
 Submit a Paper
Submit a Paper Propose a Special lssue
Propose a Special lssue Open Access
Open Access
EDITORIAL
Disharmonious Ventricular Relationship and Topology for the Given Atrioventricular Connections. Contemporary Diagnostic Approach Using 3D Modeling and Printing
1 Department of Diagnostic Imaging, Hospital for Sick Children, University of Toronto, Toronto, Canada
2 Division of Cardiology, Department of Pediatrics, Labatt Family Heart Centre, Hospital for Sick Children, University of Toronto, Toronto, Canada
3 Biosciences Division, Newcastle University, Newcastle-upon-Tyne, UK
* Corresponding Author: Shi-Joon Yoo. Email:
Congenital Heart Disease 2022, 17(5), 495-504. https://doi.org/10.32604/chd.2022.021155
Received 05 February 2022; Accepted 01 August 2022; Issue published 06 September 2022
 View Full Text
View Full Text Download PDF
Download PDFAbstract
In the last issue, two case reports separately present examples of the extremely rare and complex congenital heart diseases that show concordant atrioventricular connections to the L-looped ventricles in the presence of situs solitus. Both cases highlight that the relationship between the two ventricles within the ventricular mass is not always harmonious with the given atrioventricular connection. Such disharmony between the connections and relationships requires careful assessment of the three basic facets of cardiac building blocks, namely their morphology, the relationship of their component parts, and their connections with the adjacent segments. 3D imaging and printing can now facilitate an otherwise difficult diagnosis in such complex situations. Rotation of either the 3D images or the models permit accurate assessment of the ventricular topologic pattern by creating the right ventricular en-face septal view, thus facilitating placement of the observer’s hands. As we now emphasize, an alternative approach, which might prove more attractive to imagers, is to rotate the ventricular mass to provide the ventricular apical view, thus permitting determination of the ventricular relationship without using the hands.Graphic Abstract
Keywords
In the last issue of Congenital Heart Disease, Perens et al. [1] and Song et al. [2] separately presented examples of those extremely rare and complex congenital heart diseases that show a disharmonious setting of the ventricular relationship and topology for the given atrioventricular connection. In both cases, three-dimensional (3D) modeling and printing facilitated an otherwise difficult diagnosis. Although the two cases appear distinctly different, they share common features including: first, visceral and atrial situs solitus with right juxtaposition of the atrial appendages, second, concordant connection of the atria to the underlying ventricles, which show an L-loop relationship or left-handed topologic pattern, and third, double outlet right ventricle with a remote perimembranous ventricular septal defect. Previous reports describing the presence of a disharmonious ventricular loop pattern or topology for the given atrioventricular connection are rare [3–5]. These earlier reports were all based either on pathological specimens or two-dimensional imaging. This meant that understanding of the complex relationships as seen in 3D space could be challenging. Both reports in this issue [1,2] used 3D volume rendered images and 3D printed models to clarify the situation. We endorse this approach. In this review, we show how the contemporary approach using 3D modeling and printing has more general implications for the overall understanding of congenitally malformed hearts.
2 Relationships as Opposed to Connections in Sequential Segmental Approach
There are three facets that need to be defined during the sequential segmental approach to congenital heart diseases. These are, first, the morphology of the cardiac chambers and arterial trunks, second, the relationships of their components relative to the bodily coordinates and between themselves relative to the ventricular septum, and third, the connections between the components across the atrioventricular and ventriculoarterial junctions [6]. It is agreed among congenital heart morphologists and physicians that the chambers of the heart are named according to their intrinsic morphology, instead of their locations in space [7]. The right-left relationship of the atria and ventricles to the bodily coordinates is usually in accordance with the right-left relationship between the chambers themselves. On rare occasions, however, the atria, or the ventricles, or both, show unusual spatial relationships to the bodily coordinates while the spatial interrelationship between chambers themselves within the segment is largely maintained. When considering the ventricular segment, the concept of topology or chirality, which we discuss in the next section of our review, is the key to understanding the pathological anatomy. It is subtly different for the components of the arterial segment, which are described according to their anterior-posterior relationships as well as their right-left coordinates. The connections are determined according to the way that the cavities of the components are joined to one another, or in some instances not joined to each other, across the atrioventricular and ventriculoarterial junctions.
In the setting of congenital heart diseases in general, the connections between the atrial and ventricular segments are almost always harmonious with the relationship of the ventricles within the ventricular mass. Concordant atrioventricular connections usually occur with a D-loop ventricular relationship in situs solitus, and with an L-loop ventricular relationship in situs inversus. Discordant atrioventricular connections usually occur with an L-loop ventricular relationship in situs solitus, and with a D-loop ventricular relationship in situs inversus. Traditionally, the descriptors ‘D-loop’ and ‘L-loop’ have been used to describe the right-left relationship of the ventricles in relation to the bodily coordinates, as well as to the ventricles themselves. Although these definitions work well in the majority of cases, determination of the right-left relationship of the ventricles within the ventricular mass becomes difficult when they are superoinferiorly related, or when the atrioventricular connections themselves are twisted or criss-crossing [8–13]. It is acknowledged that the relationship between and the internal anatomy of the ventricles is not changed in these hearts, despite the distorted spatial orientation of the ventricles to the bodily coordinates [8–10]. The concept of “ventricular topology” [8], or “ventricular chirality”, or “handedness” [9,10] was developed in order to address this important feature when examining such complex hearts.
