
 Submit a Paper
Submit a Paper Propose a Special lssue
Propose a Special lssue Open Access
Open Access
ARTICLE

Associations of Self-Esteem, Life Satisfaction, Resilience, and Coping Strategies with Depression Severity: Evidence from a Comparative and Mediation Analysis
1 Department of Psychiatry, Mugla Sitki Kocman University Faculty of Medicine, Mugla, Türkiye
2 Department of Biostatistics, Mugla Sitki Kocman University Faculty of Medicine, Mugla, Türkiye
3 Department of Psychiatry, Bitlis State Hospital, Bitlis, Türkiye
4 Department of Psychiatry, Mugla Sitki Kocman University Training and Research Hospital, Mugla, Türkiye
* Corresponding Author: Mahmut Selçuk. Email:
(This article belongs to the Special Issue: Evidence-based Approaches to Managing Stress, Depression, Anxiety, and Suicide)
International Journal of Mental Health Promotion 2026, 28(2), 12 https://doi.org/10.32604/ijmhp.2026.076391
Received 19 November 2025; Accepted 22 January 2026; Issue published 27 February 2026
 View Full Text
View Full Text Download PDF
Download PDFAbstract
Background: Self-esteem, life satisfaction, resilience, and coping strategies are closely linked to depression; however, their interrelationships and relative contributions to depressive outcomes remain insufficiently understood. This study aimed to examine these associations in individuals with major depressive disorder (MDD) and healthy controls and to evaluate their predictive and mediating roles in depression. Methods: This analytical cross-sectional study included 311 participants (158 patients with MDD and 153 healthy controls) recruited from the Psychiatry Outpatient Clinics of Mugla Training and Research Hospital. Psychiatric diagnoses were confirmed using the Structured Clinical Interview for DSM-5 (SCID-5). Groups were balanced for age, sex, and education using propensity score matching (PSM). Participants completed the Rosenberg Self-Esteem Scale, Satisfaction with Life Scale, Brief Resilience Scale, Brief COPE Inventory, and Beck Depression Inventory. Results: Compared with healthy controls, individuals with MDD reported significantly lower life satisfaction and resilience and higher depressive symptom severity, whereas self-esteem did not differ significantly between groups. Emotion-focused coping decreased with increasing depression severity, while avoidant coping showed a modest but significant increase in severe depression. Logistic regression analyses identified life satisfaction (OR = 0.95, p = 0.004) and resilience (OR = 0.92, p = 0.002) as significant protective predictors of depression. Mediation analyses demonstrated that life satisfaction partially mediated the relationship between self-esteem and depression, whereas resilience exerted a predominantly direct effect. Conclusion: Life satisfaction and resilience emerge as key protective factors against depression. Self-esteem appears to influence depressive outcomes indirectly through life satisfaction rather than through a direct effect. These findings underscore the importance of interventions that enhance resilience and promote positive evaluations of life in individuals at risk for depression.Keywords
Depression is one of the most common psychiatric disorders worldwide and remains a leading contributor to the global burden of disease. According to recent estimates, more than 332 million people are affected globally, making depression a major source of disability, premature mortality, and reduced quality of life [1,2]. Beyond affective symptoms, depression is strongly associated with cognitive dysfunction, impaired social functioning, and significant occupational and interpersonal difficulties [3]. Despite substantial progress in understanding its biological and psychosocial underpinnings, depression remains highly heterogeneous, suggesting that a wide range of vulnerability and protective factors are involved in its onset, course, and treatment response. This complexity has led to increasing interest in examining psychological strengths—such as self-esteem, life satisfaction, resilience, and coping strategies—as potential buffers that may mitigate the risk of depression or reduce its severity [4,5].
Self-esteem, defined as a person’s overall evaluation of self-worth, has consistently been shown to protect against depression. Low self-esteem is not only a risk factor for the development of depressive symptoms but also predicts poor treatment response and higher relapse risk [6]. Mediation models further suggest that self-esteem exerts both direct and indirect influences on depression outcomes. For instance, Awad et al. [7] demonstrated that depression partially mediated the relationship between self-esteem and health-related behaviors, supporting the notion that self-esteem influences psychological outcomes through intermediary processes even outside clinical depression contexts. Notably, cross-cultural studies suggest that the role and expression of self-esteem in psychological well-being may vary across contexts, being stronger in individualist cultures and weaker in collectivist societies, where relational well-being is more central [8,9].
Life satisfaction, representing the cognitive-evaluative dimension of subjective well-being, has also been closely linked to depression. Recent evidence suggests that lower life satisfaction predicts increases in depressive symptoms over time, while higher life satisfaction is associated with resilience and improved recovery from mental health difficulties [5,10,11]. In addition, life satisfaction may function as an important explanatory pathway linking other psychological resources, such as self-esteem and resilience, to depression severity [4,11]. This positions life satisfaction as both a protective factor and a potential explanatory pathway in depression research.
Psychological resilience, often defined as the ability to adapt and maintain functioning despite adversity, has emerged as another crucial determinant of mental health. Meta-analytic findings confirm that resilience is moderately and negatively correlated with depression and other mood symptoms [3]. Moreover, resilience buffers the impact of both acute and chronic stressors, including pandemic-related adversities, on psychological outcomes [10,12]. Importantly, resilience is not a static trait but a dynamic process that interacts with coping strategies, life satisfaction, and self-esteem [13]. Neurobiological evidence also links resilience to more adaptive hypothalamic–pituitary–adrenal axis functioning and lower inflammatory reactivity, underscoring its biopsychosocial relevance [14].
Coping strategies represent another set of mechanisms through which individuals manage psychological distress [4]. Coping is typically categorized into problem-focused, emotion-focused, and avoidant styles. Evidence suggests that maladaptive coping strategies, such as avoidant or ruminative coping, are strongly associated with greater depression severity, whereas adaptive coping styles, such as problem-focused strategies, are generally protective [3,4]. However, findings remain inconsistent, and the effectiveness of coping appears to depend on stressor controllability—known as the “fit hypothesis [15]. Thus, the role of coping strategies in depression may vary according to situational and cultural contexts.
