
 Submit a Paper
Submit a Paper Propose a Special lssue
Propose a Special lssue Open Access
Open Access
ARTICLE

Can Physical Activities Suppress Negative Impact of Stress on the Mental Health of Adolescents?
Faculty of Education, Josip Juraj Strossmayer University of Osijek, Osijek, 31000, Croatia
* Corresponding Author: Tena Velki. Email:
International Journal of Mental Health Promotion 2024, 26(3), 211-219. https://doi.org/10.32604/ijmhp.2024.047950
Received 23 November 2023; Accepted 22 February 2024; Issue published 08 April 2024
 View Full Text
View Full Text Download PDF
Download PDFAbstract
Early adolescence is a crucial developmental phase marked by significant physical, cognitive, and socioemotional changes. While stress is widely recognized as a notable risk factor during this period, not all individuals experiencing stress concurrently manifest compromised mental health. The association between stress and mental health outcomes is influenced by individual differences in characteristics and coping strategies. This study’s purpose was to assess the negative impact of stress on mental health, specifically focusing on symptoms of anxiety, depression, and psychological distress. Additionally, the research investigates whether different levels of physical activity can suppress the negative effects of stress. A total of 212 upper elementary school students (52.8% girls and 47.2% boys) from rural and urban areas voluntarily participated in the research. Participants online self-assessed on several measures: The Young Person’s CORE, Children’s Anxiety Scale, Children’s Depression Inventory, School Stress Intensity Scale for Students, and Physical Activity Questionnaire for Older Children. The results revealed a significant increase in adolescents experiencing impaired mental health. More than two-thirds (67.5%) of students self-assessed significant symptoms of depression, additionally, 57.5% of them had significant symptoms of psychological distress, and 27.8% had significant symptoms of anxiety. Stress demonstrated a significant direct negative effect, leading to increased symptoms of anxiety (t = 5.35, p = 0.00) and psychological distress (t = 4.29, p = 0.00); however, there was no significant influence on depression (t = 1.33, p = 0.18)). Regarding regular physical activity, a significant moderating effect was identified, effectively suppressing the negative impact of stress on anxiety (F = 3.88(2,206); p = 0.02). In contrast, no significant moderation effect of physical activity was found for symptoms of depression (F = 1.45(2,206); p = 0.24) and psychological distress (F = 1.14(2,206); p = 0.32), highlighting a complex and intricate association between physical activity and various mental health outcomes. In conclusion, the practical implications of this study emphasize the importance of creating environments that reduce stressors for adolescents and promote regular physical activity as a means of fostering positive mental health outcomes.Keywords
Mental Health in Early Adolescence
Early adolescence (age 10 to 15) is a critical developmental period characterized by profound physical, cognitive, and socio-emotional changes [1]. As young individuals navigate the transition from childhood to adolescence, their mental health becomes a pivotal aspect influencing overall well-being and future trajectories. Mental health in early adolescence is a multidimensional construct encompassing emotional, psychological, and social dimensions, playing a fundamental role in shaping the foundation for lifelong mental well-being.
During this developmental stage, individuals face a number of challenges, including increased academic demands, social pressures, identity exploration, and emerging autonomy [2]. These challenges, combined with biological changes and the quest for independence, create a unique context that can significantly impact mental health outcomes. Moreover, early adolescence serves as a sensitive period for the emergence of various mental health disorders, including anxiety and depression [3]. A meta-analysis conducted across 11 high-income countries, utilizing a pooled sample of 61,545 children aged 4–18 years, has revealed a prevalence rate of 12.7% for any childhood mental disorder. Specifically, the prevalence rates for anxiety and depressive disorders were found to be 5.2% and 1.3%, respectively [4]. Recent mental health statistic data [5] showed that 18.0% of children aged 7–16 had a probable mental disorder in 2022 in the UK, with most common symptoms of anxiety (5.9%) or depression (3.3%). Using a national sample from the United States and data spanning from 2013 to 2019, it is observed that mental disorders manifest in early childhood, impacting children across various sociodemographic profiles. Throughout this timeframe, anxiety emerged as one of the most prevalent diagnoses among U.S. children and adolescents aged 3–17 years, affecting approximately one in 11 (9.8%) individuals. Furthermore, among children and adolescents aged 12–17 years, a significant proportion (20.9%) reported having experienced a major depressive episode at some point [6].
Most of the research examining the correlation between stress and mental health has predominantly centered on the conceptualization of mental health, operationalized as the absence of symptomatic manifestations indicative of psychological disorders or mental health issues [7]. Findings across studies have consistently affirmed that stress exhibits a significant association with emotional disorders, i.e., anxiety and depression [8]. Extant literature has demonstrated a positive correlation between daily stressors and mental health problems [9–11]. The daily experiences of elementary school students are marked by various stressors, originating from their academic environment, family dynamics, peer interactions, extracurricular activities, and exposure to technology. School-related stress, influenced by academic pressures and social expectations, can significantly impact emotional well-being [12]. Family conflicts [13,14], peer pressure [1,15], and the demand for excellence in extracurricular activities [12] contribute further to the stress burden. Additionally, the pervasive influence of technology, particularly social media, introduces a new dimension of stress, as children navigate online interactions and exposure to potentially harmful content [16].
While stress is acknowledged as a significant risk factor, not all individuals encountering stress concurrently manifest compromised mental health. The strength of the association between stress and mental health is contingent upon the individual differences in characteristics and coping strategies that distinguish one person from another [17,18]. One such characteristic that has emerged definitively as influential in stress reduction is regular engagement in physical activity.
The role of physical activity in mental health issues
Physical activity plays a pivotal role in promoting mental health and is recognized as a valuable component in managing various mental health issues, particularly depression and anxiety [19–21]. Numerous studies have consistently demonstrated the positive impact of regular physical activity on mental well-being during adolescence [22–25]. Engaging in exercise triggers the release of neurotransmitters such as endorphins, which act as natural mood lifters and stress relievers, contributing to an improved emotional state [26,27].
In the context of depression, physical activity has been shown to have antidepressant effects by influencing neurochemical processes in the brain. Exercise stimulates the production of serotonin, a neurotransmitter associated with mood regulation, and promotes the growth of new neurons in the hippocampus, a region linked to emotional processing and memory [28,29]. Moreover, the sense of accomplishment and improved self-esteem that often accompanies physical activity can counteract the negative thought patterns characteristic of depression.