This topology, or chirality, of the ventricular mass specifies the spatial relationship between the two ventricles irrespective of their orientation relative to the bodily coordinates (Fig. 1). The topological arrangement is said to be right-handed when the right ventricular septal surface accepts the palm of the observer’s right hand such that the thumb fits in the right ventricular inlet, or extends toward the atrial segment, and the fingers can be placed in the right ventricular outlet or toward the arterial segment (Fig. 1A). This right-handed pattern, equivalent to the D-loop ventricular relationship, is usually retained even if the spatial orientation of the ventricles is unexpected for the given atrioventricular connections. The left-handed pattern is found when the right ventricular septal surface accepts the palm of the observer’s left hand with the thumb in the right ventricular inlet or toward the atrial segment and the fingers in the right ventricular outlet or toward the arterial segment (Fig. 1B). This left-handed pattern, equivalent to the L-loop ventricular relationship, is, again usually retained even if the spatial orientation of the ventricles is unusual for the given atrioventricular connections.
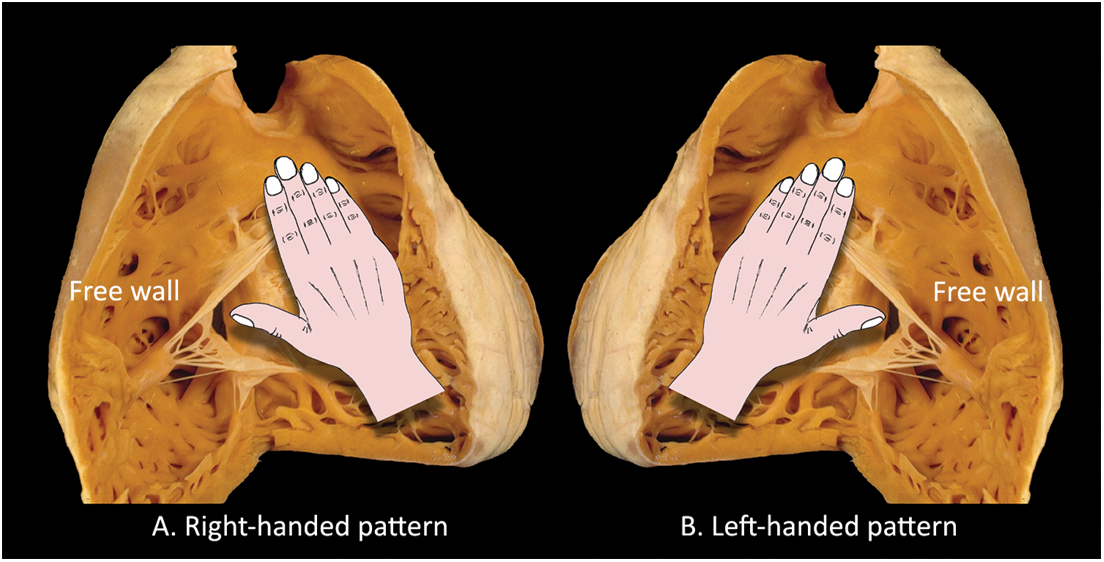
Figure 1: The morphologically right ventricle is opened to show the concept of ventricular topology or chirality. (A) In the right-handed pattern, the consequence of rightward (D-looping) looping during cardiac development, it is the palm of the observer’s right hand that can be placed on the right ventricular septal surface with the wrist on the apex, the thumb in the inlet and the fingers in the outlet. (B) In the presence of left-handed topology, or L-looping, the septal surface of the morphologically right ventricle accepts only the palm of the observer’s left hand
It follows that the concept of ventricular topology, or looping, will be helpful in defining the intrinsic relationship between the ventricles within the ventricular mass should the hearts have been removed from the body. In this setting, the observer has the freedom to rotate the removed specimen in any direction so as to place the palm of one or other of her or his hands on the septal surface of the morphologically right ventricle. This concept of “placing of hands”, however, is much more difficult during imaging, and during interpretation of the images produced, since it requires the imagination of the observer to simulate the maneuver with the two-dimensional images displayed on a computer screen. The process is prone to error, making it difficult, on occasion, readily to explain the ventricular topology to others. This is particularly the case when the orientation of the ventricles themselves is unusual and complex. In this regard, the development of 3D modeling and printing presents a major breakthrough. As shown by the two cases reported in this issue, the observers can appropriately define the ventricular topology and relationship simply by rotating the 3D volume-rendered images on the computer screen, or the 3D-printed models in their hands. This can be achieved by using either of the two different approaches. The first is to replicate the approach taken by the morphologists and produce an en-face view of the right ventricular septal surface. The second approach, which may be more attractive to imagers, is to produce the ventricular apical view (Figs. 2 and 3). The right ventricular en-face septal view is produced by rotating the 3D image in such a way to place the ventricular septum parallel to the computer screen, with the right ventricular free wall facing the observer and the arterial trunks directed upward. Then, as can be achieved in pathological examination, the palm of the observer is placed on the computer screen. The ventricular apical view is reproduced by rotation of the 3D image in such a way as to place the two ventricles side-by-side, with the ventricular septum placed vertically and at right angles to the computer screen in a neutral position, with the tricuspid valvar orifice facing the observer and the arterial trunks directed upward. This view allows immediate recognition of the relationships of the two ventricles relative to the ventricular septum without having to use the hands. The principle can also be applied to a stack of short axis two-dimensional images that are displayed as seen from the ventricular apex. Application of either of these views in the two cases reported in this issue shows that, despite the concordant atrioventricular connections and situs solitus, there are left-handed ventricular topologic patterns, with L-loop ventricular relationships (Fig. 4). The ventricles are related mainly in anteroposterior fashion in the case reported by Perens et al. [1], and in superoinferior fashion in the case of Song et al. [2].