Guided by subjective well-being frameworks and stress–vulnerability models, psychological resources can be conceptualized as operating at interconnected levels. Self-esteem reflects a core self-evaluative resource, whereas life satisfaction represents a higher-order cognitive appraisal of one’s overall life circumstances and serves as a proximal indicator of subjective well-being [3,8]. Resilience encompasses adaptive capacity in the face of adversity, and coping strategies reflect behavioral regulation in response to stress. From this perspective, depressive outcomes are shaped not only by the presence of single risk or protective factors but also by how these resources cohere and interact, with distal self-evaluations plausibly influencing depression partly through more proximal cognitive appraisals of life [4,13]. Importantly, longitudinal research has demonstrated that depressive symptoms and related aspects of psychological functioning are dynamic processes that evolve, rather than static traits. Cross-lagged and prospective studies indicate that depressive symptoms and broader indicators of psychological functioning show reciprocal and time-dependent associations, with substantial heterogeneity across developmental stages and population groups. For example, longitudinal evidence from cross-lagged panel designs suggests that the strength and direction of associations between depressive symptoms and functional outcomes may vary across individuals and contexts, underscoring the complexity of these relationships [16].
Although these psychological constructs have each been investigated in relation to depression, there is a notable gap in the literature regarding their theoretically grounded combined and mediational effects. Few studies have simultaneously evaluated self-esteem, life satisfaction, resilience, and coping strategies within the same analytic framework, particularly in clinical adult populations. Moreover, whether self-esteem exerts its influence on depression directly or indirectly through life satisfaction remains insufficiently addressed, especially in non-Western and collectivist contexts.
Building on this theoretical framework, the study hypotheses were informed by established models of subjective well-being and cognitive appraisal. Within this perspective, self-esteem can be conceptualized as a relatively distal self-evaluative resource, whereas life satisfaction represents a more proximal cognitive evaluation of overall life quality and is more directly associated with emotional outcomes, including depressive symptoms. Accordingly, self-esteem was expected to be associated with depression both directly and indirectly through life satisfaction. In contrast, resilience was conceptualized as an adaptive capacity that may exert a more immediate and direct protective effect against depression, rather than operating primarily through global life evaluations. This hierarchical conceptualization guided the mediation pathways examined in the present study [4,8].
The present study was designed to address these gaps by examining the interplay between self-esteem, life satisfaction, resilience, and coping strategies in adults with and without depression. By integrating comparative analyses, logistic regression, and mediation models, we sought to clarify both the direct and indirect associations of these constructs with depression presence and severity.
We hypothesized that: (Hypothesis 1) Participants with depression would report lower self-esteem, life satisfaction, and resilience, and show differences in coping strategies compared to healthy controls. (Hypothesis 2) Life satisfaction and resilience would emerge as the strongest protective factors against depression. (Hypothesis 3) The relationship between self-esteem and depression would be partially mediated by life satisfaction. (Hypothesis 4) Maladaptive coping (emotion-focused and avoidant) would be associated with higher depression severity, whereas problem-focused coping would show weaker or non-significant associations.
By testing these hypotheses, this study aims to provide a comprehensive assessment of protective psychological resources in depression, highlight the mediational role of life satisfaction, and contribute to a multidimensional understanding of factors associated with depression severity.
This was an analytical cross-sectional study conducted between May and September 2025 at the Psychiatry Outpatient Clinics of Mugla Training and Research Hospital. The study aimed to compare self-esteem, life satisfaction, coping strategies, and psychological resilience between individuals with and without depression, and to examine correlations and mediation effects among these variables.
The study protocol was reviewed and approved by the Mugla Sıtkı Koçman University Medical and Health Sciences Ethics Committee (Approval No: 250060/86, Date: 16/04/2025). All procedures were carried out in accordance with the ethical standards of the Helsinki Declaration.
The sample consisted of patients diagnosed with major depressive disorder (MDD) and healthy controls, aged 18–65 years. An a priori power analysis (effect size = 0.25, α = 0.05, power = 0.99) using G*Power 3.1.2 indicated a minimum of 148 participants per group. To account for 1:1 matching and an anticipated 30% exclusion rate among controls, the final target sample size was set at ≥148 patients with MDD and ≥192 controls (total ≥340 participants).
Depression diagnoses were established using the Structured Clinical Interview for DSM-5 (SCID-5), whereas healthy controls were confirmed to have no psychiatric diagnosis through the same structured interview.
Inclusion Criteria:
MDD group: (1) age 18–65 years, (2) adequate literacy and cognitive capacity to complete questionnaires, (3) no psychotropic medication use within the last month, and (4) fulfillment of DSM-5 diagnostic criteria for MDD as assessed by the Structured Clinical Interview for DSM-5 (SCID-5).
Control group: (1) age 18–65 years, (2) adequate literacy and cognitive capacity, (3) no current psychiatric diagnosis or treatment, and (4) absence of psychiatric disorders confirmed through SCID-5.
Exclusion Criteria (both groups): (1) severe physical illness affecting quality of life, (2) current use of psychotropic medication, and (3) insufficient literacy or cognitive ability to complete the study instruments.
Patients meeting the inclusion criteria and providing consent were evaluated by a psychiatrist using the SCID-5. After diagnostic confirmation, participants completed the study instruments in a quiet setting under supervision. Healthy controls were recruited among hospital staff, patients’ relatives, and companions from other clinics. Each underwent an SCID-5 interview to rule out psychiatric disorders before completing the same battery of instruments under comparable conditions.
All participants completed the full assessment battery under supervision. No questionnaires were excluded due to missing data, incomplete responses, or invalid answer patterns. The only exclusions in the analytic sample occurred during the propensity score matching (PSM) procedure, where unmatched control participants were removed.
All scales are self-administered and widely validated for use in Turkish populations.
2.4.1 Structured Clinical Interview for DSM-5 (SCID-5)
A semi-structured diagnostic interview is used to confirm psychiatric diagnoses according to DSM-5 criteria. The Turkish adaptation has demonstrated good reliability [17].
2.4.2 Sociodemographic Data Form
The research team designed this form to collect sociodemographic and clinical information, including age, gender, marital status, educational level, income, psychiatric background, and prior treatment history.
2.4.3 Rosenberg Self-Esteem Scale (RSES)
Developed by Rosenberg [18], it is widely used to assess global self-esteem. The Turkish version was validated by Çuhadaroğlu [19]. In this study, each of the 10 items was rated on a 4-point scale (0–3), with higher total scores indicating lower self-esteem. For ease of interpretation, mean scores were calculated, ranging from 0 to 3. In the present study, the internal consistency of the scale was satisfactory, with a Cronbach’s alpha coefficient of 0.82.
A 28-item short form developed by Carver (1997) to assess coping strategies [20]. It evaluates problem-focused, emotion-focused, and avoidant coping. Turkish adaptation was conducted by Bacanlı et al. [21]. Each item is scored on a 4-point Likert scale ranging from 1 (“I haven’t been doing this at all”) to 4 (“I’ve been doing this a lot”). Subscale scores are obtained by summing relevant items, with higher scores reflecting greater use of the corresponding coping strategy. In the present study, Cronbach’s alpha coefficients were 0.79 for problem-focused coping, 0.81 for emotion-focused coping, and 0.74 for avoidant coping.