Similarly, physical activity serves as a potent antidote to anxiety. Regular exercise helps regulate the body’s stress response system, reducing levels of stress hormones such as cortisol [30]. The rhythmic and repetitive nature of certain exercises, such as walking, running, or swimming, can induce a state of relaxation, alleviating symptoms of anxiety [31]. Additionally, engaging in physical activity provides an opportunity for individuals to break the cycle of anxious thoughts and redirect their focus, fostering a sense of control and mastery over their mental well-being [32,33].
The persistent evidence establishing the deleterious effects of stress on mental health underscores the significance of this relationship. Moreover, the expanding body of research substantiating the connection between physical activity and mental well-being emphasizes the pivotal role of incorporating exercise as a fundamental element in a comprehensive strategy aimed at fostering mental health, managing conditions like depression and anxiety, and ultimately alleviating stress. However, there exists a gap in current research concerning the potential moderating influence of physical activities in mitigating the negative impact of stress on mental health. This research gap underscores the need for focused investigations to unveil the complex interplay between physical activity, stress, and mental health outcomes, thereby contributing to a more comprehensive understanding of the intricate dynamics at play in this multifaceted relationship. This study presents a more profound investigation into the link between stress and mental health. Additionally, considering the absence of a direct impact of stress on mental health, the study could further innovate by conducting a detailed exploration of the intricate dynamics between stress and various mental health outcomes, potentially uncovering mediating or moderating factors. Furthermore, expanding the analysis of the relationship between physical activity and mental health, with a focus on specific aspects that may positively affect diverse mental outcomes, could enhance the comprehensiveness of the research.
Therefore, the aim of the research is to assess the negative impact of stress on mental health (measured using three aspects: symptoms of anxiety, symptoms of depression, and overall psychological distress) in early adolescence and to investigate whether different intensities of physical activity (inactive, moderate, regular) can contribute to reducing the negative impact of stress (Fig. 1).
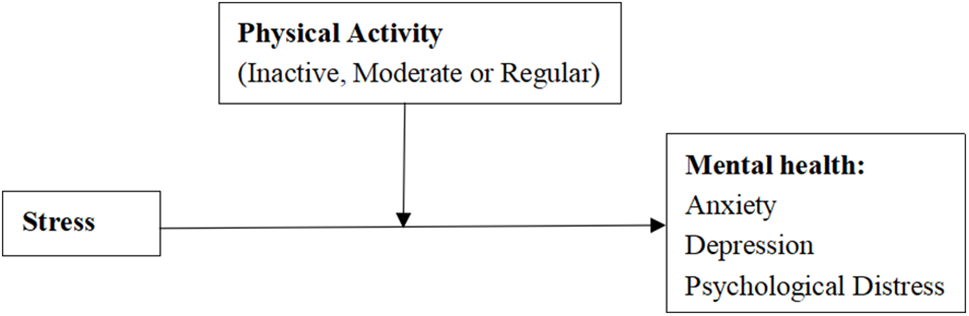
Figure 1: Conceptual model: the moderating role of physical activity on the relationship between stress and mental health.
H1: Stress will have a direct negative impact on the adolescents’ mental health.
H2: Physical activity will suppress the negative impact of stress on adolescents’ mental health.
Two hundred twelve upper elementary school students (from the fifth to the eighth grade) participated in the research. About 20% of students did not have parental consent to participate in the research, therefore they did not fill out the online questionnaires. All participants who had signed parental consent participated in the research. Of these, 112 students were from urban areas, while 100 students were from rural areas. Approximately half of the participants were girls (n = 112, 52.8%), and the other half were boys (n = 100, 47.2%). The questionnaire was completed by 36 5th grade students (16.9%), 54 6th grade students (25.5%), 68 7th grade students (32.1%) and 54 8th grade students (25.5%). The age range of the students varied from 10 to 15 years, with an average age of M = 12.33 (SD = 1.25). The average age of fifth grade students was M = 10.64 (SD = 0.54), the average age of sixth grade students was M = 11.70 (SD = 0.54), the average age of seventh grade students was M = 12.49 (SD = 0.50) while the average age of eighth students grades was M = 13.91 (SD = 0.71).
The Young Person’s CORE (YP–CORE; Twigg et al. [34])
The YP-CORE (original version, Twigg et al. [34]) is an instrument designed to measure psychological distress in children and young people. It consists of 10 items that assess anxiety (2 items), depression (2 items), trauma (1 item), physical difficulties (1 item), functioning (3 items), and the risk of auto aggressive behavior (1 item). Students self-evaluate the frequency of described problems on a 5-point Likert scale (0–not at all, 1–only occasionally, 2-sometimes, 3-often, 4-most or all of the time). Participants respond retrospectively, providing answers for the past week. Each answer is assigned the appropriate score (0–4), and 3 items are scored in reverse. The total score is obtained by adding all the points. A higher score indicates that the student reported more problems and emotional difficulties, feeling more disturbed. The critical value of 12 has proven to be important in distinguishing between clinical and non-clinical groups of children aged 10 to 14 in Croatia (Croatian version, Marinković et al. [35]). Internal reliability in the conducted research was moderate, Cronbach’s α = 0.74.
Children’s Anxiety Scale (SKAN; Purić, 1992 according to Caser [36])
The Children’s Anxiety Scale (Caser [36]) is intended for children aged 9 to 15 years. It comprises 27 statements where students should mark ‘T’ if they believe the statement is true for them or ‘N’ if they believe the statement is not valid for them. Statements, which children noted as being true for them, are scored, while other answers are not. Each true statement is worth 1 point, and the point range is between 0 and 27. The greater the number of true statements and points, the higher the student’s anxiety level. The questionnaire covers three areas of anxiety: test anxiety, social anxiety, and general anxiety unrelated to specific situations. The total score for the general level of anxiety can also be utilized. The average score is 10, with a standard deviation of 5.25, and the critical value (self-perceived diagnosis of anxiety) is a score above 1 standard deviation, i.e., a value of 16 and above (according to Zaić [37]). Internal reliability in the conducted research was high, Cronbach’s α = 0.89.
Children’s Depression Inventory (CDI; Kovacs [38])
The Child Depression Scale-CDI (original version, Kovacs [38]; Croatian version, Marinović et al. [39] was created by modifying the Beck Depression Scale, originally intended for examining depression in adults (BDI). The scale consists of 27 items covering a broad spectrum of cognitive, affective, and behavioral symptoms of depression in children and adolescents aged 7 to 17. Each item presents three statements, from which the child chooses the one that best describes their feelings. Statements are scored with 0, 1, and 2 points, where a higher score indicates a stronger intensity of symptoms. The total score is derived as a unique linear combination of responses to individual items, ranging from 0 to 54. On a sample of unselected school children, the average score is around 9, with a standard deviation of approximately 7. As a threshold to identify the top 10% of respondents with the most pronounced depressive symptoms (self-perceived diagnosis of depression), a score of 19 is used [39]. Internal reliability in the conducted research was satisfactory, Cronbach’s α = 0.66.