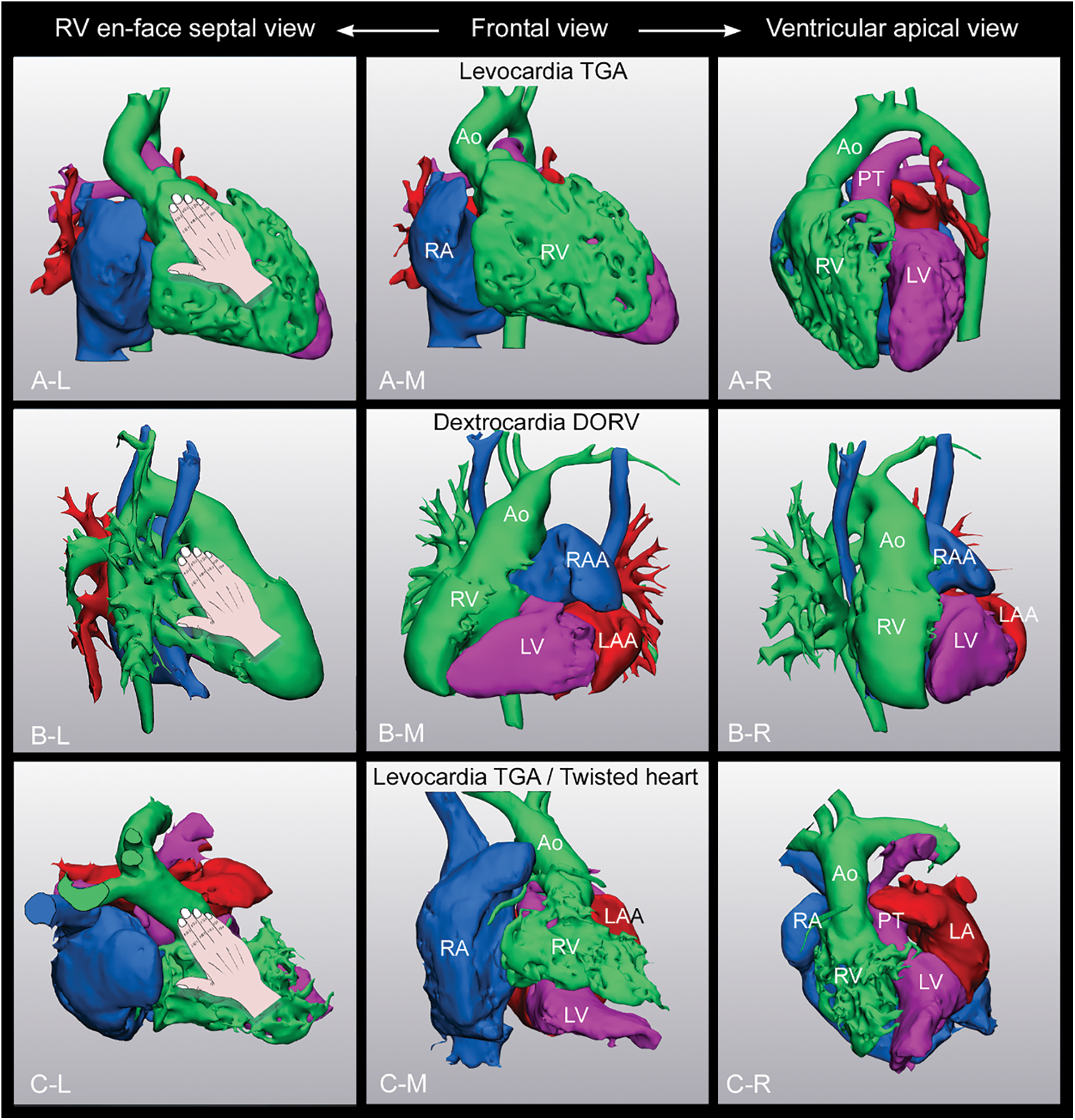
Figure 2: 3D volume-rendered images from three different patients with D-loop ventricles. A. Transposition of the great arteries (TGA) occurring in situs solitus and levocardia. B. Concordant atrioventricular connection and double outlet right ventricle (DORV) occurring in situs solitus and dextrocardia. C. Transposition of the great arteries with twisted atrioventricular connection occurring in situs solitus and levocardia. The middle panels show the frontal views. The left panels show the right ventricular (RV) en-face septal views that are reproduced by rotating the 3D image so as that the ventricular septum is placed parallel to the computer screen with the right ventricular free wall facing the observer and the arterial trunks upward. The observer’s hand is superimposed on the reproduced images to simulate the ventricular topology. In all three cases, the right ventricular septal surface accepts the palm of the observer’s right hand. The right panels show the ventricular apical views that are produced by rotating the 3D images in such a way that the tricuspid valvar orifice faces the observer with the arterial trunks directed upward and the ventricular septum vertically oriented. Both the right-handed ventricular topology pattern and the D-loop ventricular relationship are unequivocally clear
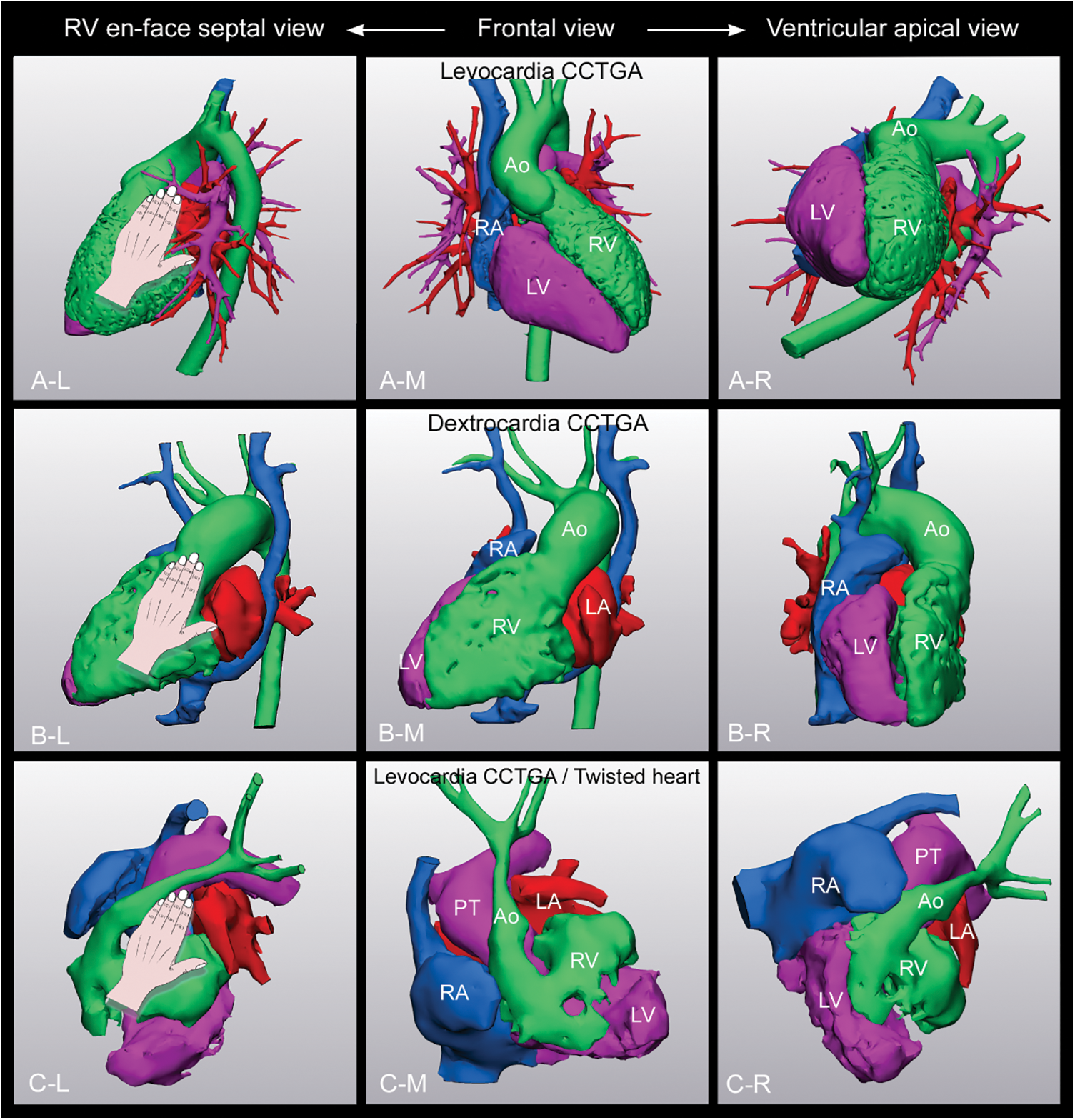
Figure 3: 3D volume-rendered images from three different patients with L-loop ventricles in situ solitus. All had congenitally corrected transposition of the great arteries but different ventricular orientations; A in levocardia, B in dextrocardia and C in levocardia with twisted atrioventricular connections. The middle panels show the frontal views. The left panels show the right ventricular (RV) en-face septal views that are reproduced by rotating the 3D image so as that