
 Submit a Paper
Submit a Paper Propose a Special lssue
Propose a Special lssue Open Access
Open Access
ARTICLE
Intelligence COVID-19 Monitoring Framework Based on Deep Learning and Smart Wearable IoT Sensors
1 Information Assurance and Security Research Group (IASRG), Faculty of Computing, Universiti Teknologi Malaysia (UTM), Johor Bahru, Johor, 81310, Malaysia
2 Department of Computer Science, College of Computers and Information Technology, Taif University, Taif, 21944, Saudi Arabia
3 Department of Information Systems, Faculty of Computing and Information Technology, King Abdulaziz University, Jeddah, 21589, Saudi Arabia
4 College of Computing and Informatics, Department of Computer Science, University of Sharjah, Sharjah, 27272, United Arab Emirates
* Corresponding Author: Fadhil Mukhlif. Email:
Computers, Materials & Continua 2023, 77(1), 583-599. https://doi.org/10.32604/cmc.2023.038757
Received 31 January 2023; Accepted 11 April 2023; Issue published 31 October 2023
 View Full Text
View Full Text Download PDF
Download PDFAbstract
The World Health Organization (WHO) refers to the 2019 new coronavirus epidemic as COVID-19, and it has caused an unprecedented global crisis for several nations. Nearly every country around the globe is now very concerned about the effects of the COVID-19 outbreaks, which were previously only experienced by Chinese residents. Most of these nations are now under a partial or complete state of lockdown due to the lack of resources needed to combat the COVID-19 epidemic and the concern about overstretched healthcare systems. Every time the pandemic surprises them by providing new values for various parameters, all the connected research groups strive to understand the behavior of the pandemic to determine when it will stop. The prediction models in this research were created using deep neural networks and Decision Trees (DT). DT employs the support vector machine method, which predicts the transition from an initial dataset to actual figures using a function trained on a model. Extended short-term memory networks (LSTMs) are a special sort of recurrent neural network (RNN) that can pick up on long-term dependencies. As an added bonus, it is helpful when the neural network can both recall current events and recall past events, resulting in an accurate prediction for COVID-19. We provided a solid foundation for intelligent healthcare by devising an intelligence COVID-19 monitoring framework. We developed a data analysis methodology, including data preparation and dataset splitting. We examine two popular algorithms, LSTM and Decision tree on the official datasets. Moreover, we have analysed the effectiveness of deep learning and machine learning methods to predict the scale of the pandemic. Key issues and challenges are discussed for future improvement. It is expected that the results these methods provide for the Health Scenario would be reliable and credible.Keywords
World Health Organization (WHO) decided on 11 March 2020 that the global spread of the coronavirus illness COVID-19 warranted the declaration of a pandemic [1]. The 2019 new coronavirus epidemic, dubbed COVID-19 by the World Health Organization (WHO), has also put several countries in a difficult situation. At first, mainly felt by Chinese people, the effects of the COVID-19 outbreaks have now become a major global issue. Many nations have gone under partial or total lockdown due to the lack of resources to deal with the COVID-19 pandemic and the concern of overwhelmed healthcare systems. There has been a worldwide epidemic of coronaviruses, with over 585 million cases confirmed by laboratories and over 6 million fatalities attributed to the virus as of August 14, 2022 as shown in Fig. 1. Fig. 2 also depicts the global distribution of confirmed cases across regions, with Europe having the highest total at over 275 million, followed by the Western Pacific with over 204 million confirmed cases. However, Africa and the Eastern Mediterranean have the most people living in extreme poverty, with over 9 and 23 million, respectively [2].