2.4.5 Brief Resilience Scale (BRS)
A 6-item scale developed by Smith et al. [22] to assess the ability to recover from stress. The Turkish version was validated by Doğan [23]. Items are rated on a 5-point scale from 1 (“Strongly disagree”) to 5 (“Strongly agree”). Three items are reverse-scored, and then all items are averaged. Higher mean scores indicate greater resilience. For descriptive and analytical purposes, summed scores were used in group comparisons. The scale demonstrated good internal consistency in this study, with a Cronbach’s alpha of 0.85.
2.4.6 Satisfaction with Life Scale (SWLS)
A 5-item scale developed by Diener et al. [24], to measure global life satisfaction. The Turkish adaptation was validated by Köker [25]. Each item is rated on a 7-point Likert scale (1 = “Strongly disagree”, 7 = “Strongly agree”). Scores range from 5 to 35, with higher scores reflecting greater life satisfaction. In the current sample, the Cronbach’s alpha coefficient was 0.88, indicating high internal consistency.
2.4.7 Beck Depression Inventory (BDI)
A 21-item scale developed by Beck et al. [26] to assess depressive symptoms. The Turkish version was validated by Hisli [27]. Each item is scored on a 0–3 scale, with higher total scores indicating greater symptom severity. For this study, BDI scores were categorized into three levels: mild depression (10–16), moderate depression (17–29), and severe depression (30–63). In the present study, the internal consistency of the BDI was high, with a Cronbach’s alpha coefficient of 0.90.
All statistical procedures were carried out using SPSS software (version 27.0; IBM Corp., Armonk, NY, USA), while R software (version 4.5.1; R Foundation for Statistical Computing, Vienna, Austria) was utilized for PSM and mediation analyses. PSM was performed using the MatchIt package, and mediation analyses were conducted using the mediation package in R. The distribution of continuous variables was evaluated using the Kolmogorov-Smirnov test. Group differences were examined with independent-samples t-tests when normality assumptions were met, and with Mann-Whitney U tests when distributions deviated from normality; categorical variables were analyzed using chi-square tests. Differences among levels of depression severity were assessed using one-way analysis of variance (ANOVA) or the Kruskal–Wallis test, as appropriate. When the Kruskal–Wallis test indicated significant group differences, post-hoc comparisons were performed using Dunn’s test with Bonferroni correction. Effect sizes were calculated as Cohen’s r for binary group comparisons and eta squared (η2) for comparisons involving more than two groups. Descriptive data were presented as mean ± standard deviation, median with interquartile range, or number and percentage, depending on variable type. Statistical significance was defined as a two-sided p-value below 0.05.
To minimize selection bias, PSM was performed to balance age, sex, and education between the MDD and control groups. Propensity scores were estimated using logistic regression, and 1:1 nearest-neighbor matching without replacement was applied. Participants who could not be matched were excluded from further analyses.
Predictors of depression were explored using logistic regression models, with results reported as odds ratios (ORs) accompanied by 95% confidence intervals (CIs). Subsequently, mediation analyses were conducted to investigate whether life satisfaction mediated the relationships between self-esteem, resilience, and depression. Indirect effects were evaluated using a bootstrapping approach with 5000 resamples, and bias-corrected 95% confidence intervals were calculated.
Initially, 350 individuals were assessed for eligibility between April and September 2025, including 158 patients diagnosed with MDD and 192 healthy controls. Following PSM based on age, sex, and education, 39 control participants could not be matched and were excluded. The final analytic sample, therefore, consisted of 311 participants: 158 individuals with MDD and 153 healthy controls (Fig. 1).
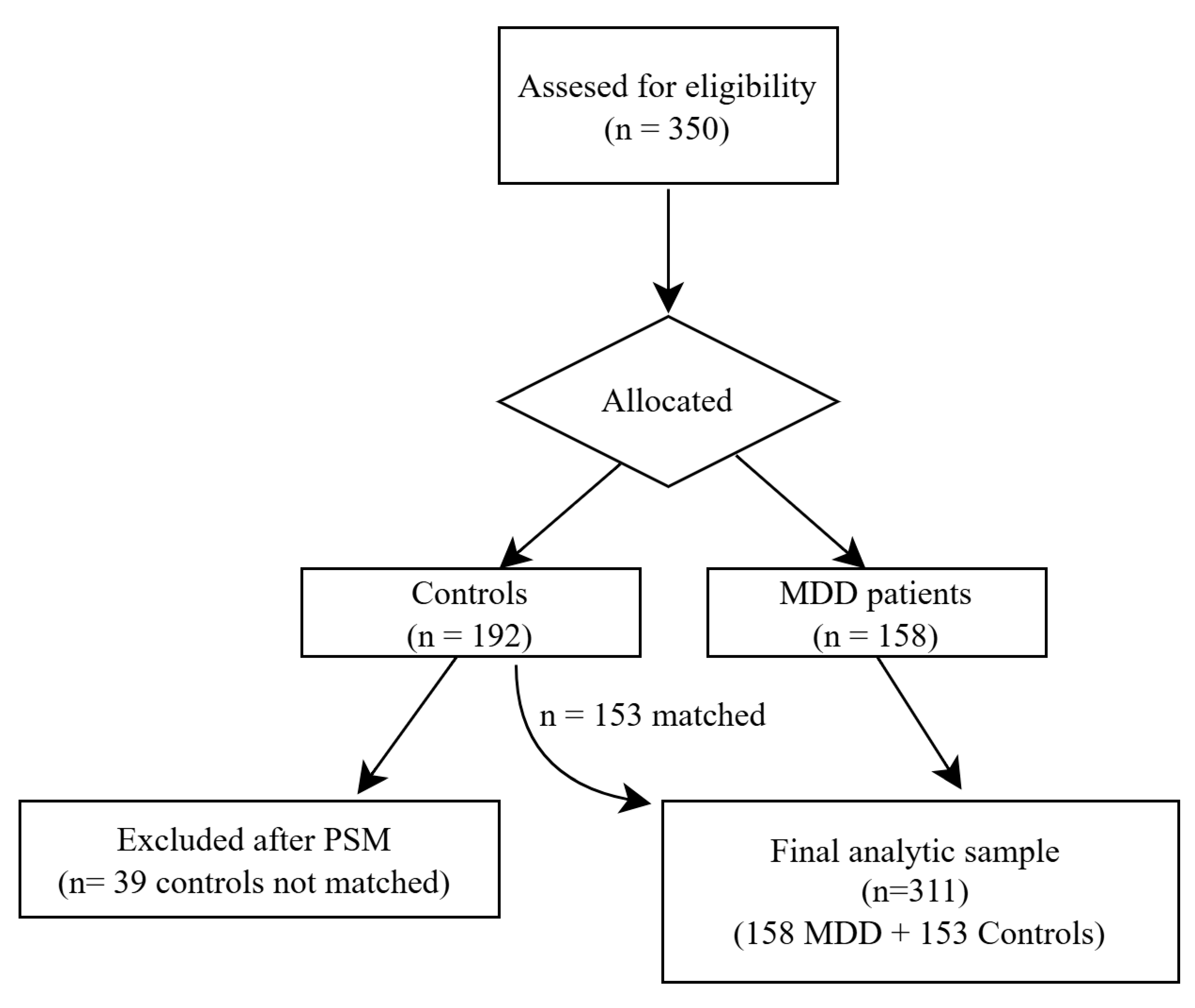
Figure 1: Flow diagram of participant recruitment, eligibility, and final sample analyzed.
