 Open Access
Open Access
REVIEW
First-Line Treatment Strategies in IMDC Favourable-Risk Metastatic Clear Cell Renal Cell Carcinoma
Alejandro Valdés1,2, Jaime González-Montero1,3, Carlos Rojas1,3, Mauricio Burotto1,3,*
1 Bradford Hill Clinical Research Center, Santiago, Chile
2 Instituto Nacional del Cáncer, Santiago, Chile
3 Faculty of Medicine, Finis Terrae University, Santiago, Chile
* Corresponding Author: Mauricio Burotto. Email: 
Oncology Research https://doi.org/10.32604/or.2026.077711
Received 15 December 2025; Accepted 03 April 2026; Published online 26 May 2026
Abstract
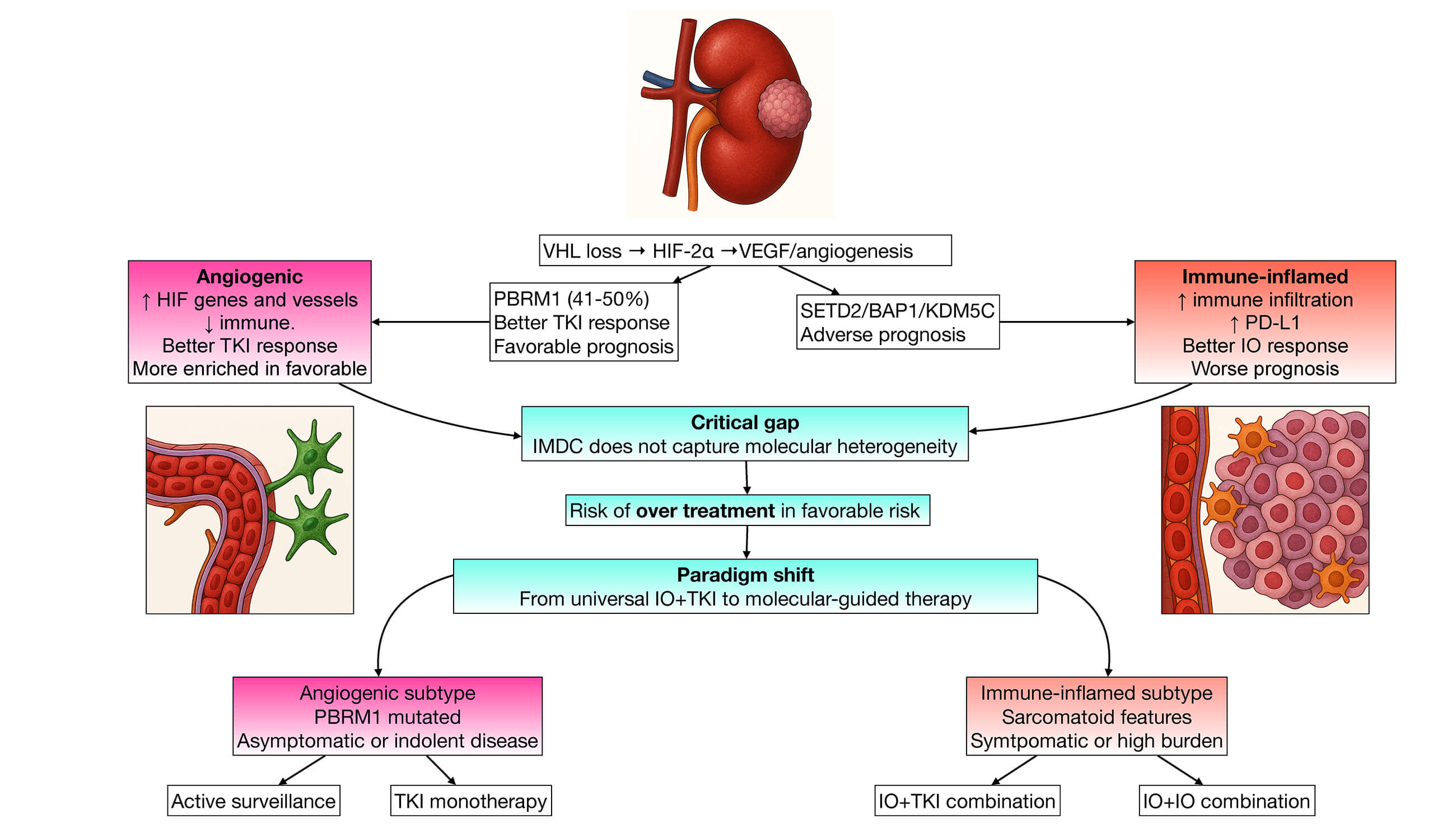
Immune checkpoint inhibitors (ICIs) combined with vascular endothelial growth factor tyrosine kinase inhibitors (VEGF-TKIs) have transformed the treatment landscape of advanced clear cell renal cell carcinoma (ccRCC). Current guidelines favour ICI plus VEGF-TKI (IO+TKI) combinations for favourable-risk disease (International Metastatic RCC Database Consortium [IMDC] score 0) based on improved objective response rates and progression-free survival. However, no IO+TKI combination has demonstrated a statistically significant overall survival (OS) benefit in this subgroup. A pooled analysis of four pivotal phase III trials (n = 839 favourable-risk patients) revealed no OS advantage for IO+TKI versus sunitinib monotherapy (hazard ratio [HR] 1.24; 95% CI 0.86–1.78) despite higher toxicity rates (71–82% Grade ≥ 3 adverse events vs. 63–72% with sunitinib) and substantially greater cost. The IMDC favourable-risk category represents approximately 20% of metastatic ccRCC cases and is often characterised by indolent disease biology. Emerging molecular classifications reveal distinct transcriptomic subgroups, including an angiogenic subtype (ccA/CC-e.2/clusters 1–2) enriched in favourable-risk patients, characterised by high hypoxia-inducible factor (HIF) pathway gene expression, frequent PBRM1 mutations, robust VEGF-TKI responsiveness, and comparatively lower benefit from immunotherapy. Current clinical risk stratification fails to capture this molecular heterogeneity, limiting optimal treatment selection. VEGF-TKI monotherapy (median OS 47.6–79.4 months) and active surveillance remain valid, evidence-based alternatives in carefully selected favourable-risk patients, particularly those with asymptomatic, metachronous, or otherwise indolent disease. Uncritical universal use of IO+TKI in this population may therefore represent overtreatment. The development and validation of predictive biomarkers, refinement of molecular risk stratification, and exploration of novel agents with more favourable toxicity profiles (e.g., HIF-2α inhibitors) are urgently required to personalise therapy and identify candidates for rational treatment de-escalation.
Graphical Abstract
Keywords
Renal cell carcinoma; clear cell renal carcinoma; favourable risk; IMDC; TKI; VEGF-TKI; immunotherapy; IO; first-line treatment; active surveillance

 Submit a Paper
Submit a Paper Propose a Special lssue
Propose a Special lssue Download PDF
Download PDF Downloads
Downloads
 Citation Tools
Citation Tools