
 Submit a Paper
Submit a Paper Propose a Special lssue
Propose a Special lssue Open Access
Open Access
REVIEW
First-Line Treatment Strategies in IMDC Favourable-Risk Metastatic Clear Cell Renal Cell Carcinoma
1 Bradford Hill Clinical Research Center, Santiago, Chile
2 Instituto Nacional del Cáncer, Santiago, Chile
3 Faculty of Medicine, Finis Terrae University, Santiago, Chile
* Corresponding Author: Mauricio Burotto. Email:
(This article belongs to the Special Issue: Advances in Genitourinary Cancer)
Oncology Research 2026, 34(8), 4 https://doi.org/10.32604/or.2026.077711
Received 15 December 2025; Accepted 03 April 2026; Issue published 16 July 2026
 View Full Text
View Full Text Download PDF
Download PDFAbstract
Immune checkpoint inhibitors (ICIs) combined with vascular endothelial growth factor tyrosine kinase inhibitors (VEGF-TKIs) have transformed the treatment landscape of advanced clear cell renal cell carcinoma (ccRCC). Current guidelines favour ICI plus VEGF-TKI (IO+TKI) combinations for favourable-risk disease (International Metastatic RCC Database Consortium [IMDC] score 0) based on improved objective response rates and progression-free survival. However, no IO+TKI combination has demonstrated a statistically significant overall survival (OS) benefit in this subgroup. A pooled analysis of four pivotal phase III trials (n = 839 favourable-risk patients) revealed no OS advantage for IO+TKI versus sunitinib monotherapy (hazard ratio [HR] 1.24; 95% CI 0.86–1.78) despite higher toxicity rates (71–82% Grade ≥ 3 adverse events vs. 63–72% with sunitinib) and substantially greater cost. The IMDC favourable-risk category represents approximately 20% of metastatic ccRCC cases and is often characterised by indolent disease biology. Emerging molecular classifications reveal distinct transcriptomic subgroups, including an angiogenic subtype (ccA/CC-e.2/clusters 1–2) enriched in favourable-risk patients, characterised by high hypoxia-inducible factor (HIF) pathway gene expression, frequent PBRM1 mutations, robust VEGF-TKI responsiveness, and comparatively lower benefit from immunotherapy. Current clinical risk stratification fails to capture this molecular heterogeneity, limiting optimal treatment selection. VEGF-TKI monotherapy (median OS 47.6–79.4 months) and active surveillance remain valid, evidence-based alternatives in carefully selected favourable-risk patients, particularly those with asymptomatic, metachronous, or otherwise indolent disease. Uncritical universal use of IO+TKI in this population may therefore represent overtreatment. The development and validation of predictive biomarkers, refinement of molecular risk stratification, and exploration of novel agents with more favourable toxicity profiles (e.g., HIF-2α inhibitors) are urgently required to personalise therapy and identify candidates for rational treatment de-escalation.Graphic Abstract
Keywords
Renal cancer accounts for approximately 2% of all malignancies, with a global estimate of 434,419 new cases (14th) and 155,702 deaths (16th) annually [1,2]. Renal cell carcinoma (RCC) comprises > 90% of kidney cancers, with clear cell RCC (ccRCC) as the most common subtype (70%). The remaining subtypes are grouped as non–clear cell RCCs, of which papillary and chromophobe carcinomas are the most frequent [3].
Localised disease is managed with partial or radical nephrectomy; however, approximately 30% of patients present with metastases at diagnosis, and an additional 30% experience recurrence following nephrectomy [4]. Prognosis in advanced disease remains poor, with a five-year survival rate near 15% [5]. Historically considered chemoresistant, RCC treatment saw its first meaningful gains with cytokine therapy (interferon-α and interleukin-2), which produced low overall response rates (ORRs) and substantial toxicity, although a minority of patients experienced durable benefits [6]. The advent of vascular endothelial growth factor receptor (VEGF) tyrosine kinase inhibitors (VEGF-TKIs) transformed care. Immunotherapy with immune checkpoint inhibitors (ICIs) targeting PD-1/PD-L1 and CTLA-4 further improved outcomes.
First-line therapy selection in advanced ccRCC is often guided by the International Metastatic RCC Database Consortium (IMDC) criteria—developed during the advent of VEGF-TKI therapies—which stratify patients into favourable, intermediate, and poor risk groups [7]. Approximately 20% of patients are favourable-risk, typically with a more indolent disease presentation [8]. Current guidelines recommend combination regimens: ICI with VEGF-TKI (IO+TKI) or dual ICI (anti–PD-1 with anti–CTLA-4; IO+IO) [9,10,11]. In intermediate–poor-risk disease, these combinations confer a median overall survival (mOS) advantage over TKI monotherapy. Guidelines recommend IO+TKI in favourable-risk patients due to higher ORR and longer median progression-free survival (mPFS) versus TKI alone; however, the absence of a consistent mOS advantage, in addition to increased toxicity and cost, argues against a one-size-fits-all approach. In carefully selected scenarios, TKI monotherapy, IO+IO combinations, or active surveillance (AS) remain reasonable options. Emerging molecular classifications suggest biologically distinct subgroups with differing angiogenic and immune signatures, with potential implications for therapy selection [12]. The development and validation of predictive biomarkers are therefore urgently required to refine treatment selection and personalise care.
2 Characterisation of Favourable-Risk ccRCC
The current definition of risk groups relies on prognostic models developed in the pre-immunotherapy era. Numerous studies have identified prognostic factors in renal cancer to refine outcome estimation and help trial stratification. The most widely used tools—the Memorial Sloan Kettering Cancer Center (MSKCC) model [13,14] (developed during the cytokine therapy era) and the IMDC criteria [8]—utilise clinical and laboratory variables to estimate prognosis (Table 1). Both tools categorise patients into three risk groups (favourable, intermediate, and poor) based on pre-treatment prognostic features. The IMDC model has been externally validated in diverse populations [15,16]. Further refinement of the IMDC database identified a ‘very favourable’ subgroup [17]. The following variables were independently associated with OS in a multivariable analysis (hazard ratio [HR] approximately 1.4–1.5; p < 0.05): time from initial diagnosis to systemic therapy (<3 vs. ≥3 years), Karnofsky Performance Status (80 vs. >80%), and the presence of brain, liver, or bone metastases. Patients were classified as very favourable (0 risk factors; 29%) or favourable (≥1 risk factor; 71%), with an mOS of 64.8 vs. 45.6 months, respectively (HR 1.84; p < 0.001). This new group underwent external validation in a Turkish cohort [18].
Developed during the VEGF-TKI era, the IMDC criteria demonstrated the advantages of VEGF-TKI therapies across all risk groups, albeit with poorer outcomes in the intermediate and poor categories. Contemporary ccRCC trials evaluating immunotherapy combinations (IO+IO or IO+TKI), therefore continue to stratify patients by IMDC risk. Retrospective analyses from the IMDC database suggest that the model retains prognostic discrimination in patients treated with IO-based doublets, supporting its ongoing use as a robust prognostic tool [19].
In practice, IMDC risk is often—imperfectly—treated as a predictive biomarker to guide first-line regimen selection [20]. However, IMDC was designed to estimate disease aggressiveness and overall survival primarily independently of the therapy received, not to predict differential benefit between treatments. Its use as a predictive biomarker is based partially on the initial results of CheckMate 214 [21], in which sunitinib outperformed nivolumab plus ipilimumab in the favourable-risk subgroup. Establishing a predictive biomarker of treatment benefit requires a formal test of interaction between biomarker status (positive vs. negative) and treatment effect across at least two therapies (or therapy vs. placebo) [22]. IO+TKI doublets have not improved mOS over TKI monotherapy in favourable-risk disease [23], and updated CheckMate 214 data show a nonsignificant trend towards improved mOS with IO+IO versus TKI [21]. Moreover, a retrospective analysis of CheckMate 214 suggests that the prognostic performance of IMDC attenuates over time and with IO exposure, raising questions about its long-term prognostic capability in the immunotherapy era [24]. Extrapolating IMDC categories as a predictive biomarker, therefore, risks conflating prognosis with genuine treatment-effect modification.
Whether newer models should remain purely prognostic or evolve to incorporate predictive elements remains an open question. Some IMDC variables (e.g., anaemia, thrombocytosis, neutrophilia) are surrogates of systemic inflammation and may correlate with tumour biology; clinical variables alone cannot capture underlying molecular drivers. Genomic profiling may enhance risk discrimination and is an active area of investigation. For example, retrospective analyses of COMPARZ and RECORD-3 identified mutations in BAP1, PBRM1, and TP53 as independent prognostic factors that improved stratification in addition to the MSKCC criteria [25]. Nonetheless, integrating molecular predictive biomarkers into routine care presents practical obstacles, including cost, assay availability, analytical validity, and uncertain incremental clinical utility [26].
Table 1: The Memorial Sloan Kettering Cancer Center (MSKCC) and International Metastatic RCC Database Consortium (IMDC) prognostic models.
| A | MSKCC Model (also Known as the Motzer Criteria) | IMDC Model (also Known as the Heng Criteria) |
|---|---|---|
| Patient cohort and data derivation | Single-centre retrospective analysis. 670 patients treated between 1975 and 1996; majority received interferon or interleukin. Other patients received ineffective therapies (chemotherapy or hormonal therapy). | Multicentre international database (IMDC). 645 patients with metastatic RCC treated with vascular endothelial growth factor (VEGF)–targeted agents (sunitinib, sorafenib, or bevacizumab plus interferon) between August 2004 and July 2008. |
| Risk factors | Low Karnofsky Performance Status (KPS < 80%) Anaemia (<LLN) High lactate dehydrogenase (LDH > 1.5 × ULN) Hypercalcaemia (corrected calcium > ULN) Short interval from diagnosis to systemic treatment (<1 year) | Low Karnofsky Performance Status (KPS < 80%) Anaemia (<LLN) Hypercalcaemia (corrected calcium > ULN) Neutrophilia (elevated neutrophil count) (>ULN) Thrombocytosis (>ULN) Short interval from diagnosis to systemic treatment (<1 year) |
| Risk group classification | Favourable: 0 factors Intermediate: 1–2 factors Poor: ≥3 factors | Favourable: 0 factors Intermediate: 1–2 factors Poor: ≥3 factors |
| Prognostic significance (median OS) | Favourable risk: 29.6 months (95% CI 20.9–37.8 months); 3-year survival 45% Intermediate risk: 13.8 months (95% CI 12.4–15.9); 3-year survival 17% Poor risk: 4.9 months (95% CI 4.3–6.3); 3-year survival 2% | Favourable risk: 43.2 months (95% CI 31.4–50.1) Intermediate risk: 22.5 months (95% CI 18.7–25.1) Poor risk: 7.8 months (95% CI 6.5–9.7) |
3 Refining the Definition of Favourable Risk
Most ccRCCs are initiated by biallelic VHL inactivation, typically through loss of chromosome 3p followed by somatic mutation or promoter methylation [27]. VHL encodes pVHL, the substrate-recognition subunit of an E3 ubiquitin ligase complex which targets prolyl-hydroxylated HIF-α for proteasomal degradation [28]. The loss of pVHL stabilises HIF-α—predominantly HIF-2α in ccRCC—which dimerises with ARNT (HIF-1β) and drives a pseudohypoxic program, upregulating VEGF, EPO, CA9, and GLUT1 and promoting angiogenesis and metabolic reprogramming [29,30].
The loss of pVHL alone is usually insufficient for malignant transformation; co-alterations in other 3p tumour suppressors modulate phenotype and prognosis. PBRM1, SETD2, and BAP1 encode epigenetic regulators which define partially distinct molecular and clinicopathologic subsets [31]. PBRM1 (mutated in 41–50% of cases) encodes BAF180, a PBAF SWI/SNF complex subunit involved in chromatin remodelling; its loss is common in more indolent tumours and is associated with relatively favourable outcomes [32]. SETD2 and BAP1 (mutated in 13–28% and 11–17% of cases, respectively), which regulate H3K36me3 and H2AK119ub1, respectively, are enriched in higher-grade, more aggressive disease and portend inferior survival [33,34]. KDM5C, an X-linked H3K4 demethylase which mutates more often in male tumours, is implicated in metabolic reprogramming and increased tumorigenicity, aligning with adverse biology in some series [35].
An inflamed tumour microenvironment with T-cell infiltration and variable PD-L1 expression are often observed in ccRCC; myeloid-driven immunosuppression and T-cell dysfunction are also common, supporting initial sensitivity and adaptive resistance to immune checkpoint blockade [36,37]. Angiogenic, T-effector, and myeloid-inflammatory signatures have shown distinct associations with response to VEGF-targeted therapy or immunotherapy-based combinations [38]. Marked intratumour heterogeneity with branched evolution is characteristic: truncal events such as 3p loss and VHL inactivation are shared across regions, whereas PBRM1, SETD2, BAP1, and KDM5C mutations and arm-level copy-number alterations are often subclonal [39,40,41].
The clinical heterogeneity of ccRCC has a clear molecular basis, with multi-omics studies defining reproducible subgroups differing in gene expression programs, dominant mutations, epigenetic features, and clinical behaviour [12,42]. The earliest widely adopted transcriptomic classification identified two main subtypes: clear cell A (ccA) and clear cell B (ccB) [43]. Overexpression of hypoxia-, angiogenesis-, and metabolism-related genes was observed in ccA tumours, which were associated with better survival than ccB. A subsequent meta-analysis of 480 tumours validated the ccA/ccB subtypes and identified a third VHL wild-type subgroup (Cluster 3) [44].
The Cancer Genome Atlas (TCGA) program integrated mRNA, miRNA, DNA methylation, copy-number, and proteomic data from 446 nephrectomy specimens and defined four mRNA (m1–m4) and four miRNA (mi1–mi4) clusters [45]. Three integrative subtypes (CC-e.1, CC-e.2, CC-e.3) were subsequently described across 894 RCCs. In ccRCC, CC-e.2 aligned with the angiogenic ccA subtype and had the best survival, CC-e.3 aligned with the more aggressive ccB subtype and had the worst outcomes, and CC-e.1 exhibited intermediate features. A French group subsequently linked transcriptomic subtypes to VEGF-targeted therapy in 53 primary tumours from patients later administered sunitinib [46]. Four clusters (ccrcc1–ccrcc4) were identified, alongside analyses of copy-number, methylation, and VHL/PBRM1 mutations. The ccrcc2 subgroup showed an angiogenic/metabolic gene signature, overlapped with ccA, and had a good prognosis.
