [52]. However, for students and highly educated groups, primary stressors—such as academic competition and professional pressures—tend to be systemic and high-intensity, exceeding the buffering capacity of exercise alone [47]. Therefore, although exercise maintains fundamental health value, its marginal impact on mental health may be constrained if core stress sources are not simultaneously addressed.
These findings have important policy and practical implications. First, they call for more targeted and precise public health interventions. For employed and low-educated adults, investing in community green spaces and implementing “exercise + psychological counseling” programs in workplaces can generate high health returns. Second, for students and highly educated individuals, policymakers and educational institutions should recognize that promoting exercise alone is insufficient. Interventions should simultaneously address macro-environmental factors, such as reforming educational evaluation systems, providing career development support, and ensuring access to mental health resources, to reduce psychological burdens at their source. This aligns with the core objectives of Healthy China 2030 [80], which emphasize integrated development of physical and mental health for all citizens.
Several limitations should be acknowledged. First, the analysis relies on only two waves of CFPS data (2020–2022), limiting the ability to capture long-term trends and dynamic effects of exercise on mental health. Future research could extend the temporal scope with additional waves. Second, exercise types were not differentiated; distinct modalities may have unique effects on mental health. Finally, the spatial granularity of the data is limited to the provincial level, which may mask city-level variations. Future studies should consider more detailed geographic data.
This study utilizes data from the 2020 and 2022 waves of the China Family Panel Studies (CFPS) to systematically examine the impact of individual exercise frequency on mental health outcomes. Indicators such as the CESD depression index, self-rated health, and life satisfaction are used as key measures. The results show that exercise frequency significantly reduces depression levels while positively enhancing self-rated health and life satisfaction, with the findings demonstrating strong robustness. Furthermore, after addressing potential endogeneity by introducing average green space per capita and the number of extreme temperature days as instrumental variables, the core conclusions remain valid.
Also, the heterogeneity analysis highlight that the mental health benefits of exercise are not uniformly distributed across groups. While no significant effects are observed among students regardless of educational attainment, exercise proves especially beneficial for employed individuals with lower levels of education. This suggests that policies and interventions aiming to promote mental well-being through exercise may yield the greatest returns when targeted toward lower-educated segments of the working population.
In addition to the aforementioned research methods, this study also examined several potential mediators, including daily cigarette consumption, sleep duration, and Body Mass Index (BMI). The results indicate that cigarette consumption exerts a significant mediating effect, whereas sleep duration and BMI do not show statistically significant mediation in the current sample and model specifications. Nonetheless, the latter factors may still hold relevance in other populations or under alternative modeling approaches, suggesting avenues for further investigation in future research.
Overall, this study not only confirms the positive effects of exercise on mental health but also uncovers the variation in effects across different demographic groups. These findings offer empirical evidence and theoretical support for the design of targeted mental health interventions and more precise policy implementation.
Acknowledgement:
Funding Statement: The authors received no specific funding for this study.
Author Contributions: The authors confirm contribution to the paper as follows: Conceptualization, Chun-Chieh Hu; Methodology, Chun-Chieh Hu; Validation, Chun-Chieh Hu; Software, Shuhan Zheng and Youjia Lin; Formal analysis, Chun-Chieh Hu, Shuhan Zheng and Youjia Lin; Data curation, Youjia Lin and Shuhan Zheng; Writing original draft preparation, Shuhan Zheng and Youjia Lin; Writing-review and editing, Chun-Chieh Hu; Visualization, Shuhan Zheng; Supervision, Chun-Chieh Hu; Project administration, Chun-Chieh Hu. All authors reviewed the results and approved the final version of the manuscript.
Availability of Data and Materials: The data that support the findings of this study are openly available in China Family Panel Studies at https://cfpsdata.pku.edu.cn/#/home.
Ethics Approval: Not applicable.
Conflicts of Interest: The authors declare no conflicts of interest to report regarding the present study.