School Stress Intensity Scale for Students (Sabljić [40])
The School Stress Intensity Scale for Students (Sabljić [40]) consist of 31 items and assesses the intensity of stress experienced by students in the school environment. The items are content categorized into several domains: those related to school curriculum and the learning environment, teachers, parents, and classmates. Students self-evaluate the level of stress on a 5-point Likert scale (from 0 to 4), and the overall score is expressed as a simple linear combination of responses. The theoretical range of scores is from 0 to 124, with a higher score indicating a greater intensity of school stress. Internal reliability in the conducted research was high, Cronbach’s α = 0.96.
Physical Activity Questionnaire for Older Children (PAQ-C; Kowalski et al. [41])
The PAQ-C (original version, Kowalski et al. [41]; Croatian version, Vidaković Samaržija et al. [42]) measures the general physical activity of a child and consists of 10 items where students respond to questions about their engagement in physical activities over the past seven days. This questionnaire assesses the intensity, duration, and frequency of physical activity in children and adolescents based on self-report. It is designed for students aged 8 to 14 years. Each item has a value from 1 to 5. Item 1 pertains to leisure-time sports activities, where a ‘no’ response is scored as 1, and a ‘7 times or more’ response is scored as 5, with the average of all activities calculated. Items 2 to 8 relate to physical education, after-school breaks, evenings, weekends, and what best describes the individual. Scores for these items are calculated so that minimal engagement is scored as 1, and maximal engagement is scored as 5, with the average of all activities calculated. Item 9 concerns daily engagement in any physical activity over the previous week and is calculated as the average for all days of the week, where ‘nothing’ is scored as 1 and ‘very often’ as 5. The overall result is obtained as the average of the described three parts of questionnaire, with a theoretical response range from 1 to 5. Item number 10 is not used as part of the final result but serves to identify any unusual activities students engaged in the previous week. The questionnaire allows classification into three groups: physically inactive (total score 1 to 2.4), moderately physically active (total score between 2.5 and 3.4), and regularly physically active (total score from 3.5 to 5). Internal reliability in the conducted research was high, Cronbach’s α = 0.87.
The Ethics Committee of the Faculty of Education J.J. Strossmayer University of Osijek approved research. The research was entirely voluntary and anonymous. After obtaining the school director’s consent, parents were requested to provide written approval for their children’s participation in the study. Data collection took place online during a class community session lasting approximately 30 min. In order to finish filling out the questionnaire, the students had to answer all the questions, therefore there were no missing data. Homeroom teachers were briefed in advance about the research’s objectives and methodology. In addition to the written notification, researchers verbally explained the research’s purpose, emphasized its voluntary nature, and informed students that they could withdraw from the process at any time.
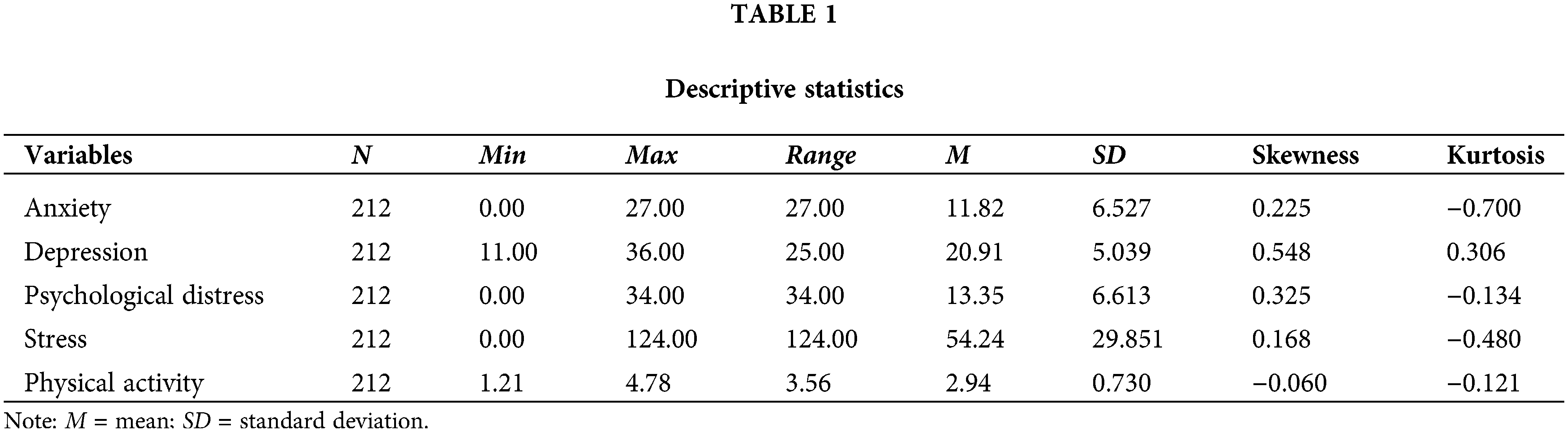
Criteria for the use of parametric statistics (Table 1) and assumptions for regression analysis were met. Asymmetry indices (Skewness and Kurtosis) have not exceeded the critical value of +/−2, so the normality of the distribution is not violated. Average values of measured variables (M, SD) were as expected. Main analyses were performed in IBM SPSS Statistics 24.0, using PROCESS v4.2 by Andrew F. Hayes plug-in, model 1b (moderation analysis with categorical moderator). Hypothesis 1 tested direct effects and hypothesis 2 tested simple moderation effects with categorical moderators. For the purpose of moderation analysis, all predictors were mean-centered, and the moderator variable had three levels (i.e., inactive (coding 0, 0), moderately active (coding 1, 0) and regularly active (coding 0, 1). Fig. 1 represents the conceptual model that was tested.