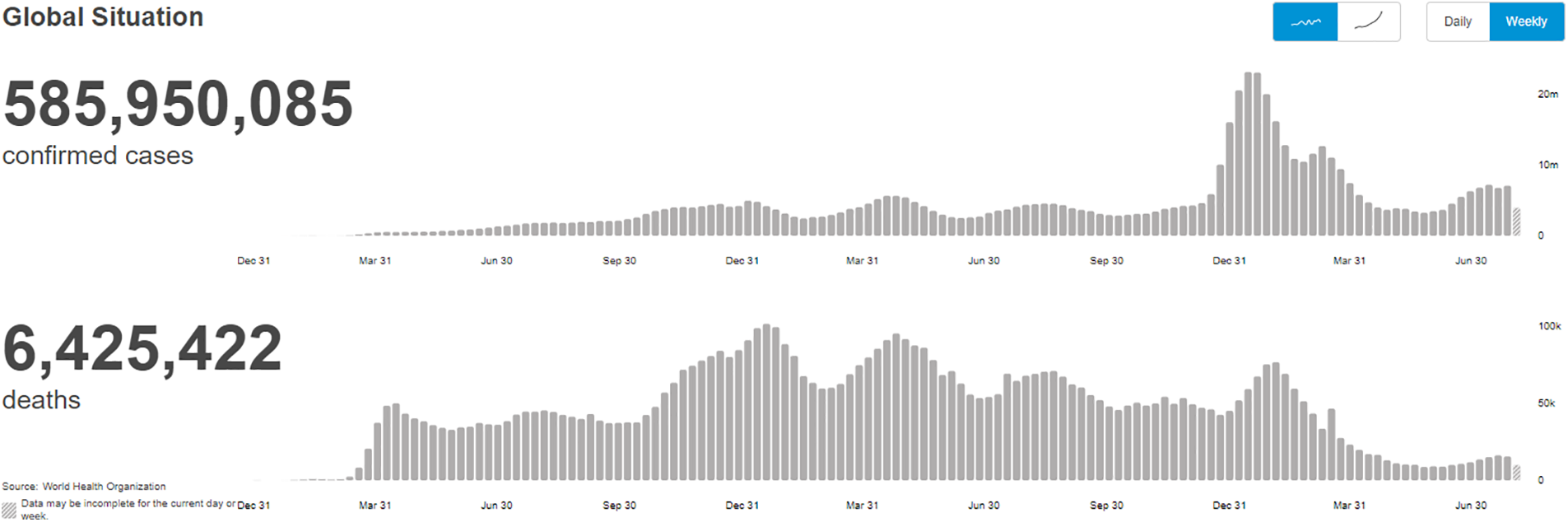
Figure 1: Global situation of COVID-19
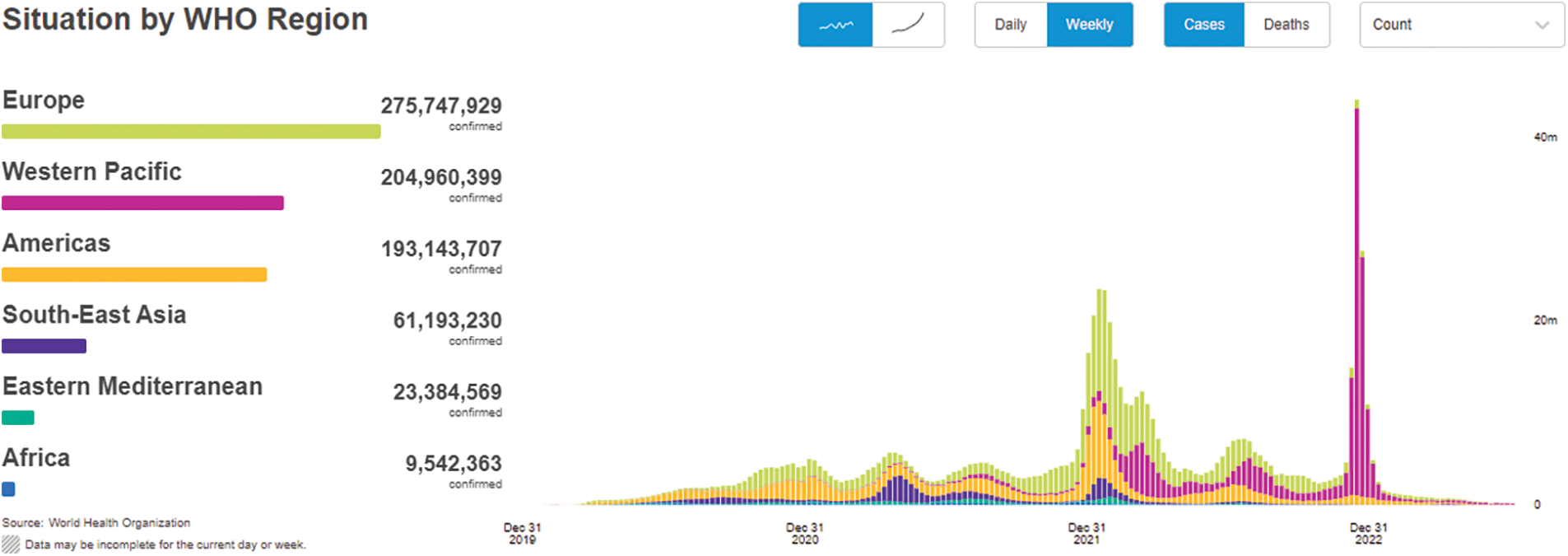
Figure 2: COVID-19 situation by region
According to [2], this condition is marked by rapid development and serious vulnerability to infection. Droplets expelled while sneezing and coughing, as well as contact with infected surfaces, are the primary transmission vectors. Moreover, it could be spread from asymptomatic carriers to others who come into touch with them. The incubation period for this virus is short, ranging from one day to two weeks, yet it is still contagious. In addition, it may live for up to nine days at ambient temperature on surfaces, which aids in its transmission. This infectious illness is, thus, a pressing issue in the medical community. The coronaviruses are also known to cause severe respiratory diseases. COVID-19 may cause many symptoms, such as a high body temperature, a persistent cough, extreme exhaustion, and difficulty breathing. Acute respiratory syndrome coronavirus and Middle East respiratory syndrome coronavirus are two more coronaviruses that cause pneumonia similarly to this one. Moreover, it may result in organ failure, leading to a decline in a person’s physiological state and ultimately death. Complications might be more severe for the elderly and people with several medical conditions [3,4].
Therefore, it is essential to create reliable outbreak prediction models to investigate the transmission of this illness. As such, we advocated deploying a model like the one shown in Fig. 3 to identify and anticipate emerging social problems. Because of this concept, governments and other legislative bodies may propose new policies and evaluate their efficacy. In contrast to previous recent pandemics, the worldwide COVID-19 pandemic behaves novel, demonstrating the doubtful accuracy of established models. Furthermore, the complexity of population behavior across areas and the variety of containment measures contribute to the wide range of estimates given by the models.
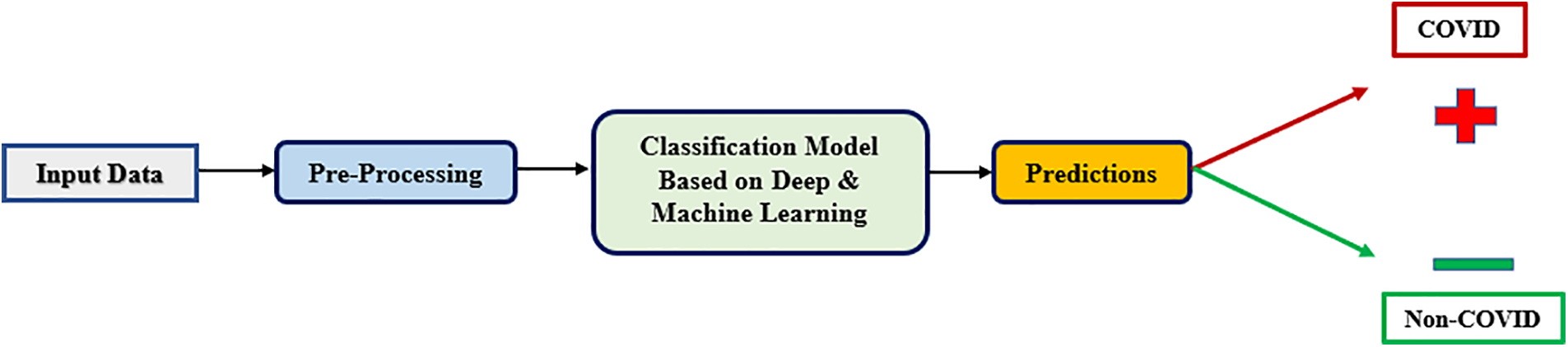
Figure 3: Proposed system architecture
Meanwhile, IoT-cloud integrated an intelligent healthcare system [5]. From the standpoint of the smart city, this design employs smart connection sensors and deep learning (DL) for intelligent decision-making. The smart technology monitors patients in real-time and provides an affordable, high-quality medical treatment that is also trustworthy, and prompt medical treatment. To evaluate the proposed system’s effectiveness, we conduct tests to identify COVID-19 using DL. The healthcare data we capture, transmit, and monitor is done so with the use of a sensor. The cognitive module is kept in the cloud, and IoT sensors upload CT scan pictures from patients. The system analyzes Computer Tomography (CT) scan pictures to determine the patient’s condition. This choice is made in real-time by the DL cognitive module. On the contrary, wearables are linked to the internet and serve to improve communication while they are worn on the body. Smartwatches like the Apple Watch, activity trackers, personal sensors, and patches are all examples of wearable technology. Considering the present health crisis, wearables are well suited for deployment in the healthcare industry to help with COVID-19 impact management due to their capacity to monitor physical and mental health. This wearable technology enables remote health monitoring of their personnel and documentation of any COVID-19 transmission among them. It allows us to control the illness before it spreads over the whole population. When activated, it searches for nearby wearables and records their proximity and interactions. The tech within the gadgets consists of a passive GPS position tracker, Bluetooth-enabled proximity sensors, ultra-wideband connection, built-in Long Term Evolution (LTE), and a rechargeable battery [6].