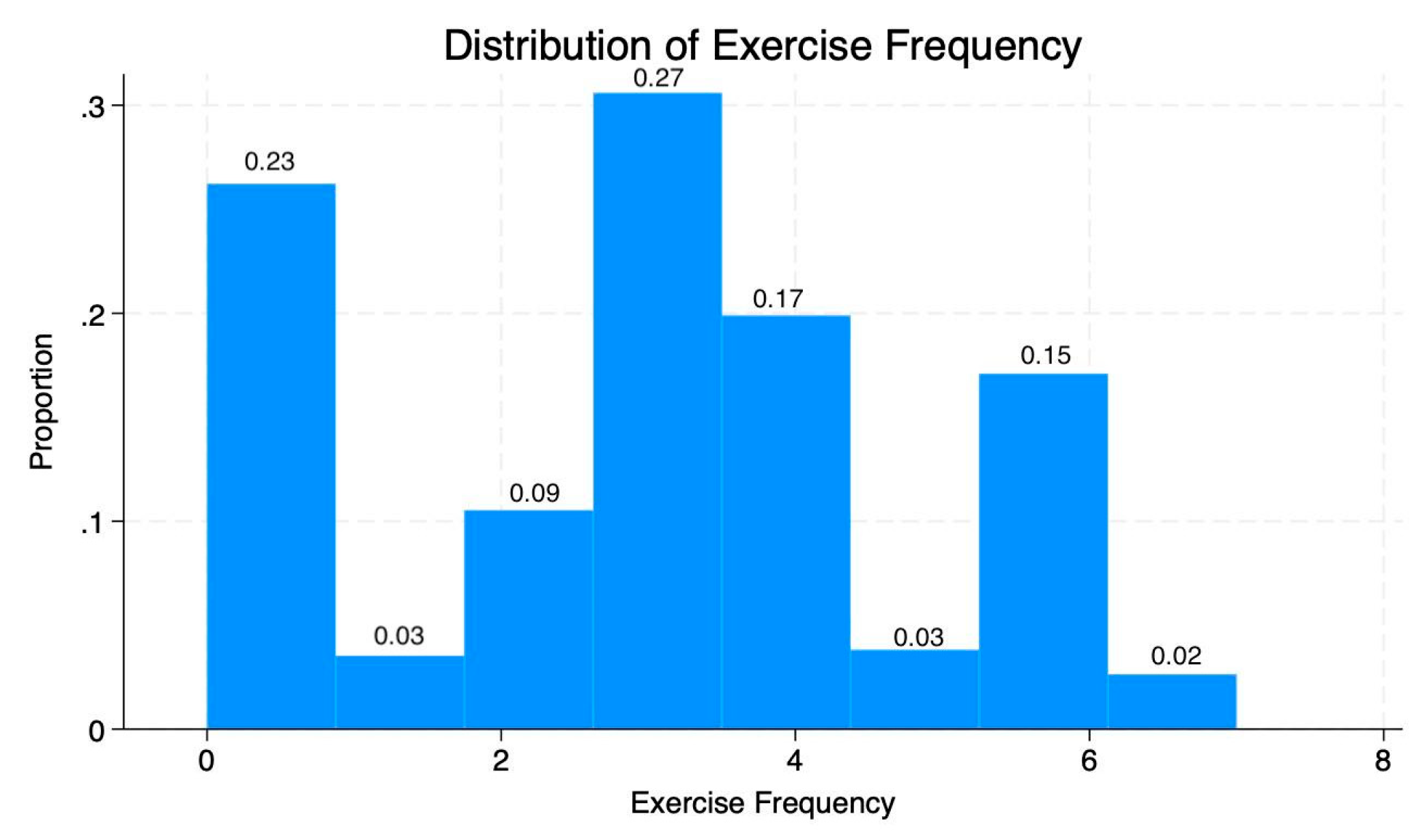
Figure A1: Distribution of exercise frequency.