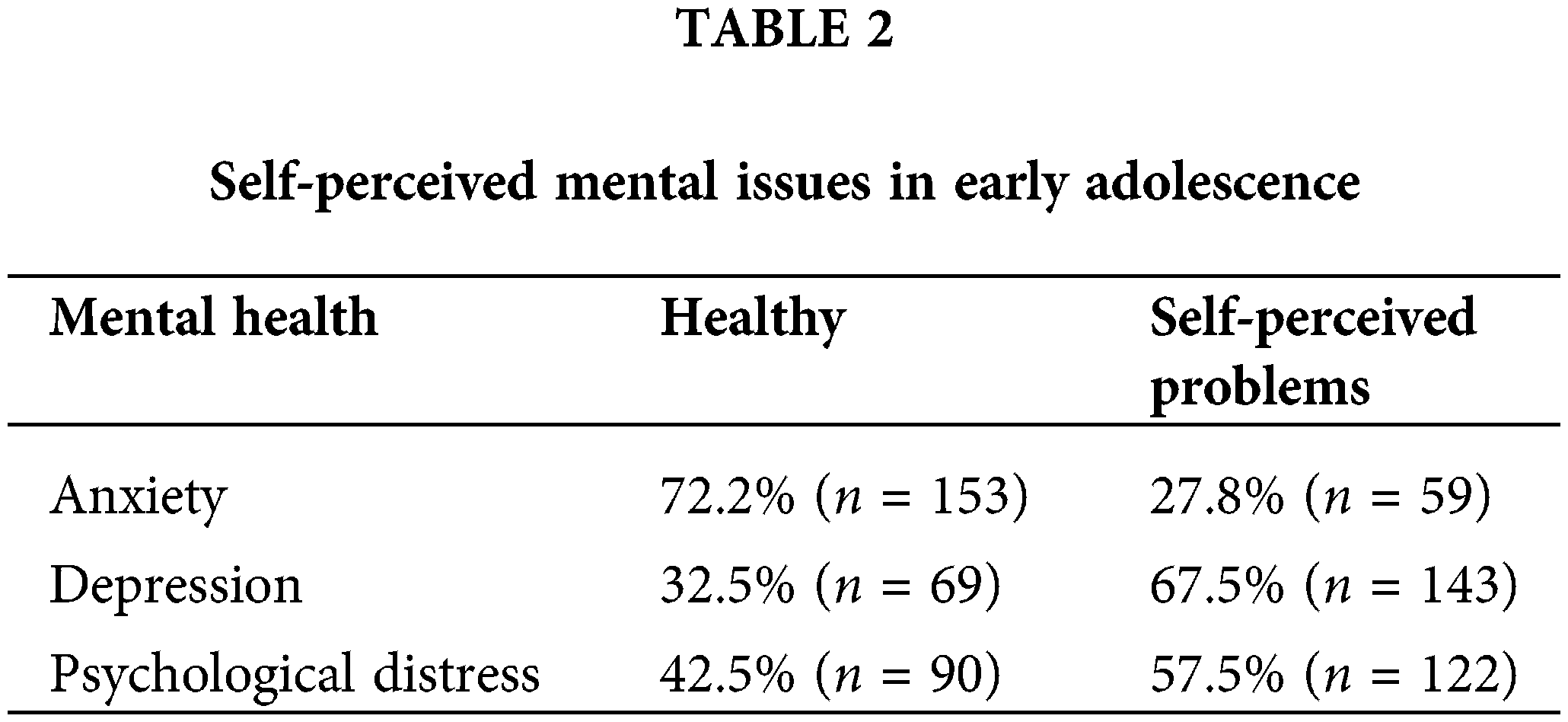
Following the instructions outlined in the Croatian versions of the questionnaire used in this study, we classified students into two groups: those who self-assessed clinically significant symptoms indicating impaired mental health (such as symptoms of depression, anxiety, or general psychological distress) and those who self-assessed without significant symptoms, i.e., those considered mentally healthy (see Table 2). More than two thirds of students self-assessed significant symptoms of depression, more than half of them significant symptoms of psychological distress and more than one quarter of them significant symptoms of anxiety. The findings reveal a notably higher prevalence of adolescents with impaired mental health compared to previous studies [4–6], particularly concerning symptoms of depression.
One plausible consideration is the changing socio-cultural dynamics and the impact of modern lifestyles on adolescent well-being. Factors such as increased academic pressures, social media influence, and the fast-paced nature of contemporary society [12–16] may contribute to heightened stress levels and, consequently, a higher prevalence of mental health issues. However, it is imperative to acknowledge the exclusive reliance on self-reports by students across all mental health measures in this study. No anamnestic data were collected, nor were diagnoses proffered by medical professionals. Given the tumultuous emotional landscape inherent in early adolescence [1–3], there exists the potentiality that students may have overestimated the manifestation of symptoms associated with mental disorders.
Nevertheless, the substantial increase in the prevalence of mental health problems in early adolescence prompts a critical reflection on the effectiveness of current mental health support systems for students. It raises questions about the accessibility and adequacy of mental health resources, as well as the awareness and utilization of available services.
Negative impact of stress on the adolescents’ mental health
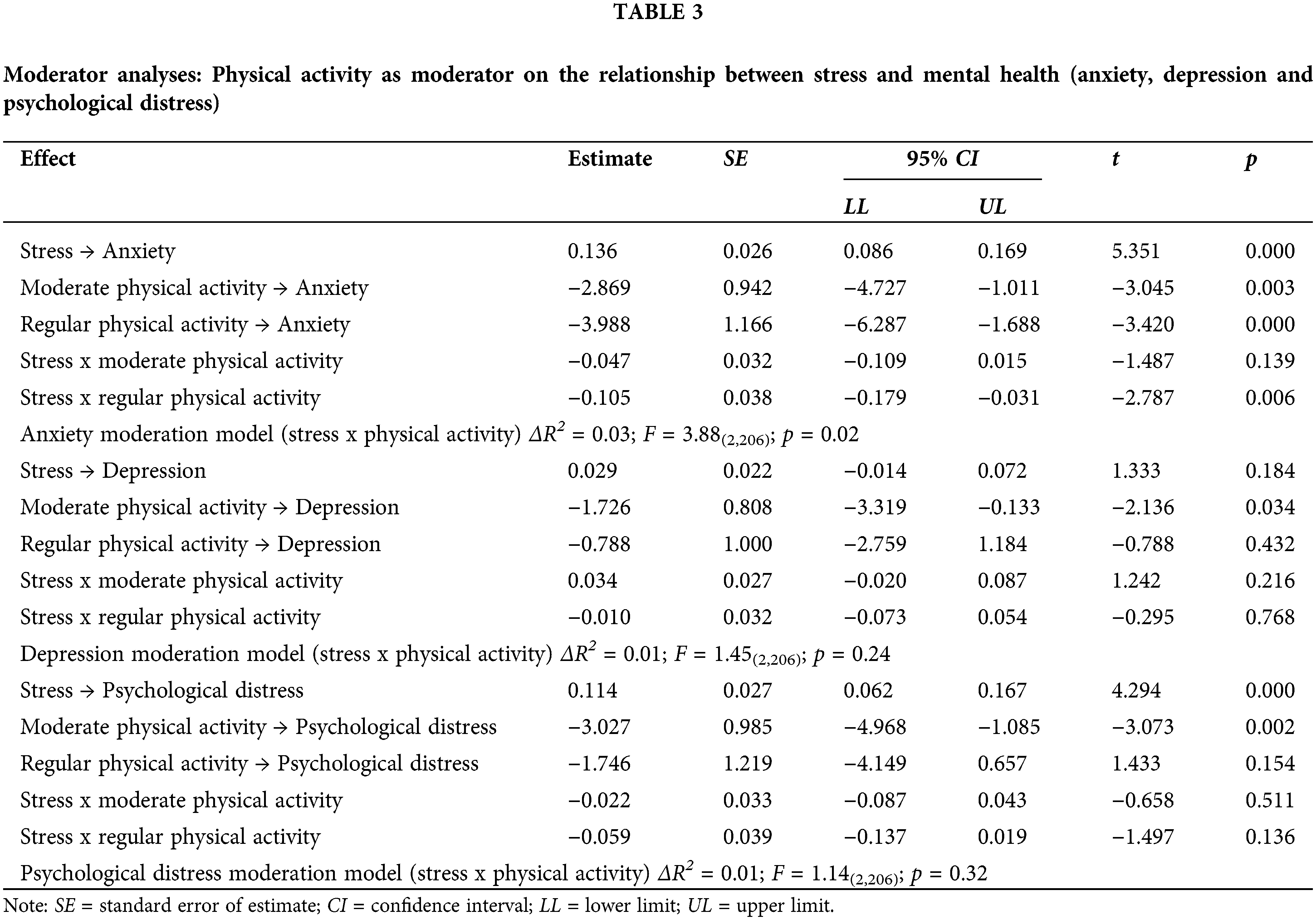
In line with the first hypothesis, the presence of a negative impact of stress on adolescents’ mental health was examined (Table 3). Stress demonstrated a significant direct negative effect, leading to increased symptoms of anxiety and psychological distress; however, it exhibited no influence on depression. There is a corresponding increase in symptoms of anxiety and psychological distress, suggesting that stress itself, without the mediation of other factors, contributes to higher levels of anxiety and psychological distress. In contrast to its impact on anxiety and psychological distress, stress is reported to have no influence on depression.