Moreover, like a wristwatch, each gadget features a display and control buttons that light up when activated. These buttons will let workers keep track of their current health conditions as they happen. If the wearer is healthy, experiencing symptoms, or has been confirmed to be sick, the user can update their status accordingly. An individual’s health status updates are saved in a centralized database for up to six weeks after the wearer has entered them. Devices of this kind come in three forms: a card-shaped one, a pebble-shaped one worn around the neck, and a wrist-worn one [3].
To analyze the massive amounts of data required to intelligently discover infected persons by a virus, artificial intelligence technologies like deep learning and machine learning must be optimized for the size of the dataset. Deep learning algorithms are more efficient than classic ML methods in processing ever-increasing data loads. However, traditional machine learning methods outperform deep learning algorithms on small datasets [7]. Deep Learning (DL) and Decision Tree (DT) are examples of common machine learning techniques inspired by how humans think. Deep learning (DL) algorithms rely on Neural Networks (NN) to explain complicated systems; these NNs are built on top of conventional Artificial Neural Networks (ANN) and are structured similarly to the human brain in terms of a hierarchical network of primary neurons [8]. Suppose you want to improve the readability of a classification system based on a collection of if-then rules. In that case, you should look at decision trees (DT), a supervised machine learning technique. In a decision tree, there are two nodes: leaf nodes (representing the outcomes of a process) and decision nodes (choice between alternatives). Decision trees are used to forecast a class or target using inferred decision rules from training data. According to their specific traits, DL and DT algorithms fall under the umbrella of supervised learning [9,10].
The most important contribution of this study are as follows:
• We provide an overview of the intelligence COVID-19 monitoring.
• We developed a solid foundation for smart healthcare and monitoring systems.
• We proposed an intelligence COVID-19 monitoring framework
• We calculate the total number of infections, cures, and deaths using dataset collected from the official WHO website.
• We examine the use of deep learning and decision tree models data reported up to August 2022.
• We Analyze the effectiveness of deep learning and decision tree methods to predict the scale of the pandemic.
The rest of the paper is laid out: The associated activities and inspirations are discussed in Section 2. In Section 3, we cover the framework for an intelligent healthcare scenario. In Section 4, the materials and procedures are outlined. Model evaluation procedures are discussed in detail in Section 5. In Section 6, we look at the study’s difficulties and potential for improvement. In Section 7, we cover what we see in store for the future. The results are summed up and the paper is wrapped up in Section 8.
To forecast the health of COVID-19 patients for effective monitoring and early treatment, the authors of [11] developed a decision-level fusion technique that incorporates Random Forest (RF), Gradient Boosting (GB), and X Gradient Boosting (XGB) classification algorithms. Soft voting combines the results from all three approaches into a single final forecast. The selected categorization approaches and suggested fusion techniques employ the COVID-19 patients’ health data, including demographic and geographical information about their travels, to speculate on the likely result of COVID-19 cases. Patients’ data may indicate that the prediction’s outcomes range from recovery to death. Experiments are performed on a public new Corona Virus 2019 dataset with a variable ratio of test sets. The COVID-19 epidemic in Egypt is predicted using AI-based models [12]. Among them are the LSTM, the convolutional neural network, and the multilayer perceptron neural network models. Dataset records from 14 February 2020 to 15 August 2020 are used for training and validation. The models’ performance is measured by the root mean square error and the determination coefficient.
When comparing several models for estimating future cumulative infections, the LSTM model performs the best a week and a month out. To create these forecasting models, we employed the Support Vector Regression (SVR) and deep neural network approach. Using a training model, SVR applies the notion of a support vector machine, which estimates the mapping from the input domain to the actual numbers using a function. Extended short-term memory networks (LSTM) are a subtype of RNN that may be trained to recognize and generalize across time-dependent relationships. In addition to being an accurate predictor of COVID-19, it is also advantageous when the neural network needs to flip between remembering everyday items and things from a long time ago [13]. COVID-19 spreads gradually yet have widespread, devastating effects. But most infected persons only have mild to moderate symptoms and do not need hospitalization. That is why it is crucial to work on early detection and therapy methods. One example is proteomic technology, which uses a procedure called blood protein profiling. The purpose of this investigation is to use Deep Learning (DL), Random Forest (RF), and Gradient Boosted Trees (GBTs) to categorize COVID-19-positive patients into three categories (mild, severe, and critical) and a control group based on the blood protein profile [14].