More recently, a multi-omics analysis of pre-treatment samples from the IMmotion151 trial (625 primary, 198 metastatic) defined seven RNA-based clusters [38]. Clusters 1 (angiogenic) and 2 (angiogenic–stromal) were enriched in MSKCC/IMDC favourable-risk patients, VEGF pathway activation, and PBRM1/KDM5C mutations. In IMmotion151 (atezolizumab–bevacizumab vs. sunitinib), these angiogenic clusters derived similar benefit from both treatment arms; a post-hoc analysis of JAVELIN Renal 101 (axitinib–avelumab versus sunitinib) showed improvement in mPFS with VEGF–IO doublets across all clusters [47].
Across transcriptomic classification systems, a reproducible angiogenic favourable subtype emerges, corresponding broadly to ccA, TCGA CC-e.2, CIT ccrcc2/3 and IMmotion clusters 1–2. This subtype is characterized by strong HIF–VEGF axis activity, relative paucity of immune infiltration, and frequent PBRM1 mutations, and is associated clinically with favourable early-to-intermediate outcomes and substantial sensitivity to VEGF-targeted agents. Conversely, durable benefit from immune checkpoint blockade appears less common in this context. However, IMDC favourable-risk status is not synonymous with this angiogenic molecular phenotype, as a proportion of clinically favourable-risk tumours display immune-inflamed biology and may benefit more from IO-based combinations. Incorporating simple biomarkers, including angiogenesis gene signatures, PBRM1 mutation status, and pragmatic surrogates of immune infiltration, could refine the definition of ‘favourable-risk’ and help identify patients suitable for de-escalation strategies such as AS and VEGF-TKI monotherapy.
3.3 The Search for Predictive Biomarkers
Currently, there is no validated predictive biomarker in clinical use for the selection of IO or TKI in ccRCC treatment [48]. Biomarker discovery remains a challenge because the most frequent genomic alterations involve tumour suppressor genes, and the predominance of loss-of-function events limits the identification of directly actionable predictive targets [49]. This challenge is compounded by pronounced spatial and temporal intratumour heterogeneity. Although alterations in genes such as PBRM1, SETD2, and BAP1 may carry biologic and prognostic significance, their association with treatment benefit has been inconsistent across studies, and no single genomic alteration has entered clinical practice as a predictive biomarker [32].
Traditional markers of immunotherapy response have no role in ccRCC; tumour mutation burden is usually low, and PD-L1 is not useful in clinical practice. There is a discrepancy in PD-L1 positivity among clinical trials [50]. Sarcomatoid differentiation repeatedly demonstrates a disproportionate response to IO-containing regimens compared with sunitinib; however, formal, prespecified interaction testing to establish it as a predictive biomarker is lacking [51]. Kidney injury molecule-1 (KIM-1), a transmembrane glycoprotein overexpressed in ccRCC, is a promising biomarker. A phase III trial (IMmotion010) reported that patients with high serum KIM-1 had worse disease-free survival (DFS); however, DFS improved following treatment with adjuvant atezolizumab versus placebo (HR 0.72, 95% CI 0.52–0.99) [52]. A post-hoc analysis of the CheckMate 214 trial showed similar results, with worse DFS both in the IO and TKI arms [53]. A reduction in serum KIM-1 after a single cycle of nivolumab plus ipilimumab was associated with long-term efficacy of this IO doublet.
Multiple biomarker modalities are under active study in ccRCC, including liquid biopsy with circulating tumour DNA (ctDNA) and circulating tumour cells (CTCs), microbiome profiling, single-cell/spatial transcriptomics, and radiomics. Each offers complementary windows to tumour biology and the tumour–host interface [48,54]. Machine-learning radiomics applied to routine baseline CT imaging appears feasible for discriminating responders vs. non-responders to PD-1 blockade, providing a scalable “digital biomarker” that can be paired with clinical features for individualised risk–benefit decisions [55]. In parallel, liquid biopsy dynamics—particularly early on-treatment changes in circulating tumour DNA—have demonstrated potential as a real-time, minimally invasive marker of ICI response, enabling earlier identification of primary resistance and adaptive sequencing strategies [56].
Transcriptomic programs related to angiogenesis, T-effector activity, and myeloid inflammation have improved understanding of the biologic determinants of response in ccRCC, although their predictive value has been inconsistent across IO+IO and IO+TKI studies [57,58,59]. Collectively, these observations suggest that future biomarker development in ccRCC will likely depend on integrated models rather than any single assay. In this context, incorporation of accessible molecular and microenvironmental features, including angiogenesis-related gene signatures, PBRM1 status, and pragmatic surrogates of immune infiltration, may help refine the biologic definition of favourable-risk disease and better identify patients most suitable for de-escalation strategies such as active surveillance or VEGF-targeted monotherapy.
4 Systemic Treatment for Favourable-Risk Advanced Disease
VEGF-TKIs transformed the therapy of metastatic ccRCC after the interleukin era. Phase III trials of sunitinib [60,61], pazopanib [62,63], and sorafenib [64,65] demonstrated improvements in mPFS and ORR, but only sunitinib improved mOS. The IMDC model was developed in a cohort of 645 patients with metastatic RCC administered VEGF-targeted therapy (sunitinib, sorafenib, or bevacizumab plus interferon), reporting an mOS of 29.6 months (95% CI, 20.9–37.8) and a 3-year survival of 45% in favourable-risk patients [8]. Across phase III trials using sunitinib as the control group, mPFS ranged from 12.9 to 20.6 months and mOS from 47.6 to 79.4 months within the favourable-risk population (Table 2). Sunitinib and pazopanib remain in clinical use; sorafenib has largely been abandoned due to inferior efficacy and an unfavourable toxicity profile. Next-generation VEGF-TKIs have also been investigated in the first-line setting. A phase III trial of axitinib [66] and the phase III TIVO-1 trial [67] with tivozanib failed to improve mOS compared with sorafenib.
COMPARZ [68], a noninferiority randomised phase III trial, compared first-line sunitinib with pazopanib in advanced ccRCC. Pazopanib achieved an mPFS of 8.4 months versus 9.5 months with sunitinib (HR, 1.05; 95% CI, 0.90–1.22), meeting the noninferiority margin (upper bound of the 95% CI < 1.25); mOS was 28.4 versus 29.3 months (HR, 0.91; 95% CI, 0.76–1.08) and ORR was similar (33% with pazopanib [1 CR] vs. 29% with sunitinib [3 CR]). Toxicity profiles differed: sunitinib was associated with more fatigue, hand–foot syndrome, mucositis, and haematologic adverse events; pazopanib caused more hepatotoxicity and weight loss. Quality-of-life (QoL) scores favoured pazopanib in 11 of 14 health domains. In the PISCES crossover preference study [69], 70% of patients preferred pazopanib (citing less fatigue and better overall QoL), 22% preferred sunitinib (frequently citing less diarrhoea), and 8% had no preference (p < 0.001). Real-world data show similar mOS between first-line sunitinib vs. pazopanib when adjusted for IMDC criteria [70].
Multiple sunitinib dosing schedules have been explored [71,72]. The pivotal phase III trial recommended 50 mg once daily for 4 weeks on and 2 weeks off (4/2). Continuous daily dosing did not improve the efficacy of the 4/2 schedule [73]. Phase II studies of an alternative 2/1 regimen demonstrated similar efficacy with reduced toxicity [74,75,76]. Treatment breaks (‘stop-and-go’ strategy) trials have sought to improve QoL and reduce cost. The open-label, noninferiority phase II/III STAR trial [77] randomised 920 patients to conventional continuous therapy with pazopanib or sunitinib or a drug-free-interval strategy after 24 weeks of treatment until radiographic progression [78]. Noninferiority for OS was attained in the intention-to-treat analysis (HR, 0.94; 95% CI, 0.80–1.09) but not within the prespecified margin in the per-protocol population. Noninferiority in quality-adjusted life-years was achieved in both the intention-to-treat and per-protocol analyses (per-protocol marginal difference, 0.04).
The phase III CheckMate 214 trial compared four cycles of nivolumab plus ipilimumab, followed by nivolumab alone, versus sunitinib [79]. Randomisation was stratified by IMDC risk. Coprimary endpoints (ORR, mPFS, and mOS) were assessed in the intermediate-/poor-risk cohort; analyses in favourable-risk patients were prespecified as exploratory. In intermediate-/poor-risk disease, nivolumab plus ipilimumab significantly improved ORR (including complete responses [CR]) and mOS. Although mPFS was numerically longer, the difference did not reach statistical significance. These benefits were maintained over extended follow-up [21]. Sunitinib demonstrated higher ORRs and mPFS in the favourable-risk subgroup (Table 2), resulting in guideline restriction of nivolumab plus ipilimumab to IMDC intermediate/poor-risk patients. Notably, the initial advantage of sunitinib attenuated with longer follow-up: a greater proportion of patients achieved CR with nivolumab plus ipilimumab (12.8% vs. 6.5%), with mOS trending longer (77.9 vs. 66.7 months; HR 0.82, 95% CI 0.60–1.13).
In the phase II PRISM trial [80], reduced-frequency ipilimumab plus nivolumab lowered grade 3–5 toxicity versus standard scheduling (32.8% vs. 53.1%; OR 0.43), but failed to meet the prespecified 12-month PFS efficacy threshold. Whether first-line nivolumab requires concurrent anti–CTLA-4 remains uncertain. Adaptive phase II trials—OMNIVORE [81], HCRN GU16-260 [82], and TITAN-RCC [83]—tested deferred salvage ipilimumab after nivolumab, but cross-trial interpretation is limited by population and design heterogeneity. A pooled analysis found deferred ipilimumab had limited efficacy and feasibility, supporting upfront nivolumab plus ipilimumab as standard therapy [84].
Following the efficacy of dual checkpoint blockade in CheckMate 214, multiple phase III randomised trials compared IO+TKI combinations with sunitinib monotherapy. The addition of an ICI to a VEGF-directed TKI aims to extend durable disease control in a subset of patients; distinct mechanisms of action may delay resistance, and preclinical data support potential synergy between anti-angiogenic therapy and immunotherapy [85,86].
Across the ccRCC population, the following three regimens (vs. sunitinib) consistently improved ORR, mPFS, and mOS: pembrolizumab + axitinib in KEYNOTE-426 [87,88,89,90], nivolumab + cabozantinib in CheckMate-9ER [91,92,93,94], and lenvatinib + pembrolizumab in CLEAR [95,96,97] (Table 2). In JAVELIN Renal 101, avelumab + axitinib increased ORR and mPFS, but without a statistically significant mOS difference [98,99,100,101,102].
Within the IMDC favourable-risk subgroup, the main benefits are confined to higher ORR and longer mPFS. Across trials, a consistent OS advantage over sunitinib has not been demonstrated, with hazard ratios commonly near unity. These subgroup findings should be interpreted cautiously and regarded as hypothesis-generating rather than definitive. The lack of OS benefit is partly explained by the long natural history of favourable-risk disease and the low number of deaths, making OS analyses underpowered. In addition, the control arm is comparatively strong because favourable-risk tumours are often angiogenesis-high and VEGF-sensitive, consistent with the association between an angiogenesis signature and outcomes on sunitinib in KEYNOTE-426 (Rini et al. 2025). OS separation may be further attenuated by effective post-progression therapy—typically an ICI—and by the indolent biology of many tumours, which reduces the likelihood that early intensification translates into an OS gain [89]. Supporting this, an exploratory pooled analysis of favourable-risk patients (n = 839) from KEYNOTE-426, CheckMate-9ER, CLEAR, and JAVELIN Renal 101 reported no OS benefit for IO+TKI versus sunitinib (HR 1.24; 95% CI 0.86–1.78) [103]. Meta-analyses are concordant, finding no significant OS improvement in favourable-risk disease and highlighting the need for longer follow-up and more mature data [23,104]. Real-world evidence from ARON-1, a retrospective cohort of 524 favourable-risk patients, likewise showed no difference in median OS between sunitinib and IO+TKI combinations (p = 0.761) [105].