the ventricular septum is placed parallel to the computer screen with the right ventricular free wall facing the observer and the arterial trunks upward. The observer’s hand is superimposed on the reproduced images. In all three cases, the right ventricular septal surface accepts the palm of the observer’s left hand. The right panels show the ventricular apical views that are produced by rotating the 3D images in such a way that the tricuspid valvar orifice faces the observer with the arterial trunks directed upward and the ventricular septum vertically oriented. Both the left-handed ventricular topology pattern and the L-loop ventricular relationship are unequivocally clear
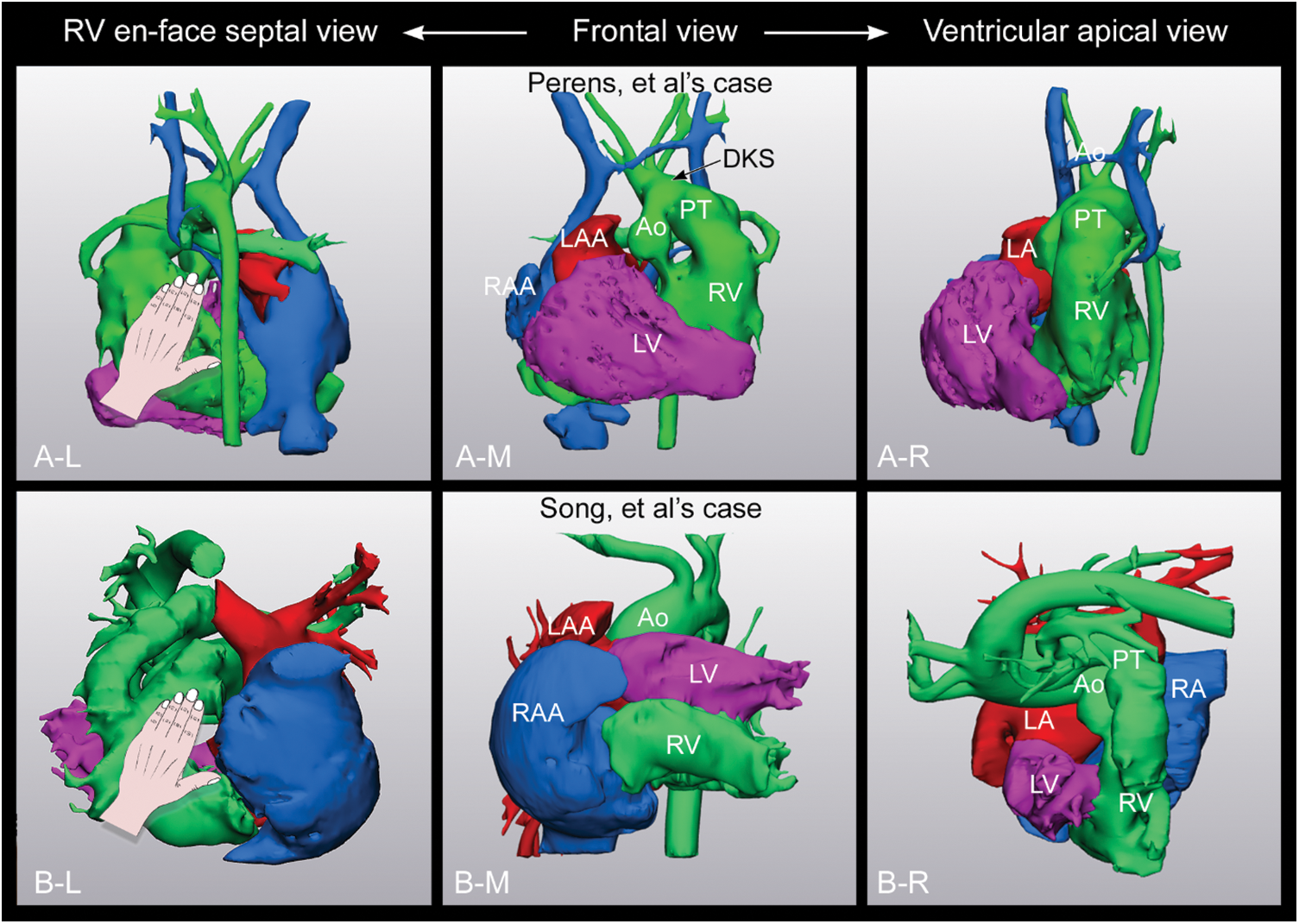
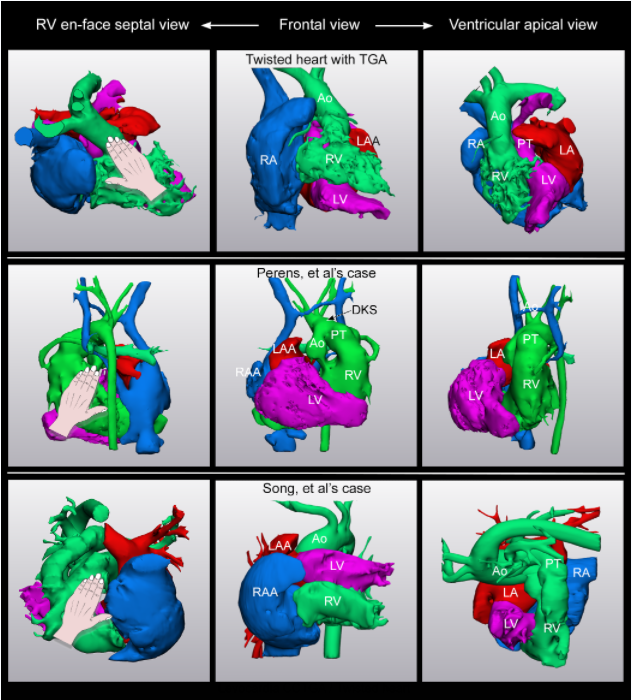
Figure 4: 3D volume-rendered images from the two patients reported by Perens et al. [1] and Song et al. [2] in last issue. The ventricular orientation appears very different. Both cases, nonetheless, show the left-handed pattern of ventricular topology with L-loop ventricular relationship in the presence of concordant atrioventricular connections in the setting of situs solitus
3 Disharmony between the Atrioventricular Connection and the Anticipated Ventricular Relationship and Topology
As far as we are aware, the earliest report of a case showing the disharmonious ventricular relationship and topology for the given atrioventricular connection was provided by Wagner et al. in 1970, when describing a series of patients with right juxtaposition of the atrial appendages [3]. In their Case 6, with situs solitus and concordant atrioventricular connections, the right atrium was connected to the posteriorly positioned right ventricle on the left side of the anteriorly positioned morphologically left ventricle. Wagner et al., however, in their initial account, mistakenly interpreted the ventricular inversion