IoT-cloud integrated an intelligent healthcare system [5]. From the standpoint of the smart city, this design employs smart connection sensors and deep learning (DL) for intelligent decision-making. The smart technology monitors patients in real-time and provides an affordable, high-quality medical treatment that is also trustworthy, and prompt medical treatment. To evaluate the proposed system’s effectiveness, we conduct tests to identify COVID-19 using DL. The healthcare data we capture, transmit, and monitor is done so with the use of a sensor. The cognitive module is kept in the cloud, and IoT sensors upload CT scan pictures from patients. The system analyzes CT scan pictures to determine the patient’s condition. This choice is made in real-time by the DL cognitive module. To identify and categorize whether patients are healthy or infected with COVID-19, we employ a state-of-the-art classification method based on DL, i.e., ResNet50, to be relayed to a cognitive module. Until a vaccine is available, the authors [15] stress the significance of adopting integrated technology to cope with COVID-19 and future pandemics. They discussed potential frameworks for mental health care, infection prevention, physical health monitoring, and contract tracking. In addition, we introduced the VIrus Resistance Framework employing the Internet of Medical Things (VIRFIM), which integrates all the modules, gave a high-level explanation of how it works, and outlined some of the difficulties we anticipate encountering along with the strategies we propose for overcoming them. Additionally, VIRFIM is assumed to be able to protect people from catching new coronaviruses via the use of best practices. We anticipate that VIRFIM will not only draw attention to the benefits of adopting wearable/mobile sensors for personal prevention but also encourage governmental and corporate decision-makers to reallocate funds to the program.
The beta coronavirus that causes Severe Acute Respiratory Syndrome (SARS-CoV-2) is responsible for the 19th coronavirus outbreak disease (COVID-19) [16]. On 31 December 2019, the first instance of infection with COVID-19 was recorded in Wuhan City, Hubei Province of China. Since then, the virus has spread rapidly to almost all nations, 214 countries, and territories since writing this article. The situation shows no signs of improving, and the number of new infections and fatalities continues to rise. In response to the worldwide significance of the COVID-19 epidemic, many resources have been devoted to finding effective countermeasures. The government’s activities are crucial in stopping the pandemic; for example, they must quarantine the affected region, give a crisis package to mitigate the effects on the economy and population and create adaptive policies in response to the COVID-19 epidemic.
Meanwhile, people are urged to take preventative measures for their health and the health of others by, for example, washing their hands regularly, keeping a socially foreign policy, and reporting any new symptoms to the local health center. However, efforts to advance knowledge in areas directly related to COVID-19 have recently garnered increased funding and attention from a wide range of institutional and organizational actors. References [17], for instance, investigated many characteristics of supply networks, such as their viability, stability, robustness, and resilience, and showed significant implications of the COVID-19 pandemic on the global supply chain. The battle against the COVID-19 coronavirus has included early attempts by computer science experts and the worldwide endeavor to create a viable vaccine and medical therapy. We offer state-of-the-art techniques and approaches based on AI and big data for combating the COVID-19 coronavirus illness, motivated by the fantastic success of AI and big data in numerous sectors [18].
It has been shown that deep learning could be a valuable tool for helping healthcare professionals and academics uncover previously undiscovered links in healthcare data. Medical professionals may utilize deep learning to make more precise diagnoses and benefit from the field’s insights on illness treatment. Deep learning has the potential to aid in the development of novel medications and the further refinement of current ones via its use in the field of drug discovery. Deep learning methods may examine a patient’s medical records and provide therapy recommendations based on what’s found. Additional information may be gleaned from patient records, such as the results of tests and observations of symptoms, to make predictions about future trends. Magnetic Resonance Imagings (MRIs), CT scans, and Electrocardiograms (ECGs) are medical imaging that may benefit from deep learning methods to detect and diagnose potentially life-threatening conditions, including cardiovascular illness, cancer, and brain tumors. Doctors can properly assess potentially fatal conditions, which benefits patients and the quality of care they deliver. Early detection of cancer and other similar disorders is possible using deep learning. Patient insurance fraud may be discovered using deep learning methods by evaluating medical insurance and claims data. Potential allegations of fraud may be anticipated using this method. Using patient data, deep learning may also promote the health insurance sector [7]. References [7,19] developed a Smart Healthcare System for Severity Prediction and Critical Tasks Management (SHSSP-CTM) for COVID-19 patients. While reference [20] identifies three important indicators (lymphocyte, CRP, and SpO2) that have been proven pathologically and technically. Reference [21] proposes a Multidimensional Examination Framework (MEF) for the prioritization of COVID-19 severe patients based on combined multi-criteria decision-making (MCDM) methods.
Meanwhile, wearables are linked to the web and serve to improve communication while they are worn on the body. Smartwatches like the Apple Watch, activity trackers like the Fitbit, smart headbands like the Dreem, and even personal sensors and patches are all examples of wearable technology. Wearables are an excellent tool for use in healthcare because of their potential to monitor patients’ physical health and emotional well-being. In response to the present health problem, several companies have released updated products or introduced brand-new wearables to mitigate the effects of COVID-19 [3].
After the advent of modern computers, Alan Turing invented the term Artificial Intelligence (AI) in 1950 [22,23]. To differentiate between machines and humans, he created the Turing Test, which consists of a series of questions and replies. If the computer proved itself intelligent, it would be treated as a human. In 1956, AI became its academic field after being investigated by a few academics in response to the Turing Test [24]. The original definition of AI centered on the ability of the agent to learn and solve problems in response to a dynamic external environment. However, although many researchers sought to apply AI to many study topics over the course of 60 years, it did not substantially progress until the 21st century, due in part to difficulties in seeing the environment’s variability as a restriction of computing capabilities. Artificial Intelligence (AI) has made significant strides in the 2000s because of the proliferation of Internet-connected devices, sensors, big data, and other technologies that facilitate the sharing, merging, and synthesis of information and expertise [25]. Natural language processing, knowledge representation, automated reasoning, and machine learning are a few of the numerous modern study foci in artificial intelligence [26,27]. Among them, machine learning is an essential field of study for AI. Scientists have been attempting to use machine learning to spot patterns in data or extrapolate future outcomes from existing datasets without manually instructing the computer.
