Induction Therapy Followed by Surgery in Advanced Thymic Epithelial Tumors: A 20-Year Systematic Review and Meta-Analysis
Giovanni Leuzzi1,*, Michele Ferrari1, Federica Sabia1, Alessandro Pardolesi1, Alessia Stanzi1, Claudia Proto2, Giuseppe Lo Russo2, Arsela Prelaj2, Monica Ganzinelli2, Matteo Calderoni1, Clarissa Uslenghi1, Ugo Pastorino3, Piergiorgio Solli1
1 Division of Thoracic Surgery, Fondazione IRCCS Istituto Nazionale dei Tumori, Milan, Italy
2 Department of Medical Oncology, Fondazione IRCCS Istituto Nazionale dei Tumori, Milan, Italy
3 Lung Cancer Prevention Research, Fondazione IRCCS Istituto Nazionale dei Tumori, Milan, Italy
* Corresponding Author: Giovanni Leuzzi. Email: 
(This article belongs to the Special Issue: Integrative Strategies in Cancer Therapy)
Oncology Research https://doi.org/10.32604/or.2026.077158
Received 03 December 2025; Accepted 28 May 2026; Published online 22 June 2026
Abstract
Backgrounds: Despite the availability of multimodal strategies, no universally accepted guidelines exist for the management of advanced Thymic Epithelial Tumors (TETs), particularly in locally advanced thymomas. The aim of this study was to evaluate the oncological and surgical outcomes of induction therapy (IT) followed by surgery in patients with Masaoka–Koga stage III–IVA TETs. To this end, we conducted a systematic review and meta-analysis assessing surgical-pathological and survival outcomes.
Methods: Following Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, a systematic search of PubMed, Embase, and the Cochrane Central Register of Controlled Trials was performed. Twenty-four studies published between 2003 and 2023 were included, comprising 749 patients treated with IT before surgical resection. The co-primary endpoints were Overall survival (OS) and Progression-free survival (PFS). Random-effects meta-analysis assessed pooled outcomes, while heterogeneity, publication bias, and meta-regression analyses were performed to explore potential moderators (year, histology, stage). The study was registered in Prospective Register of Systematic Reviews (PROSPERO) (CRD420251026044).
Results: Of the included studies, 6 were prospective and 18 retrospective; 9 analyzed thymomas only, while 15 included both thymomas and thymic carcinomas. Regarding stage distribution, 4 studies focused on stage III, 11 on stage III–IV, 3 on stage IV, and 2 also included earlier stages. Response to IT was assessed by Response Evaluation Criteria in Solid Tumors (RECIST) in 11 studies and World Health Organization (WHO) criteria in 4. The pooled rate of radiological response to IT, completeness of resection, 5-year OS, 10-year OS and 5-year PFS were 62.8%, 71.6%, 77.6%, 54.3% and 55.6%, respectively. Meta-regression showed histology significantly influenced 10-year OS (
p-value 0.0418) as well as on PFS (
p-value 0.0042) and treatment period on PFS (
p-value 0.0007)
Conclusions: Induction therapy followed by surgery provides acceptable long-term outcomes in advanced TETs. Histology remains a key prognostic factor, but 10-year OS has not improved over the past two decades, underscoring the need for innovative, histology-tailored therapeutic strategies to enhance survival.
Graphical Abstract
Keywords
Induction therapy; thymic epithelial tumors; metaregression; survival; CAP; multimodality therapy
 Open Access
Open Access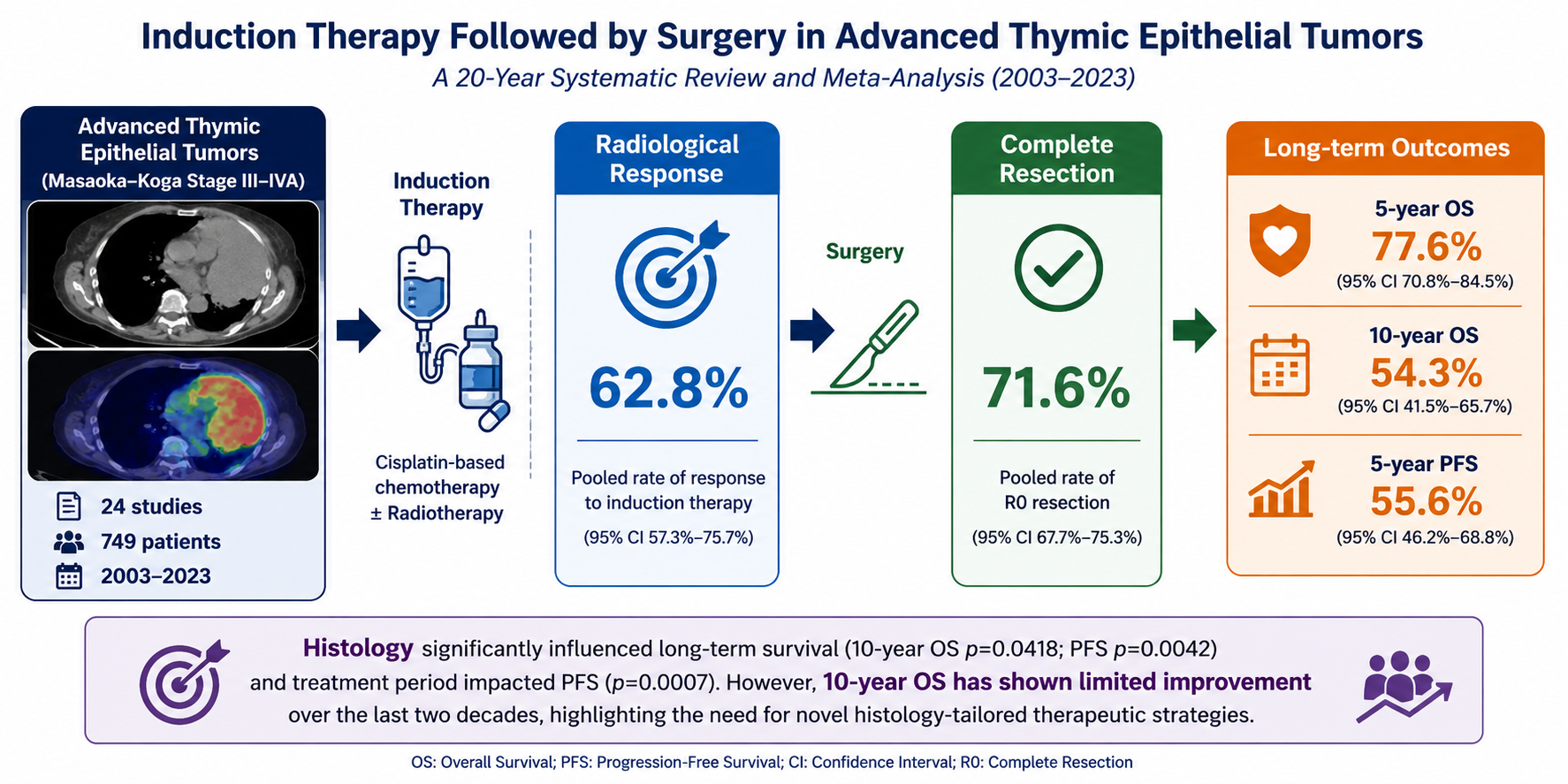

 Submit a Paper
Submit a Paper Propose a Special lssue
Propose a Special lssue Download PDF
Download PDF Supplementary Material File
Supplementary Material File Downloads
Downloads
 Citation Tools
Citation Tools