being the consequence of malrotation of a D-loop [3]. When the case was reported again by van Praagh et al., in the proceedings of the first World Society of Paediatric Cardiology, the ventricular relationship was correctly described as representing an L-loop [10]. Subsequent to this early report, Anderson and colleagues reported two cases with segmental disharmony, indicating that the problem of description was resolved when both the atrioventricular connection and the ventricular topology were specified separately. In their first case, there was a left-handed pattern of ventricular topology in the presence of concordant atrioventricular connections in the setting of situs solitus, which they described as usual atrial arrangement, with left juxtaposition of the atrial appendages [4]. In their second case, which showed situs solitus with a left-sided heart, discordant atrioventricular connections were associated with right-handed ventricular topology, in this instance with right juxtaposition of the atrial appendages. Seo et al. [5] then described a case similar to the one reported by Wagner et al. [3]. The two cases reported in this issue now show further examples of the hearts with disharmony between the atrioventricular connection and the ventricular relationship and topology [1,2].
It is surely of note that all 6 cases reported to date have had juxtaposition of the atrial appendages, 5 on the right and 1 on the left [1–5]. Of interest, the ventricular apex pointed to the left in all 5 with right juxtaposition, while it pointed to the right in the example with left juxtaposition [1–5]. A feature of juxtaposition is elongation of the body of the atrium with displacement of its atrioventricular valve toward the side of juxtaposition. In other words, the appendage and the atrioventricular valve are displaced together and in the same direction.