Deep Learning (DL) and Decision Tree (DT) are examples of common machine learning techniques inspired by how humans think. Deep Learning (DL) algorithms rely on Neural Networks (NN) to explain complicated systems; these NNs are built on top of conventional Artificial Neural Networks (ANN) and are structured similarly to the human brain in terms of a hierarchical network of primary neurons [8]. Suppose you want to improve the readability of a classification system based on a collection of if-then rules. In that case, you should look at Decision Trees (DT), a supervised machine learning technique. In a decision tree, there are two nodes: leaf nodes (representing the outcomes of a process) and decision nodes (choice between alternatives). Decision trees are used to forecast a class or target using inferred decision rules from training data. According to their specific traits, DL and DT algorithms fall under the umbrella of supervised learning [9,10].
3 Smart Healthcare Scenario Architecture
Innovative healthcare frameworks are being created as part of a smart city’s infrastructure. Intelligent sensor devices for health monitoring are made possible for doctors, stakeholders, and locals. They can access their electronic health records from anywhere due to cloud computing and the Internet of Things. Determinations are more rational and precise when cognitive abilities are present. The real-time analysis, tracking, and integration of data performed by the cognitive system inform patients’ decisions about the most appropriate care they may get. Reports about a person’s health are uploaded to a cloud service and can be accessed by doctors remotely to provide patients with better advice. The smart healthcare system focuses on four primary goals: accurate diagnosis, cheap cost, reduced patient expenses, easy access, and improved quality of life. We propose an Internet of Things and a cloud-based medical infrastructure to achieve these aims. Residents of a smart city must sign up for infrastructure to use its services. Residents and medical professionals may communicate freely after registering.
Authorized parties may access the cognitive module to obtain health data and other sensitive information about patients safely. In an emergency, the patient’s position is continually tracked so that help may be sent immediately. The cognitive system retrieves the patient’s condition and sends the gathered data to the cloud, which is processed by the deep learning cognitive module. When COVID-19 is found, the deep learning module provides the results of a binary classification. These results suggest that the brain is trying to get a jump on future projects. The outcomes are shared with medical specialists for in-depth analysis through health reports. When an emergency occurs, the cognitive gadget sends out alerts and messages. A smart ambulance or mobile clinic can locate the patient and arrive at their location in record time. The smart traffic system also ensures that emergency services can quickly and efficiently reach the scene. This is how the digital cognitive smart healthcare system provides its citizens with access to necessary medical treatment.
Fig. 4 depicts the architecture of the proposed intelligent health care system. Smart Internet of Things sensors sends the data they gather. Low-power networking devices are used in the Local Area Network (LAN). Tier 2 is where the data from the intelligent IoT sensor and the device are sent to another layer, the hosting layer. Intelligent gadgets, such as portable multimedia players and laptops with the ability to store and send signals, make up the hosting layer. When smart devices are linked to a Wide Area Network (WAN), they may upload their data to a remote server.

Figure 4: Intelligence COVID-19 monitoring framework
The wide area network (WAN) layer facilitates instantaneous data transfers to the cloud using high-speed data networks like Cellular local area network (LAN), Fifth Generation (5G), or Sixth Generation (6G). Patient data is verified on the cloud by the cloud manager and then sent to the deep learning cognitive module. Connected sensors that can process and transmit data intelligently are employed. Patients may have any of these sensors implanted into their environment. Similarly, this gadget can communicate with other IoT gadgets. Zigbee, Low Power Wide Area Network (LoWPAN), and Bluetooth are just a few examples of the short-range networking technologies that make up the LAN.
The hosting layer provides access to many forms of intelligence, such as multimedia cellphones, laptops, tablets, and human digital assistants. Devices like this use in-house memory and custom-built software to decode incoming signals. These little computers can provide users with preliminary and broad health assessments. The access layer sends data to the middleware in the cloud, which processes the information. The cloud layer comprises a cloud manager and a deep learning cognitive module. The cloud administrator controls the flow of information and employs all authentication procedures to verify the identities of all participants in the intelligent city ecosystem. After patient verification, the DL cognitive module examines the data to make a diagnosis. It uses intelligent inference from compiled data to pinpoint COVID-19. The cognitive module receives identification results from deep learning models and then ultimately assesses the patient’s status and notifies the relevant parties. After that, doctors and nurses check in on the patients to see how things are doing.
During this epidemic, it is crucial to keep an eye on people’s physical health, mainly if they have chosen to isolate themselves out of fear of infection or precaution after receiving the vaccination. It also relieves pressure on overburdened healthcare facilities that see individuals with very minor conditions. A higher price tag goes hand in hand with an increase in integrated sensors. However, certain high-quality, low-cost smartwatches may be utilized for inexpensive physical health monitoring. Some digital equipment designed to track a patient’s physical condition on an individual basis may also be used for this purpose. Connected to a smartphone, a “smartwatch” may keep tabs on a user’s activity, temperature, oxygen levels, and any other observable anomalies that may indicate a need for medical attention. Aside from being a valuable tool for monitoring the patient’s behavior, regular physical exercise enhances the body’s defenses. In the next part, we’ll explain how to improve your immunity with exercise and a healthy diet. Here, we discuss keeping tabs on the patient’s physical activity and making sure it stays consistent with the regimen their caregiver or doctor has prescribed when they are home alone.
The accelerometer, gyroscope, magnetometer, and orientation sensors included in smartphones and smartwatches have seen a widespread application for tracking motion throughout the years. The inconsistency in sampling rate, recording units, and other metrics across wearable sensor devices, as well as the absence of individualized data, are significant obstacles to the adaption of activity monitoring systems. Some studies partially address this issue by employing semi-population calibration to enable personalized activity recognition with a low-to-moderate amount of annotated data or by using transfer learning strategies that consider the domain adaptation of different sensor characteristics. Patients may be monitored automatically and with little human intervention, thanks to advances in physical activity detection.
Due to the severity of the COVID-19 pandemic, monitoring both skin temperature and oxygen saturation levels is of the highest significance. As a respiratory syndrome, COVID-19 (SARS-nCOV-19) produces high fever and breathing difficulties in the afflicted person. World Health Organization reports that fever and breathing problems are the most frequent symptoms of contracting the COVID 19 virus. It is reassuring for both patients and physicians because smartwatches may be used to track vital signs, including body temperature and Oxygen Saturation (SpO2). During the quarantine period, an increase in skin temperature or a drop-in oxygen level might prompt the patient to act or alert the attending physician. When vaccinated, a person may choose to isolate themselves voluntarily; in this scenario, the sensor modalities may be employed to record temperature and oxygen responses [5].