The observed escalation in symptoms of anxiety and psychological distress emphasizes the susceptibility of adolescents to the adverse effects of stress [7,8]. The absence of a direct influence on depression prompts a deeper exploration into the intricate dynamics between stress and distinct mental health outcomes. It is also possible that stress had no effect on depression because almost all adolescents self-assessed that they had significant symptoms of depression, which reduces the variability in depression and makes it impossible to detect the effects of other variables. These findings are in line with previous research [9–11], accentuating the variability in how stress may manifest across diverse dimensions of mental health.
Generally, this study contributes valuable insights into the direct impact of stress on specific facets of mental health in adolescents. The complex findings underscore the need for comprehensive assessments, considering various dimensions of mental health. This knowledge is essential for refining interventions aimed at promoting mental well-being in the vulnerable phase of early adolescence.
The moderating role of physical activity on the relationship between stress and mental health
In alignment with the second hypothesis, which assumes that regular physical activity moderates the negative impact of stress on adolescents’ mental health, a moderation analysis was conducted. The majority of students self-assessed moderate physical activity (n = 112, 52.8%), and approximately an equal number of them assessed that they were inactive (n = 55, 25.9%) and regularly physically active (n = 45, 21.2%). The results revealed a significant moderating effect of physical activity solely in the context of anxiety moderation models. Conversely, in relation to the negative impact of stress on symptoms of depression (p = 0.24) and psychological distress (p = 0.32), no significant moderation effect of physical activity was observed (Table 3). In the anxiety moderation model (p = 0.02), moderate physical activity exhibited a partial moderation effect, mitigating the negative impact of stress on anxiety symptoms. Furthermore, in the case of regular physical activity, a complete moderation effect was observed, resulting in the full suppression of the negative impact of stress on anxiety (Fig. 2). As shown in Fig. 2, there is no significant negative effect of student stress on anxiety symptoms under the influence of regular physical activity. In students who do not regularly engage in physical activity, the negative effect of stress on the increase in anxiety symptoms is clearly observed.
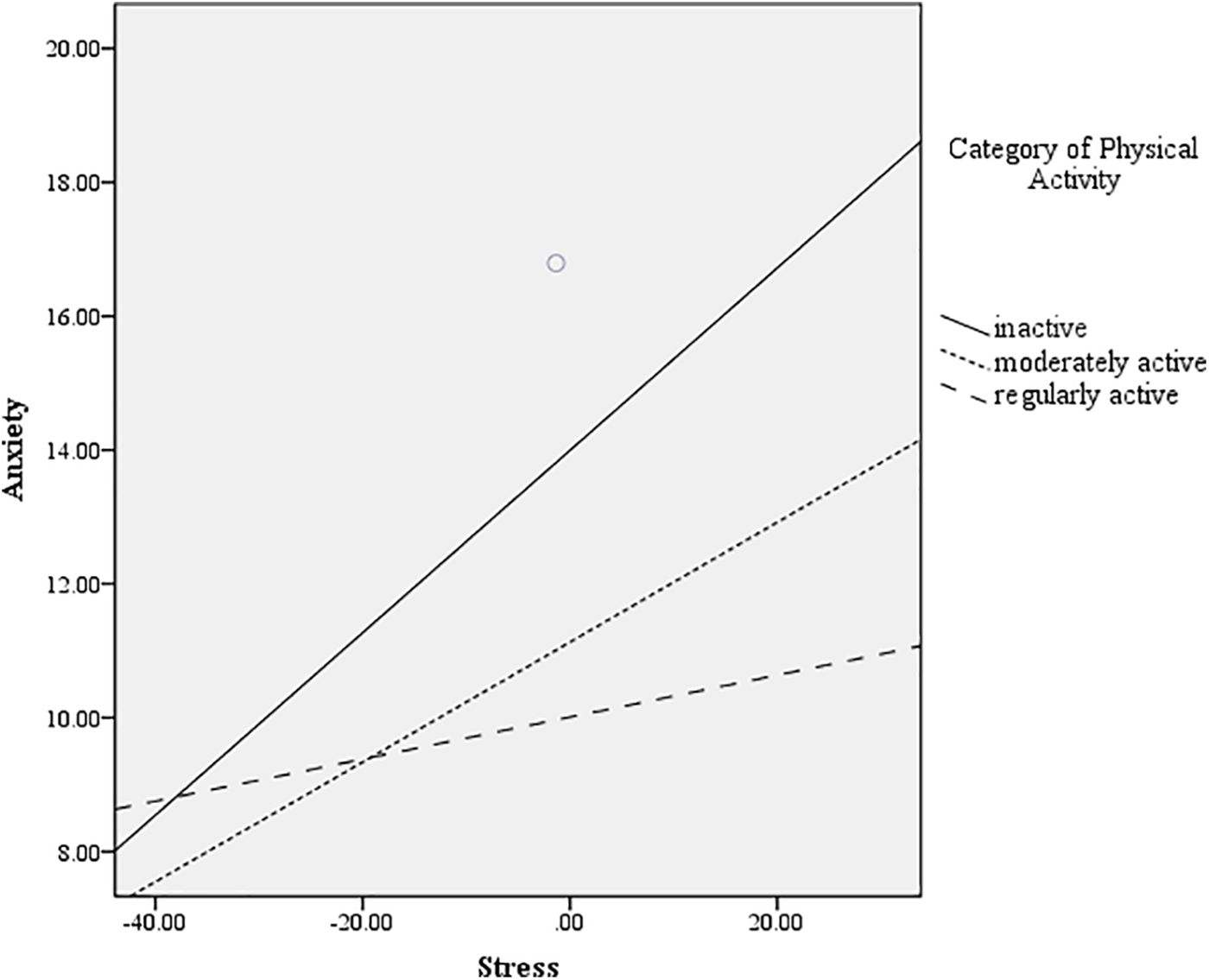
Figure 2: The moderating role of physical activity on the relationship between stress and anxiety.