References
1. Hossain MM , Tasnim S , Sultana A , Faizah F , Mazumder H , Zou L , et al. Epidemiology of mental health problems in COVID-19: a review. F1000Research. 2020; 9( 1): 636. doi:10.12688/f1000research.24457.1. [Google Scholar] [CrossRef]
2. Cénat JM , Farahi SMMM , Dalexis RD , Darius WP , Bekarkhanechi FM , Poisson H , et al. The global evolution of mental health problems during the COVID-19 pandemic: a systematic review and meta-analysis of longitudinal studies. J Affect Disord. 2022; 315: 70– 95. doi:10.1016/j.jad.2022.07.011. [Google Scholar] [CrossRef]
3. Nochaiwong S , Ruengorn C , Thavorn K , Hutton B , Awiphan R , Phosuya C , et al. Global prevalence of mental health issues among the general population during the coronavirus disease-2019 pandemic: a systematic review and meta-analysis. Sci Rep. 2021; 11( 1): 10173. doi:10.1038/s41598-021-89700-8. [Google Scholar] [CrossRef]
4. Wu T , Jia X , Shi H , Niu J , Yin X , Xie J , et al. Prevalence of mental health problems during the COVID-19 pandemic: a systematic review and meta-analysis. J Affect Disord. 2021; 281: 91– 8. doi:10.1016/j.jad.2020.11.117. [Google Scholar] [CrossRef]
5. Jiloha RC . COVID-19 and mental health. Epidem Int. 2020; 5( 1): 7– 9. doi:10.24321/2455.7048.202002. [Google Scholar] [CrossRef]
6. Bruffaerts R , Mortier P , Auerbach RP , Alonso J , Hermosillo De la Torre AE , Cuijpers P , et al. Lifetime and 12-month treatment for mental disorders and suicidal thoughts and behaviors among first year college students. Int J Methods Psych Res. 2019; 28( 2): e1764. doi:10.1002/mpr.1764. [Google Scholar] [CrossRef]
7. Chen B , Xie M , Zhang Y , Zhang H , Yu NX , Lin D . Is it a vicious circle and for whom? The reciprocal association between rumination and somatic symptoms and moderation by stress: a daily diary study among Chinese college students. Appl Psych Health Well. 2024; 16( 2): 460– 76. doi:10.1111/aphw.12499. [Google Scholar] [CrossRef]
8. Huang Y , Wang Y , Zeng L , Yang J , Song X , Rao W , et al. Prevalence and correlation of anxiety, insomnia and somatic symptoms in a Chinese population during the COVID-19 epidemic. Front Psychiatry. 2020; 11: 568329. doi:10.3389/fpsyt.2020.568329. [Google Scholar] [CrossRef]
9. Fan W , Zhang H , Lei P , Tang Y , Du J , Li J . Uncovering the complex interactions of mental health symptoms in Chinese college students: insights from network analysis. BMC Psychol. 2025; 13( 1): 448. doi:10.1186/s40359-025-02731-y. [Google Scholar] [CrossRef]
10. Tan M , Wu Z , Li J , Liang Y , Lv W . Analyzing the impact of unemployment on mental health among Chinese university graduates: a study of emotional and linguistic patterns on Weibo. Front Public Health. 2024; 12: 1337859. doi:10.3389/fpubh.2024.1337859. [Google Scholar] [CrossRef]
11. AL Mutlaqah MN , Al-Mutairi JM , Ali WK , Almutayri AMH , Al-Dhafiri MKM , Thubab AHA , et al. The comprehensive role of physical exercise in enhancing mental health: an academic review of current evidence and implications for treatment strategies. J Ecohumanism. 2024; 3( 8): 9259– 66. doi:10.62754/joe.v3i8.5542. [Google Scholar] [CrossRef]
12. Schuch FB , Vancampfort D , Firth J , Rosenbaum S , Ward PB , Silva ES , et al. Physical activity and incident depression: a meta-analysis of prospective cohort studies. Am J Psychiatry. 2018; 175( 7): 631– 48. doi:10.1176/appi.ajp.2018.17111194. [Google Scholar] [CrossRef]