The mean age was 39.6 years (SD = 10.9) in the MDD group and 38.8 years (SD = 11.2) in the control group, with no significant difference between groups (p = 0.51). Gender distribution was comparable, with women comprising 55.2% of the MDD group and 55.4% of the control group (p = 0.93). Educational attainment did not differ significantly between groups (p = 0.64), with high school education being the most common level, followed by university and postgraduate education (Table 1).
Comparisons of psychological variables showed that individuals with MDD reported significantly higher depressive symptom severity and significantly lower life satisfaction and psychological resilience compared to healthy controls (all p < 0.001), whereas no statistically significant group difference was observed for self-esteem (p = 0.086) (Table 1).
Table 1: Demographic, clinical, and psychological characteristics of participants.
| Variable | MDD (n = 158) | Control (n = 153) | Test Statistic | p-Value | Effect Size (r) |
|---|---|---|---|---|---|
| Age (years), mean ± SD | 39.6 ± 10.9 | 38.8 ± 11.2 | t = 0.65 | 0.51 | — |
| Female, n (%) | 87 (55.2) | 85 (55.4) | χ2 = 0.01 | 0.93 | — |
| Education, n (%) | χ2 = 0.89 | 0.64 | — | ||
| High school | 71 (44.9) | 66 (43.1) | |||
| University | 55 (34.8) | 57 (37.3) | |||
| Postgraduate | 32 (20.3) | 30 (19.6) | |||
| Psychological scales | |||||
| BDI, mean ± SD | 20.11 ± 8.25 | 10.76 ± 5.80 | t = 12.4 | <0.001 | 0.42 |
| SWLS, mean ± SD | 17.85 ± 5.72 | 21.67 ± 6.10 | t = −5.6 | <0.001 | 0.25 |
| BRS, mean ± SD | 15.95 ± 4.55 | 18.68 ± 4.90 | t = −5.2 | <0.001 | 0.23 |
| RSES, mean ± SD | 0.74 ± 0.45 | 0.64 ± 0.41 | t = 1.72 | 0.086 | 0.10 |
| Brief COPE subscales | |||||
| Problem-focused coping, mean ± SD | 18.9 ± 4.7 | 19.3 ± 4.2 | t = −0.65 | 0.51 | 0.04 |
| Emotion-focused coping, mean ± SD | 31.2 ± 6.9 | 35.6 ± 6.5 | t = −6.0 | <0.001 | 0.32 |
| Avoidant coping, mean ± SD | 19.9 ± 5.0 | 19.2 ± 4.9 | t = 1.2 | 0.22 | 0.07 |
Within the MDD group, 53 participants (33.5%) were classified as having mild depression, 58 (36.7%) moderate depression, and 47 (29.8%) severe depression according to Beck Depression Inventory cut-off scores. Life satisfaction differed significantly across severity groups, showing a graded decline from controls to severe depression, with a large effect size (η2 = 0.33) (Table 2).
Table 2: Life satisfaction (SWLS) scores across groups.
| Group | Mean ± SD | H | p-Value | η2 | Pairwise Comparisons |
|---|---|---|---|---|---|
| Controls (n = 153) | 24.69 ± 5.82 | — | — | — | — |
| Mild depression (n = 53) | 20.11 ± 5.60 | — | — | — | — |
| Moderate depression (n = 58) | 15.33 ± 5.12 | — | — | — | — |
| Severe depression (n = 47) | 13.92 ± 4.88 | 103.9 | <0.001 | 0.33 | Controls > Mild > Moderate > Severe* |
Self-esteem scores also differed significantly across severity levels, with RSES scores increasing progressively from mild to severe depression, indicating lower self-esteem with increasing depression severity (η2 = 0.24) (Table 3).
Table 3: Self-esteem (RSES) scores across groups.
| Group | Mean ± SD | H | p-Value | η2 | Pairwise Comparisons |
|---|---|---|---|---|---|
| Controls (n = 153) | 0.52 ± 0.35 | — | — | — | — |
| Mild depression (n = 53) | 0.51 ± 0.38 | — | — | — | — |
| Moderate depression (n = 58) | 0.73 ± 0.42 | — | — | — | — |
| Severe depression (n = 47) | 1.17 ± 0.50 | 77.4 | <0.001 | 0.24 | Controls & Mild < Moderate < Severe* |
Coping strategies varied across severity groups (Table 4). Problem-focused coping did not differ significantly, whereas emotion-focused coping decreased significantly with increasing depression severity, with large group differences (η2 = 0.14). Avoidant coping showed a small but significant difference, with higher scores observed in the severe depression group compared to controls.
Table 4: Coping strategies across groups.
| Coping Style | Control (n = 153), Mean ± SD | Mild Depression (n = 53), Mean ± SD | Moderate Depression (n = 58), Mean ± SD | Severe Depression (n = 47), Mean ± SD | H | p-Value | η2 | Pairwise Comparisons |
|---|---|---|---|---|---|---|---|---|
| Problem-focused | 19.1 ± 4.2 | 19.4 ± 4.5 | 18.5 ± 4.7 | 18.6 ± 4.8 | 3.21 | 0.359 | 0.01 | Not significant |
| Emotion-focused | 35.6 ± 6.5 | 34.1 ± 6.2 | 31.4 ± 6.8 | 29.4 ± 6.9 | 27.8 | <0.001 | 0.14 | Controls > Mild > Moderate = Severe* |
| Avoidant | 19.2 ± 4.9 | 19.6 ± 5.1 | 19.2 ± 4.8 | 20.1 ± 5.0 | 8.1 | 0.034 | 0.03 | Severe > Controls† |
Multivariate logistic regression analysis identified lower life satisfaction (OR = 0.95, p = 0.004) and lower resilience (OR = 0.92, p = 0.002) as significant independent predictors of depression status, while self-esteem and coping strategy subscales were not significant predictors after adjustment (Table 5).