The finding that regular physical activity demonstrated a significant moderating effect in the context of anxiety aligns with existing literature emphasizing the positive impact of exercise on anxiety symptoms [30–33]. The observed partial moderation effect of moderate physical activity on anxiety symptoms suggests a graded relationship between the intensity of physical activity and its moderating effect on stress-induced anxiety. However, the absence of a substantial moderation effect of physical activity in relation to symptoms of depression and psychological distress prompts further exploration. These results indicate complex relationship between physical activity and different mental health outcomes, emphasizing the need for a comprehensive understanding of the diverse impacts of exercise on adolescents’ well-being. Exploring potential mediators and moderators, such as social support or individual resilience, could enhance our understanding of the complex pathways involved. Moreover, considering the diverse contexts in which adolescents engage in physical activity, including school-based programs, organized sports, and recreational activities, can provide a more nuanced perspective.
Shortcomings and implications for future
In scrutinizing the research, several limitations come to light. Firstly, the sample, comprising upper elementary school students from specific regions, may restrict the generalizability of findings to a broader adolescent population. Moreover, parental consent was not obtained for 20% of students and they could not participate in the research. The study’s reliance on self-report measures, particularly for physical activity, introduces potential biases due to subjective interpretation and recall, compromising the precision of the results. To assess the mental health of students, only self-assessment measures were used, and there was no objective assessment of health conditions by medical doctors. Furthermore, the cross-sectional design, while informative, only provides a snapshot, preventing the establishment of causal relationships and limiting insights into how changes over time may impact the observed associations. The study also falls short in exploring external factors, such as socioeconomic status and family dynamics, which could potentially confound the relationship between physical activity, stress, and mental health.
To address these limitations, future research should consider several key areas. Longitudinal studies are recommended to explore the temporal dynamics between physical activity, stress, and mental health. Diversifying the participant sample to include various demographic groups and incorporating objective measures of physical activity, such as accelerometers, could enhance the study’s applicability and accuracy. Exploring additional psychosocial factors like family environment and socioeconomic status is advised for a more holistic understanding of the relationships. Intervention studies assessing the causal impact of promoting physical activity on stress reduction in adolescents are proposed. Extending the age range of participants and including a broader spectrum of mental health outcome measures beyond anxiety and depression are also suggested to capture more comprehensive insights. Addressing these considerations in future research would strengthen methodology, improve result interpretation, and increase findings’ applicability to diverse populations and contexts.
The findings of this study hold several practical implications for educators, parents, and policymakers involved in adolescent mental health and well-being. Stress’s direct negative impact on mental well-being underscores the need for stress alleviation strategies in academic settings. Schools can adopt stress management programs to create supportive environments. The study emphasizes the preventive role of regular physical activity against the adverse effects of stress on mental health. Prioritizing physical education and extracurricular activities in schools is crucial. Parents are encouraged to actively support their adolescents in engaging in regular physical activities, fostering both mental well-being and family bonds. At the policy level, evidence-based interventions promoting physical activity should be integrated into broader mental health initiatives. Policymakers are urged to allocate resources for the development and implementation of such programs, recognizing their long-term benefits. In essence, collaborative efforts among educators, parents, and policymakers are crucial for comprehensive strategies supporting adolescent mental well-being.
The results brought attention to a significant increase in adolescents experiencing impaired mental health, especially in symptoms of depression, when contrasted with earlier studies. The noted escalation in symptoms of anxiety and psychological distress highlights the vulnerability of adolescents to stress. Simultaneously, the lack of a direct impact on depression prompts further investigation into the intricate dynamics between stress and distinct mental health outcomes. In terms of regular physical activity, a significant moderating effect was evident, effectively mitigating the negative impact of stress on anxiety. Conversely, no significant moderation effect of physical activity was identified for symptoms of depression and psychological distress. This indicates a subtle and complex association between physical activity and diverse mental health outcomes.
In conclusion, the practical implications of this study emphasize the importance of creating environments that reduce stressors for adolescents and promote regular physical activity as a means of fostering positive mental health outcomes. These efforts require collaboration among educators, parents, and policymakers to create comprehensive and effective strategies for supporting the mental well-being of adolescents.
Acknowledgement: All the work in this study was completed by Tena Velki.
Funding Statement: The author received no specific funding for this study.
Author Contributions: The author, Tena Velki, confirms her contribution to the whole paper.
Availability of Data and Materials: Given that the research was conducted with minor students for whom parental consent was obtained, and in accordance with the approval of the ethics committee of the Faculty of Education, in order to protect the privacy of children and some of their medical data, the data is not available online. For the application of the used measurement instruments (questionnaires) in this research, it is necessary to seek the consent of their authors.
Ethics Approval: The Ethics Committee of the Faculty of Education J.J. Strossmayer University of Osijek, in accordance with the Code of Ethics of Psychological Work (NN13/2005), the Code of Ethics for Research with Children in Croatia (Ajduković and Keresteš, 2020) and the UN Convention on the Rights of the Child from 1989, at the Faculty Council Session held in February 2023, recommended conducting research with children on the topic of Mental health and physical activity, under the condition of maximum protection of the privacy of children involved in the research, which was approved on the session. All participants signed the informed consent in this study.