13. Bennie JA , Teychenne MJ , De Cocker K , Biddle SJH . Associations between aerobic and muscle-strengthening exercise with depressive symptom severity among 17,839 U.S. adults. Prev Med. 2019; 121: 121– 7. doi:10.1016/j.ypmed.2019.02.022. [Google Scholar] [CrossRef]
14. Pujari V . Moving to improve mental health—the role of exercise in cognitive function: a narrative review. J Pharm Bioallied Sci. 2024; 16( Suppl 1): S26. doi:10.4103/jpbs.jpbs_614_23. [Google Scholar] [CrossRef]
15. Kpame MB , Richard J . Aerobic exercise intervention as part of management options for depression and anxiety. KIU J Soc Sci. 2020; 6( 1): 145– 50. [Google Scholar]
16. Sharma A , Madaan V , Petty FD . Exercise for mental health. Prim Care Companion J Clin Psychiatry. 2006; 8( 2): 106. doi:10.4088/PCC.v08n0208a. [Google Scholar] [CrossRef]
17. Wu Q , Dai L , Zhen Q , Zhang J , Gu L , Zhang C , et al. China Family Panel Studies 2016 Database Introduction and Data Cleaning Report [Internet]. 2018 [cited 2025 Jan 1]. Available from: http://www.isss.pku.edu.cn/cfps/docs/20201201085335172101.pdf. (In Chinese). [Google Scholar]
18. Campbell F , Blank L , Cantrell A , Baxter S , Blackmore C , Dixon J , et al. Factors that influence mental health of university and college students in the UK: a systematic review. BMC Public Health. 2022; 22( 1): 1778. doi:10.1186/s12889-022-13943-x. [Google Scholar] [CrossRef]
19. Sivertsen B , Hysing M , Knapstad M , Harvey AG , Reneflot A , Lønning KJ , et al. Suicide attempts and non-suicidal self-harm among university students: prevalence study. BJPsych Open. 2019; 5( 2): e26. doi:10.1192/bjo.2019.4. [Google Scholar] [CrossRef]
20. Jessop DC , Herberts C , Solomon L . The impact of financial circumstances on student health. Br J Health Psychol. 2005; 10( 3): 421– 39. doi:10.1348/135910705X25480. [Google Scholar] [CrossRef]
21. Bewick B , Koutsopoulou G , Miles J , Slaa E , Barkham M . Changes in undergraduate students’ psychological well‐being as they progress through university. Stud High Educ. 2010; 35( 6): 633– 45. doi:10.1080/03075070903216643. [Google Scholar] [CrossRef]
22. Frankham C , Richardson T , Maguire N . Psychological factors associated with financial hardship and mental health: a systematic review. Clin Psychol Rev. 2020; 77: 101832. doi:10.1016/j.cpr.2020.101832. [Google Scholar] [CrossRef]
23. Frankham C , Richardson T , Maguire N . Do locus of control, self-esteem, hope and shame mediate the relationship between financial hardship and mental health? Community Ment Health J. 2020; 56( 3): 404– 15. doi:10.1007/s10597-019-00467-9. [Google Scholar] [CrossRef]
24. Barros C , Fonte C , Alves S , Baylina P . Can psychosocial work factors influence psychologists’ positive mental health? Occup Med. 2019; 69( 3): 204– 10. doi:10.1093/occmed/kqz034. [Google Scholar] [CrossRef]
25. Gauthier CA , Pacheco T , Proteau É , Auger É , Coulombe S . Self-management at work’s moderating effect on the relations between psychosocial work factors and well-being. Int J Environ Res Public Health. 2025; 22( 7): 1070. doi:10.3390/ijerph22071070. [Google Scholar] [CrossRef]
26. Hastings PD , Guyer AE , Parra LA . Conceptualizing the influence of social and structural determinants of neurobiology and mental health: why and how biological psychiatry can do better at addressing the consequences of inequity. Biol Psychiatry Cogn Neurosci Neuroimaging. 2022; 7( 12): 1215– 24. doi:10.1016/j.bpsc.2022.06.004. [Google Scholar] [CrossRef]
27. Cheng Y , Zhang L , Wang F , Zhang P , Ye B , Liang Y . The effects of family structure and function on mental health during China’s transition: a cross-sectional analysis. BMC Fam Pract. 2017; 18( 1): 59. doi:10.1186/s12875-017-0630-4. [Google Scholar] [CrossRef]