Table 2: Results from phase III IO+IO and IO+TKI trials, including favourable-risk patients.
| Trial | CheckMate 214 [21,79] | CheckMate 9ER [91,92,93,94] | KEYNOTE-426 [87,88,89,90] | CLEAR (Study 307) [95,96,97] | JAVELIN Renal 101 [98,99,100,101,102] |
|---|---|---|---|---|---|
| Intervention vs. comparator | Nivolumab 3 mg/kg + ipilimumab 1 mg/kg every 3 weeks for 4 doses, followed by nivolumab 3 mg/kg every 2 weeks vs. sunitinib 50 mg daily for 4 weeks (6-week cycle). | Nivolumab + cabozantinib vs. sunitinib 50 mg daily for 4 weeks (6-week cycle). | Pembrolizumab 200 mg q3w + axitinib 5 mg bid vs. sunitinib 50 mg daily for 4 weeks (6-week cycle). | Lenvatinib 20 mg qd + pembrolizumab 200 mg q3w (L+P) vs. lenvatinib 18 mg qd + everolimus 5 mg qd (L+E) vs. sunitinib 50 mg daily for 4 weeks (6-week cycle) (S) (1:1:1). | Avelumab 10 mg/kg + axitinib 5 mg bid vs. sunitinib 50 mg daily for 4 weeks (6-week cycle). |
| Total number of patients (n, %) | 1096 (249, 23%) | 651 (146, 22%) | 861 (269, 31.2%) | 1069 (348, 32%) | 886 (196, 22%) |
| ORR overall population (%) | 39.5 vs. 33.0 (12.0 vs. 9.0). | 56 vs. 28 (13.3 vs. 4.9). | 60.5 vs. 39.6 (11.6 vs. 4.0). | L+P vs. S: 71.3 vs. 36.7 (18.3 vs. 4.8). | 64.8 vs. 31.4 (7.8 vs. 4.5). |
| ORR favourable risk (CR) % | 29.6 vs. 51.6 (12.8 vs. 6.5). | 67.6 vs. 45.8 (16.2 vs. 9.7). | 68.8 vs. 50.4 (13 vs. 6.1). | L+P vs. S: 68.2 vs. 50.8 (20.9 vs. 4.8). | 75.5 vs. 48.8 (9.6 vs. 5.2). |
| mPFS overall population, months (HR, 95%CI) | 12.4 vs. 12.3 (0.88, 0.75–1.03). | 16.6 vs. 8.4 (0.59, 0.49–0.71). | 15.7 vs. 11.1 (0.69, 0.59–0.81). | L+P vs. S: 23.9 vs. 9.2 (0.47, 0.38–0.57; p < 0.0001). | 13.9 vs. 8.5 (0.66, 0.57–0.77; p < 0.0001). |
| mPFS favourable risk, months (HR, 95%CI) | 12.8 vs. 20.6 (1.03, 0.77–1.37). | 21.4 vs. 13.9 (0.76, 0.57–1.02) | 20.7 vs. 17.9 (0.76, 0.57–1.02). | L+P vs. S: 28.6 vs. 12.9 (0.50, 0.35–0.71). | 20.7 vs. 13.8 (0.75, 0.53–1.07; p = 0.1109). |
| OS overall population, months (HR, 95%CI) | 52.7 vs. 37.8 (0.72, 0.62–0.83). | 49.5 vs. 35.5 (0.70, 0.56–0.87). | 47.2 vs. 40.8 (0.84, 0.71–0.99). | L+P vs. S: 53.7 vs. 54.3 (0.79, 0.63–0.99; p = 0.0424). | 44.8 vs. 38.9 (0.88, 0.75–1.04; p = 0.0669). |
| OS favourable risk, months (HR, 95%CI) | 77.9 vs. 66.7 (0.82, 0.60–1.13). | NR vs. 47.6 (1.07, 0.63–1.79). | 60.3 vs. 62.4 (1.10, 0.79–1.54). | L+P vs. S: NR vs. 59.9 (0.94, 0.58–1.52). | 79.4 vs. 65.5 (0.73, 0.48–1.10; p = 0.129). |
| Adverse events (%) | All grades 93.0 vs. 97.0 Grade ≥ 3 46.0 vs. 63.0 | All grades 99.7 vs. 99.1 Grade ≥ 3 75.3 vs. 70.6 | All grades 98.4 vs. 99.5 Grade ≥ 3 75.8 vs. 70.6 | All grades L+P vs. S: 99.7 vs. 98.5 Grade ≥ 3 L+P vs. S: 82.4 vs. 71.8 | All grades 99.5 vs. 99.3 Grade ≥ 3 71.2 vs. 71.5 |
| QoL | Improved | Similar | Similar | Similar | Not reported |
Certain patients exhibit indolent tumour growth kinetics and may be suitable for AS in lieu of immediate systemic therapy, deferring treatment-related toxicity. Economic benefit is uncertain, as many patients ultimately require therapy. Potential risks include anxiety or reduced QoL in some individuals who prefer active intervention, and the possibility of clinical compromise if rapid tumour acceleration occurs. Prospective and retrospective studies have established AS as a safe and valid alternative [106,107].
A single-arm phase II trial was conducted on asymptomatic, treatment-naïve metastatic RCC (including non–clear cell histologies; prior surgery or radiotherapy allowed) [108]. Management consisted of observation with treatment initiation at the joint discretion of the clinician and patient; progression alone did not mandate stopping AS. Of the 48 enrolled patients (96% clear cell; 98% prior nephrectomy; 77% IMDC intermediate/poor risk), the median AS duration was 14.9 months (95% CI 10.6–25.0) with 38 months median follow-up. Overall, 90% experienced progression (median time to progression 9.4 months; 95% CI 7.4–13.4), and mOS was 44.5 months (95% CI 37.6–NR). Multivariable analyses delineated two prognostic strata: a favourable group (60%) with 0–1 IMDC factors and metastases confined to 1–2 organs (median AS 22.2 months; 95% CI 13.8–33.3) and an unfavourable group (all others; median AS 8.4 months; 95% CI 3.2–14.1; p = 0.0056). Patient-reported anxiety/depression and FKSI QoL scores remained stable during surveillance. A retrospective exploratory analysis identified SMARC4 and TP53 mutations as independent predictors of aggressive disease [109].
No universally accepted clinical criteria define candidacy for active surveillance (AS) in metastatic ccRCC, and the breadth of eligibility in the prospective cohort reported by Rini et al. illustrates this heterogeneity. Patients often viewed as suboptimal AS candidates—including those with adverse IMDC risk and even brain metastases—were eligible, highlighting the need for more consistent selection tools. We therefore propose pragmatic clinical criteria to identify patients most suitable for AS (Table 3), while recognising that patient preference, values, and capacity for close follow-up are central; some individuals will reasonably choose immediate systemic therapy. Given the high efficacy and quality-of-life gains achievable with contemporary regimens, AS is best suited to patients with minimal or no cancer-related symptoms and no lesions at imminent risk of causing organ-threatening complications. Rapid tumour growth can precipitate oncologic emergencies (e.g., vertebral metastases with cord compression), yet robust models to predict metastatic growth kinetics are lacking [110]. Tumour growth may also be non-linear, often described by Gompertzian dynamics with an early exponential phase followed by deceleration, which warrants particular caution when baseline metastatic burden is substantial [111]. Clinically, lower IMDC scores (0–1) and metachronous relapse ≥ 1 year after local therapy are more frequently associated with indolent behaviour and may favour an AS-first approach. In the Rini et al. trial, median tumour growth during surveillance was 0.09 cm/month (IQR 0.04–0.17) [108]. To operationalise “slow-growing” for practice and research, we use an approximate reference of approximately 0.1 cm/month increase in RECIST 1.1 sum of diameters (SLD), anchored to these prospective data rather than intended as a validated cut-off; where feasible, growth kinetics should be estimated over at least two sequential scans separated by ≥3 months and interpreted in the context of symptoms, lesion location, and overall disease tempo. Because unidimensional RECIST measurements are subject to meaningful inter- and intra-observer variability that can influence apparent growth rates and response categorisation, numeric slopes should not be used in isolation to mandate treatment initiation. Similarly, any lesion-size limits (e.g., “no dominant lesion > 3 cm”) should be stated explicitly as heuristics for low-volume, non–organ-threatening disease rather than standardised criteria.
In the Rini et al. trial, surveillance visits occurred every 3 months in year 1, every 4 months in year 2, and every 6 months thereafter [108]. Clear, validated triggers to end AS are not established. Reasonable criteria for initiating therapy include emergence or worsening of disease-related symptoms, RECIST-consistent progression (particularly rapid or multisite), development of lesions in organ-threatening locations, increase in IMDC risk category, and patient preference. The real-world prospective observational data (MaRCC) demonstrate the feasibility of embedding standardised PRO monitoring during AS, helping to define patient-centred triggers for treatment initiation [107].
Table 3: Proposed criteria for active surveillance.
| A |
|---|
| Minimal or no symptoms attributable to the tumour (including paraneoplastic syndromes). |
| No potential complications in the event of rapid tumour growth (e.g., no spinal bone metastases). |
| Low tumour burden/small metastases (<3 cm of lesion diameter) and indolent growth (≤0.1 cm/month). |
| Metachronous disease, with time to recurrence ≥ 1 year from previous nephrectomy. |
| International Metastatic RCC Database Consortium risk score 0–1 points. |
| Patient preference and adherence. |
5 Treatment Selection in Favourable-Risk Advanced ccRCC
First-line therapy for advanced ccRCC comprises VEGF-TKIs and ICIs—anti–PD-1/PD-L1 and anti–CTLA-4 monoclonal antibodies—used alone or in combination. Regimen selection is typically guided by IMDC risk score, comorbidities, and patient preference. Preferred options for intermediate/poor-risk disease include dual ICI (IO+IO; anti–CTLA-4 plus anti–PD-1/PD-L1) or an ICI combined with a VEGF-TKI (IO+TKI; VEGF-TKI plus anti–PD-1/PD-L1). Options for favourable-risk disease include IO+TKI, VEGF-TKI monotherapy, IO+IO, and AS. Guidelines favour IO+TKI [9,10,11] for favourable-risk patients, with TKI monotherapy a less preferred option. Uncritical universal use in all IMDC favourable-risk patients is not evidence based and may constitute overtreatment in carefully selected indolent cases. As the updated CheckMate 214 results showed a non-significant OS trend for nivolumab plus ipilimumab versus sunitinib in this subgroup, IO + IO was included as a preferred regimen in the NCCN guidelines. AS is acknowledged in guidelines, but explicit selection criteria remain undefined. Given the breadth of effective options, management is not one-size-fits-all. Therapy should be individualised, ideally delivered through a multidisciplinary tumour board, with consideration of patient preferences. This work proposes a decision algorithm for favourable-risk disease, including special scenarios (Fig. 1).

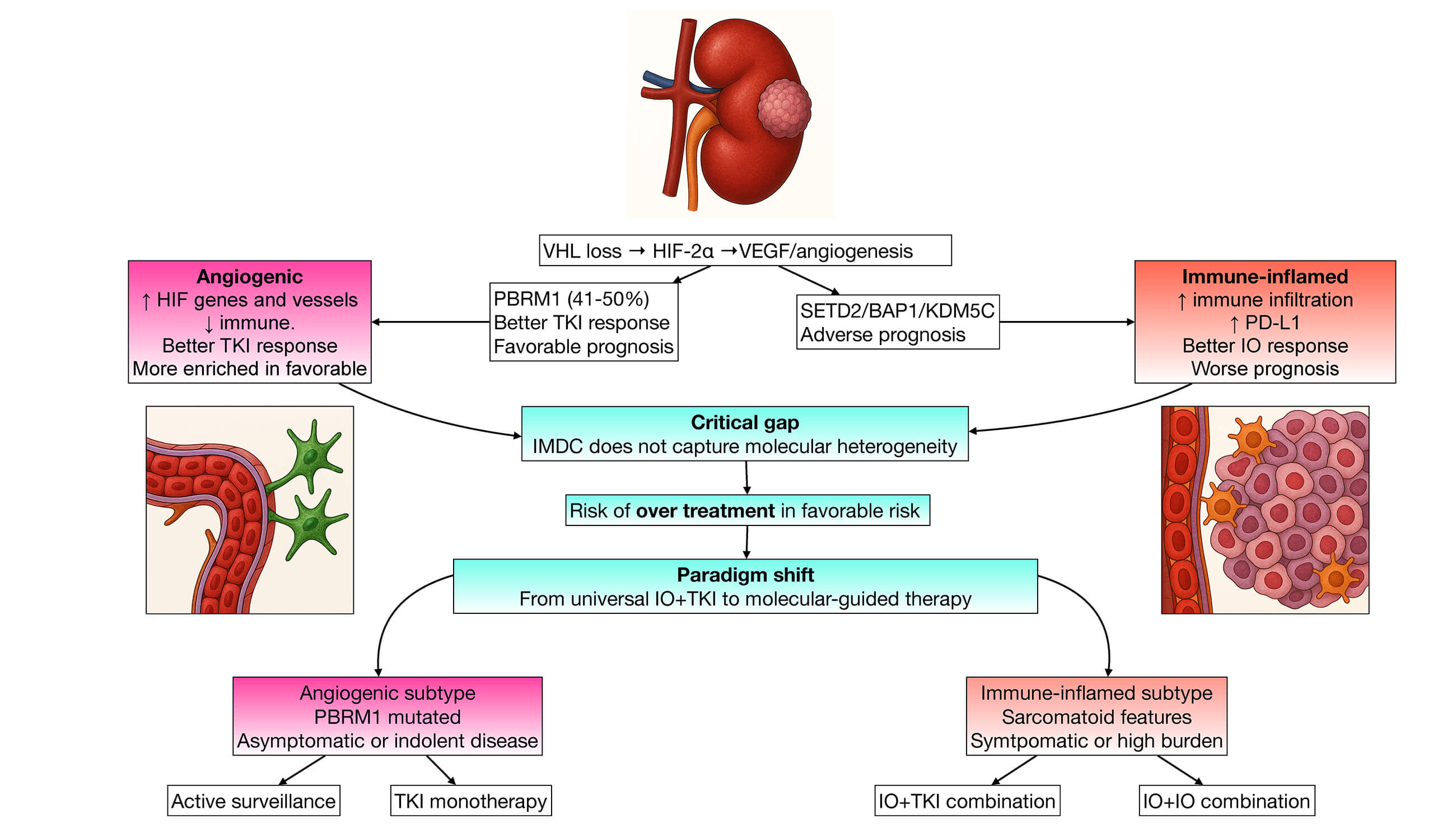
Figure 1: Proposed treatment-selection framework for IMDC favourable-risk metastatic clear-cell renal cell carcinoma (ccRCC), integrating clinical features and candidate biomarkers. Left panel (clinical algorithm): Patients with oligometastatic disease amenable to locoregional therapy may be considered for metastasis-directed treatment (surgery and/or stereotactic body radiotherapy [SBRT]) to metastases and/or the primary tumour; if rendered M1-NED after nephrectomy and MDT, adjuvant pembrolizumab may be considered. In patients not suitable for locoregional therapy, sarcomatoid features favour an immune checkpoint inhibitor doublet (IO+IO). Patients who are symptomatic or have high tumour burden requiring rapid disease control are directed toward an IO+TKI regimen. Patients meeting de-escalation criteria (asymptomatic, low-volume, indolent kinetics, and no imminent risk of organ-threatening progression) may be managed with VEGF-TKI monotherapy or active surveillance (AS), with escalation to systemic combination therapy if progression or symptoms develop. When none of the above criteria clearly apply, treatment is individualised based on the physician and patient preference, comorbidities, and access. Right panel (molecularly guided therapy—investigational): Two broad transcriptional phenotypes recur across ccRCC classification systems: an immune-inflamed state (higher immune infiltration and PD-L1 expression), associated with poorer baseline prognosis but potentially greater sensitivity to immunotherapy, and an angiogenic state (high HIF/angiogenesis-related gene expression), associated with favourable prognosis and relative VEGF-TKI sensitivity. Selected tumour alterations are shown as candidate prognostic/predictive correlates, including PBRM1 (often linked to more favourable biology) and BAP1/SETD2/KDM5C (often linked to adverse prognosis). These biomarkers are not yet validated to direct routine first-line selection and should be interpreted as hypothesis-generating. Abbreviations: AS, active surveillance; IO, immune checkpoint inhibitor; TKI, VEGF receptor tyrosine kinase inhibitor; SBRT, stereotactic body radiotherapy; PD-L1, programmed death-ligand 1; HIF, hypoxia-inducible factor.