Table 5: Multivariate logistic regression predicting depression (MDD vs. control).
| Predictor | OR | 95% CI | p-Value |
|---|---|---|---|
| Life satisfaction (SWLS) | 0.95 | 0.92–0.98 | 0.004 |
| Resilience (BRS) | 0.92 | 0.88–0.97 | 0.002 |
| Self-esteem (RSES) | 1.12 | 0.83–1.51 | 0.463 |
| Problem-focused coping (COPE_PF) | 0.98 | 0.94–1.03 | 0.482 |
| Emotion-focused coping (COPE_EF) | 1.01 | 0.98–1.04 | 0.692 |
| Avoidant coping (COPE_AV) | 1.05 | 0.99–1.11 | 0.088 |
Mediation analyses indicated that the association between resilience and depression was primarily direct, with no statistically significant indirect effect via life satisfaction (p = 0.402). In contrast, life satisfaction significantly mediated the relationship between self-esteem and depression, accounting for approximately 24% of the total effect (Table 6). These mediation pathways are illustrated in Fig. 2.
Table 6: Mediation analysis of self-esteem, resilience, and life satisfaction on depression.
| Model | Total Effect | Direct Effect | Indirect Effect | Proportion Mediated |
|---|---|---|---|---|
| Resilience (BRS) → Life satisfaction (SWLS) → Depression (BDI) | −1.26 (p = 0.002) | −0.95 (p < 0.001) | −0.31 (p = 0.402) | 23.6% |
| Self-esteem (RSES) → Life satisfaction (SWLS) → Depression (BDI) | 14.53 (p < 0.001) | 11.07 (p < 0.001) | 3.46 (p < 0.001) | 23.8%* |
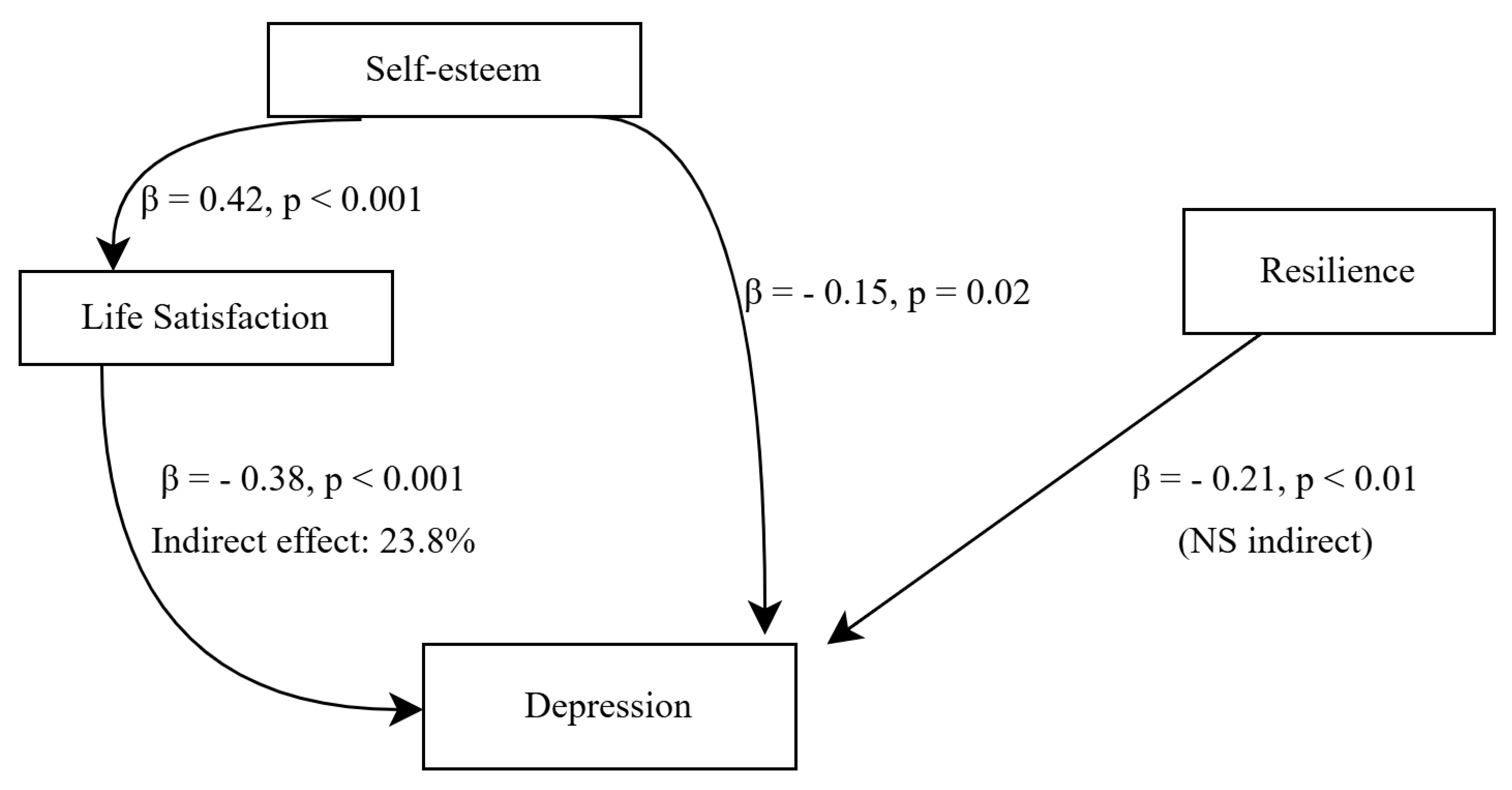
Figure 2: Mediation model of self-esteem, life satisfaction, resilience, and depression. Note: Higher self-esteem was associated with greater life satisfaction, which in turn predicted lower depression scores. Life satisfaction significantly mediated the relationship between self-esteem and depression, accounting for 23.8% of the total effect. Resilience showed a significant direct effect on depression, but no significant indirect effect through life satisfaction. Path coefficients (β) and p-values are displayed on the arrows. NS indicates a non-significant indirect effect.