There has been much talk about the potential of wearable sensors for use in anomaly detection. Due to memory loss or other factors, many elderly people choose to live alone, putting them at risk of accidents like falls or slips and the possibility of not taking their prescriptions. Anomaly detection in the isolation phase may be used to keep an eye out for unusual behavior that might signal for help in the event of a sudden fall or remind a patient to take their prescription at a particular time. Several research studies have suggested smartwatches and cellphones to reliably detect falls [15]. Object, infrared, or location sensors might be installed at the isolation center or the site where people go to be isolated to identify abnormal sleeping, eating, and physical habits, which could provide valuable insight to caretakers tracking the spread of the infection.
The Physical Healthcare Monitoring Module (PHM) is a theoretical framework we suggest. The smartphone is the middleware that transfers sensor data to the service layer, which may be used to provide the requested service. After that, the smartphone must either get the decision from the protocol stack and display it in the smartphone app or it must communicate the decision to the medical personnel for further action. The physical healthcare monitoring module for patient monitoring consists of Skin Temperature (ST), Oxygen Saturation (SpO2), Physical Activity Monitoring (PAM), and Anomaly Detection (AD).
Predicting the spread of the COVID-19 pandemic is the primary focus of this investigation. Fig. 5 displays the proposed framework’s technique for making predictions. The following procedures are used to get this goal: The six stages of producing a COVID-19 prediction are as follows: collecting data, processing it, dividing it into training and testing sets, utilizing deep and machine learning models, evaluating model performance, and employing the best model for forecasting. The following sections elaborate on the suggested structure.

Figure 5: Research approach flowchart
Not only that, but the data, models, and evaluation metrics are vital to the whole process of the article strategy. As can be seen in the diagram below, our proposed data architecture is very flexible. By modifying the input data, models, or evaluation model, one may get wholly different results for different circumstances. Therefore, consider this one of our inputs to the conversation. Nonetheless, Fig. 6 illustrates the analysis of the dataset supplied in this article to elaborate on the technique of the proposed system. As a result, the data set went through four distinct phases: collection, classification, presentation, and evaluation.

Figure 6: Data analysis
Back propagating long sequences can result in an inaccurate learned model and a protracted training process, and both problems are common with sequence data. The data must be cleaned and sorted before being fed into neural networks, making preprocessing an essential step. In the data preparation step, normalization and standardization are two methods that are often utilized [12]. In this analysis, data standardization was used to convert all values to a scale between zero and one for both the mean and standard deviation. Once the information is standardized, neural networks analyze time series by breaking down each sub-sequence into input and output observations. The first 20 data points of each subsequence are used as inputs in a model, and the final data point is predicted directly from the model.
More specifically, the first 80% of the dataset is used for training, while the remaining 20% is used for testing. Models are trained and optimized with the help of the training set, while model efficacy is evaluated with the help of the test set.
Deep Learning is a kind of artificial intelligence that allows computers to learn how to recognize images, recognize faces, and extract other types of features. It uses a series of layers to carry out its functions. The output of one layer is sent into the next layer to be further processed [14]. Deep learning algorithms are a subset of machine learning algorithms that differ from the norm. Rather than relying on a single mathematical model to guide their computations, deep learning algorithms use network topologies depicted as a neural network. This research used a multi-layer feed-forward neural network trained using stochastic gradient descent and backpropagation as our deep learning architecture.
• Long Short-Term Memory Network (LSTM)
LSTM, a kind of deep recurrent neural network (RNN), has become so popular because of the built-in memory it provides. Long-term data processing and dependency learning are two of their strong suits. Several modules form a chain in this network’s design. Information from earlier processing steps is saved in these modules. These modules’ architectures are different from those of conventional recurrent neural networks. A typical LSTM is built from many independent memory units (cells). Cell states, such as whether they are hidden, are passed down from one cell to the next. The data is being processed during its onward progress through the cell state. Input, forget, and output gates are the main controllers of the memory blocks. The input gate augments the current state of the cell with new data, while the forget gate eliminates any irrelevant or unnecessary data. The current cell state’s output is shown at the output gate. These gates regulate the learning process and prevent dependence, improving the network’s performance [13].
The Decision Tree method is a popular algorithm for training set. The decision tree approach is unique among supervised learning algorithms in that it can be used for either regression or classification [14]. Training models like as Decision Trees can be used to infer the class or value of a target variable with relative training data. Based on the variable being targeted, decision trees may be classified as either categorical or continuous. Decision Tree was utilized in conjunction with LSTM to assess and evaluate input data for the purpose of predicting new instances of COVID-19 infections based on the suggested model in this research.
Determination Coefficient (R2) and Root Mean Square Error (RMSE) are used to evaluate the forecasting models. These metrics provide understanding of the precision and reliability of the models applied to the data. The mathematical expressions for these indices are given in Eqs. (1) and (2) [12].
where
Numerous elements and qualities from the patient’s history need to be explored to generate a COVID-19 for a given outcome. Due to the critical nature of COVID-19 health status prediction and the sometimes-unbalanced nature of training data, mere accuracy is insufficient for validating the findings. As a result, we employed many metrics to assess the effectiveness of the suggested strategy and the other current methods we investigated. Calculations use the following symbols: True Positive (TP), True Negative (TN), False Positive (FP), and False Negative (FN), respectively.
True Positive (TP) and True Negative (TN) indicate that the classifier successfully identified “Death” and “Recovered” cases. FP: the total number of false-positive results generated by the model. Patients who tested negative were mislabeled as positive, denoted by the notation “FN”.
The precision of the categorization and prediction model is an essential indicator of its efficacy. To determine how well a classifier performed on a dataset consisting of (TP + TN) instances, we may use the formula:
Important measures like precision and Recall could be employed to find the accurately identified patients in a dataset with a mismatch across classes. The precision metric is found by dividing the number of TP instances by the sum of TP and FP instances, as shown in the following formula:
To find the suitable patients among all the correctly anticipated instances, recall/sensitivity is crucial. Consider the proportion of TP samples relative to the combined TP and FN proportions. Assuming you already know the values of TP and FN, you can use this equation to calculate recall.