IO+TKI/IO+IO: The principal advantages of IO+TKI regimens are higher ORRs and a greater probability of complete response (Table 2), which are valuable for symptomatic patients or those requiring rapid tumour control. Cross-trial comparisons between different IO+TKI combinations are inappropriate due to differing populations and designs. TKIs vary in potency, spectrum of kinase inhibition, and toxicity profile; choice should reflect clinician experience and comorbidities [112]. Incorporating checkpoint blockade (IO+IO or IO+TKI) offers the possibility of prolonged disease control and is often preferred in younger, fitter patients with longer life expectancy. The IMDC favourable-risk category likely contains molecular subsets that derive marked benefit from immunotherapy but are not identifiable with current clinical risk models, and later-line IO may be precluded by patient attrition. Disadvantages include higher costs and the risk of immune-related adverse events (irAEs). However, no validated predictive biomarkers reliably identify patients likely to achieve durable benefit, underscoring the limitations of IMDC alone for IO selection in favourable-risk disease.
IO+IO offers deep and durable responses in some patients, a finite treatment course (a fixed 2-year duration is a reasonable strategy, supported indirectly by contemporary IO+TKI trial designs), and avoidance of chronic VEGF-TKI toxicities. These advantages are counterbalanced by the higher rates of immune-related adverse events and lower ORR with a greater proportion of primary PD compared with IO+TKI. Nivolumab plus ipilimumab has a substantially higher immune-mediated toxicity than TKI+IO therapies, with any-grade irAEs in most patients and grade ≥ 3 irAEs in roughly one-third across the RCC series. While IO+TKI regimens exhibit similar or higher overall grade ≥ 3 AE rates (approximately 70–80%) due to the VEGFR–TKI component, grade ≥ 3 immune-mediated events are generally in the 5–10% range [113,114]. Patients with low-volume disease who prioritise durable control and the possibility of treatment-free intervals may be well suited to an IO+IO regimen, acknowledging its lower likelihood of achieving an early response.
Patient comorbidities can help steer regimen selection. Individuals with cardiovascular disease or poorly controlled hypertension, a history or high risk of thromboembolism, clinically significant proteinuria or chronic kidney disease, or likelihood of major surgery are often suboptimal candidates for VEGF-TKIs. Conversely, patients with clinically significant autoimmune disease or a history of solid-organ transplantation face an increased risk of irAEs with checkpoint inhibitors [115]. irAEs are an on-target consequence of immune checkpoint blockade, arising from loss of peripheral tolerance and amplification of autoreactive immunity [116]. This risk–benefit trade-off becomes particularly salient when the absolute efficacy advantage is small, as may occur in selected favourable-risk disease. In IO+TKI regimens, early recognition of toxicity and accurate attribution (immune-mediated versus VEGFR on-target effects) are crucial, as initial management often diverges: irAEs typically require treatment interruption and immunosuppression, whereas TKI toxicities are usually addressed with supportive measures plus dose interruption and/or reduction [117,118].
When irAEs are suspected, infection, disease progression, and alternative aetiologies should be excluded [119,120]. Grade 1 events are often managed symptomatically with close monitoring, while grade ≥ 2 generally warrants holding immunotherapy and initiating corticosteroids, followed by a gradual taper over several weeks to minimise rebound. Endocrinopathies usually require hormone replacement rather than prolonged high-dose steroids, and steroid-refractory toxicity may necessitate organ-specific second-line immunosuppression with multidisciplinary input.
In contrast, VEGFR–TKI adverse effects (e.g., hypertension, diarrhoea, hand–foot syndrome, mucositis, fatigue, proteinuria, transaminitis, hypothyroidism) are best mitigated through proactive monitoring and targeted supportive care, using temporary interruptions and stepwise dose reductions to restore tolerability while preserving efficacy [121,122]. Overall quality of life is broadly similar with IO+TKI and TKI alone, and appears higher with IO+IO than with TKI in the overall population [123].
Sarcomatoid dedifferentiation is present in 5–10% of mRCC cases overall; however, only a small minority of these cases are IMDC favourable risk [124]. In the sarcomatoid subset of the CheckMate-214 trial, nivolumab plus ipilimumab yielded superior outcomes versus sunitinib at 5 years: median OS was 48.6 vs. 14.2 months (HR 0.46), with benefits irrespective of PD-L1 status [125]. IO+TKI combinations are also effective in this phenotype [126].
TKI monotherapy/AS: VEGF-TKI alone remains appropriate for patients who do not require maximal response rates (e.g., asymptomatic individuals or those with metachronous, indolent recurrences). Due to extensive clinical experience and well-characterised safety profiles, we favour sunitinib or pazopanib over less established first-line TKIs. Newer agents such as cabozantinib, tivozanib, and axitinib are better reserved for subsequent lines, consistent with their evidence base [127]. AS remains a reasonable alternative for appropriately selected patients with indolent tumour biology (Table 3), particularly where competing comorbidities shorten life expectancy or reduce tolerance for treatment-related toxicity. AS and VEGF-TKI monotherapy are pragmatic approaches for favourable-risk patients in low- to middle-income settings [128,129,130]. Sunitinib and pazopanib present a less expensive alternative to newer TKIs, and immunotherapy can be used in later lines of treatment according to the CheckMate-025 trial [131,132]. Where IO+IO or IO+TKI are accessible, their use should be prioritised for higher-risk disease as absolute benefits are greater.
Metastatic site: Traditional risk models do not incorporate metastatic sites, despite clear differences in prognosis [133,134]. Certain metastatic sites, such as pancreatic/glandular regions, lymph nodes only, and lungs, hold better prognoses, making them ideal for de-escalation strategies such as VEGF-TKI and AS. Pancreatic-tropic ccRCC often follows an indolent course and is enriched for angiogenic programs, frequent PBRM1 loss, and relatively fewer aggressive alterations (e.g., BAP1), aligning with VEGF-TKI sensitivity [135]. Hepatic and bone metastases are associated with aggressive biology and worse prognosis [136,137,138]. In such cases, the adverse prognostic impact of liver or bone involvement should override IMDC favourable status; de-escalation strategies such as AS or TKI monotherapy are generally inappropriate.
Locoregional treatment: Metastasis-directed therapy (MDT) such as surgery, stereotactic body radiotherapy, and ablation can delay or avoid systemic therapy. Favourable features include ≤ 3–5 lesions amenable to complete ablation/resection, favourable/intermediate IMDC risk, long disease-free interval (>1–2 years), good performance status, and lung-dominant metastases. Patients achieving M1 NED (no evidence of disease) after nephrectomy and MDT have improved OS with adjuvant pembrolizumab following nephrectomy and MDT. AS is also acceptable in late metachronous M1-NED recurrences. Upfront cytoreductive nephrectomy (CN) is no longer routine where systemic therapy is indicated [139], but may be considered in favourable-risk patients. The CARMENA [140,141] and SURTIME trials [142] favoured initial systemic treatment with TKIs. In the current treatment landscape, retrospective series [143] and meta-analyses [144,145] show that CN is consistently associated with better OS in ICI-treated mRCC, but the data are retrospective and subject to confounding factors. Current management usually reserves CN for fit patients with favourable or selected intermediate risk, low metastatic burden, or potentially achievable eradication. Palliative CN remains appropriate for uncontrolled bleeding, pain, or obstruction.
Treatment duration: Contemporary trials have largely standardised anti–PD-L1 duration at 2 years; the optimal duration of VEGF-TKI remains undefined. TKIs are traditionally continued until unacceptable toxicity or progression [146]. Data supporting elective ‘drug holidays’ or discontinuation are limited; however, this may be considered in patients with persistent TKI-related toxicity and durable disease control after 2 years of therapy.
Clinical trials are usually conducted in the general ccRCC population, with favourable-risk patients remaining a minority. This hinders the interpretation of results in this subpopulation, as trials are not sufficiently powered to detect significant differences between groups. The IMDC favourable-risk label identifies a population for whom less intensive strategies (e.g., AS or VEGF-TKI monotherapy) may be appropriate. This label is necessary, but not sufficient, for de-escalation eligibility. Clinical features indicating indolent biology, such as metastatic sites with good prognoses (lungs/lymph nodes/pancreas), slow growth, and minimal symptoms, should guide eligibility in prospective de-escalation studies. Such studies should include standardised escalation triggers, QoL measures, and economic endpoints. Drug exposure reduction strategies are being tested, with new trials exploring alternate dosing of cabozantinib and imaging-guided treatment holidays.
Research in the HIF pathway/angiogenesis genes associated with favourable-risk and ‘angiogenic’ molecular subtypes could lead to actionable targets. A bispecific PD-1/VEGF mAb (ivonescimab/AK112) antibody is under analysis in RCC studies, with a planned Ib/II single-arm trial confined to IMDC favourable-risk, first-line patients (NCT06472895). In the phase III LITESPARK-005 study, belzutifan (an HIF-2α inhibitor which targets the truncal pVHL/HIF axis [29]) improved PFS and ORR (vs. everolimus) in previously treated ccRCC with improved patient-reported outcomes and QoL [147,148]. The favourable toxicity profile and on-target mechanism make HIF-2α inhibitors particularly suitable as future first-line de-escalation strategies in favourable-risk disease. A randomised trial will compare AS versus belzutifan (NCT07023432).
Personalised therapy, in which first-line choice is driven by tumour biology, is under investigation in clinical trials using tumour molecular subgroups. The objective is to avoid unnecessary toxicity and cost by exploiting tractable vulnerabilities. Two prospective programs explicitly test transcriptomic subtyping to guide therapy. The BIONIKK phase II trial assigned treatment according to the French group 35-gene classifier (ccRCC1–4) [58,149]. The ccRCC2 showed ORR 50% with sunitinib versus 51% nivolumab + ipilimumab. The hypothesis-generating data demonstrate the feasibility of first-line personalisation using a transcriptomic subtype and suggest that ccRCC2 is highly TKI-responsive yet may benefit from IO. The ongoing OPTIC RCC phase II trial, a biomarker-guided study, uses RNA-seq clusters derived from IMmotion151 to assign therapy, with angiogenic clusters (1/2) receiving nivolumab + cabozantinib (IO+TKI) [150]. Biologically meaningful ccRCC subtypes can be acted on prospectively, but routine use awaits assay standardisation, solutions to sampling heterogeneity, phase III-level proof of predictive utility, and practical/financial solutions.
Radiopharmaceutical strategies, exemplified by CAIX-targeted 177Lu-girentuximab combined with nivolumab+cabozantinib (STARLITE-1), aim to pair tumour-directed radiation with IO+TKI. Cellular therapies are re-entering RCC via CD70-directed platforms (e.g., allogeneic CAR-T ALLO-316) with early signals of activity in heavily pretreated ccRCC [151]. Vaccines are re-emerging with stronger evidence: while a multipeptide vaccine (IMA901) failed to improve survival when added to sunitinib in metastatic ccRCC, personalised neoantigen peptide vaccination in resected high-risk RCC has demonstrated consistent immunogenicity with vaccine-reactive T cells, supporting combination trial designs [152,153]. Next-generation immunomodulators, including engineered IL-2 agonists and PD-L1-VEGF bispecific antibodies, are being developed to intensify antitumor immunity while improving tolerability and potentially overcoming resistance [154,155].
IO+TKI combinations have reshaped ccRCC care, but most metastatic cases still progress, and effective later-line options remain limited. IMDC risk stratification will continue to guide treatment selection, yet it should not be the sole driver of therapy choice. In favourable-risk disease, the typically indolent course and VEGF sensitivity support TKI monotherapy or AS for carefully selected, asymptomatic patients with low-burden, slow-growing tumours. Given its higher toxicity and cost, IO+TKI should not be a default approach without a consistent overall survival benefit in this subgroup. Prospective trials are needed to test AS, planned treatment breaks, and other de-escalation strategies—particularly in resource-limited settings—while measuring survival, QoL, and cost-effectiveness against continuous therapy. Achieving safe de-escalation will require biomarker-driven personalisation, as clinical prognostic models only indirectly reflect tumour biology; robust predictive biomarkers, especially for immunotherapy benefit; and lower-toxicity novel agents.
Acknowledgement:
Funding Statement: The authors received no specific funding for this study.
Author Contributions: Alejandro Valdés (conceptualization, investigation, project administration, supervision, writing—original draft, writing—review & editing), Jaime González-Montero (investigation, project administration, writing—original draft, writing—review & editing), Carlos Rojas (investigation, writing—original draft, writing—review & editing), Mauricio Burotto (conceptualization, investigation, project administration, supervision, writing—original draft, writing—review & editing). All authors reviewed and approved the final version of the manuscript.
Availability of Data and Materials: Not applicable.
Ethics Approval: Not applicable.
Conflicts of Interest: Alejandro Valdés has received payments for ad boards and lectures from Merck, Bristol Myers Squibb, MSN labs and Pfizer. Carlos Rojas has received payments for lectures from Roche/Genentech, Bristol Myers Squib, MSD Oncology, Novartis, and AstraZeneca. Mauricio Burotto has received payments for lectures from Roche/Genentech, Bristol Myers Squibb, MSD Oncology, Novartis, and AstraZeneca.