28. Grüning Parache L , Vogel M , Meigen C , Kiess W , Poulain T . Family structure, socioeconomic status, and mental health in childhood. Eur Child Adolesc Psychiatry. 2024; 33( 7): 2377– 86. doi:10.1007/s00787-023-02329-y. [Google Scholar] [CrossRef]
29. Park H , Lee KS . The association of family structure with health behavior, mental health, and perceived academic achievement among adolescents: a 2018 Korean nationally representative survey. BMC Public Health. 2020; 20( 1): 510. doi:10.1186/s12889-020-08655-z. [Google Scholar] [CrossRef]
30. Yeo G , Tan C , Ho D , Baumeister RF . How do aspects of selfhood relate to depression and anxiety among youth? A meta-analysis. Psychol Med. 2023; 53( 11): 4833– 55. doi:10.1017/s0033291723001083. [Google Scholar] [CrossRef]
31. Dalgard OS , Tambs K . Urban environment and mental health. Br J Psychiatry. 1997; 171( 6): 530– 6. doi:10.1192/bjp.171.6.530. [Google Scholar] [CrossRef]
32. Allen J , Balfour R , Bell R , Marmot M . Social determinants of mental health. Int Rev Psychiatry. 2014; 26( 4): 392– 407. doi:10.3109/09540261.2014.928270. [Google Scholar] [CrossRef]
33. Liu Z , Su M , Zhang T , Zhang W , Li D . What role does social class play in the impact of social environment on residents’ health. Sci Rep. 2025; 15: 13430. doi:10.1038/s41598-025-97525-y. [Google Scholar] [CrossRef]
34. Kao CH . Neurotransmitters and their influence on mental health disorders. Perspect Neurosci Psych Open Access. 2024; 7( 6): 284– 6. doi:10.47532/npoa.2024.7(6).284-286. [Google Scholar] [CrossRef]
35. Wanjau MN , Möller H , Haigh F , Milat A , Hayek R , Lucas P , et al. Physical activity and depression and anxiety disorders: a systematic review of reviews and assessment of causality. AJPM Focus. 2023; 2( 2): 100074. doi:10.1016/j.focus.2022.100030. [Google Scholar] [CrossRef]
36. Hallgren M , Kandola A , Stubbs B , Nguyen TTD , Wallin P , Andersson G , et al. Associations of exercise frequency and cardiorespiratory fitness with symptoms of depression and anxiety—a cross-sectional study of 36,595 adults. Ment Health Phys Act. 2020; 19: 100351. doi:10.1016/j.mhpa.2020.100351. [Google Scholar] [CrossRef]
37. Hassmén P , Koivula N , Uutela A . Physical exercise and psychological well-being: a population study in finland. Prev Med. 2000; 30( 1): 17– 25. doi:10.1006/pmed.1999.0597. [Google Scholar] [CrossRef]
38. Liu Q , Jiang M , Li S , Yang Y . Social support, resilience, and self-esteem protect against common mental health problems in early adolescence. Medicine. 2021; 100( 4): e24334. doi:10.1097/MD.0000000000024334. [Google Scholar] [CrossRef]
39. Tang J , Chen N , Liang H , Gao X . The effect of built environment on physical health and mental health of adults: a nationwide cross-sectional study in China. Int J Environ Res Public Health. 2022; 19( 11): 6492. doi:10.3390/ijerph19116492. [Google Scholar] [CrossRef]
40. Gong C , Li Y , Chen G . Relationship between physical exercise and risk of depression: an assessment of intermediate variables through self-assessed health status and life satisfaction in the Chinese family tracking survey (CFPS) data. Risk Manag Healthc Policy. 2024; 17: 3315– 25. doi:10.2147/rmhp.s499489. [Google Scholar] [CrossRef]
41. Ren C , Wang C , Zhang M . The antidepressant effect of physical exercise: evidence from China Family Panel Studies. PLoS One. 2022; 17( 10): e0274321. doi:10.1371/journal.pone.0274321. [Google Scholar] [CrossRef]