The present study examined the interrelationships among self-esteem, life satisfaction, resilience, and coping strategies in individuals with and without MDD, with the aim of testing a set of predefined hypotheses. Overall, the findings largely supported the proposed hypotheses. In partial support of Hypothesis 1, individuals with depression reported significantly lower life satisfaction and resilience and showed differences in coping strategies compared to healthy controls; however, self-esteem did not differ significantly between groups. Consistent with Hypothesis 2, life satisfaction and resilience emerged as the strongest protective factors against depression. Hypothesis 3 was supported, as life satisfaction partially mediated the relationship between self-esteem and depression. Finally, Hypothesis 4 received partial support: maladaptive coping strategies, particularly avoidant coping, were associated with greater depression severity, whereas problem-focused coping did not emerge as protective. Together, these findings provide an integrative framework clarifying the distinct and interacting roles of psychological resources and coping processes in depression. Building on these overall findings, one of the most notable results of the present study was the mediating role of life satisfaction in the relationship between self-esteem and depression. Approximately one-quarter of the total effect of self-esteem on depressive symptoms was explained by life satisfaction, supporting previous models of subjective well-being as a cognitive appraisal mechanism that integrates personal traits with environmental conditions [4,11]. Longitudinal studies indicate that life satisfaction predicts a lower incidence of depressive symptoms over time [5], and meta-analytic evidence has confirmed its protective role across diverse populations, particularly in adolescent and young adult populations [12]. These findings underscore the clinical relevance of interventions that directly target life satisfaction. Positive psychology interventions, such as gratitude training, savoring, and meaning-oriented therapies, have demonstrated moderate-to-large effects on both well-being and depressive symptoms [28,29]. Taken together, the present findings suggest that life satisfaction may represent a modifiable therapeutic target that bridges self-appraisals and long-term outcomes.
Resilience emerged as a robust independent protective factor. Unlike self-esteem, its effect was not mediated by life satisfaction, which highlights the unique contribution of resilience to depression. Systematic reviews and meta-analyses consistently show that resilience is moderately and negatively associated with depression and other mood symptoms [3,12]. The lack of mediation suggests that resilience protects against depression through direct adaptive mechanisms, including stress-response regulation, cognitive flexibility, and social connectedness. Neurobiological research has linked resilience to more efficient hypothalamic–pituitary–adrenal axis functioning and reduced inflammatory reactivity to stress [3,14]. Importantly, resilience is not a static trait; intervention studies demonstrate that resilience-building programs in schools, workplaces, and clinical settings produce sustained improvements in resilience and reductions in depressive symptoms [28,30]. These converging findings support the prioritization of resilience-focused strategies in both preventive and clinical contexts.
Contrary to traditional assumptions, self-esteem alone did not differ significantly between depressed and non-depressed groups (Table 1). However, when depression severity was considered, self-esteem scores progressively increased from mild to severe groups (Table 3). Given that higher scores on the RSES indicate lower self-esteem, this pattern reflects a decline in self-esteem as depression severity worsens. Importantly, mediation analysis demonstrated that the impact of self-esteem on depression was largely indirect, operating through life satisfaction. This is consistent with recent studies showing that depression can mediate the relationship between self-esteem and other psychological outcomes, such as eating behavior [7,11], suggesting that self-esteem’s influence may operate through intermediary processes. Clinically, these findings suggest that self-esteem enhancement should not be pursued as an isolated therapeutic goal. Instead, interventions should ensure that improvements in self-worth translate into enduring positive life evaluations in order to yield meaningful clinical benefits.
Coping strategies revealed differentiated associations across depression severity. Maladaptive components of emotion-focused coping, particularly rumination and self-blame, were associated with higher depression severity, in line with previous work identifying maladaptive emotion regulation as a risk factor [15,31]. Interestingly, emotion-focused coping decreased with severity, possibly reflecting emotional blunting or withdrawal processes in severe depression. Avoidant coping showed a small but significant increase in severe cases, consistent with its role in maintaining symptoms. Surprisingly, problem-focused coping was not protective, which may be explained by the “fit hypothesis” that coping effectiveness depends on stressor controllability [15,32]. Since depressive stressors are often internal and less controllable, problem-focused strategies may not yield benefits in this context. Interventions such as rumination-focused cognitive-behavioral therapy (RFCBT) and acceptance and commitment therapy (ACT) have demonstrated efficacy in reducing maladaptive coping and improving psychological flexibility [33,34]. These approaches may help patients adaptively match coping strategies to the controllability of stressors.
The cultural context also provides insight into the observed findings. In collectivist societies such as Turkiye, relational well-being and global evaluations of life may play a stronger role in predicting mental health outcomes compared to individual-focused constructs like self-esteem. Cross-cultural studies indicate that self-esteem has a weaker protective role in interdependent contexts, whereas life satisfaction and social connectedness are stronger predictors [8,35]. This perspective helps explain why life satisfaction, rather than self-esteem, emerged as the central factor in this sample. Future research should test cultural moderators, including family cohesion, community integration, and interdependent values, to clarify how protective resources operate across societies.
The clinical implications of this study are noteworthy. Interventions for depression should extend beyond symptom reduction to actively cultivate psychological resources. In particular, approaches that enhance overall well-being, strengthen resilience, and address maladaptive coping patterns may be especially beneficial. At the policy level, public health initiatives that improve quality of life, reduce social inequality, and strengthen social support systems may help reduce population-level depression risk.
This study has several methodological strengths. Diagnostic accuracy was ensured through structured clinical interviews (SCID-5), and PSM was applied to balance key sociodemographic variables between groups. The relatively large and well-matched sample increases confidence in the findings, and mediation analyses with bootstrapping provided robust estimates of indirect effects.
Nevertheless, several limitations should be acknowledged. First, the cross-sectional design precludes causal inference among the examined variables. Second, all psychological constructs were assessed using self-report measures, which may introduce common method bias as well as recall or social desirability effects, potentially inflating observed associations despite the use of validated instruments and supervised data collection. Third, coping strategies were assessed independently of specific situational contexts, which may limit interpretation regarding coping flexibility. Finally, the single-center nature of the study conducted in Turkiye may restrict the generalizability of the findings to other cultural or clinical settings.
In addition, although the present study examined mediation pathways across the overall sample, it did not formally test whether these mechanisms differed between clinical and non-clinical groups. Future research could extend these findings by using moderated mediation or network-based analytic approaches to examine whether the structure and strength of these relationships vary as a function of diagnostic status. Such analyses were beyond the scope of the current study but represent important directions for future research.