References
1. Bukavina L , Bensalah K , Bray F , Carlo M , Challacombe B , Karam JA , et al. Epidemiology of renal cell carcinoma: 2022 update. Eur Urol. 2022; 82( 5): 529– 42. doi:10.1016/j.eururo.2022.08.019. [Google Scholar] [CrossRef]
2. Cirillo L , Innocenti S , Becherucci F . Global epidemiology of kidney cancer. Nephrol Dial Transpl. 2024; 39( 6): 920– 8. doi:10.1093/ndt/gfae036. [Google Scholar] [CrossRef]
3. WHO Classification of Tumours Editorial Board, International Agency for Research on Cancer . Urinary and Male Genital Tumours. Lyon, France: International Agency for Research on Cancer; 2022. 590 p. [Google Scholar]
4. Hsieh JJ , Purdue MP , Signoretti S , Swanton C , Albiges L , Schmidinger M , et al. Renal cell carcinoma. Nat Rev Dis Primers. 2017; 3: 17009. doi:10.1038/nrdp.2017.9. [Google Scholar] [CrossRef]
5. Demasure S , Spriet I , Debruyne PR , Laenen A , Wynendaele W , Baldewijns M , et al. Overall survival improvement in patients with metastatic clear-cell renal cell carcinoma between 2000 and 2020: A retrospective cohort study. Acta Oncol. 2022; 61( 1): 22– 9. doi:10.1080/0284186X.2021.1989720. [Google Scholar] [CrossRef]
6. Dutcher JP , Flippot R , Fallah J , Escudier B . On the shoulders of giants: The evolution of renal cell carcinoma treatment-cytokines, targeted therapy, and immunotherapy. Am Soc Clin Oncol Educ Book. 2020; 40: 1– 18. doi:10.1200/EDBK_280817. [Google Scholar] [CrossRef]
7. Navani V , Heng DYC . Treatment selection in first-line metastatic renal cell carcinoma-the contemporary treatment paradigm in the age of combination therapy: A review. JAMA Oncol. 2022; 8( 2): 292– 9. doi:10.1001/jamaoncol.2021.4337. [Google Scholar] [CrossRef]
8. Heng DYC , Xie W , Regan MM , Warren MA , Golshayan AR , Sahi C , et al. Prognostic factors for overall survival in patients with metastatic renal cell carcinoma treated with vascular endothelial growth factor-targeted agents: Results from a large, multicenter study. J Clin Oncol. 2009; 27( 34): 5794– 9. doi:10.1200/JCO.2008.21.4809. [Google Scholar] [CrossRef]
9. Powles T , Albiges L , Bex A , Comperat E , Grünwald V , Kanesvaran R , et al. Renal cell carcinoma: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann Oncol. 2024; 35( 8): 692– 706. doi:10.1016/j.annonc.2024.05.537. [Google Scholar] [CrossRef]
10. Bex A , Abu Ghanem Y , Albiges L , Bonn S , Campi R , Capitanio U , et al. European association of urology guidelines on renal cell carcinoma: The 2025 update. Eur Urol. 2025; 87( 6): 683– 96. doi:10.1016/j.eururo.2025.02.020. [Google Scholar] [CrossRef]
11. Motzer RJ , Jonasch E , Agarwal N , Alva A , Baine M , Beckermann K , et al. Kidney cancer, version 3.2022, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2022; 20( 1): 71– 90. doi:10.6004/jnccn.2022.0001. [Google Scholar] [CrossRef]
12. Casuscelli J , Vano YA , Fridman WH , Hsieh JJ . Molecular classification of renal cell carcinoma and its implication in future clinical practice. Kidney Cancer. 2017; 1( 1): 3– 13. doi:10.3233/KCA-170008. [Google Scholar] [CrossRef]
13. Motzer RJ , Mazumdar M , Bacik J , Berg W , Amsterdam A , Ferrara J . Survival and prognostic stratification of 670 patients with advanced renal cell carcinoma. J Clin Oncol. 1999; 17( 8): 2530– 40. doi:10.1200/JCO.1999.17.8.2530. [Google Scholar] [CrossRef]
14. Motzer RJ , Bacik J , Murphy BA , Russo P , Mazumdar M . Interferon-Alfa as a comparative treatment for clinical trials of new therapies against advanced renal cell carcinoma. J Clin Oncol. 2002; 20( 1): 289– 96. doi:10.1200/JCO.2002.20.1.289. [Google Scholar] [CrossRef]
15. Heng DYC , Xie W , Regan MM , Harshman LC , Bjarnason GA , Vaishampayan UN , et al. External validation and comparison with other models of the International Metastatic Renal-Cell Carcinoma Database Consortium prognostic model: A population-based study. Lancet Oncol. 2013; 14( 2): 141– 8. doi:10.1016/S1470-2045(12)70559-4. [Google Scholar] [CrossRef]
16. Tanaka N , Mizuno R , Ito K , Shirotake S , Yasumizu Y , Masunaga A , et al. External validation of the MSKCC and IMDC risk models in patients treated with targeted therapy as a first-line and subsequent second-line treatment: A Japanese multi-institutional study. Eur Urol Focus. 2016; 2( 3): 303– 9. doi:10.1016/j.euf.2015.11.001. [Google Scholar] [CrossRef]
17. Schmidt AL , Xie W , Gan CL , Wells C , Dudani S , Donskov F , et al. The very favorable metastatic renal cell carcinoma (mRCC) risk group: Data from the International Metastatic RCC Database Consortium (IMDC). J Clin Oncol. 2021; 39 (6_suppl):339. doi:10.1200/JCO.2021.39.6_suppl.339. [Google Scholar] [CrossRef]
18. Yekedüz E , Karakaya S , Ertürk İ , Tural D , Uçar G , Şentürk Öztaş N , et al. External validation of a novel risk model in patients with favorable risk renal cell carcinoma defined by international metastatic renal cell carcinoma database consortium (IMDC): Results from the Turkish oncology group kidney cancer consortium (TKCC) database. Clin Genitourin Cancer. 2023; 21( 1): 175– 82. doi:10.1016/j.clgc.2022.07.006. [Google Scholar] [CrossRef]
19. Ernst MS , Navani V , Wells JC , Donskov F , Basappa N , Labaki C , et al. Outcomes for international metastatic renal cell carcinoma database consortium prognostic groups in contemporary first-line combination therapies for metastatic renal cell carcinoma. Eur Urol. 2023; 84( 1): 109– 16. doi:10.1016/j.eururo.2023.01.001. [Google Scholar] [CrossRef]
20. Dudani S , Savard MF , Heng DYC . An update on predictive biomarkers in metastatic renal cell carcinoma. Eur Urol Focus. 2020; 6( 1): 34– 6. doi:10.1016/j.euf.2019.04.004. [Google Scholar] [CrossRef]
21. Tannir NM , Albigès L , McDermott DF , Burotto M , Choueiri TK , Hammers HJ , et al. Nivolumab plus ipilimumab versus sunitinib for first-line treatment of advanced renal cell carcinoma: Extended 8-year follow-up results of efficacy and safety from the phase III CheckMate 214 trial. Ann Oncol. 2024; 35( 11): 1026– 38. doi:10.1016/j.annonc.2024.07.727. [Google Scholar] [CrossRef]
22. Ballman KV . Biomarker: Predictive or prognostic? J Clin Oncol. 2015; 33( 33): 3968– 71. doi:10.1200/JCO.2015.63.3651. [Google Scholar] [CrossRef]
23. Bolek H , Yekedüz E , Ürün Y . Combination therapies in patients with favorable risk metastatic renal cell Carcinoma: A Systematic Review and Meta-Analysis. Cancer Treat Rev. 2024; 122: 102667. doi:10.1016/j.ctrv.2023.102667. [Google Scholar] [CrossRef]
24. Mantia CM , Jegede OA , McDermott DF , Heng DYC , Xie W , Choueiri TK , et al. Long-term performance of prognostic models for advanced renal cell carcinoma in the era of improved survival with immune checkpoint inhibitors. JCO Oncol Pract. 2025: OP2500089. doi:10.1200/OP-25-00089. [Google Scholar] [CrossRef]
25. Voss MH , Reising A , Cheng Y , Patel P , Marker M , Kuo F , et al. Genomically annotated risk model for advanced renal-cell carcinoma: A retrospective cohort study. Lancet Oncol. 2018; 19( 12): 1688– 98. doi:10.1016/S1470-2045(18)30648-X. [Google Scholar] [CrossRef]
26. Zhao L , Lee VHF , Ng MK , Yan H , Bijlsma MF . Molecular subtyping of cancer: Current status and moving toward clinical applications. Brief Bioinform. 2019; 20( 2): 572– 84. doi:10.1093/bib/bby026. [Google Scholar] [CrossRef]
27. Linehan WM , Ricketts CJ . The Cancer Genome Atlas of renal cell carcinoma: Findings and clinical implications. Nat Rev Urol. 2019; 16( 9): 539– 52. doi:10.1038/s41585-019-0211-5. [Google Scholar] [CrossRef]
28. Gossage L , Eisen T , Maher ER . VHL the story of a tumour suppressor gene. Nat Rev Cancer. 2015; 15( 1): 55– 64. doi:10.1038/nrc3844. [Google Scholar] [CrossRef]
29. Mazumder S , Higgins PJ , Samarakoon R . Downstream targets of VHL/HIF-α signaling in renal clear cell carcinoma progression: Mechanisms and therapeutic relevance. Cancers. 2023; 15( 4): 1316. doi:10.3390/cancers15041316. [Google Scholar] [CrossRef]
30. Liao C , Hu L , Zhang Q . Von Hippel-Lindau protein signalling in clear cell renal cell carcinoma. Nat Rev Urol. 2024; 21( 11): 662– 75. doi:10.1038/s41585-024-00876-w. [Google Scholar] [CrossRef]
31. Walton J , Lawson K , Prinos P , Finelli A , Arrowsmith C , Ailles L . PBRM1, SETD2 and BAP1—The trinity of 3p in clear cell renal cell carcinoma. Nat Rev Urol. 2023; 20( 2): 96– 115. doi:10.1038/s41585-022-00659-1. [Google Scholar] [CrossRef]
32. Carril-Ajuria L , Santos M , Roldán-Romero JM , Rodriguez-Antona C , de Velasco G . Prognostic and predictive value of PBRM1 in clear cell renal cell carcinoma. Cancers. 2019; 12( 1): 16. doi:10.3390/cancers12010016. [Google Scholar] [CrossRef]
33. Peña-Llopis S , Vega-Rubín-de-Celis S , Liao A , Leng N , Pavía-Jiménez A , Wang S , et al. BAP1 loss defines a new class of renal cell carcinoma. Nat Genet. 2012; 44( 7): 751– 9. doi:10.1038/ng.2323. [Google Scholar] [CrossRef]
34. Santos VE , da Costa WH , Bezerra SM , da Cunha IW , Nobre JQC , Brazão ES , et al. Prognostic impact of loss of SETD2 in clear cell renal cell carcinoma. Clin Genitourin Cancer. 2021; 19( 4): 339– 45. doi:10.1016/j.clgc.2021.03.003. [Google Scholar] [CrossRef]
35. Ricketts CJ , Linehan WM . Gender specific mutation incidence and survival associations in clear cell renal cell carcinoma (CCRCC). PLoS One. 2015; 10( 10): e0140257. doi:10.1371/journal.pone.0140257. [Google Scholar] [CrossRef]
36. Braun DA , Hou Y , Bakouny Z , Ficial M , Sant’ Angelo M , Forman J , et al. Interplay of somatic alterations and immune infiltration modulates response to PD-1 blockade in advanced clear cell renal cell carcinoma. Nat Med. 2020; 26( 6): 909– 18. doi:10.1038/s41591-020-0839-y. [Google Scholar] [CrossRef]
37. Díaz-Montero CM , Rini BI , Finke JH . The immunology of renal cell carcinoma. Nat Rev Nephrol. 2020; 16( 12): 721– 35. doi:10.1038/s41581-020-0316-3. [Google Scholar] [CrossRef]
38. Motzer RJ , Banchereau R , Hamidi H , Powles T , McDermott D , Atkins MB , et al. Molecular subsets in renal cancer determine outcome to checkpoint and angiogenesis blockade. Cancer Cell. 2020; 38( 6): 803– 17.e4. doi:10.1016/j.ccell.2020.10.011. [Google Scholar] [CrossRef]
39. Gerlinger M , Rowan AJ , Horswell S , Larkin J , Endesfelder D , Gronroos E , et al. Intratumor heterogeneity and branched evolution revealed by multiregion sequencing. N Engl J Med. 2012; 366( 10): 883– 92. doi:10.1056/NEJMoa1113205. [Google Scholar] [CrossRef]
40. Turajlic S , Xu H , Litchfield K , Rowan A , Chambers T , Lopez JI , et al. Tracking cancer evolution reveals constrained routes to metastases: TRACERx renal. Cell. 2018; 173( 3): 581– 94.e12. doi:10.1016/j.cell.2018.03.057. [Google Scholar] [CrossRef]
41. Mitchell TJ , Turajlic S , Rowan A , Nicol D , Farmery JHR , O’Brien T , et al. Timing the landmark events in the evolution of clear cell renal cell cancer: TRACERx renal. Cell. 2018; 173( 3): 611– 23.e17. doi:10.1016/j.cell.2018.02.020. [Google Scholar] [CrossRef]
42. Dizman N , Philip EJ , Pal SK . Genomic profiling in renal cell carcinoma. Nat Rev Nephrol. 2020; 16( 8): 435– 51. doi:10.1038/s41581-020-0301-x. [Google Scholar] [CrossRef]
43. Brannon AR , Reddy A , Seiler M , Arreola A , Moore DT , Pruthi RS , et al. Molecular stratification of clear cell renal cell carcinoma by consensus clustering reveals distinct subtypes and survival patterns. Genes Cancer. 2010; 1( 2): 152– 63. doi:10.1177/1947601909359929. [Google Scholar] [CrossRef]