The right and left atrial outlets are displaced toward the abnormally positioned right and left atrioventricular junctions, respectively. As a further consequence of rearrangement of the atrial cavity and atrioventricular valves, the plane of the atrial septum is changed from its usual oblique vertical orientation posteriorly to a horizontal orientation anteriorly. Despite their abnormal relationship and position, however, the opening axes of the atrioventricular valves remain parallel. This is in contrast to the arrangement found with twisted atrioventricular connections, also known as the criss-cross arrangement in which the two atrioventricular valves are not arranged in parallel fashion, while the harmony between the atrioventricular connections and ventricular topology is retained [10–12].
4 Left Ventricle on Top of the Right Ventricle
Only a few cases have been reported in which the left ventricular inlet is located on top of the right ventricular inlet [14–16], as is the situation with the two cases reported in this issue [1,2], Case 6 of Wagner et al. [3] and Case 1 of Seo et al. [5] are additional examples of the heart with the left ventricle and the mitral valve on top of the right ventricle and tricuspid valve.
One of us also had an opportunity to provide 3D printing service of a case of tetralogy of Fallot with the left ventricular inlet displaced on top of the right ventricular inlet due to twisted atrioventricular connection (Fig. 5). The findings in this case contrasted most examples of twisted or criss-cross hearts, in which the right ventricular inlet is superior to the left ventricular inlet [11–13,16]. Twisting around the long axis of the heart, in the majority of cases, occurs so as to place the right ventricular inlet above the left ventricular inlet [12,13]. In the case shown in Fig. 5, twisting was in an opposite direction.
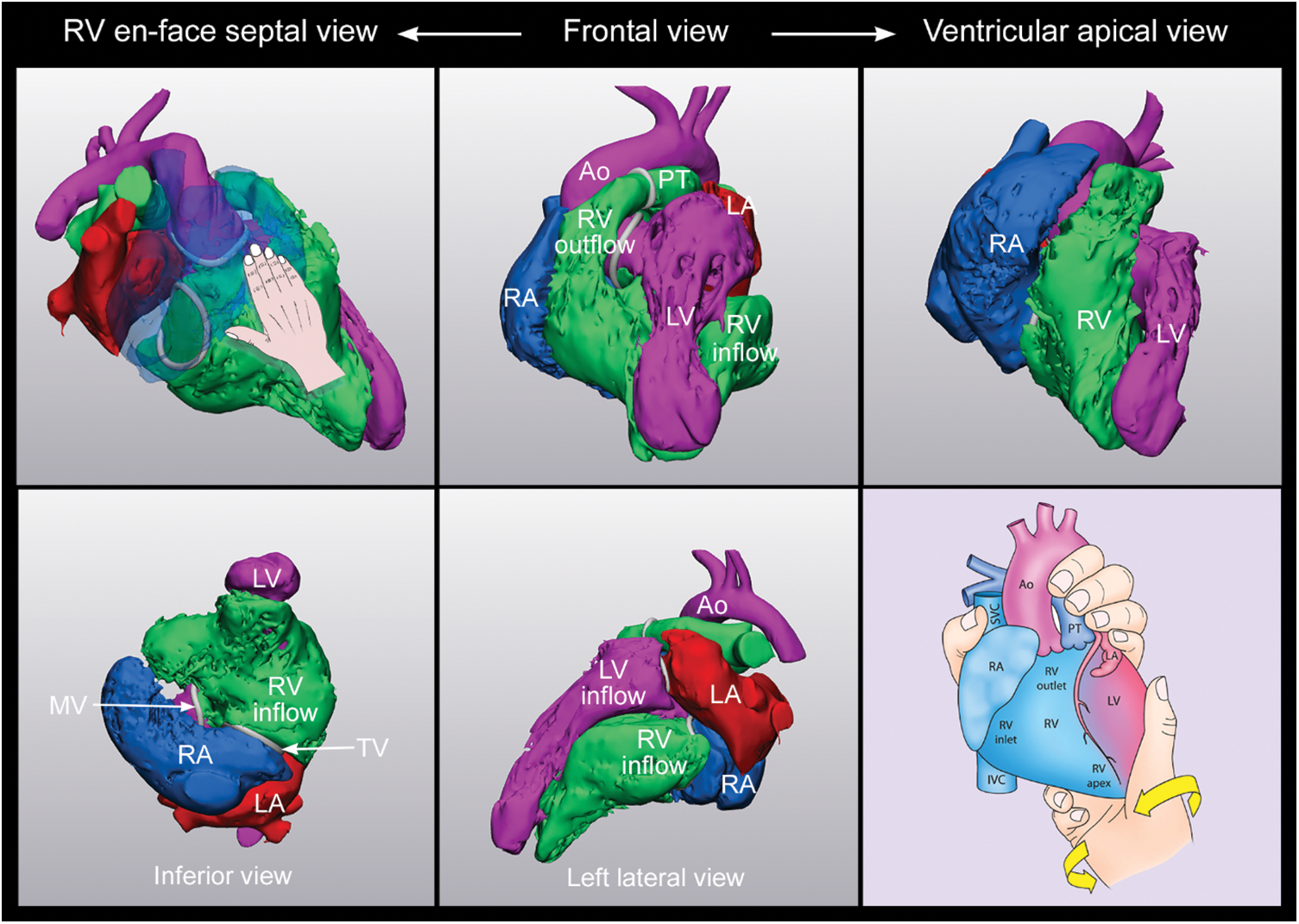
Figure 5: Tetralogy of Fallot with left ventricle on top of the right ventricle due to twisted atrioventricular connection (Courtesy of Drs. Linda Haramati and Samuel Weinstein, Montefiore Medical Center, USA). The heart is in the midline with the apex pointing downward and forward as shown in the frontal view in the upper middle panel. The tricuspid valve (TV) and the underlying right ventricular (RV) inlet are displaced to the left. The mitral valve (MV) is displaced upward and rightward. As a result, the mitral valve is located right superior to the tricuspid valve in the setting of atrial situs solitus (best appreciated in the inferior view on the left lower panel). The tricuspid and mitral valves are not parallel. The right ventricle wraps around the left ventricle (LV) from behind. The right ventricular (RV) en-face septal view in left upper panel shows the right-handed pattern of ventricular topology. The ventricular apical view in the right upper panel shows the D-loop ventricular relationship as the right ventricle is on the right side of the septum. Cartoons in the right lower panel shows the mechanism of twisting. Counter clockwise twisting of the heart with usual chamber orientation as shown by a curved arrow will result in the abnormal relationship of the cardiac chambers as shown in the upper middle panel. Ao, aorta; IVC, inferior vena cava; LA, left atrium; PT, pulmonary arterial trunk; RA, right atrium; SVC, superior vena cava
5 Topsy-Turvy Relationship of the Cardiac Chambers
It is of further interest that the heart described by Song et al. [2] shows not only disharmonious ventricular relationship and topology for the given atrioventricular connection, but also the arrangement described as the “topsy-turvy” relationship. This very unusual pattern was first described by Freedom and his associates in their seminal textbook “Angiocardiography of Congenital Heart Disease” published in 1984 [17]. Surprisingly, the case report they submitted for publication at this time was not deemed suitable for publication. In the two cases described in their book, the ventricles were related in supero-inferior fashion with the arterial pole of the heart rotated posteroinferiorly. This resulted in the arterial trunks arising from the diaphragmatic aspect of the ventricular mass. The term was then revived by one of us, with his colleagues, when describing a case recognized during fetal echocardiography [18]. Since this time, a a few cases with topsy-turvy heart have been reported [19–25]. We have previously used the 3D modeled images of the case now reported by Song et al. [2] as an example of the topsy-turvy heart [12]. As their current report emphasizes, the case of Song and colleagues differs from the other topsy-turvy hearts in that it also shows disharmonious ventricular relationship and topology for the given atrioventricular connections [19–25]. It is also of note that the majority of individuals with topsy-turvy heart originated from South Asia, Middle East, Turkey and Egypt. Perhaps it would be appropriate to limit the usage of the term “topsy-turvy heart” to those occurring in an otherwise normal segmental setting.