Conflicts of Interest: The author declares that she has no conflicts of interest to report regarding the present study.
References
1. Bishop PA, Harrison LM. The successful middle school: this we believe. Association for Middle Level Education; 2021. Available from: https://www.amle.org/the-successful-middle-school-this-we-believe/. [Accessed 2023]. [Google Scholar]
2. McCarthy K, Brady M, Hallman K. Investing when it counts: reviewing the evidence and charting a course of research and action for very young adolescents. Population Council; 2016. Available from: https://www.popcouncil.org/uploads/pdfs/2016PGY_InvestingWhenItCounts.pdf. [Accessed 2023]. [Google Scholar]
3. Gore FM, Bloem PJ, Patton GC, Ferguson J, Joseph V, Coffey C, et al. Global burden of disease in young people aged 10–24 years: a systematic analysis. Lancet. 2011;377(9783):2093–102. doi:10.1016/S0140-6736(11)60512-6. [Google Scholar] [PubMed] [CrossRef]
4. Barican JL, Yung D, Schwartz C, Zheng Y, Georgiades K, Waddel C. Prevalence of childhood mental disorders in high-income countries: a systematic review and meta-analysis to inform policymaking. Evid-Based Ment Health. 2022;25(1):36–44. doi:10.1136/ebmental-2021-300277. [Google Scholar] [PubMed] [CrossRef]
5. Baker C, Kirk-Wade E. Mental health statistics: prevalence, services and funding in England; 2023. Available from: https://researchbriefings.files.parliament.uk/documents/SN06988/SN06988.pdf. [Accessed 2023]. [Google Scholar]
6. Bitsko RH, Claussen AH, Lichstein J, Black LI, Everett Jones S, Danielson ML, et al. Mental health surveillance among children—United States, 2013–2019. Morb Mortal Weekly Rep. 2022;71(2):1–42. doi:10.15585/mmwr.su7102a1. [Google Scholar] [PubMed] [CrossRef]
7. Parrish BP, Cohen LH, Laurenceau JP. Prospective relationship between negative affective reactivity to daily stress and depressive symptoms. J Soc Clin Psychol. 2011;30(3):270–96. doi:10.1521/jscp.2011.30.3.270. [Google Scholar] [CrossRef]
8. Hammen C. Depression and stressful environments: identifying gaps in conceptualization and measurement. Anxiety, Stress, & Coping. 2016;29(4):335–51. doi:10.1080/10615806. [Google Scholar] [CrossRef]
9. Page KM, Milner AJ, Martin A, Turrell G, Giles-Corti B, LaMontagne AD Workplace stress. J Occup Environ Med. 2014;56(8):814–9. doi:10.1097/JOM.0000000000000230. [Google Scholar] [PubMed] [CrossRef]
10. Schneiderman N, Ironson G, Siegel SD. Stress and health: psychological, behavioral, and biological determinants. Annu Rev Clin Psycho. 2005;1(1):607–28. doi:10.1146/annurev.clinpsy.1.102803.144141. [Google Scholar] [PubMed] [CrossRef]
11. Serrão C, Duarte I, Castro L, Teixeira A. Burnout and depression in Portuguese healthcare workers during the COVID-19 pandemic-the mediating role of psychological resilience. Int J Environ Res Public Health. 2021;18(2):636. doi:10.3390/ijerph18020636. [Google Scholar] [PubMed] [CrossRef]
12. Kidger J, Araya R, Donovan J, Gunnell D. The effect of the school environment on the emotional health of adolescents: a systematic review. Pediatr. 2012;129(5):925–49. doi:10.1542/peds.2011-2248. [Google Scholar] [PubMed] [CrossRef]
13. Herrenkohl TI, Kosterman R, Hawkins JD, Mason WA. Effects of growth in family conflict in adolescence on adult depressive symptoms: mediating and moderating effects of stress and school bonding. J Adolesc Health. 2009;44(2):146–52. doi:10.1016/j.jadohealth.2008.07.005. [Google Scholar] [PubMed] [CrossRef]
14. Moylan CA, Herrenkohl TI, Sousa C, Tajima EA, Herrenkohl RC, Russo MA. The effects of child abuse and exposure to domestic violence on adolescent internalizing and externalizing behavior problems. J Fam Violence. 2010;25(1):53–63. doi:10.1007/s10896-009-9269-9. [Google Scholar] [PubMed] [CrossRef]
15. Giletta M, Choukas-Bradley S, Maes M, Linthicum KP, Card NA, Prinstein MJ. A meta-analysis of longitudinal peer influence effects in childhood and adolescence. Psychol Bull. 2021;147(7):719–47. doi:10.1037/bul0000329. [Google Scholar] [PubMed] [CrossRef]
16. Ricci RC, Paulo ASC, Freitas AKPB, Ribeiro IC, Pires LSA, Leite Facina MA, et al. Impacts of technology on children’s health: a systematic review. Revista Paulista de Pediatria: Orgao Oficial da Sociedade de Pediatria de Sao Paulo. 2022;41:e2020504. doi:10.1590/1984-0462/2023/41/2020504. [Google Scholar] [PubMed] [CrossRef]
17. Leiva-Bianchi M, Baher G, Poblete C. The effects of stress coping strategies in post-traumatic stress symptoms among earthquake survivors: an explanatory model of post-traumatic stress. Terapia Psicológica. 2012;30(2):51–9. doi:10.4067/S0718-48082012000200005. [Google Scholar] [CrossRef]
18. Kantor E, Vuletić G. The relationship between mental health and stress: the moderating role of satisfaction with friendships. Adv Ment Health. 2023;53:1–14. doi:10.1080/18387357.2023.2282046. [Google Scholar] [CrossRef]
19. Delisle TT, Werch CE, Wong AH, Bian H, Weiler R. Relationship between frequency and intensity of physical activity and health behaviors of adolescents. J School Health. 2010;80(3):134–40. doi:10.1111/j.1746-1561.2009.00477.x. [Google Scholar] [PubMed] [CrossRef]
20. Hallgren M, Stubbs B, Vancampfort D, Lundin A, Jääkallio P, Forsell Y. Treatment guidelines for depression: greater emphasis on physical activity is needed. Eur Psychiatry. 2017;40:1–3. doi:10.1016/j.eurpsy.2016.08.011. [Google Scholar] [PubMed] [CrossRef]
21. Denche-Zamorano Á, Barrios-Fernandez S, Gómez-Galán R, Franco-García JM, Carlos-Vivas J, Mendoza-Muñoz M, et al. Associations between physical activity level and mental health in the Spanish population: a cross-sectional study. Healthcare. 2022;10(8):1442. doi:10.3390/healthcare10081442. [Google Scholar] [PubMed] [CrossRef]