44. Brannon AR , Haake SM , Hacker KE , Pruthi RS , Wallen EM , Nielsen ME , et al. Meta-analysis of clear cell renal cell carcinoma gene expression defines a variant subgroup and identifies gender influences on tumor biology. Eur Urol. 2012; 61( 2): 258– 68. doi:10.1016/j.eururo.2011.10.007. [Google Scholar] [CrossRef]
45. Cancer Genome Atlas Research Network . Comprehensive molecular characterization of clear cell renal cell carcinoma. Nature. 2013; 499 (7456): 43–9. doi:10.1038/nature12222. [Google Scholar] [CrossRef]
46. Beuselinck B , Job S , Becht E , Karadimou A , Verkarre V , Couchy G , et al. Molecular subtypes of clear cell renal cell carcinoma are associated with sunitinib response in the metastatic setting. Clin Cancer Res. 2015; 21( 6): 1329– 39. doi:10.1158/1078-0432.CCR-14-1128. [Google Scholar] [CrossRef]
47. Saliby RM , Labaki C , Jammihal TR , Xie W , Sun M , Shah V , et al. Impact of renal cell carcinoma molecular subtypes on immunotherapy and targeted therapy outcomes. Cancer Cell. 2024; 42( 5): 732– 5. doi:10.1016/j.ccell.2024.03.002. [Google Scholar] [CrossRef]
48. Saliby RM , Saad E , Kashima S , Schoenfeld DA , Braun DA . Update on biomarkers in renal cell carcinoma. Am Soc Clin Oncol Educ Book. 2024; 44( 2): e430734. doi:10.1200/EDBK_430734. [Google Scholar] [CrossRef]
49. Hsieh JJ , Le VH , Oyama T , Ricketts CJ , Ho TH , Cheng EH . Chromosome 3p loss-orchestrated VHL, HIF, and epigenetic deregulation in clear cell renal cell carcinoma. J Clin Oncol. 2018; 36( 36): JCO2018792549. doi:10.1200/JCO.2018.79.2549. [Google Scholar] [CrossRef]
50. Rosellini M , Marchetti A , Mollica V , Rizzo A , Santoni M , Massari F . Prognostic and predictive biomarkers for immunotherapy in advanced renal cell carcinoma. Nat Rev Urol. 2023; 20( 3): 133– 57. doi:10.1038/s41585-022-00676-0. [Google Scholar] [CrossRef]
51. Blum KA , Gupta S , Tickoo SK , Chan TA , Russo P , Motzer RJ , et al. Sarcomatoid renal cell carcinoma: Biology, natural history and management. Nat Rev Urol. 2020; 17( 12): 659– 78. doi:10.1038/s41585-020-00382-9. [Google Scholar] [CrossRef]
52. Rini BI , Albiges L , Tang X , Koeppen H , Bex A , Suárez C , et al. Circulating kidney injury molecule-1 (KIM-1) and association with outcome to adjuvant immunotherapy in renal cell carcinoma. Ann Oncol. 2025; 36( 12): 1525– 34. doi:10.1016/j.annonc.2025.08.007. [Google Scholar] [CrossRef]
53. Xu W , Vemula SV , Motzer RJ , Chhibber A , Chowbene D , Perrot N , et al. Evaluation of circulating kidney injury marker-1 (KIM-1) as a prognostic and predictive biomarker in advanced renal cell carcinoma (aRCC): Post-hoc analysis of CheckMate 214. J Clin Oncol. 2025; 43(5_suppl): 437. doi:10.1200/JCO.2025.43.5_suppl.437. [Google Scholar] [CrossRef]
54. Lyskjær I , Iisager L , Axelsen CT , Nielsen TK , Dyrskjøt L , Fristrup N . Management of renal cell carcinoma: Promising biomarkers and the challenges to reach the clinic. Clin Cancer Res. 2024; 30( 4): 663– 72. doi:10.1158/1078-0432.CCR-23-1892. [Google Scholar] [CrossRef]
55. Malone ER , Sim HW , Stundzia A , Pierre S , Metser U , O’Malley M , et al. Predictive radiomics signature for treatment response to nivolumab in patients with advanced renal cell carcinoma. Can Urol Assoc J. 2022; 16( 2): E94– 101. doi:10.5489/cuaj.7467. [Google Scholar] [CrossRef]
56. Koh Y , Nakano K , Katayama K , Yamamichi G , Yumiba S , Tomiyama E , et al. Early dynamics of circulating tumor DNA predict clinical response to immune checkpoint inhibitors in metastatic renal cell carcinoma. Int J Urol. 2022; 29( 5): 462– 9. doi:10.1111/iju.14816. [Google Scholar] [CrossRef]
57. Motzer RJ , Choueiri TK , McDermott DF , Powles T , Vano YA , Gupta S , et al. Biomarker analysis from CheckMate 214: Nivolumab plus ipilimumab versus sunitinib in renal cell carcinoma. J Immunother Cancer. 2022; 10( 3): e004316. doi:10.1136/jitc-2021-004316. [Google Scholar] [CrossRef]
58. Vano YA , Elaidi R , Bennamoun M , Chevreau C , Borchiellini D , Pannier D , et al. Nivolumab, nivolumab-ipilimumab, and VEGFR-tyrosine kinase inhibitors as first-line treatment for metastatic clear-cell renal cell carcinoma (BIONIKK): A biomarker-driven, open-label, non-comparative, randomised, phase 2 trial. Lancet Oncol. 2022; 23( 5): 612– 24. doi:10.1016/S1470-2045(22)00128-0. [Google Scholar] [CrossRef]
59. Motzer RJ , Porta C , Eto M , Hutson TE , Rha SY , Merchan JR , et al. Biomarker analyses from the phase III randomized CLEAR trial: Lenvatinib plus pembrolizumab versus sunitinib in advanced renal cell carcinoma. Ann Oncol. 2025; 36( 4): 375– 86. doi:10.1016/j.annonc.2024.12.003. [Google Scholar] [CrossRef]
60. Motzer RJ , Hutson TE , Tomczak P , Michaelson MD , Bukowski RM , Rixe O , et al. Sunitinib versus interferon Alfa in metastatic renal-cell carcinoma. N Engl J Med. 2007; 356( 2): 115– 24. doi:10.1056/NEJMoa065044. [Google Scholar] [CrossRef]
61. Motzer RJ , Hutson TE , Tomczak P , Michaelson MD , Bukowski RM , Oudard S , et al. Overall survival and updated results for sunitinib compared with interferon Alfa in patients with metastatic renal cell carcinoma. J Clin Oncol. 2009; 27( 22): 3584– 90. doi:10.1200/JCO.2008.20.1293. [Google Scholar] [CrossRef]
62. Sternberg CN , Davis ID , Mardiak J , Szczylik C , Lee E , Wagstaff J , et al. Pazopanib in locally advanced or metastatic renal cell carcinoma: Results of a randomized phase III trial. J Clin Oncol. 2010; 28( 6): 1061– 8. doi:10.1200/JCO.2009.23.9764. [Google Scholar] [CrossRef]
63. Sternberg CN , Hawkins RE , Wagstaff J , Salman P , Mardiak J , Barrios CH , et al. A randomised, double-blind phase III study of pazopanib in patients with advanced and/or metastatic renal cell carcinoma: Final overall survival results and safety update. Eur J Cancer. 2013; 49( 6): 1287– 96. doi:10.1016/j.ejca.2012.12.010. [Google Scholar] [CrossRef]
64. Escudier B , Eisen T , Stadler WM , Szczylik C , Oudard S , Siebels M , et al. Sorafenib in advanced clear-cell renal-cell carcinoma. N Engl J Med. 2007; 356( 2): 125– 34. doi:10.1056/NEJMoa060655. [Google Scholar] [CrossRef]
65. Escudier B , Eisen T , Stadler WM , Szczylik C , Oudard S , Staehler M , et al. Sorafenib for treatment of renal cell carcinoma: Final efficacy and safety results of the phase III treatment approaches in renal cancer global evaluation trial. J Clin Oncol. 2009; 27( 20): 3312– 8. doi:10.1200/JCO.2008.19.5511. [Google Scholar] [CrossRef]
66. Hutson TE , Lesovoy V , Al-Shukri S , Stus VP , Lipatov ON , Bair AH , et al. Axitinib versus sorafenib as first-line therapy in patients with metastatic renal-cell carcinoma: A randomised open-label phase 3 trial. Lancet Oncol. 2013; 14( 13): 1287– 94. doi:10.1016/S1470-2045(13)70465-0. [Google Scholar] [CrossRef]
67. Motzer RJ , Nosov D , Eisen T , Bondarenko I , Lesovoy V , Lipatov O , et al. Tivozanib versus sorafenib as initial targeted therapy for patients with metastatic renal cell carcinoma: Results from a phase III trial. J Clin Oncol. 2013; 31( 30): 3791– 9. doi:10.1200/JCO.2012.47.4940. [Google Scholar] [CrossRef]
68. Motzer RJ , Hutson TE , Cella D , Reeves J , Hawkins R , Guo J , et al. Pazopanib versus sunitinib in metastatic renal-cell carcinoma. N Engl J Med. 2013; 369( 8): 722– 31. doi:10.1056/NEJMoa1303989. [Google Scholar] [CrossRef]
69. Escudier B , Porta C , Bono P , Powles T , Eisen T , Sternberg CN , et al. Randomized, controlled, double-blind, cross-over trial assessing treatment preference for pazopanib versus sunitinib in patients with metastatic renal cell carcinoma: PISCES Study. J Clin Oncol. 2014; 32( 14): 1412– 8. doi:10.1200/JCO.2013.50.8267. [Google Scholar] [CrossRef]
70. Ruiz-Morales JM , Swierkowski M , Wells JC , Fraccon AP , Pasini F , Donskov F , et al. First-line sunitinib versus pazopanib in metastatic renal cell carcinoma: Results from the International Metastatic Renal Cell Carcinoma Database Consortium. Eur J Cancer. 2016; 65: 102– 8. doi:10.1016/j.ejca.2016.06.016. [Google Scholar] [CrossRef]
71. Kalra S , Rini BI , Jonasch E . Alternate sunitinib schedules in patients with metastatic renal cell carcinoma. Ann Oncol. 2015; 26( 7): 1300– 4. doi:10.1093/annonc/mdv030. [Google Scholar] [CrossRef]
72. Guida FM , Santoni M , Conti A , Burattini L , Savini A , Zeppola T , et al. Alternative dosing schedules for sunitinib as a treatment of patients with metastatic renal cell carcinoma. Crit Rev Oncol Hematol. 2014; 92( 3): 208– 17. doi:10.1016/j.critrevonc.2014.07.006. [Google Scholar] [CrossRef]
73. Motzer RJ , Hutson TE , Olsen MR , Hudes GR , Burke JM , Edenfield WJ , et al. Randomized phase II trial of sunitinib on an intermittent versus continuous dosing schedule as first-line therapy for advanced renal cell carcinoma. J Clin Oncol. 2012; 30( 12): 1371– 7. doi:10.1200/JCO.2011.36.4133. [Google Scholar] [CrossRef]
74. Atkinson BJ , Kalra S , Wang X , Bathala T , Corn P , Tannir NM , et al. Clinical outcomes for patients with metastatic renal cell carcinoma treated with alternative sunitinib schedules. J Urol. 2014; 191( 3): 611– 8. doi:10.1016/j.juro.2013.08.090. [Google Scholar] [CrossRef]
75. Najjar YG , Mittal K , Elson P , Wood L , Garcia JA , Dreicer R , et al. A 2 weeks on and 1 week off schedule of sunitinib is associated with decreased toxicity in metastatic renal cell carcinoma. Eur J Cancer. 2014; 50( 6): 1084– 9. doi:10.1016/j.ejca.2014.01.025. [Google Scholar] [CrossRef]
76. Lee JL , Kim MK , Park I , Ahn JH , Lee DH , Ryoo HM , et al. RandomizEd phase II trial of Sunitinib four weeks on and two weeks off versus Two weeks on and One week off in metastatic clear-cell type REnal cell carcinoma: RESTORE trial. Ann Oncol. 2015; 26( 11): 2300– 5. doi:10.1093/annonc/mdv357. [Google Scholar] [CrossRef]
77. Brown JE , Royle KL , Gregory W , Ralph C , Maraveyas A , Din O , et al. Temporary treatment cessation versus continuation of first-line tyrosine kinase inhibitor in patients with advanced clear cell renal cell carcinoma (STAR): An open-label, non-inferiority, randomised, controlled, phase 2/3 trial. Lancet Oncol. 2023; 24( 3): 213– 27. doi:10.1016/S1470-2045(22)00793-8. [Google Scholar] [CrossRef]
78. Powles T , Kayani I , Sharpe K , Lim L , Peters J , Stewart GD , et al. A prospective evaluation of VEGF-targeted treatment cessation in metastatic clear cell renal cancer. Ann Oncol. 2013; 24( 8): 2098– 103. doi:10.1093/annonc/mdt130. [Google Scholar] [CrossRef]
79. Motzer RJ , Tannir NM , McDermott DF , Arén Frontera O , Melichar B , Choueiri TK , et al. Nivolumab plus ipilimumab versus sunitinib in advanced renal-cell carcinoma. N Engl J Med. 2018; 378( 14): 1277– 90. doi:10.1056/NEJMoa1712126. [Google Scholar] [CrossRef]
80. Vasudev NS , Ainsworth G , Brown S , Pickering L , Waddell T , Fife K , et al. Standard versus modified ipilimumab, in combination with nivolumab, in advanced renal cell carcinoma: A randomized phase II trial (PRISM). J Clin Oncol. 2024; 42( 3): 312– 23. doi:10.1200/JCO.23.00236. [Google Scholar] [CrossRef]
81. McKay RR , McGregor BA , Xie W , Braun DA , Wei X , Kyriakopoulos CE , et al. Optimized management of nivolumab and ipilimumab in advanced renal cell carcinoma: A response-based phase II study (OMNIVORE). J Clin Oncol. 2020; 38( 36): 4240– 8. doi:10.1200/JCO.20.02295. [Google Scholar] [CrossRef]