The two cases reported in this issue share the unexpected feature of disharmony between the atrioventricular connections and ventricular relationship and topology. Interpretation of the cases focuses attention on the importance of three basic facets of cardiac building blocks, namely their morphology, the relationship of their component parts, and their connections with the adjacent segments. All three components must be separately assessed during sequential segmental approach. The need for separate assessment points to a flaw in the original segmental approach, when it was assumed that ventricular looping was always harmonious with atrial situs. As we have emphasized, 3D imaging and printing can now facilitate an otherwise difficult diagnosis in such complex situations. Rotation of either the 3D images or the models permits accurate assessment of the ventricular topologic pattern by creating the right ventricular en-face septal view, thus facilitating placement of the observer’s hands. As we now emphasize, an alternative approach, which might prove more attractive to imagers, is to rotate the ventricular mass to provide the ventricular apical view, thus permitting determination of the ventricular relationship without using the hands.
Authorship: The authors confirm contribution to the paper as follows: S.J.Y.: study conception and design: S.J.Y., A.S.; data collection: S.J.Y., R.H.A.; manuscript preparation with extensive literature review and discussion: A.S., C.Z.L., R.H.A. All authors reviewed the results and approved the final version of the manuscript.
Funding Statement: The authors received no specific funding for this study.
Conflicts of Interest: The author, Dr. Shi-Joon Yoo is an editorial board member of Congenital Heart Disease, who was completely avoided being involved in the entire review process. The other authors declare that they have no conflicts of interest to report regarding the present article.
References
1. Perens, G., Yoshida, T., Finn, J. P. (2022). A rare case of concordant atrioventricular connection to L-looped ventricles in situs solitus: 4-dimensional magnetic resonance imaging and 3D printing. Congenital Heart Disease, 17(4), 387–392. DOI 10.32604/chd.2022.021233. [Google Scholar] [CrossRef]
2. Song, M. K., Kim, G. B., Kim, W. H., Lee, W., Bae, E. (2022). Concordant atrioventricular connection to L-looped ventricles with the left ventricle on top of the right ventricle in situs solitus: A case report with 3D modelling and printing. Congenital Heart Disease, 17(4), 393–398. DOI 10.32604/chd.2022.019603. [Google Scholar] [CrossRef]
3. Wagner, H. R., Alday, L. E., Vlad, P. (1970). Juxtaposition of the atrial appendages: A report of six necropsied cases. Circulation, 42(1), 157–163. DOI 10.1161/01.CIR.42.1.157. [Google Scholar] [CrossRef]
4. Anderson, R. H., Smith, A., Wilkinson, J. L. (1987). Disharmony between atrioventricular connections and segmental combinations: Unusual variants of “crisscross” hearts. Journal of American College of Cardiology, 10(6), 1274–1277. DOI 10.1016/S0735-1097(87)80130-4. [Google Scholar] [CrossRef]
5. Seo, J. W., Choe, G. Y., Chi, J. G. (1989). An unusual ventricular loop associated with right juxtaposition of the atrial appendages. International Journal of Cardiology, 25(2), 219–228. DOI 10.1016/0167-5273(89)90111-3. [Google Scholar] [CrossRef]
6. Tynan, M. J., Becker, A. E., Macartney, F. J., Jiménez, M. Q., Shinebourne, E. A. et al. (1979). Nomenclature and classification of congenital heart disease. British Heart Journal, 41(5), 544–553. DOI 10.1136/hrt.41.5.544. [Google Scholar] [CrossRef]
7. Lev, M. (1954). Pathologic diagnosis of positional variations in cardiac chambers in congenital heart disease. Laboratory Investigation, 3(1), 71–82. [Google Scholar]
8. Anderson, R. H. (1982). Criss-cross hearts revisited. Pediatric Cardiology, 3(4), 305–313. DOI 10.1007/BF02427032. [Google Scholar] [CrossRef]