42. Chen H , Lu T , Sui H , Tao B , Chen H , Yan J . Bidirectional relationships between physical exercise and depressive symptoms among Chinese older adults evidence from the China family panel studies. Sci Rep. 2025; 15: 15689. doi:10.1038/s41598-025-00947-x. [Google Scholar] [CrossRef]
43. Gu J . Physical activity and depression in adolescents: evidence from China family panel studies. Behav Sci. 2022; 12( 3): 71. doi:10.3390/bs12030071. [Google Scholar] [CrossRef]
44. Ekeland E , Heian F , Hagen KB , Abbott JM , Nordheim L . Exercise to improve self-esteem in children and young people. Cochrane Database Syst Rev. 2004; 1( 1): CD003683. doi:10.4073/csr.2005.4. [Google Scholar] [CrossRef]
45. Carter T , Callaghan P , Khalil E , Morres I . The effectiveness of a preferred intensity exercise programme on the mental health outcomes of young people with depression: a sequential mixed methods evaluation. BMC Public Health. 2012; 12( 1): 187. doi:10.1186/1471-2458-12-187. [Google Scholar] [CrossRef]
46. Pascoe MC , Bailey AP , Craike M , Carter T , Patten R , Stepto NK , et al. Exercise interventions for mental disorders in young people: a scoping review. BMJ Open Sport Exerc Med. 2020; 6( 1): e000678. doi:10.1136/bmjsem-2019-000678. [Google Scholar] [CrossRef]
47. Deci EL , Ryan RM . The “what”and “why”of goal pursuits: human needs and the self-determination of behavior. Psychol Inq. 2000; 11( 4): 227– 68. doi:10.1207/s15327965pli1104_01. [Google Scholar] [CrossRef]
48. Locke EA , Bandura A . Social foundations of thought and action: a social-cognitive view. Acad Manag Rev. 1987; 12( 1): 169. doi:10.2307/258004. [Google Scholar] [CrossRef]
49. Hu Y , Huang Y , Zhang H , Fang M , Chen G . Insights from China: understanding the impact of community resilience and government trust in psychological resilience and anxiety during COVID-19. Front Public Health. 2023; 11: 1298269. doi:10.3389/fpubh.2023.1298269. [Google Scholar] [CrossRef]
50. Anderies J , Walker B , Kinzig A . Insight, Part of a Special Feature on Exploring Resilience in Social-Ecological Systems Fifteen Weddings and a Funeral: Case Studies and Resilience-Based Management [Internet]. 2016 [cited 2025 Dec 7]. Available from: https://www.semanticscholar.org/paper/Insight%2C-part-of-a-Special-Feature-on-Exploring-in-Anderies-Walker/da4e42dc58240c3e44171c62a0ce88602732a6fb. [Google Scholar]
51. Robinson G , Lee E , Leckning B , Silburn S , Nagel T , Midford R . Validity and reliability of resiliency measures trialled for the evaluation of a preventative Resilience-promoting social-emotional curriculum for remote Aboriginal school students. PLoS One. 2022; 17( 1): e0262406. doi:10.1371/journal.pone.0262406. [Google Scholar] [CrossRef]
52. Cohen S , Wills TA . Stress, social support, and the buffering hypothesis. Psychol Bull. 1985; 98( 2): 310– 57. doi:10.1037/0033-2909.98.2.310. [Google Scholar] [CrossRef]
53. Aznárez-Sanado M , Artuch-Garde R , Carrica-Ochoa S , García-Roda C , Arellano A , Ramírez-Castillo D , et al. Lifetime mental health problems in adult lower secondary education: a student survey. Front Psychol. 2020; 11: 1522. doi:10.3389/fpsyg.2020.01522. [Google Scholar] [CrossRef]
54. Jeftic I , Furzer BJ , Dimmock JA , Wright K , Boyd C , Budden T , et al. Structured exercise programs for higher education students experiencing mental health challenges: background, significance, and implementation. Front Public Health. 2023; 11: 1104918. doi:10.3389/fpubh.2023.1104918. [Google Scholar] [CrossRef]