82. Atkins MB , Jegede OA , Haas NB , McDermott DF , Bilen MA , Stein M , et al. Phase II study of nivolumab and salvage nivolumab/ipilimumab in treatment-naive patients with advanced clear cell renal cell carcinoma (HCRN GU16-260-cohort a). J Clin Oncol. 2022; 40( 25): 2913– 23. doi:10.1200/JCO.21.02938. [Google Scholar] [CrossRef]
83. Grimm MO , Esteban E , Barthélémy P , Schmidinger M , Busch J , Valderrama BP , et al. Tailored immunotherapy approach with nivolumab with or without nivolumab plus ipilimumab as immunotherapeutic boost in patients with metastatic renal cell carcinoma (TITAN-RCC): A multicentre, single-arm, phase 2 trial. Lancet Oncol. 2023; 24( 11): 1252– 65. doi:10.1016/S1470-2045(23)00449-7. [Google Scholar] [CrossRef]
84. McKay RR , Leucht K , Xie W , Jegede O , Braun DA , Atkins MB , et al. A pooled analysis of 3 phase II trials of salvage nivolumab/ipilimumab after nivolumab in renal cell carcinoma. Oncologist. 2024; 29( 4): 324– 31. doi:10.1093/oncolo/oyad298. [Google Scholar] [CrossRef]
85. Khan KA , Kerbel RS . Improving immunotherapy outcomes with anti-angiogenic treatments and vice versa. Nat Rev Clin Oncol. 2018; 15( 5): 310– 24. doi:10.1038/nrclinonc.2018.9. [Google Scholar] [CrossRef]
86. Lee WS , Yang H , Chon HJ , Kim C . Combination of anti-angiogenic therapy and immune checkpoint blockade normalizes vascular-immune crosstalk to potentiate cancer immunity. Exp Mol Med. 2020; 52( 9): 1475– 85. doi:10.1038/s12276-020-00500-y. [Google Scholar] [CrossRef]
87. Rini BI , Plimack ER , Stus V , Gafanov R , Hawkins R , Nosov D , et al. Pembrolizumab plus axitinib versus sunitinib for advanced renal-cell carcinoma. N Engl J Med. 2019; 380( 12): 1116– 27. doi:10.1056/NEJMoa1816714. [Google Scholar] [CrossRef]
88. Plimack ER , Powles T , Stus V , Gafanov R , Nosov D , Waddell T , et al. Pembrolizumab plus axitinib versus sunitinib as first-line treatment of advanced renal cell carcinoma: 43-month follow-up of the phase 3 KEYNOTE-426 study. Eur Urol. 2023; 84( 5): 449– 54. doi:10.1016/j.eururo.2023.06.006. [Google Scholar] [CrossRef]
89. Rini BI , Plimack ER , Stus V , Gafanov R , Waddell T , Nosov D , et al. Pembrolizumab plus axitinib versus sunitinib for advanced clear cell renal cell carcinoma: 5-year survival and biomarker analyses of the phase 3 KEYNOTE-426 trial. Nat Med. 2025; 31( 10): 3475– 84. doi:10.1038/s41591-025-03867-5. [Google Scholar] [CrossRef]
90. Powles T , Plimack ER , Soulières D , Waddell T , Stus V , Gafanov R , et al. Pembrolizumab plus axitinib versus sunitinib monotherapy as first-line treatment of advanced renal cell carcinoma (KEYNOTE-426): Extended follow-up from a randomised, open-label, phase 3 trial. Lancet Oncol. 2020; 21( 12): 1563– 73. doi:10.1016/S1470-2045(20)30436-8. [Google Scholar] [CrossRef]
91. Powles T , Burotto M , Escudier B , Apolo AB , Bourlon MT , Shah AY , et al. Nivolumab plus cabozantinib versus sunitinib for first-line treatment of advanced renal cell carcinoma: Extended follow-up from the phase III randomised CheckMate 9ER trial. ESMO Open. 2024; 9( 5): 102994. doi:10.1016/j.esmoop.2024.102994. [Google Scholar] [CrossRef]
92. Motzer RJ , Escudier B , Burotto M , Powles T , Apolo AB , Bourlon MT , et al. Nivolumab plus cabozantinib (N+C) vs. sunitinib (S) for previously untreated advanced renal cell carcinoma (aRCC): Final follow-up results from the CheckMate 9ER trial. J Clin Oncol. 2025; 43(5_suppl):439. doi:10.1200/JCO.2025.43.5_suppl.439. [Google Scholar] [CrossRef]
93. Choueiri TK , Powles T , Burotto M , Escudier B , Bourlon MT , Zurawski B , et al. Nivolumab plus cabozantinib versus sunitinib for advanced renal-cell carcinoma. N Engl J Med. 2021; 384( 9): 829– 41. doi:10.1056/NEJMoa2026982. [Google Scholar] [CrossRef]
94. Motzer RJ , Powles T , Burotto M , Escudier B , Bourlon MT , Shah AY , et al. Nivolumab plus cabozantinib versus sunitinib in first-line treatment for advanced renal cell carcinoma (CheckMate 9ER): Long-term follow-up results from an open-label, randomised, phase 3 trial. Lancet Oncol. 2022; 23( 7): 888– 98. doi:10.1016/S1470-2045(22)00290-X. [Google Scholar] [CrossRef]
95. Motzer R , Alekseev B , Rha SY , Porta C , Eto M , Powles T , et al. Lenvatinib plus pembrolizumab or everolimus for advanced renal cell carcinoma. N Engl J Med. 2021; 384( 14): 1289– 300. doi:10.1056/NEJMoa2035716. [Google Scholar] [CrossRef]
96. Choueiri TK , Eto M , Motzer R , De Giorgi U , Buchler T , Basappa NS , et al. Lenvatinib plus pembrolizumab versus sunitinib as first-line treatment of patients with advanced renal cell carcinoma (CLEAR): Extended follow-up from the phase 3, randomised, open-label study. Lancet Oncol. 2023; 24( 3): 228– 38. doi:10.1016/S1470-2045(23)00049-9. [Google Scholar] [CrossRef]
97. Motzer RJ , Porta C , Eto M , Powles T , Grünwald V , Hutson TE , et al. Lenvatinib plus pembrolizumab versus sunitinib in first-line treatment of advanced renal cell carcinoma: Final prespecified overall survival analysis of CLEAR, a phase III study. J Clin Oncol. 2024; 42( 11): 1222– 8. doi:10.1200/JCO.23.01569. [Google Scholar] [CrossRef]
98. Motzer RJ , Penkov K , Haanen J , Rini B , Albiges L , Campbell MT , et al. Avelumab plus axitinib versus sunitinib for advanced renal-cell carcinoma. N Engl J Med. 2019; 380( 12): 1103– 15. doi:10.1056/NEJMoa1816047. [Google Scholar] [CrossRef]
99. Choueiri TK , Motzer RJ , Rini BI , Haanen J , Campbell MT , Venugopal B , et al. Updated efficacy results from the JAVELIN Renal 101 trial: First-line avelumab plus axitinib versus sunitinib in patients with advanced renal cell carcinoma. Ann Oncol. 2020; 31( 8): 1030– 9. doi:10.1016/j.annonc.2020.04.010. [Google Scholar] [CrossRef]
100. Tomita Y , Motzer RJ , Choueiri TK , Rini BI , Miyake H , Uemura H , et al. Efficacy and safety of avelumab plus axitinib in elderly patients with advanced renal cell carcinoma: Extended follow-up results from JAVELIN Renal 101. ESMO Open. 2022; 7( 2): 100450. doi:10.1016/j.esmoop.2022.100450. [Google Scholar] [CrossRef]
101. Haanen JBAG , Larkin J , Choueiri TK , Albiges L , Rini BI , Atkins MB , et al. Extended follow-up from JAVELIN Renal 101: Subgroup analysis of avelumab plus axitinib versus sunitinib by the International Metastatic Renal Cell Carcinoma Database Consortium risk group in patients with advanced renal cell carcinoma. ESMO Open. 2023; 8( 3): 101210. doi:10.1016/j.esmoop.2023.101210. [Google Scholar] [CrossRef]
102. Choueiri TK , Penkov K , Uemura H , Campbell MT , Pal S , Kollmannsberger C , et al. Avelumab + axitinib versus sunitinib as first-line treatment for patients with advanced renal cell carcinoma: Final analysis of the phase III JAVELIN Renal 101 trial. Ann Oncol. 2025; 36( 4): 387– 92. doi:10.1016/j.annonc.2024.12.008. [Google Scholar] [CrossRef]
103. Lee D , Gittleman H , Weinstock C , Suzman D , Bloomquist E , Agrawal S , et al. A U.S. food and drug administration–pooled analysis of frontline combination treatment survival benefits by risk groups in metastatic renal cell carcinoma. Eur Urol. 2023; 84( 4): 373– 8. doi:10.1016/j.eururo.2023.05.030. [Google Scholar] [CrossRef]
104. Ciccarese C , Iacovelli R , Porta C , Procopio G , Bria E , Astore S , et al. Efficacy of VEGFR-TKIs plus immune checkpoint inhibitors in metastatic renal cell carcinoma patients with favorable IMDC prognosis. Cancer Treat Rev. 2021; 100: 102295. doi:10.1016/j.ctrv.2021.102295. [Google Scholar] [CrossRef]
105. Roviello G , Molina-Cerrillo J , Massari F , Cerbone L , Fiala O , Fornarini G , et al. First-line immune-based combinations or sunitinib in favorable-risk metastatic renal cell carcinoma: A real-world retrospective comparison from the ARON-1 study. Cancer Immunol Immunother. 2025; 74( 2): 65. doi:10.1007/s00262-024-03897-x. [Google Scholar] [CrossRef]
106. Kushnir I , Basappa NS , Ghosh S , Lalani AA , Hansen AR , Wood L , et al. Active surveillance in metastatic renal cell carcinoma: Results from the Canadian kidney cancer information system. Clin Genitourin Cancer. 2021; 19( 6): 521– 30. doi:10.1016/j.clgc.2021.05.004. [Google Scholar] [CrossRef]
107. Harrison MR , Costello BA , Bhavsar NA , Vaishampayan U , Pal SK , Zakharia Y , et al. Active surveillance of metastatic renal cell carcinoma: Results from a prospective observational study (MaRCC). Cancer. 2021; 127( 13): 2204– 12. doi:10.1002/cncr.33494. [Google Scholar] [CrossRef]
108. Rini BI , Dorff TB , Elson P , Rodriguez CS , Shepard D , Wood L , et al. Active surveillance in metastatic renal-cell carcinoma: A prospective, phase 2 trial. Lancet Oncol. 2016; 17( 9): 1317– 24. doi:10.1016/S1470-2045(16)30196-6. [Google Scholar] [CrossRef]
109. Reig Torras O , Mishra A , Christie A , McKenzie T , Onabolu O , Singla N , et al. Molecular genetic determinants of shorter time on active surveillance in a prospective phase 2 clinical trial in metastatic renal cell carcinoma. Eur Urol. 2022; 81( 6): 555– 8. doi:10.1016/j.eururo.2021.12.003. [Google Scholar] [CrossRef]
110. Murphy H , Jaafari H , Dobrovolny HM . Differences in predictions of ODE models of tumor growth: A cautionary example. BMC Cancer. 2016; 16: 163. doi:10.1186/s12885-016-2164-x. [Google Scholar] [CrossRef]
111. Hartung N , Mollard S , Barbolosi D , Benabdallah A , Chapuisat G , Henry G , et al. Mathematical modeling of tumor growth and metastatic spreading: Validation in tumor-bearing mice. Cancer Res. 2014; 74( 22): 6397– 407. doi:10.1158/0008-5472.CAN-14-0721. [Google Scholar] [CrossRef]
112. Fogli S , Porta C , Del Re M , Crucitta S , Gianfilippo G , Danesi R , et al. Optimizing treatment of renal cell carcinoma with VEGFR-TKIs: A comparison of clinical pharmacology and drug-drug interactions of anti-angiogenic drugs. Cancer Treat Rev. 2020; 84: 101966. doi:10.1016/j.ctrv.2020.101966. [Google Scholar] [CrossRef]
113. Rosellini M , Tassinari E , Marchetti A , Tateo V , Nuvola G , Rizzo A , et al. An update on safety evaluation of immune-based combinations in patients with advanced renal cell carcinoma. Expert Opin Drug Saf. 2023; 22( 4): 279– 91. doi:10.1080/14740338.2023.2203486. [Google Scholar] [CrossRef]
114. Chen X , Xu Z , Wu C , Xie L , Wang P , Liu X . Efficacy and toxicity of immune checkpoint inhibitors combination therapy for advanced renal cell carcinoma: A systematic review and network meta-analysis. Front Immunol. 2024; 15: 1255577. doi:10.3389/fimmu.2024.1255577. [Google Scholar] [CrossRef]
115. Rini BI , Brugarolas J , Atkins MB . Navigating and adapting care integrating immunotherapy, antiangiogenic therapy, and combinations in patients with advanced renal cell carcinoma. J Immunother Cancer. 2023; 11( 3): e006361. doi:10.1136/jitc-2022-006361. [Google Scholar] [CrossRef]
116. Martins F , Sofiya L , Sykiotis GP , Lamine F , Maillard M , Fraga M , et al. Adverse effects of immune-checkpoint inhibitors: Epidemiology, management and surveillance. Nat Rev Clin Oncol. 2019; 16( 9): 563– 80. doi:10.1038/s41571-019-0218-0. [Google Scholar] [CrossRef]
117. McGregor B , Mortazavi A , Cordes L , Salabao C , Vandlik S , Apolo AB . Management of adverse events associated with cabozantinib plus nivolumab in renal cell carcinoma: A review. Cancer Treat Rev. 2022; 103: 102333. doi:10.1016/j.ctrv.2021.102333. [Google Scholar] [CrossRef]
118. Leucht K , Ali N , Foller S , Grimm MO . Management of immune-related adverse events from immune-checkpoint inhibitors in advanced or metastatic renal cell carcinoma. Cancers. 2022; 14( 18): 4369. doi:10.3390/cancers14184369. [Google Scholar] [CrossRef]