From a practical perspective, the present findings have implications for preventive and intervention-oriented mental health practices. Psychological resources such as life satisfaction, resilience, and adaptive coping skills are potentially modifiable targets that can be incorporated into preventive programs and psychosocial interventions. In line with recent developments in digital mental health, artificial intelligence–supported tools may offer novel opportunities to identify individuals at risk and to deliver personalized, scalable interventions. For example, AI-based screening systems and digital platforms integrating self-report data with behavioral indicators could potentially help monitor changes in well-being and resilience over time, while delivering tailored psychoeducational or skills-based interventions [36], although further empirical validation of such approaches remains necessary.
In conclusion, this study demonstrates that life satisfaction and resilience are distinct but complementary protective factors against depression, with self-esteem exerting an indirect effect through life satisfaction. Coping strategies contribute in more complex ways, with maladaptive emotion-focused and avoidant coping linked to greater severity. By demonstrating the mediating role of life satisfaction and the independent contribution of resilience, this study offers an integrative framework that links psychological resources with depression across clinical contexts, while highlighting the potential relevance of cultural factors. Clinically, these results suggest that integrative interventions combining resilience training, positive psychology, and coping flexibility enhancement may inform the development of strategies aimed at mitigating depression risk.
Acknowledgement:
Funding Statement: The authors received no specific funding for this study.
Author Contributions: The authors confirm contribution to the paper as follows: study conception and design: Mahmut Selçuk, Fulden Cantaş Türkiş, Fatma Taşkın Koca, Volkan Dizman, Sevilay Yerlikaya Boz; data collection: Mahmut Selçuk, Fatma Taşkın Koca, Volkan Dizman, Sevilay Yerlikaya Boz; analysis and interpretation of results: Mahmut Selçuk, Fulden Cantaş Türkiş; draft manuscript preparation: Mahmut Selçuk. All authors reviewed and approved the final version of the manuscript.
Availability of Data and Materials: The datasets generated and analyzed during the current study can be obtained from the corresponding author, upon reasonable request.
Ethics Approval: The study protocol was reviewed and approved by the Mugla Sıtkı Koçman University Medical and Health Sciences Ethics Committee (Approval No: 250060/86, Date: 16/04/2025). All procedures were carried out in accordance with the ethical standards of the Helsinki Declaration.
Informed Consent: All individuals were provided with detailed information regarding the aims and procedures of the study, and written informed consent was secured before their inclusion.
Conflicts of Interest: The authors declare no conflicts of interest.
Abbreviations
| ACT | Acceptance and Commitment Therapy |
| ANOVA | Analysis of Variance |
| BDI | Beck Depression Inventory |
| BRS | Brief Resilience Scale |
| CI | Confidence Interval |
| DSM-5 | Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition |
| H | Kruskal–Wallis H statistic |
| MDD | Major Depressive Disorder |
| OR | Odds Ratio |
| PSM | Propensity Score Matching |
| RFCBT | Rumination-Focused Cognitive Behavioral Therapy |
| RSES | Rosenberg Self-Esteem Scale |
| SCID-5 | Structured Clinical Interview for DSM-5 |
| SWLS | Satisfaction with Life Scale |
| η2 | Eta squared |
References
1. Zhou J , Zhang Y , He S , Xu S , Sun Q , Zhao T , et al. Accelerated global burden of depressive disorders during the COVID-19 pandemic from 2019 to 2021. Sci Rep. 2025; 15( 1): 9529. doi:10.1038/s41598-025-93923-4. [Google Scholar] [CrossRef]
2. WHO . Depression [Internet]. Geneva, Switzerland: World Health Organization; 2025 [cited 2026 Jan 1]. Available from: https://www.who.int/news-room/fact-sheets/detail/depression. [Google Scholar]
3. Imran A , Tariq S , Kapczinski F , de Azevedo Cardoso T . Psychological resilience and mood disorders: a systematic review and meta-analysis. Trends Psychiatry Psychother. 2024; 46: e20220524. doi:10.47626/2237-6089-2022-0524. [Google Scholar] [CrossRef]
4. Almeida D , Monteiro D , Rodrigues F . Satisfaction with life: mediating role in the relationship between depressive symptoms and coping mechanisms. Healthcare. 2021; 9( 7): 787. doi:10.3390/healthcare9070787. [Google Scholar] [CrossRef]
5. Chang YH , Yang CT , Hsieh S . Social support enhances the mediating effect of psychological resilience on the relationship between life satisfaction and depressive symptom severity. Sci Rep. 2023; 13( 1): 1– 8. doi:10.1038/S41598-023-31863-7. [Google Scholar] [CrossRef]
6. Prieto-Vila M , Estupiñá FJ , Cano-Vindel A . Risk factors associated with relapse in major depressive disorder in primary care patients: a systematic review. Psicothema. 2021; 33( 1): 44– 52. doi:10.7334/psicothema2020.186. [Google Scholar] [CrossRef]
7. Awad E , Malaeb D , Chammas N , Fawaz M , Soufia M , Hallit S , et al. Mediating effect of depression between self-esteem, physical appearance comparison and intuitive eating in adults. Sci Rep. 2024; 14( 1): 25109. doi:10.1038/S41598-024-77016-2. [Google Scholar] [CrossRef]
8. Diener E , Oishi S , Tay L . Advances in subjective well-being research. Nat Hum Behav. 2018; 2( 4): 253– 60. doi:10.1038/s41562-018-0307-6. [Google Scholar] [CrossRef]
9. Heine S , Lehman D , Markus HR , Kitayama S . Is there a universal need for positive self-regard? Psychol Rev. 1999; 106( 4): 766. doi:10.1037/0033-295X.106.4.766. [Google Scholar] [CrossRef]
10. Lin H , Zhu Y , Liu Q , Li S . The mediating effect of resilience between physical activity and mental health: a meta-analytic structural equation modeling approach. Front Public Health. 2024; 12: 1434624. doi:10.3389/fpubh.2024.1434624. [Google Scholar] [CrossRef]