55. Hjorth CF , Bilgrav L , Frandsen LS , Overgaard C , Torp-Pedersen C , Nielsen B , et al. Mental health and school dropout across educational levels and genders: a 4.8-year follow-up study. BMC Public Health. 2016; 16( 1): 976. doi:10.1186/s12889-016-3622-8. [Google Scholar] [CrossRef]
56. Kim MK , Han K , Kim B , Kim J , Kwon HS . Effects of exercise initiation and smoking cessation after new-onset type 2 diabetes mellitus on risk of mortality and cardiovascular outcomes. Sci Rep. 2022; 12: 10656. doi:10.1038/s41598-022-14603-1. [Google Scholar] [CrossRef]
57. Chen H , Yang Y , Miyai H , Yi C , Oliver BG . The effects of exercise with nicotine replacement therapy for smoking cessation in adults: a systematic review. Front Psychiatry. 2022; 13: 1053937. doi:10.3389/fpsyt.2022.1053937. [Google Scholar] [CrossRef]
58. Jamali Q , Bittoun R . Galantamine as a treatment option for nicotine addiction. J Smok Cessat. 2021; 2021: e7. doi:10.1155/2021/9975811. [Google Scholar] [CrossRef]
59. Prapavessis H , De Jesus S , Fitzgeorge L , Faulkner G , Maddison R , Batten S . Exercise to enhance smoking cessation: the getting physical on cigarette randomized control trial. Ann Behav Med. 2016; 50( 3): 358– 69. doi:10.1007/s12160-015-9761-9. [Google Scholar] [CrossRef]
60. Dolezal BA , Neufeld EV , Boland DM , Martin JL , Cooper CB . Interrelationship between sleep and exercise: a systematic review. Adv Prev Med. 2017; 2017: 1364387. doi:10.1155/2017/1364387. [Google Scholar] [CrossRef]
61. Kredlow MA , Capozzoli MC , Hearon BA , Calkins AW , Otto MW . The effects of physical activity on sleep: a meta-analytic review. J Behav Med. 2015; 38( 3): 427– 49. doi:10.1007/s10865-015-9617-6. [Google Scholar] [CrossRef]
62. Sun W , Huang Y , Wang Z , Yu Y , Lau A , Ali G , et al. Sleep duration associated with body mass index among Chinese adults. Sleep Med. 2015; 16( 5): 612– 6. doi:10.1016/j.sleep.2014.12.011. [Google Scholar] [CrossRef]
63. Jung SJ , Woo HT , Cho S , Park K , Jeong S , Lee YJ , et al. Association between body size, weight change and depression: systematic review and meta-analysis. Br J Psychiatry. 2017; 211( 1): 14– 21. doi:10.1192/bjp.bp.116.186726. [Google Scholar] [CrossRef]
64. Faith MS , Butryn M , Wadden TA , Fabricatore A , Nguyen AM , Heymsfield SB . Evidence for prospective associations among depression and obesity in population-based studies. Obes Rev. 2011; 12( 5): e438– 53. doi:10.1111/j.1467-789x.2010.00843.x. [Google Scholar] [CrossRef]
65. Schrempft S , Jiménez-Sánchez C , Baysson H , Zaballa ME , Lamour J , Stringhini S , et al. Pathways linking BMI trajectories and mental health in an adult population-based cohort: role of emotional eating and body dissatisfaction. Int J Obes. 2025; 49( 7): 1317– 26. doi:10.1038/s41366-025-01772-y. [Google Scholar] [CrossRef]
66. Luppino FS , de Wit LM , Bouvy PF , Stijnen T , Cuijpers P , Penninx BWJH , et al. Overweight, obesity, and depression: a systematic review and meta-analysis of longitudinal studies. Arch Gen Psychiatry. 2010; 67( 3): 220. doi:10.1001/archgenpsychiatry.2010.2. [Google Scholar] [CrossRef]
67. Xie Y , Qiu Z , Ping L . China Family Panel Studies Sampling Design [Internet]. 2012 [cited 2025 Jan 1]. Available from: http://www.isss.pku.edu.cn/cfps/docs/20201028165326806875.pdf. (In Chinese). [Google Scholar]
68. Ofstedal MB , Steffick D , Fonda S , Langa KM , Robert WB , Herzog AR . Documentation of affective functioning measures in the Health and Retirement Study [Internet]. 2000 [cited 2025 Jan 1]. Available from: http://hrsonline.isr.umich.edu/docs/userg/dr-005.pdf. [Google Scholar]