119. Schneider BJ , Naidoo J , Santomasso BD , Lacchetti C , Adkins S , Anadkat M , et al. Management of immune-related adverse events in patients treated with immune checkpoint inhibitor therapy: ASCO guideline update. J Clin Oncol. 2021; 39( 36): 4073– 126. doi:10.1200/JCO.21.01440. [Google Scholar] [CrossRef]
120. Haanen J , Obeid M , Spain L , Carbonnel F , Wang Y , Robert C , et al. Management of toxicities from immunotherapy: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann Oncol. 2022; 33( 12): 1217– 38. doi:10.1016/j.annonc.2022.10.001. [Google Scholar] [CrossRef]
121. Schmidinger M . Understanding and managing toxicities of vascular endothelial growth factor (VEGF) inhibitors. EJC Suppl. 2013; 11( 2): 172– 91. doi:10.1016/j.ejcsup.2013.07.016. [Google Scholar] [CrossRef]
122. Wood LS , Lim ZD . Safety and adverse event management of VEGFR-TKIs in patients with metastatic renal cell carcinoma. Clin J Oncol Nurs. 2025; 29( 3): 219– 29. doi:10.1188/25.CJON.219-229. [Google Scholar] [CrossRef]
123. Nolla K , Benjamin DJ , Cella D . Patient-reported outcomes in metastatic renal cell carcinoma trials using combinations versus sunitinib as first-line treatment. Nat Rev Urol. 2023; 20( 7): 420– 33. doi:10.1038/s41585-023-00747-w. [Google Scholar] [CrossRef]
124. Kyriakopoulos CE , Chittoria N , Choueiri TK , Kroeger N , Lee JL , Srinivas S , et al. Outcome of patients with metastatic sarcomatoid renal cell carcinoma: Results from the International Metastatic Renal Cell Carcinoma Database Consortium. Clin Genitourin Cancer. 2015; 13( 2): e79– e85. doi:10.1016/j.clgc.2014.08.011. [Google Scholar] [CrossRef]
125. Rini BI , Signoretti S , Choueiri TK , McDermott DF , Motzer RJ , George S , et al. Long-term outcomes with nivolumab plus ipilimumab versus sunitinib in first-line treatment of patients with advanced sarcomatoid renal cell carcinoma. J Immunother Cancer. 2022; 10( 12): e005445. doi:10.1136/jitc-2022-005445. [Google Scholar] [CrossRef]
126. Fontes-Sousa M , Calvo E . First-line immune checkpoint inhibitors in advanced or metastatic renal cell carcinoma with sarcomatoid features. Cancer Treat Rev. 2022; 105: 102374. doi:10.1016/j.ctrv.2022.102374. [Google Scholar] [CrossRef]
127. Iacovelli R , Ciccarese C , Procopio G , Astore S , Cannella MA , Maratta MG , et al. Current evidence for second-line treatment in metastatic renal cell carcinoma after progression to immune-based combinations. Cancer Treat Rev. 2022; 105: 102379. doi:10.1016/j.ctrv.2022.102379. [Google Scholar] [CrossRef]
128. Ding D , Hu H , Shi Y , She L , Yao L , Zhu Y , et al. Cost-effectiveness of pembrolizumab plus axitinib versus sunitinib as first-line therapy in advanced renal cell carcinoma in the U.S. Oncologist. 2021; 26( 2): e290– 7. doi:10.1002/ONCO.13522. [Google Scholar] [CrossRef]
129. Wang Y , Wang H , Yi M , Han Z , Li L . Cost-effectiveness of lenvatinib plus pembrolizumab or everolimus as first-line treatment of advanced renal cell carcinoma. Front Oncol. 2022; 12: 853901. doi:10.3389/fonc.2022.853901. [Google Scholar] [CrossRef]
130. Liu T , Jin Y , Dong M . Cost-effectiveness of nivolumab plus cabozantinib versus cabozantinib as first-line treatment of metastatic renal cell carcinoma. Clin Genitourin Cancer. 2023; 21( 6): e449– 60. doi:10.1016/j.clgc.2023.05.009. [Google Scholar] [CrossRef]
131. Motzer RJ , Escudier B , McDermott DF , George S , Hammers HJ , Srinivas S , et al. Nivolumab versus everolimus in advanced renal-cell carcinoma. N Engl J Med. 2015; 373( 19): 1803– 13. doi:10.1056/NEJMoa1510665. [Google Scholar] [CrossRef]
132. Motzer RJ , Escudier B , George S , Hammers HJ , Srinivas S , Tykodi SS , et al. Nivolumab versus everolimus in patients with advanced renal cell carcinoma: Updated results with long-term follow-up of the randomized, open-label, phase 3 CheckMate 025 trial. Cancer. 2020; 126( 18): 4156– 67. doi:10.1002/cncr.33033. [Google Scholar] [CrossRef]
133. Lee CH , Kang M , Kwak C , Ko YH , Kim JK , Park JY , et al. Sites of metastasis and survival in metastatic renal cell carcinoma: Results from the Korean renal cancer study group database. J Korean Med Sci. 2024; 39( 45): e293. doi:10.3346/jkms.2024.39.e293. [Google Scholar] [CrossRef]
134. Dudani S , de Velasco G , Wells C , Gan CL , Donskov F , Porta C , et al. Sites of metastasis and survival in metastatic renal cell carcinoma (mRCC): Results from the International mRCC Database Consortium (IMDC). J Clin Oncol. 2020; 38 (6_suppl):642. doi:10.1200/JCO.2020.38.6_suppl.642. [Google Scholar] [CrossRef]
135. Singla N , Xie Z , Zhang Z , Gao M , Yousuf Q , Onabolu O , et al. Pancreatic tropism of metastatic renal cell carcinoma. JCI Insight. 2020; 5( 7): e134564. doi:10.1172/jci.insight.134564. [Google Scholar] [CrossRef]
136. Hamada S , Ito K , Kuroda K , Sato A , Asakuma J , Horiguchi A , et al. Clinical characteristics and prognosis of patients with renal cell carcinoma and liver metastasis. Mol Clin Oncol. 2015; 3( 1): 63– 8. doi:10.3892/mco.2014.432. [Google Scholar] [CrossRef]
137. Abreu D , Carvalhal G , Gueglio G , Tobia I , Garcia P , Zuñiga A , et al. Prognostic factors in de novo metastatic renal cell carcinoma: A report from the Latin American renal cancer group. JCO Glob Oncol. 2021; 7: GO.20.00621. doi:10.1200/GO.20.00621. [Google Scholar] [CrossRef]
138. Grünwald V , Eberhardt B , Bex A , Flörcken A , Gauler T , Derlin T , et al. An interdisciplinary consensus on the management of bone metastases from renal cell carcinoma. Nat Rev Urol. 2018; 15( 8): 511– 21. doi:10.1038/s41585-018-0034-9. [Google Scholar] [CrossRef]
139. Das A , Shapiro DD , Craig JK , Abel EJ . Understanding and integrating cytoreductive nephrectomy with immune checkpoint inhibitors in the management of metastatic RCC. Nat Rev Urol. 2023; 20( 11): 654– 68. doi:10.1038/s41585-023-00776-5. [Google Scholar] [CrossRef]
140. Méjean A , Ravaud A , Thezenas S , Colas S , Beauval JB , Bensalah K , et al. Sunitinib alone or after nephrectomy in metastatic renal-cell carcinoma. N Engl J Med. 2018; 379( 5): 417– 27. doi:10.1056/NEJMoa1803675. [Google Scholar] [CrossRef]
141. Méjean A , Ravaud A , Thezenas S , Chevreau C , Bensalah K , Geoffrois L , et al. Sunitinib alone or after nephrectomy for patients with metastatic renal cell carcinoma: Is there still a role for cytoreductive nephrectomy? Eur Urol. 2021; 80( 4): 417– 24. doi:10.1016/j.eururo.2021.06.009. [Google Scholar] [CrossRef]
142. Bex A , Mulders P , Jewett M , Wagstaff J , van Thienen JV , Blank CU , et al. Comparison of immediate vs. deferred cytoreductive nephrectomy in patients with synchronous metastatic renal cell carcinoma receiving sunitinib: The SURTIME randomized clinical trial: The SURTIME randomized clinical trial. JAMA Oncol. 2019; 5( 2): 164– 70. doi:10.1001/jamaoncol.2018.5543. [Google Scholar] [CrossRef]
143. Bakouny Z , El Zarif T , Dudani S , Connor Wells J , Gan CL , Donskov F , et al. Upfront cytoreductive nephrectomy for metastatic renal cell carcinoma treated with immune checkpoint inhibitors or targeted therapy: An observational study from the International Metastatic renal cell carcinoma Database Consortium. Eur Urol. 2023; 83( 2): 145– 51. doi:10.1016/j.eururo.2022.10.004. [Google Scholar] [CrossRef]
144. Makrakis D , Msaouel P , Karam JA , Esagian SM . Cytoreductive nephrectomy in metastatic renal cell carcinoma treated with immune checkpoint inhibitors: A systematic review and meta-analysis of individual patient data. Eur Urol Focus. 2025; 11( 2): 356– 64. doi:10.1016/j.euf.2024.11.007. [Google Scholar] [CrossRef]
145. Li KP , Chen SY , Wang CY , Li XR , Yang L . The impact of cytoreductive nephrectomy on survival outcomes in patients with metastatic renal cell carcinoma receiving immunotherapy: An evidence-based analysis of comparative outcomes. Front Immunol. 2023; 14: 1132466. doi:10.3389/fimmu.2023.1132466. [Google Scholar] [CrossRef]
146. Buchler T , Poprach A . Planned discontinuation of tyrosine kinase inhibitor therapy in metastatic renal cell carcinoma: Lessons for the era of immunotherapy. Target Oncol. 2024; 19( 2): 175– 80. doi:10.1007/s11523-023-01031-y. [Google Scholar] [CrossRef]
147. Choueiri TK , Powles T , Peltola K , de Velasco G , Burotto M , Suarez C , et al. Belzutifan versus everolimus for advanced renal-cell carcinoma. N Engl J Med. 2024; 391( 8): 710– 21. doi:10.1056/NEJMoa2313906. [Google Scholar] [CrossRef]
148. Powles T , Albiges L , Jalkanen KJ , De Velasco G , Burotto M , Ghatalia P , et al. Belzutifan versus everolimus in participants (pts) with previously treated advanced renal cell carcinoma (RCC): Patient-reported outcomes (PROs) in the phase 3 LITESPARK-005 study. J Clin Oncol. 2024; 42 (4_suppl):361. doi:10.1200/JCO.2024.42.4_suppl.361. [Google Scholar] [CrossRef]
149. Vano YA , Phan L , Simonaggio A , Bennamoun M , Pannier D , Chevreau C , et al. Overall survival (OS) and efficacy results of second-line treatment in patients (pts) with metastatic clear cell renal cell carcinoma (mRCC) treated in the randomized phase II BIONIKK trial. J Clin Oncol. 2023; 41 (6_suppl):607. doi:10.1200/JCO.2023.41.6_suppl.607. [Google Scholar] [CrossRef]
150. Chen YW , Beckermann K , Haake SM , Reddy A , Shyr Y , Atkins MB , et al. Optimal treatment by invoking biologic clusters in renal cell carcinoma (OPTIC RCC). J Clin Oncol. 2023; 41 (6_suppl):TPS742. doi:10.1200/JCO.2023.41.6_suppl.TPS742. [Google Scholar] [CrossRef]
151. Ali Srour S , Chahoud J , Drakaki A , Curti BD , Gibney GT , Pal SK , et al. ALLO-316 in advanced clear cell renal cell carcinoma (ccRCC): Updated results from the phase 1 TRAVERSE study. J Clin Oncol. 2025; 43 (16_suppl):4508. doi:10.1200/JCO.2025.43.16_suppl.4508. [Google Scholar] [CrossRef]
152. Rini BI , Stenzl A , Zdrojowy R , Kogan M , Shkolnik M , Oudard S , et al. IMA901, a multipeptide cancer vaccine, plus sunitinib versus sunitinib alone, as first-line therapy for advanced or metastatic renal cell carcinoma (IMPRINT): A multicentre, open-label, randomised, controlled, phase 3 trial. Lancet Oncol. 2016; 17( 11): 1599– 611. doi:10.1016/S1470-2045(16)30408-9. [Google Scholar] [CrossRef]
153. Braun DA , Moranzoni G , Chea V , McGregor BA , Blass E , Tu CR , et al. A neoantigen vaccine generates antitumour immunity in renal cell carcinoma. Nature. 2025; 639 (8054): 474–82. doi:10.1038/s41586-024-08507-5. [Google Scholar] [CrossRef]
154. Calvo E , Boni V , Dumas O , Shin SJ , Rosen SD , Chaudhry A , et al. Nemvaleukin Alfa monotherapy in patients with advanced melanoma and renal cell carcinoma: Results from the phase 1/2 non-randomized ARTISTRY-1 trial. J Immunother Cancer. 2025; 13( 8): e010777. doi:10.1136/jitc-2024-010777. [Google Scholar] [CrossRef]
155. Sheng X , Luo H , Kong C , Liu F , Wei S , Wang Z , et al. 1692P A phase Ib/IIa trial to evaluate the safety and efficacy of PM8002/BNT327, a bispecific antibody targeting PD-L1 and VEGF-A, as a monotherapy in patients with advanced renal cell carcinoma. Ann Oncol. 2024; 35: S1014. doi:10.1016/j.annonc.2024.08.1785. [Google Scholar] [CrossRef]
Cite This Article
 Copyright © 2026 The Author(s). Published by Tech Science Press.
Copyright © 2026 The Author(s). Published by Tech Science Press.This work is licensed under a Creative Commons Attribution 4.0 International License , which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
 Downloads
Downloads
 Citation Tools
Citation Tools