If the dataset is unbalanced or skewed, the F1-score is the most critical metric that could be employed to assess a technique or classifier properly. To categorize the unbalanced COVID-19 patients, we focus on the F1-score to set our suggested strategy. The F1-score, which is a weighted average of recall and accuracy, is determined as follows:
Despite the usage of IoE, various issues, such as privacy, security, scalability, and quality of service, might affect how well the suggested solution is used. We briefly outline the problems and their likely fix.
• Privacy-related challenges: Since the data gathered by wearable and mobile devices contains personally identifiable information, information privacy is an important concern for the proposed system. Even if compromising their privacy could prevent the spread of a dangerous illness, people still would not do it. Another possible use for stolen data obtained via a privacy breach is criminal activity.
• Potential remedies and suggestions for further research relating to privacy issues: Moving analytical procedures to middleware or periphery equipment with lighter procedures for essential or vulnerable data while just transmitting the conclusion label to the host for further response is one approach to privacy issues.
• Security challenge: Due to the adaptability of attacks and the quick speed of changes, security concerns have recently attracted much attention from researchers. Because the decision-analysis stage contains so much significant hazards, the data acquired by wearable sensors are susceptible. These assaults may modify the analysis stage judgment, leading to behaviors that may be risky or have a negative effect. Scalability and security concerns are mutually exclusive, implying that security becomes more prone to compromise as the number of devices rises.
• Issues with customer satisfaction and manageability: Since there are now so many smart sensors and devices, manageability and customer satisfaction have become major issues. The suggested architecture could be slowed down by the problem of network congestion brought on by serving all users and devices. These challenging times highlight the need of scalability from both the architecture and the network service provider in enabling hard and soft real-time systems. The framework is necessary to manage the data creation and storage process in light of the growth in device numbers.
The suggested work has a wide range of potential possibilities. Significantly increasing the accuracy rate will likely be the biggest challenge for our future efforts. Increasing the depth of the model in the future to observe how it impacts accuracy will allow us to create a more robust and broader model. We will make these models using cutting-edge, advanced deep learning algorithms. We utilized two publicly accessible datasets for this investigation. Increasing data utilization for the COVID-19 detection challenge is one of the future approaches.
Future research on COVID-19 detection that focuses on the identification of several classes and subclasses could be extremely fruitful. The healthcare sector will need to deploy the proposed approach in a real-time situation even if it works well on a publicly available dataset. As the quantity of data for the classifier grows, it would be fascinating to see if adding additional participants will have a beneficial or bad effect on the outcomes. Research on medical diagnostics and healthcare systems would benefit from the suggested DL-based method. Additionally, it will provide a valuable second view and aid in the COVID-19 screening by medical professionals.
The findings of this study recommend implementing a high-tech healthcare system. We also emphasize the need for integrated technological solutions to help control the spread of COVID-19 and other pandemics in the interval, while a vaccine is being developed. For the monitoring of physical healthcare, we provided fictitious structures. We have included a framework that integrates the components into a single framework to identify and categorize COVID-19 using IoT-cloud technologies. To help the Framework become a reality, we quickly described the technical aspects, offered an overview of possible problems, a list of likely answers, and suggested future research possibilities. Furthermore, the use of AI-based techniques has been stressed as a substitute for clinical techniques to simulate the progression of this contagious illness. With this clever approach, the economic sector may be revitalized and the pressure on healthcare systems reduced. To forecast the global spread of the COVID-19 epidemic, two deep learning models were used in this study; long short-term memory network (LSTM) and Decision Tree (DT) were the models used. By comparing these models’ predicting abilities to those of the multilayer perceptron (MLP), determination coefficient (R2) and root mean square error were used (RMSE). However, one of the drawbacks of this study is that it does not address several additional limits, difficulties, and research areas, such as connection problems, battery consumption of wearable sensors and middleware, memory profiling, and others.
Acknowledgement: The authors are grateful to the Universiti Teknologi Malaysia and Taif University.
Funding Statement: The authors are grateful to the Taif University Researchers Supporting Project Number (TURSP-2020/36), Taif University, Taif, Saudi Arabia.
Author Contributions: The authors confirm contribution to the paper as follows: study conception and design: Fadhil Mukhlif, Norafida Ithnin; data collection: Ibrahim Hashem; analysis and interpretation of results: Roobaea Alroobaea, Sultan Algarni, Wael Y. Alghamdi; draft manuscript preparation: Fadhil Mukhlif. All authors reviewed the results and approved the final version of the manuscript.
Availability of Data and Materials: The article provide the proposed health framework, the data used from the official website of the World Health Organization (WHO) which is available in the following link: https://covid19.who.int/data.
Conflicts of Interest: The authors declare that they have no conflicts of interest to report regarding the present study.