9. van Praagh, S., LaCorte, M., Fellows, K. E., Bossina, K., Busch, H. J. et al. (1980). Superioinferior ventricles: Anatomic and angiographic findings in ten postmortem cases. In: van Praagh, R., Takao, A. (Eds.Etiology and morphogenesis of congenital heart disease, pp. 317–378. USA: Futura. [Google Scholar]
10. van Praagh, R., David, I., Gordon, D., Wright, G. B., van Praagh, S. (1981). Ventricular diagnosis and designation. In: Godman, M. J. (Ed.Pediatric cardiology, vol. 4, pp. 153–168. UK: Churchill Livingstone. [Google Scholar]
11. Seo, J. W., Yoo, S. J., Ho, S. Y., Lee, H. J., Anderson, R. H. (1992). Further morphological observations on hearts with twisted atrioventricular connections (criss-cross hearts). Cardiovascular Pathology, 1(3), 211–217. DOI 10.1016/1054-8807(92)90027-L. [Google Scholar] [CrossRef]
12. Yoo, S. J., Seo, J. W., Lim, T. H., Park, I. S., Hong, C. Y. et al. (1993). Hearts with twisted atrioventricular connections: Findings at MR imaging. Radiology, 188(1), 109–113. DOI 10.1148/radiology.188.1.8511282. [Google Scholar] [CrossRef]
13. Yoo, S. J., Anderson, R. H. (2020). Abnormal positions and relationships of the heart. In: Wernovsky, G. (Ed.Anderson’s pediatric cardiology. 4th edition, pp. 913–926. USA: Elsevier. [Google Scholar]
14. Porras, D., Kratz, C., Loukas, M., van Doesburg, N. H., Davignon, A. et al. (2003). Superoinferior ventricles with superior left ventricle and inferior right ventricle: A newly recognized form of congenital heart disease. Pediatric Cardiology, 24(6), 604–607. DOI 10.1007/s00246-002-0396-9. [Google Scholar] [CrossRef]
15. Yang, G., Wang, Q., He, J., Wu, M. (2010). Superior left ventricle in combination with inferior right ventricle: Presenting with balanced hemodynamics and mild symptoms in a late adolescent. Texas Heart Institute Journal, 37(4), 445–448. [Google Scholar]
16. Angelini, P. (2010). Left ventricle on top versus right ventricle on top in superoinferior ventricles: What are we talking about? Texas Heart Institute Journal, 37(4), 442–444. [Google Scholar]
17. Freedom, R. M., Culham, J. A. G., Moes, F. (1984). Superoinferior ventricles: A consideration of so-called criss-cross atrioventricular connections. In: Angiocardiography of congenital heart disease, pp. 629–642. USA: MacMillan Publishing Company. [Google Scholar]
18. Jaeggi, E., Chitayat, D., Golding, F., Kim, P., Yoo, S. J. (2008). Prenatal diagnosis of topsy-turvy heart. Cardiology in the Young, 18(3), 337–342. DOI 10.1017/S1047951108002308. [Google Scholar] [CrossRef]
19. Güzeltaş, A., Öztürk, E., Diker, M. (2013). Topsy-turvy heart: A very rare case of superoinferior ventricle. Pediatric Cardiology, 34(8), 2096–2098. DOI 10.1007/s00246-013-0656-x. [Google Scholar] [CrossRef]
20. Sasikumar, D., Dharan, B. S., Menon, S., Sivasubramanian, S., Kapilamoorthy, T. R. (2016). Surgical closure of aortopulmonary window in a topsy-turvy heart: A surgical challenge. Annals of Thoracic Surgery, 101(5), 1982–1984. DOI 10.1016/j.athoracsur.2015.04.128. [Google Scholar] [CrossRef]
21. Bayramoglu, Z., Yılmaz, R., Demir, A. A., Yekeler, E., Dursun, M. et al. (2017). Topsy-turvy heart and associated imaging findings. Journal of Cardiovascular Computed Tomography, 11(5), 417–418. DOI 10.1016/j.jcct.2017.04.008. [Google Scholar] [CrossRef]
22. Zakaria, R. H. (2019). Topsy-turvy heart: Volume-rendered CT angiography. Radiology, 292(1). DOI 10.1148/radiol.2019190328. [Google Scholar] [CrossRef]
23. Alkhateeb, A., Mansour, A., Tanidir, I. C. (2021). Topsy-turvy heart: A first recorded case report with intracardiac anomaly. Echocardiography, 38(1), 114–117. DOI 10.1111/echo.14950. [Google Scholar] [CrossRef]
24. Bhalgat, P., Shah, J. (2021). Antenatal assessment of topsy-turvy heart with crisscross inlet. Journal of American College of Cardiology: Case Reports, 3(5), 715–720. DOI 10.1016/j.jaccas.2020.12.040. [Google Scholar] [CrossRef]
25. Hejazi, Y., Mann, G., Boudjemline, Y., Udassi, J. P., van Leeuwen, G. et al. (2021). Topsy-turvy heart with aortopulmonary window and severe airway malacia: Prenatal diagnosis and review of the literature. Pediatric Cardiology, 43, 225–232. DOI 10.1007/s00246-021-02710-1. [Google Scholar] [CrossRef]
Cite This Article
 Copyright © 2022 The Author(s). Published by Tech Science Press.
Copyright © 2022 The Author(s). Published by Tech Science Press.This work is licensed under a Creative Commons Attribution 4.0 International License , which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
 Downloads
Downloads
 Citation Tools
Citation Tools