69. Kabisch N , Qureshi S , Haase D . Human–environment interactions in urban green spaces—a systematic review of contemporary issues and prospects for future research. Environ Impact Assess Rev. 2015; 50: 25– 34. doi:10.1016/j.eiar.2014.08.007. [Google Scholar] [CrossRef]
70. Kifayatullah S , Saqib Z , Khan MI , Zaman-ul-Haq M , Kucher DE , Ullah S , et al. Equitable urban green space planning for sustainable cities: a GIS-based analysis of spatial disparities and functional strategies. Sci Rep. 2025; 15: 22686. doi:10.1038/s41598-025-07578-2. [Google Scholar] [CrossRef]
71. Alcock I , White MP , Lovell R , Higgins SL , Osborne NJ , Husk K , et al. What accounts for ‘England’s green and pleasant land’? A panel data analysis of mental health and land cover types in rural England. Landsc Urban Plan. 2015; 142: 38– 46. doi:10.1016/j.landurbplan.2015.05.008. [Google Scholar] [CrossRef]
72. NOAA . National Centers for Environmental Information (NCEI). 2019 [cited 2025 Jan 1]. Available from: https://www.ncei.noaa.gov/. [Google Scholar]
73. Giles-Corti B , Donovan RJ . The relative influence of individual, social and physical environment determinants of physical activity. Soc Sci Med. 2002; 54( 12): 1793– 812. doi:10.1016/s0277-9536(01)00150-2. [Google Scholar] [CrossRef]
74. Chan CB , Ryan DA . Assessing the effects of weather conditions on physical activity participation using objective measures. Int J Environ Res Public Health. 2009; 6( 10): 2639– 54. doi:10.3390/ijerph6102639. [Google Scholar] [CrossRef]
75. Deschênes O , Greenstone M . Climate change, mortality, and adaptation: evidence from annual fluctuations in weather in the US. Am Econ J Appl Econ. 2011; 3( 4): 152– 85. doi:10.1257/app.3.4.152. [Google Scholar] [CrossRef]
76. Baron RM , Kenny DA . The moderator-mediator variable distinction in social psychological research: conceptual, strategic, and statistical considerations. J Pers Soc Psychol. 1986; 51( 6): 1173– 82. doi:10.1037/0022-3514.51.6.1173. [Google Scholar] [CrossRef]
77. Zhu L , Xiong X , Li Z , Meng S , Zhai Y . The relationship between exercise habits and mental health among university students in China: a cross-sectional study based on instrumental variable analysis. BMC Public Health. 2024; 24( 1): 3353. doi:10.1186/s12889-024-20825-x. [Google Scholar] [CrossRef]
78. Nurse J , Basher D , Bone A , Bird W . An ecological approach to promoting population mental health and well-being—a response to the challenge of climate change. Perspect Public Health. 2010; 130( 1): 27– 33. doi:10.1177/1757913909355221. [Google Scholar] [CrossRef]
79. Rebar AL , Stanton R , Geard D , Short C , Duncan MJ , Vandelanotte C . A meta-meta-analysis of the effect of physical activity on depression and anxiety in non-clinical adult populations. Health Psychol Rev. 2015; 9( 3): 366– 78. doi:10.1080/17437199.2015.1022901. [Google Scholar] [CrossRef]
80. Xinhua News Agency . The Central Committee of the Communist Party of China and the State Council issued the “Healthy China 2030” Planning Outline [Internet]. 2016 [cited 2025 Jan 1]. Available from: https://www.gov.cn/zhengce/2016-10/25/content_5124174.htm. [Google Scholar]
Cite This Article
 Copyright © 2026 The Author(s). Published by Tech Science Press.
Copyright © 2026 The Author(s). Published by Tech Science Press.This work is licensed under a Creative Commons Attribution 4.0 International License , which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
 Downloads
Downloads
 Citation Tools
Citation Tools