References
1. I. A. Scott and E. W. Coiera, “Can AI help in the fight against COVID-19?” Medical Journal of Australia, vol. 213, no. 10, pp. 439–441, 2020. [Google Scholar] [PubMed]
2. “WHO Coronavirus Disease (COVID-19) Dashboard,” [Online]. Available https://covid19.who.int/ [Google Scholar]
3. V. Chamola, V. Hassija, V. Gupta and M. Guizani, “A comprehensive review of the COVID-19 pandemic and the role of IoT, drones, AI, blockchain, and 5 G in managing its impact,” IEEE Access, vol. 8, pp. 90225–90265, 2020. [Google Scholar]
4. M. Cascella, M. Rajnik, A. Aleem, S. C. Dulebohn and R. di Napoli, “Features, evaluation, and treatment of coronavirus (COVID-19),” National Library of Medicine, StatpearlsPublishing, Treasure Island (FL2022. [Google Scholar]
5. D. Etherington, “Estimote launches wearables for workplace-level contact tracing for COVID-19,” TechCrunch, 2020. [Google Scholar]
6. M. Talha, S. Ali, S. Shah, F. G. Khan and J. Iqbal, “Integration of big data and deep learning,” in Deep Learning: Convergence to Big Data Analytics, Singapore: Springer, 2019. [Online]. Available: https://doi.org/10.1007/978-981-13-3459-7_4 [Google Scholar] [CrossRef]
7. A. Gumaei, W. N. Ismail, M. R. Hassan, M. M. Hassan, E. Mohamed et al., “A decision-level fusion method for COVID-19 patient health prediction,” Big Data Research, vol. 27, no. 100287, pp. 11, 2022. [Google Scholar]
8. M. Marzouk, N. Elshaboury, A. Abdel-Latif and S. Azab, “Deep learning model for forecasting COVID-19 outbreak in Egypt,” Process Safety and Environmental Protection, vol. 153, pp. 363–375, 2021. [Google Scholar] [PubMed]
9. S. Dash, S. Chakravarty, S. N. Mohanty, C. R. Pattanaik and S. Jain, “A deep learning method to forecast COVID-19 outbreak,” New Generation Computing, vol. 39, no. 3–4, pp. 515–539, 2021. [Google Scholar] [PubMed]
10. S. Yasar, C. Colak and S. Yologlu, “Artificial intelligence-based prediction of COVID-19 severity on the results of protein profiling,” Computer Methods and Programs in Biomedicine, vol. 202, no. 105996, pp. 12, 2021. [Google Scholar]
11. N. Nasser, Q. Emad-ul-Haq, M. Imran, A. Ali, I. Razzak et al., “A smart healthcare framework for detection and monitoring of COVID-19 using IoT and cloud computing,” Neural Computing and Applications, pp. 1–15, 2021. [Google Scholar]
12. S. A. Khowaja, P. Khuwaja, K. Dev and G. D’Aniello, “VIRFIM: An AI and internet of medical things-driven framework for healthcare using smart sensors,” Neural Computing and Applications, pp. 1–18, 2021. [Google Scholar]
13. C. Sohrabi, Z. Alsafi, N. O’Neill, M. Khan, A. Kerwan et al., “World health organization declares global emergency: A review of the 2019 novel coronavirus (COVID-19),” International Journal of Surgery, vol. 76, pp. 71–76, 2020. [Google Scholar] [PubMed]
14. D. Ivanov and A. Dolgui, “Viability of intertwined supply networks: Extending the supply chain resilience angles towards survivability. A position paper motivated by COVID-19 outbreak,” International Journal of Production Research, vol. 58, no. 10, pp. 2904–2915, 2020. [Google Scholar]
15. Q. V. Pham, D. C. Nguyen, T. Huynh-The, W. J. Hwang and P. N. Pathirana, “Artificial intelligence (AI) and big data for coronavirus (COVID-19) pandemic: A survey on the state-of-the-arts,” IEEE Access, vol. 8, pp. 130820–130839, 2020. [Google Scholar] [PubMed]
16. A. M. Turing, “Computing machinery and intelligence,” In: R. Epstein, G. Roberts and G. Beber (Eds.Parsing the Turing Test. Dordrecht: Springer, 2009. [Online]. Available: https://doi.org/10.1007/978-1-4020-6710-5_3 [Google Scholar] [CrossRef]
17. J. Moor, “The turing test: The elusive standard of artificial intelligence,” Computational Linguistics, vol. 30, no. 1, pp. 115–116, 2004. https://doi.org/10.1162/089120104773633420 [Google Scholar] [CrossRef]
18. D. Crevier, AI: The Tumultuous History of the Search for Artificial Intelligence. New York, USA: Basic Books, Inc., 1993. [Google Scholar]
19. H. Abdulkareem, Karrar, A. A. Mutlag, A. M. Dinar, J. Frnda et al., “Smart healthcare system for severity prediction and critical tasks management of COVID-19 patients in IoT-fog computing environments,” Computational Intelligence and Neuroscience, vol. 2022, pp. 17, 2022. [Google Scholar]
20. A. M. Dinar, E. A. Raheem, K. H. Abdulkareem, M. A. Mohammed, M. G. Oleiwie et al., “Towards automated multiclass severity prediction approach for COVID-19 infections based on combinations of clinical data,” Mobile Information Systems, vol. 2022, pp. 8, 2022. [Google Scholar]
21. K. H. Abdulkareem, M. N. Al-Mhiqani, A. M. Dinar, M. A. Mohammed, M. J. Al-Imari et al., “MEF: Multidimensional examination framework for prioritization of COVID-19 severe patients and promote precision medicine based on hybrid multi-criteria decision-making approaches,” Bioengineering, vol. 9, no. 9, pp. 457, 2022. [Google Scholar] [PubMed]
22. Y. Pan, “Heading toward artificial intelligence 2.0,” Engineering, vol. 2, no. 4, pp. 409–413, 2016. [Google Scholar]
23. B. M. Lake, T. D. Ullman, J. B. Tenenbaum and S. J. Gershman, “Building machines that learn and think like people,” Behavioral and Brain Sciences, vol. 40, pp. e253, 2017. [Google Scholar] [PubMed]
24. S. Russell and P. Norvig, Artificial Intelligence: A Modern Approach. USA: Pearson Education, Inc., 2002. [Google Scholar]
25. S. Y. Choi and D. Cha, “Unmanned aerial vehicles using machine learning for autonomous flight; state-of-the-art,” Advanced Robotics, vol. 33, no. 6, pp. 265–277, 2019. [Google Scholar]
26. D. Praveen Kumar, T. Amgoth and C. S. R. Annavarapu, “Machine learning algorithms for wireless sensor networks: A survey,” Information Fusion, vol. 49, pp. 1–25, 2019. [Google Scholar]
27. V. Praveena, A. Vijayaraj, P. Chinnasamy, I. Ali, R. Alroobaea et al., “Optimal deep reinforcement learning for intrusion detection in UAVs,” Computers, Materials & Continua, vol. 70, no. 2, pp. 2639–2653, 2022. [Google Scholar]
Cite This Article
 Copyright © 2023 The Author(s). Published by Tech Science Press.
Copyright © 2023 The Author(s). Published by Tech Science Press.This work is licensed under a Creative Commons Attribution 4.0 International License , which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
 Downloads
Downloads
 Citation Tools
Citation Tools