22. Biddle SJH, Ciaccioni S, Thomas G, Vergeer I. Physical activity and mental health in children and adolescents: an updated review of reviews and an analysis of causality. Psychol Sport Exerc. 2019;42:146–55. doi:10.1016/j.psychsport.2018.08.011. [Google Scholar] [CrossRef]
23. Wu K, Wang S, Ding T, Li Y. The direct effect of exercise on the mental health of scientific and technological professionals and the mediating effects of stress, resilience, and social support. Front Public Health. 2023;11:1074418. doi:10.3389/fpubh.2023.1074418. [Google Scholar] [PubMed] [CrossRef]
24. Ren Y, Li M. Influence of physical exercise on social anxiety of left-behind children in rural areas in China: the mediator and moderator role of perceived social support. J Affect Disord. 2020;266:223–9. doi:10.1016/j.jad.2020.01.152. [Google Scholar] [PubMed] [CrossRef]
25. Lu X, Wang K. Influence of extracurricular physical exercise on psychological capital, psychological health and social adaptability of college students. Chinese J School Health. 2019;40(3):392–5. doi:10.16835/j.cnki.1000-9817.2019.03.021. [Google Scholar] [CrossRef]
26. Thorén P, Floras JS, Hoffmann P, Seals DR. Endorphins and exercise: physiological mechanisms and clinical implications. Med Sci Sport Exer. 1990;22(4):417–28. [Google Scholar]
27. Schwarz L, Kindermann W. Changes in β-endorphin levels in response to aerobic and anaerobic exercise. Sports Med. 1992;13(1):25–36. doi:10.2165/00007256-199213010-00003. [Google Scholar] [PubMed] [CrossRef]
28. Maletic V, Robinson M, Oakes T, Iyengar S, Ball SG, Russel J. Neurobiology of depression: an integrated view of key findings. Int J Clin Pract. 2007;61(12):2030–40. doi:10.1111/j.1742-1241.2007.01602.x. [Google Scholar] [PubMed] [CrossRef]
29. Xie Y, Wu Z, Sun L, Zhou L, Wang G, Xiao L, et al. The effects and mechanisms of exercise on the treatment of depression. Front Psychiatry. 2021;12:705559. doi:10.3389/fpsyt.2021.705559. [Google Scholar] [PubMed] [CrossRef]
30. Telles S, Gupta RK, Bhardwaj AK, Singh N, Mishra P, Kumar Pal D, et al. Increased mental well-being and reduced state anxiety in teachers after participation in a residential yoga program. Med Sci Monit Basic Res. 2018;24:105–12. doi:10.12659/MSMBR.909200. [Google Scholar] [PubMed] [CrossRef]
31. DiLorenzo TM, Bargman EP, Stucky-Ropp R, Brassington GS, Frensch PA, LaFontaine T. Long-term effects of aerobic exercise on psychological outcomes. Prev Med. 1999;28(1):75–85. doi:10.1006/pmed.1998.0385. [Google Scholar] [PubMed] [CrossRef]
32. Petruzzello SJ, Landers DM, Hatfield BD, Kubitz KA, Salazar W. A meta-analysis on the anxiety-reducing effects of acute and chronic exercise. Outcomes Mech. Sports Med. 1991;11(3):143–82. doi:10.2165/00007256-199111030-00002. [Google Scholar] [PubMed] [CrossRef]
33. McDowell CP, Dishman RK, Gordon BR, Herring MP. Physical activity and anxiety: a systematic review and meta-analysis of prospective cohort studies. Am J Prev Med. 2019;57(4):545–56. doi:10.1016/j.amepre.2019.05.012. [Google Scholar] [PubMed] [CrossRef]
34. Twigg E, Barkham M, Bewick BM, Mulhern B, Connell J, Cooper M. The young person’s CORE: development of a brief outcome measure for young people. Couns Psychother Res: Linking Res Pract. 2010;9:160–8. doi:10.1080/14733140902979722. [Google Scholar] [CrossRef]
35. Marinković V, Vrsaljko D, Vulić-Prtorić A. Psychometric validation of the CORE questionnaire in a sample of adolescents. In: Vulić-Prtorić A, Ćubela Adorić V, Proroković A, Sorić I, Valerjev P, editors. Psychology days in Zadar. Zadar: Department of Psychology, University of Zadar; 2008. pp. 13. [Google Scholar]
36. Caser H. Anxiety, depression, perceived competence, and locus of control in healthy children and children with psychiatric disorders. Master’s thesis. Faculty of Education, University of Rijeka: Rijeka; 1997. [Google Scholar]
37. Zaić A. The relationship between symptoms of anxiety, depression, and somatization in childhood (Master’s Thesis). Department of Psychology, Faculty of Humanities and Social Sciences, University of Zagreb: Zagreb; 2005. [Google Scholar]
38. Kovacs M. Rating scales to assess depression in school-aged children. Acta Paedopsychiatr. 1981;46:305–15. [Google Scholar] [PubMed]
39. Marinović L, Vulić-Prtorić A. A comparison of two scales of child depression regarding some psychometric characteristics. Papers Fac Philos Zadar. 2000;39(16):155–77. doi:10.15291/radovifpsp.2543. [Google Scholar] [CrossRef]
40. Sabljić E. Examining school absences with respect to gender, grade, academic performance, and the intensity of school stress (Unpublished Undergraduate Thesis). Faculty of Humanities and Social Sciences, University of Zagreb: Zagreb; 2000. [Google Scholar]
41. Kowalski KC, Crocker PRE, Donen RM. The Physical Activity Questionnaire for Older Children (PAQ-C) and Adolescents (PAQ-A) manual. Saskatoon, Canada: College of Kinesiology, University of Saskatchewan; 2004. [Google Scholar]
42. Vidaković Samaržija D, Mišigoj-Duraković M. Reliability of the croatian version of the questionnaire for assessing the overall level of physical activity in younger school-aged children. Croat Sport Med J. 2013;28(1):24–32. [Google Scholar]
Cite This Article
 Copyright © 2024 The Author(s). Published by Tech Science Press.
Copyright © 2024 The Author(s). Published by Tech Science Press.This work is licensed under a Creative Commons Attribution 4.0 International License , which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
 Downloads
Downloads
 Citation Tools
Citation Tools