11. Martins V , Serrão C , Teixeira A , Castro L , Duarte I . The mediating role of life satisfaction in the relationship between depression, anxiety, stress and burnout among Portuguese nurses during COVID-19 pandemic. BMC Nurs. 2022; 21( 1): 188. doi:10.1186/S12912-022-00958-3. [Google Scholar] [CrossRef]
12. Luo S , Hu J , Zhang J , Mei Z , Tang Z , Luo S . The correlation between resilience and mental health of adolescents and young adults: a systematic review and meta-analysis. Front Psychiatry. 2025; 16: 1536553. doi:10.3389/fpsyt.2025.1536553. [Google Scholar] [CrossRef]
13. Usán Supervía P , Salavera Bordás C , Quílez Robres A . The mediating role of self-esteem in the relationship between resilience and satisfaction with life in adolescent students. Psychol Res Behav Manag. 2022; 15: 1121– 9. doi:10.2147/prbm.s361206. [Google Scholar] [CrossRef]
14. Kalisch R , Russo SJ , Müller MB . Neurobiology and systems biology of stress resilience. Physiol Rev. 2024; 104( 3): 1205– 63. doi:10.1152/physrev.00042.2023. [Google Scholar] [CrossRef]
15. Cheng C , Lau HPB , Chan MPS . Coping flexibility and psychological adjustment to stressful life changes: a meta-analytic review. Psychol Bull. 2014; 140( 6): 1582– 607. doi:10.1037/A0037913. [Google Scholar] [CrossRef]
16. Cao X , Liu X . Effect of depressive symptoms and learning difficulty on academic achievement among adolescents in china: a cross-lagged panel study. Int J Psychol. 2025; 60( 6): e70113. doi:10.1002/ijop.70113. [Google Scholar] [CrossRef]
17. Elbir M , Alp Topbas O , Bayad S , Kocabas T , Topak OZ , Cetin S , et al. Adaptation and reliability of the structured clinical ınterview for DSM-5-disorders—clinician version (SCID-5/CV) to the Turkish language. Turk Psikiyatri Derg. 2019; 30( 1): 51– 6. doi:10.5080/u23431. [Google Scholar] [CrossRef]
18. Rosenberg M . Society and the adolescent self-image. Princeton, NJ, USA: Princeton University Press; 1965. [Google Scholar]
19. Çuhadaroğlu F . Adolescents’ self-esteem: a study of related factors [ dissertation]. Ankara, Turkiye: Hacettepe University; 1986. [Google Scholar]
20. Carver CS . You want to measure coping but your protocol’ too long: Consider the brief cope. Int J Behav Med. 1997; 4: 92– 100. doi:10.1207/s15327558ijbm0401_6. [Google Scholar] [CrossRef]
21. Bacanlı H , Sürücü M , İlhan T . Başa çıkma stilleri ölçeği kısa formunun (BÇSÖ-KF) psikometrik özelliklerinin incelenmesi: geçerlik ve güvenirlik çalışması. Kuram ve Uygulamada Eğitim Bilimleri. 2013; 13( 1): 81– 96. (In Turkish). [Google Scholar]
22. Smith BW , Dalen J , Wiggins K , Tooley E , Christopher P , Bernard J . The brief resilience scale: assessing the ability to bounce back. Int J Behav Med. 2008; 15( 3): 194– 200. doi:10.1080/10705500802222972. [Google Scholar] [CrossRef]
23. Doğan T . Adaptation of the brief resilience scale into Turkish: a validity and reliability study. J Happiness Well-Being. 2015; 3( 1): 93– 102. [Google Scholar]
24. Diener E , Emmons RA , Larsem RJ , Griffin S . The satisfaction with life scale. J Pers Assess. 1985; 49( 1): 71– 5. doi:10.1207/s15327752jpa4901_13. [Google Scholar] [CrossRef]
25. Köker S . Comparison of life satisfaction levels of normal and problematic adolescents [ master’s thesis]. Ankara, Turkiye: Ankara University; 1991. [Google Scholar]
26. Beck AT . An inventory for measuring depression. Arch Gen Psychiatry. 1961; 4( 6): 561– 71. doi:10.1001/archpsyc.1961.01710120031004. [Google Scholar] [CrossRef]
27. Hisli N . Beck Depresyon Envanterinin Üniversite Öğrencileri İçin Geçerliği, Güvenirliği. Psikoloji Dergisi. 1989; 7( 23): 3– 13. (In Turkish). [Google Scholar]
28. Sin NL , Lyubomirsky S . Enhancing well-being and alleviating depressive symptoms with positive psychology interventions: a practice-friendly meta-analysis. J Clin Psychol. 2009; 65( 5): 467– 87. doi:10.1002/jclp.20593. [Google Scholar] [CrossRef]
29. Chakhssi F , Kraiss JT , Sommers-Spijkerman M , Bohlmeijer ET . The effect of positive psychology interventions on well-being and distress in clinical samples with psychiatric or somatic disorders: a systematic review and meta. BMC Psychiatry. 2018; 18( 1): 211. doi:10.1186/S12888-018-1739-2. [Google Scholar] [CrossRef]
30. Robertson IT , Cooper CL , Sarkar M , Curran T . Resilience training in the workplace from 2003 to 2014: a systematic review. J Occup Organ Psychol. 2015; 88( 3): 533– 62. doi:10.1111/joop.12120. [Google Scholar] [CrossRef]
31. Crisan SM , Nechita DM . Maladaptive emotion regulation strategies and trait anger as predictors of depression severity. Clin Psychol Psychother. 2022; 29( 3): 1135– 43. doi:10.1002/cpp.2702. [Google Scholar] [CrossRef]
32. Lazarus RS , Folkman S . Stress, appraisal, and coping. Berlin/Heidelberg, Germany: Springer; 1984. [Google Scholar]
33. Langenecker SA , Westlund Schreiner M , Bessette KL , Roberts H , Thomas L , Dillahunt A , et al. Rumination-focused cognitive behavioral therapy reduces rumination and targeted cross-network connectivity in youth with a history of depression: replication in a preregistered randomized clinical trial. Biol Psychiatry Glob Open. 2024; 4( 1): 1– 10. doi:10.1016/j.bpsgos.2023.08.012. [Google Scholar] [CrossRef]
34. Hayes S , Strosahl K , Wilson K . Acceptance and commitment therapy: the process and practice of mindful change. 2nd ed. New York, NY, USA: Guilford Press; 2011. [Google Scholar]
35. Oishi S , Diener E . Goals, culture, and subjective well-being. Pers Soc Psychol Bull. 2001; 27( 12): 1674– 82. doi:10.1177/01461672012712010. [Google Scholar] [CrossRef]
36. Liu X-Q , Wang X . Adolescent suicide risk factors and the integration of social-emotional skills in school-based prevention programs. World J Psychiatry. 2024; 14( 4): 494– 506. doi:10.5498/wjp.v14.i4.494. [Google Scholar] [CrossRef]
Cite This Article
 Copyright © 2026 The Author(s). Published by Tech Science Press.
Copyright © 2026 The Author(s). Published by Tech Science Press.This work is licensed under a Creative Commons Attribution 4.0 International License , which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
 Downloads
Downloads
 Citation Tools
Citation Tools